176 Liver Biopsy Evaluation: A Novel Approach To Arriving at Differential Diagnosis. Gary Kanel MD
|
|
|
- Monica Harvey
- 6 years ago
- Views:
Transcription
1 176 Liver Biopsy Evaluation: A Novel Approach To Arriving at Differential Diagnosis Gary Kanel MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste Chicago, IL 60603
2 176 Liver Biopsy Evaluation: A Novel Approach To Arriving at Differential Diagnosis Liver biopsies show various histologic features that most often involve both the portal tracts and parenchyma. The pathologist, for instance, may see a liver biopsy demonstrating portal lymphocytic infiltrates, atypical bile ducts, mild lobular inflammation, and mild fatty change. Many liver diseases can show these individual features, yet only a few show most or all of the features together. This session will discuss the most common liver histology in table format and how the information acquired from these tables can be used in arriving at differential diagnoses. The session will also show the attendees how pertinent clinical and laboratory correlation can help arrive at the most probable diagnosis. A general review of liver pathology highlighting these pertinent histologic features will be presented. Identify the various morphologic features in the portal tracts and parenchyma seen in liver biopsy material Arrive at likely diagnoses and differential possibilities using access to specific tables that list the various liver diseases that show these individual features Assess the pertinent clinical and laboratory data to arrive at a most probable clinical-pathologic diagnosis FACULTY: Gary Kanel MD Practicing Pathologists Surgical Pathology Surgical Pathology (GI, GU, Etc.) 2.0 CME/CMLE Credits Accreditation Statement: The American Society for Clinical Pathology (ASCP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education (CME) for physicians. This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME). Credit Designation: The ASCP designates this enduring material for a maximum of 2 AMA PRA Category 1 Credits. Physicians should only claim credit commensurate with the extent of their participation in the activity. ASCP continuing education activities are accepted by California, Florida, and many other states for relicensure of clinical laboratory personnel. ASCP designates these activities for the indicated number of Continuing Medical Laboratory Education (CMLE) credit hours. ASCP CMLE credit hours are acceptable to meet the continuing education requirements for the ASCP Board of Registry Certification Maintenance Program. All ASCP CMLE programs are conducted at intermediate to advanced levels of learning. Continuing medical education (CME) activities offered by ASCP are acceptable for the American Board of Pathology s Maintenance of Certification Program.
3 Liver Biopsy Evaluation: A Novel Approach to Arriving at Differential Diagnoses Gary C. Kanel, M.D. Professor of Clinical Pathology Keck School of Medicine, USC Associate Pathologist LAC+USC Medical Center and USC University Hospital Disclosure In compliance with the ACCME and ASCP expectations of CME that is independent from commercial influence or bias, I disclose my relevant financial relationships below: Lead author of Atlas of Liver Pathology 3e Elsevier publisher, 2011 Objective and goals of this session This session addresses the use of tables at arriving at differential diagnoses in liver biopsy interpretation. Use of tables is a useful adjunct in helping solve diagnostic problems. For example, if a Mallory body is present on liver biopsy, it is quite useful to refer to a table listing all of the liver diseases associated with Mallory bodies. We often signal out, however, only one morphologic feature and don t give others much importance. Are other features significant as well? For example, in this same biopsy, is a portal or lobular lymphocytic infiltrate important in diagnoses, or are those features rather insignificant? Does the presence of a granuloma as well entirely change the diagnostic possibilities, or not? 1


4 Objective and goals of this session Why not note and list all of the morphology seen on biopsy, whether we initially feel those features are important or not? After all of the features are listed, not giving any significance of one over the other, the pathologist can refer to specific tables addressing each of these features, these tables listing the various diseases associated with that particular histology. By reviewing all of the tables, the pathologist can then arrive at a possible diagnosis with differentials by noting the diseases listed more than once. A final diagnosis can then be made after pertinent clinical and laboratory information is integrated. Objective and goals of this session This session addresses this approach, with the use of tables in a more objective rather than subjective way. The session will be presented as follows: Review of the anatomy and histology of the normal liver Review of the numerous tables, with histologic examples, that list liver diseases that frequently (in italics) as well as less commonly show specific histological features Show four examples demonstrating how the tables work together in arriving at diagnoses and differential possibilities Briefly discuss the corresponding liver disorders for each of these examples Gross Anatomy of Normal Liver 2




5 Three Dimensional Architecture Lobule with terminal hepatic (central) venule Portal tract Hepatic lobule Terminal hepatic (central) venule Portal tract Normal Liver Portal Tracts Bile ducts Hepatic arteriole Portal venule Fibroconnective tissue framework 3
 7 Bile Ducts: Inflammation by Lymphocytes")
6 Normal Liver Parenchyma Hepatic cords Sinusoids Kupffer/ Endothelial cells Terminal (central) hepatic venules Histological features (Table format*) Portal Tracts 1 Portal Lymphocytes 2 Portal Neutrophils 3 Portal Plasma Cells 4 Portal Eosinophils 5 Portal Fibrosis, Cirrhosis 6 Bile Ducts: Inflammation by Neutrophils (Acute Cholangitis) 7 Bile Ducts: Inflammation by Lymphocytes (Nonsuppurative Cholangitis) 8 Bile Ducts: Periductal Fibrosis 9 Bile Ducts: Cytologic Atypia, Duct Loss (Ductopenia) Parenchyma and Vessels 10 Lobular Necrosis with Inflammation 11 Lobular Necrosis with Minimal to Absent Inflammation 12 Cholestasis, Simple 13 Fatty Change 14 Granulomas 15 Mallory Bodies 16 Inclusions: Hepatocytes 17 Pigments 18 Sinusoids: Fibrosis 19 Sinusoids: Circulating Cells 20 Vessels (Excluding Sinusoids): Inflammation 21 Vessels (Excluding Sinusoids): Thrombosis, Occlusion *Modified from Kanel GC, Korula J. Atlas of Liver Pathology, 3e. Elsevier, 2011 Portal Lymphocytes Acute viral hepatitis, HCV Chronic viral hepatitis, HCV Periportal interface activity ( piecemeal necrosis) 4
7 Allograft, acute (cellular) rejection Alcoholic cirrhosis Autoimmune hepatitis Biliary atresia, extrahepatic Brucellosis Caroli disease Chronic granulomatous disease of childhood Cytomegalovirus Epstein Barr virus Erythropoietic protoporphyria Extrahepatic bile duct obstruction, late stage Graft versus host disease Idiopathic adulthood ductopenia Indian childhood cirrhosis Inflammatory bowel disease Lassa fever Table 1 Portal Lymphocytes Leukemia, lymphocytic Lymphoma, Hodgkin s (non tumor liver) and non Hodgkin s Neonatal hepatitis Non alcoholic steatohepatitis Nonspecific reactive hepatitis Porphyria cutanea tarda Primary biliary cirrhosis Primary sclerosing cholangitis Q fever Rheumatoid arthritis Rocky Mountain spotted fever Salmonellosis Sarcoidosis Tuberculosis Viral hepatitis, acute and chronic Wilson disease Yellow fever Periportal interface inflammation in active stage of disease Portal Neutrophils Recurrent pyogenic cholangiohepatitis Portal microabscess Table 2 Portal Neutrophils Alcoholic hepatitis Allograft, acute (cellular) rejection Autoimmune hepatitis Biliary atresia, extrahepatic Caroli disease Choledochal cyst (associated bile duct obstruction) Churg Strauss syndrome Cystic fibrosis Extrahepatic bile duct obstruction, early and mid stages Hepatic vein phlebitis Hyperalimentation (TPN), infants Inspissated bile syndrome Polyarteritis nodosa Primary biliary cirrhosis Primary sclerosing cholangitis Pylephlebitis Pyogenic abscess Reactive changes, bacterial infections Recurrent pyogenic cholangiohepatitis Syphilis, secondary Toxic shock syndrome Tuberculosis (severe) 5
 Echinococcosis (hydatid cyst) Epstein Barr virus Hodgkin s lymphoma (nontumor liver) Leishmaniasis Multiple myeloma Primary")
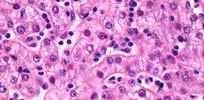
8 Portal Plasma Cells Autoimmune hepatitis Table 3 Portal Plasma Cells Acute viral hepatitis, HAV Allograft, acute (cellular) rejection Autoimmune hepatitis Chronic granulomatous disease of childhood Chronic viral hepatitis, HBV Chronic viral hepatitis (other than HBV) Echinococcosis (hydatid cyst) Epstein Barr virus Hodgkin s lymphoma (nontumor liver) Leishmaniasis Multiple myeloma Primary biliary cirrhosis Primary sclerosing cholangitis Q fever Visceral larva migrans Waldenstrom s macroglobulinemia Wilson disease Portal Eosinophils Allograft, acute (cellular) rejection 6
 rejection Churg Strauss syndrome Eosinophilic gastroenteritis Epstein Barr virus Hodgkin s lymphoma (non tumor liver)")
9 Table 4 Portal Eosinophils Parasitic infestations Ascariasis Capillariasis Clonorchiasis Echinococcosis (hydatid cyst) Enterobiasis Fascioliasis Schistosomiasis (early) Strongyloidiasis Visceral larva migrans Acute fatty liver of pregnancy Allograft, acute (cellular) rejection Churg Strauss syndrome Eosinophilic gastroenteritis Epstein Barr virus Hodgkin s lymphoma (non tumor liver) Hypereosinophilic syndrome Polyarteritis nodosa Primary sclerosing cholangitis Primary biliary cirrhosis Recurrent pyogenic cholangiohepatitis Portal Fibrosis, Cirrhosis Alcoholic liver disease Portal and perivenular fibrosis (trichrome) Chronic hepatitis, HCV Well established cirrhosis (trichrome) Table 5 Portal Fibrosis, Cirrhosis Alcoholic cirrhosis Metabolic diseases (e.g., Glycogen Alcoholic hepatitis storage disease III, Gaucher disease) Alpha 1 antitrypsin deficiency Non alcoholic steatohepatitis Autoimmune hepatitis (cholangitis) * Paucity of ducts syndrome, nonsyndromatic* Autoimmune hepatitis Biliary atresia, extrahepatic * Primary biliary cirrhosis * Cystic fibrosis * Primary sclerosing cholangitis * Extrahepatic bile duct obstruction, Progressive familial intrahepatic late stage * cholestasis (Byler syndrome)* Erythropoietic protoporphyria Sarcoidosis Hereditary hemochromatosis Syphilis, tertiary (hepar lobatum) Idiopathic adulthood ductopenia * Veno occlusive disease (VOD), Hepatic venous outflow obstruction chronic (Budd Chiari syndrome), chronic Venous congestion secondary to Hyperalimentation (TPN) right sided heart failure, chronic Indian childhood cirrhosis Viral hepatitis, chronic Inflammatory bowel disease: Wilson disease Ulcerative colitis (* Biliary type Cardiac type) 7
10 Bile Ducts: Inflammation by Neutrophils (Acute Cholangitis) Acute bile duct obstruction Table 6 Bile Ducts: Inflammation by Neutrophils (Acute Cholangitis) Allograft, acute (cellular) rejection Biliary atresia, extrahepatic Caroli disease Choledochal cyst Cystic fibrosis Echinococcosis (hydatid cyst) (cyst rupture) Extrahepatic bile duct obstruction Hepatic artery thrombosis Parasitic infestations Primary sclerosing cholangitis (large ducts only) Pyogenic abscess Reactive changes, bacterial infections Recurrent pyogenic cholangiohepatitis Salmonellosis Syphilis, secondary Toxic shock syndrome Tuberculosis Bile Ducts: Inflammation by Lymphocytes (Nonsuppurative Cholangitis) Primary biliary cirrhosis 8
 Chronic viral hepatitis, HCV Cryptosporidiosis Cytomegalovirus Epstein Barr virus Graft versus host disease Hodgkin s lymphoma (non tumor liver) Human immunodeficiency virus")
11 Table 7 Bile Ducts: Inflammation by Lymphocytes (Nonsuppurative Cholangitis) Acute viral hepatitis, HCV, HEV Allograft, acute (cellular) rejection Autoimmune hepatitis (cholangitis) Caroli disease (biliary cyst walls) Chronic viral hepatitis, HCV Cryptosporidiosis Cytomegalovirus Epstein Barr virus Graft versus host disease Hodgkin s lymphoma (non tumor liver) Human immunodeficiency virus (HIV) associated cholangiopathy) Idiopathic adulthood ductopenia Paucity of ducts syndrome, syndromatic (Alagille s) Primary biliary cirrhosis Primary sclerosing cholangitis (also large ducts) Recurrent pyogenic cholangiohepatitis (large ducts only) Sarcoidosis Bile Ducts: Periductal Fibrosis Primary sclerosing cholangitis Table 8 Bile Ducts: Periductal Fibrosis Caroli disease Choledochal cyst Cryptosporidiosis Echinococcosis (hydatid cyst) Eosinophilic gastroenteritis Extrahepatic bile duct obstruction, early stage Extrahepatic bile duct obstruction, early to mid stage Extrahepatic bile duct obstruction, late stage Human immunodeficiency virus (HIV) associated cholangiopathy Idiopathic adulthood ductopenia Microsporidiosis idi i Primary sclerosing cholangitis Recurrent pyogenic cholangiohepatitis 9
12 Bile Ducts: Cytologic Atypia, Duct Loss (Ductopenia) Allograft, early chronic rejection Duct atypia Primary sclerosing cholangitis Duct loss Table 9 Bile Ducts: Cytologic Atypia, Duct Loss (Ductopenia) Allograft, hepatic artery thrombosis Allograft, chronic rejection Autoimmune hepatitis (cholangitis) Cystic fibrosis Cytomegalovirus, adult Extrahepatic bile duct obstruction, late stage (small ducts) Graft versus host disease Hodgkin s lymphoma (non tumor liver) Human immunodeficiency virus (HIV) associated cholangiopathy) Idiopathic adulthood ductopenia Paucity of ducts syndrome, non syndromatic Paucity of ducts syndrome, syndromatic (Alagille s) Polycystic disease, perinatal (infantile) form Primary biliary cirrhosis Primary sclerosing cholangitis (small ducts) Progressive familial intrahepatic cholestasis (Byler syndrome) Sarcoidosis Lobular Necrosis with Inflammation Acute viral hepatitis, HCV Lymphocytic infiltrates Alcoholic hepatitis Neutrophilic infiltrates 10
13 Table 10 Lobular Necrosis with Inflammation Alcoholic hepatitis PMN * Alcoholic foamy degeneration PMN, L * Allograft, acute (cellular) rejection PMN, L * Alpha 1 antitrypsin deficiency L Autoimmune hepatitis L, PC * Benign recurrent intrahepatic cholestasis L ** Biliary atresia, extrahepatic PMN, L ** Caroli disease PMN, L ** Choledochal cyst (with bile duct obstruction) PMN ** Cystic fibrosis PMN * Extrahepatic bile duct obstruction PMN ** Graft versus host disease L Hemochromatosis L Indian childhood cirrhosis PMN, L *Cholestasis in active disease **Cholestasis as a primary factor in the disease L Lymphocytes PMN Neutrophils PC Plasma cells EO Eosinophils Table 10 Lobular Necrosis with Inflammation Infections, non viral Bacterial (pyogenic abscess) PMN * Bacterial (e.g., salmonellosis) PMN Fungal (e.g., cryptococcosis) L Mycobacterium L Parasitic (e.g., Amebiasis) L, EO Inflammatory bowel disease L Neonatal hepatitis PMN, L * Non alcoholic steatohepatitis PMN, L Primary biliary cirrhosis L, PC Primary sclerosing cholangitis L * Recurrent pyogenic cholangiohepatitis PMN ** Sarcoidosis L * Viral hepatitis, acute and chronic Hepatotropic viruses L * EBV/CMV hepatitis L Wilson disease L * *Cholestasis in active disease **Cholestasis as a primary factor in the disease L Lymphocytes PMN Neutrophils PC Plasma cells EO Eosinophils Lobular Necrosis with Minimal to Absent Inflammation Coagulative ischemic necrosis 11
14 Table 11 Lobular Necrosis with Minimal to Absent Inflammation Acute hepatic venous outflow obstruction (Budd Chiari syndrome) Allograft, hepatic artery thrombosis Amebiasis Aspergillosis Babesiosis Churg Strauss syndrome Dengue fever Hyperpyrexia and heat stroke Hypoxic injury secondary to hypotension Malaria Pneumocystis carinii infection Polyarteritis nodosa Viruses, non A G (e.g., Ebola, Marburg, Adenovirus, Echovirus, Lassa fever, HSV) Rheumatoid arthritis Sickle cell anemia Spontaneous rupture in pregnancy Systemic lupus erythematosus (secondary to arteritis) Toxemia of pregnancy Veno occlusive disease (VOD) Cholestasis, Simple Hyperalimentation (TPN) Table 12 Cholestasis, Simple Acute fatty liver of pregnancy Amyloidosis Criglar Najjar syndrome Cystic fibrosis Fibrolamellar hepatocellular carcinoma Hepatic venous outflow obstruction (Budd Chiari syndrome), acute and chronic Hepatocellular carcinoma, common patterns Hyperalimentation (TPN) Hypoxic injury secondary to hypotension Infection associated (reactive) hemophagocytic syndrome Inspissated bile syndrome Intrahepatic cholestasis of pregnancy Liver cell adenoma Nodular regenerative hyperplasia Paucity of ducts syndrome, syndromatic (Alagille s) and nonsyndromatic Progressive familial intrahepatic cholestasis (Byler syndrome) Sickle cell anemia Veno occlusive disease (VOD), acute and chronic Venous congestion secondary to right sided heart failure, acute and chronic 12
15 Fatty Change Alcoholic fatty liver Table 13 Fatty Change (>50% liver cells involved) Macrovesicular Abetalipoproteinemia Acute alcoholic fatty liver with or without cholestasis Alcoholic fatty liver Alcoholic hepatitis Galactosemia Hereditary fructose intolerance Homocystinuria Kwashiorkor (later stage) Long chain acyl CoA dehydrogenase deficiency Non alcoholic fatty liver Non alcoholic steatohepatitis Perivenular alcoholic fibrosis Systemic carnitine deficiency Weber Christian disease Microvesicular Acute fatty liver of pregnancy Alcoholic foamy degeneration Alper s disease Cholesterol ester storage disease Kwashiorkor (early stage) dehydrogenase deficiency Medium chain acyl CoA dehydrogenase deficiency Reye syndrome Wolman s disease Table 13 Fatty Change (<50% cells involved, macrovesicular) Allograft, recurrent hepatitis, HCV Alpha 1 antitrypsin deficiency Amebiasis Chronic viral hepatitis, HCV Cystic fibrosis Cytomegalovirus Epstein Barr virus Gilbert syndrome Glycogen storage disease I, II, VI Hereditary hemochromatosis Hereditary tyrosinemia Human immunodeficiency virus (HIV) Hyperalimentation (TPN), adult Inflammatory bowel diseases Leishmaniasis Malaria Mannosidosis Marasmus Porphyria cutanea tarda Primary sclerosing cholangitis Q fever Reactive changes, non specific and bacterial infections Rheumatoid arthritis Rocky Mountain spotted fever Sickle cell anemia Systemic lupus erythematosus Toxoplasmosis Tuberculosis Wilson disease 13
16 Table 13 Fatty Change (<50% cells involved, microvesicular) Acute and chronic viral hepatitis, HBV and delta Hyperpyrexia and heat stroke Lyme disease Salmonellosis Toxic shocksyndrome syndrome Yellow fever Granulomas Tuberculosis Acute alcoholic fatty liver with/without cholestasis Alcoholic fatty liver Alcoholic hepatitis Chronic granulomatous disease of childhood Eosinophilic gastroenteritis Foreign body giant cell reaction Idiopathic granulomatous hepatitis Infectious: Viral (e.g., acute HCV, CMV, EBV) Fungal (e.g., Cryptococcus, Histoplasma) Bacterial (e.g., Salmonella, Brucella) Mycobacterium Parasitic (e.g., Schistosoma, visceral larva migrans) Inflammatory bowel disease: Crohn s disease Table 14 Granulomas Neoplasms, tumor like lesions: Hepatocellular carcinoma Hodgkin s lymphoma (non tumor liver) Inflammatory pseudotumor Langerhans cell histiocytosis Liver cell adenoma Non alcoholic steatohepatitis Nonspecific reactive hepatitis Polyarteritis nodosa Polymyalgia rheumatica Primary biliary cirrhosis Rheumatoid arthritis Sarcoidosis Systemic lupus erythematosus 14
17 Mallory Bodies Alcoholic hepatitis Abetalipoproteinemia Alcoholic hepatitis Alpha 1 antitrypsin deficiency Biliary atresia, extrahepatic Extrahepatic bile duct obstruction, mid/late stage Focal nodular hyperplasia Glycogen storage disease Ia Hepatocellular carcinoma, common patterns Hyperalimentation (TPN), adults Table 15 Mallory Bodies Indian childhood cirrhosis Kwashiorkor Liver cell adenoma Non alcoholic steatohepatitis Perivenular alcoholic fibrosis Primary biliary cirrhosis Primary sclerosing cholangitis Weber Christian disease Wilson disease Inclusions: Hepatocytes Chronic viral hepatitis, HBV Ground glass cells (HBsAg) Non alcoholic steatosis Glycogenated nuclei 15
18 Table 16 Inclusions: Hepatocytes Nuclear Viral inclusions Adenovirus Cytomegalovirus (immunocompromised, allograft) Herpes simplex virus (Cowdry A, B) Herpes zoster Parvovirus (B19 virus) Rubeola Yellow fever Glycogenated nuclei Alpha 1 antitrypsin deficiency Glycogen storage diseases I, III, VI Hereditary hemochromatosis Non alcoholic li fatty liver Non alcoholic steatohepatitis Porphyria cutanea tarda Wilson disease Table 16 Inclusions: Hepatocytes Cytoplasmic Acute fatty liver of pregnancy Megamitochondria Alcoholic liver disease Megamitochondria Fatty liver, foamy degeneration, alcoholic hepatitis Alpha 1 antitrypsin deficiency Periportal eosinophilic DiPAS + globule (A 1 AT) Chronic viral hepatitis, HBV Ground glass cells Cytomegalovirus Cytoplasmic inclusions (Immunocompromised, allograft) Fibrinogen storage disease Eosinophilic globules (fibrinogen) Glycogen storage disease IV Eosinophilic DiPAS + globules (amylopectin) Hypoxic injury from hypotension Eosinophilic hyaline globules (zone 3 liver cells) Non alcoholic steatohepatitis Megamitochondria Porphyria cutanea tarda Needle shaped, birefringent Reye syndrome Distorted mitochondria Rubeola Eosinophilic globules Venous congestion secondary to Eosinophilic hyaline globules (zone 3 liver cells) right sided heart failure Pigments Hereditary hemochromatosis Hemosiderin with iron stain 16
19 Pigments Dubin Johnson syndrome Lipochrome like Table 17 Pigments: Hemosiderin Hepatocytes Portal macrophages, Kupffer cells Acute viral hepatitis + Alcoholic cirrhosis + Chronic viral hepatitis, HCV + Cystic fibrosis + Erythropoietic protoporphyria + Galactosemia + Gaucher disease + Graft versus host disease + Hematologic abnormalities Anemias secondary to abnormal + ++ hemoglobins, hemolysis Anemias secondary to infection, + + ineffective erythropoiesis Leukemia, lymphoma, + ++ myeloproliferative disorders Table 17 Pigments: Hemosiderin Hepatocytes Portal macrophages, Kupffer cells Hemosiderosis (secondary iron overload) + ++ Hereditary hemochromatosis ++ + Hereditary tyrosinemia + Hyperalimentation (TPN), adults + + Infection associated (reactive) + hemophagocytic syndrome Inspissated bile syndrome + Malaria + ++ Neonatal hepatitis +/++ Non alcoholic steatohepatitis + Porphyria cutanea tarda +/++ Wilson disease
20 Table 17 Pigments: Copper Often abundant Biliary atresia, extrahepatic Idiopathic adulthood ductopenia Indian childhood cirrhosis Paucity of ducts syndrome, nonsyndromatic Paucity of ducts syndrome, syndromatic (Alagille s) Primary biliary cirrhosis (late stage) Primary sclerosing cholangitis (late stage) Progressive familial intrahepatic cholestasis (Byler syndrome) Wilson disease Occasionally increased Alpha 1 antitrypsin deficiency (neonate) Congenital hepatic fibrosis Cystic fibrosis Extrahepatic bile duct obstruction, late stage Fibrolamellar hepatocellular carcinoma Focal nodular hyperplasia Galactosemia Graft versus host disease Hereditary fructose intolerance Hyperalimentation (TPN), adults Table 17 Pigments: Other Angiosarcoma Thorotrast (in non tumor) Chronic granulomatous Lipochrome disease of childhood Chronic viral hepatitis IV particulate injectant (IV drug users) Cystinosis Cystine Dubin Johnson syndrome Lipochrome like Erythropoietic protoporphyria Protoporphyrin Focal nodular hyperplasia Lipochrome Gilbert syndrome Lipochrome Hepatoblastoma Melanin Liver cell adenoma Lipochrome Malaria Hemozoin Niemann Pick disease Lipochrome like Porphyria cutanea tarda Lipochrome Schistosomiasis Hemozoin like Wilson disease Lipochrome Sinusoids: Fibrosis Alcoholic hepatitis Perivenular fibrosis (trichrome ) 18
, adults Hyperalimentation (TPN), infants Indian childhood cirrhosis Leishmaniasis (long")
 Neonatal hepatitis Non alcoholic steatohepatitis Non cirrhotic portal fibrosis Paucity of ducts syndrome, nonsyndromatic")
21 Table 18 Sinusoids: Fibrosis Alcoholic foamy degeneration Alcoholic hepatitis Allograft, fibrosing cholestatic hepatitis Allograft, chronic (ductopenic) rejection Chronic viral hepatitis, HCV Cystic fibrosis Erythropoietic protoporphyria Hyperalimentation (TPN), adults Hyperalimentation (TPN), infants Indian childhood cirrhosis Leishmaniasis (long term infection) Metabolic (e.g., cholesterol ester storage disease, gangliosidosis, GM2, Gaucher disease) Neonatal hepatitis Non alcoholic steatohepatitis Non cirrhotic portal fibrosis Paucity of ducts syndrome, nonsyndromatic Perivenular alcoholic fibrosis Schistomosiasis Sickle cell anemia Syphilis, congenital Wilson disease Sinusoids: Circulating Cells T cell lymphoma/cll Table 19 Sinusoids: Circulating Cells Acute viral hepatitis, HCV L Alcoholic hepatitis PMN Allograft, acute (cellular) L rejection (severe) Chronic viral hepatitis, HCV L Cytomegalovirus L Epstein Barr virus L Leishmaniasis L Leukemia, CLL L Leukemia, CML PMN Lyme disease L, PMN Malaria (tropical L splenomegaly syndrome ) Nonspecific reactive L hepatitis Pyogenic abscess PMN Reactive changes, PMN bacterial infections Rheumatoid arthritis L Rocky Mountain L spotted fever Salmonellosis L Surgical hepatitis PMN L Lymphocytes PMN Neutrophils 19
22 Vessels (Excluding Sinusoids): Inflammation, Thrombosis/Occlusion Churg Strauss syndrome Arteritis Table 20 Vessels (Excluding Sinusoids): Inflammation Arteries, arterioles Allograft, acute (cellular) rejection Allograft, hyperacute (humoral) rejection Churg Strauss syndrome Hereditary hemorrhagic telangiectasia (OWR) Polyarteritis nodosa Rheumatoid arthritis Rocky Mountain spotted fever Syphilis, secondary Syphilis, tertiary Systemic lupus erythematosus Toxic shock syndrome Veins, venules Acute viral hepatitis Allograft, acute (cellular) rejection Autoimmune hepatitis Epstein Barr virus Graft versus host disease Hepatic vein phlebitis Non alcoholic steatohepatitis Perivenular alcoholic fibrosis Pylephlebitis Recurrent pyogenic cholangiohepatitis Salmonellosis Sarcoidosis Schistosomiasis Syphilis, secondary Toxic shock syndrome Table 21 Vessels (Excluding Sinusoids): Thrombosis, Occlusion Thrombosis, fibrous thickening/occlusion Alcoholic hepatitis Alcoholic cirrhosis Allograft, chronic (ductopenic) rejection Allograft, hepatic artery thrombosis Churg Strauss syndrome Congenital hepatic fibrosis Hepatic vein phlebitis Hepatic venous outflow obstruction (Budd Chiari syndrome), acute and chronic Myeloproliferative disorders (secondary hepatic vein thrombosis) Non cirrhotic portal fibrosis Polyarteritis nodosa Pylephlebitis Schistosomiasis Sickle cell anemia Venous congestion secondary to right sided heart failure, chronic Veno occlusive changes Alcoholic cirrhosis Alcoholic hepatitis Graft versus host disease Non alcoholic steatohepatitis Perivenular alcoholic fibrosis Veno occlusive disease (VOD), acute and chronic 20
23 Case Examples Case #1 56 year old woman with pruritus Liver tests: AST 56 ALT 87 Alkaline phosphatase 456 Total bilirubin 0.8 Normal albumin, globulin Biopsy performed and showed the following features Case #1 Portal fibrosis with bridging 21


 Case")

24 Case #1 Prominent portal plasma cell infiltrates Case #1 Interlobular bile ducts with cytologic atypia and focal infiltration by lymphocytes ( Nonsuppurative cholangitis ) Case #1 Interlobular bile duct with cytologic atypia and surrounding lymphocytes, histiocytes and plasma cells 22
 Prominent surrounding")

25 Case #1 Interlobular bile duct with focal infiltration by lymphocytes ( Nonsuppurative cholangitis ) Prominent surrounding plasma cells Case #1 Interlobular bile duct with focal infiltration by lymphocytes ( Nonsuppurative cholangitis ) Case #1 Mallory bodies 23
 Table 7: \"Bile Ducts: Inflammation by Lymphocytes Mallory bodies in")
 that appear to recur more often within the tables (in this example the diseases listed three or more times are underlined) List")
26 Case #1 Epithelioid granulomas Case #1 Summary of liver pathology: Portal fibrosis with bridging Table 5: "Portal Fibrosis, Cirrhosis Portal lymphocytes with increased numbers of plasma cells Tbl Table 3: "Portal Plasma Cll Cells Lymphocytes surrounding and invading interlobular bile ducts (nonsuppurative cholangitis) Table 7: "Bile Ducts: Inflammation by Lymphocytes Mallory bodies in periportal hepatocytes Table 15: "Mallory Bodies Portal and lobular granuloma formation Table 14: Granulomas Case #1 Briefly review all five tables, with the diseases in italics the more frequent diseases showing that feature Highlight g the diseases (>underline) that appear to recur more often within the tables (in this example the diseases listed three or more times are underlined) List these diseases in order of frequency for differential diagnoses 24
27 Table 5 Portal Fibrosis, Cirrhosis Alcoholic cirrhosis Metabolic diseases (e.g., Glycogen Alcoholic hepatitis storage disease III, Gaucher disease) Alpha 1 antitrypsin deficiency Non alcoholic steatohepatitis Autoimmune hepatitis (cholangitis) * Paucity of ducts syndrome, nonsyndromatic* Autoimmune hepatitis Biliary atresia, extrahepatic * Primary biliary cirrhosis * Cystic fibrosis * Primary sclerosing cholangitis * Extrahepatic bile duct obstruction, Progressive familial intrahepatic late stage * cholestasis (Byler syndrome)* Erythropoietic protoporphyria Sarcoidosis Hereditary hemochromatosis Syphilis, tertiary (hepar lobatum) Idiopathic adulthood ductopenia * Veno occlusive disease (VOD), Hepatic venous outflow obstruction chronic (Budd Chiari syndrome), chronic Venous congestion secondary to Hyperalimentation (TPN) right sided heart failure, chronic Indian childhood cirrhosis Viral hepatitis, chronic Inflammatory bowel disease: Wilson disease Ulcerative colitis (* Biliary type Cardiac type) Table 5 Portal Fibrosis, Cirrhosis Alcoholic cirrhosis Metabolic diseases (e.g., Glycogen Alcoholic hepatitis storage disease III, Gaucher disease) Alpha 1 antitrypsin deficiency >Non alcoholic steatohepatitis Autoimmune hepatitis (cholangitis) * Paucity of ducts syndrome, nonsyndromatic* >Autoimmune hepatitis Biliary atresia, extrahepatic * >Primary biliary cirrhosis * Cystic fibrosis * >Primary sclerosing cholangitis * Extrahepatic bile duct obstruction, Progressive familial intrahepatic late stage * cholestasis (Byler syndrome)* Erythropoietic protoporphyria >Sarcoidosis Hereditary hemochromatosis Syphilis, tertiary (hepar lobatum) Idiopathic adulthood ductopenia * Veno occlusive disease (VOD), Hepatic venous outflow obstruction chronic (Budd Chiari syndrome), chronic Venous congestion secondary to Hyperalimentation (TPN) right sided heart failure, chronic Indian childhood cirrhosis Viral hepatitis, chronic Inflammatory bowel disease: >Wilson disease Ulcerative colitis (* Biliary type Cardiac type) Table 3 Portal Plasma Cells Acute viral hepatitis, HAV Allograft, acute (cellular) rejection Autoimmune hepatitis Chronic granulomatous disease of childhood Chronic viral hepatitis, HBV Chronic viral hepatitis (other than HBV) Echinococcosis (hydatid cyst) Epstein Barr virus Hodgkin s lymphoma (nontumor liver) Leishmaniasis Multiple myeloma Primary biliary cirrhosis Primary sclerosing cholangitis Q fever Visceral larva migrans Waldenstrom s macroglobulinemia Wilson disease 25
28 Table 3 Portal Plasma Cells Acute viral hepatitis, HAV Allograft, acute (cellular) rejection >Autoimmune hepatitis Chronic granulomatous disease of childhood Chronic viral hepatitis, HBV Chronic viral hepatitis (other than HBV) Echinococcosis (hydatid cyst) >Epstein Barr virus Hodgkin s lymphoma (nontumor liver) Leishmaniasis Multiple myeloma >Primary biliary cirrhosis >Primary sclerosing cholangitis Q fever Visceral larva migrans Waldenstrom s macroglobulinemia >Wilson disease Table 7 Bile Ducts: Inflammation by Lymphocytes (Nonsuppurative Cholangitis) Acute viral hepatitis, HCV, HEV Allograft, acute (cellular) rejection Autoimmune hepatitis (cholangitis) Caroli disease (biliary cyst walls) Chronic viral hepatitis, HCV Cryptosporidiosis Cytomegalovirus Epstein Barr virus Graft versus host disease Hodgkin s lymphoma (non tumor liver) Human immunodeficiency virus (HIV) associated cholangiopathy) Idiopathic adulthood ductopenia Paucity of ducts syndrome, syndromatic (Alagille s) Primary biliary cirrhosis Primary sclerosing cholangitis (also large ducts) Recurrent pyogenic cholangiohepatitis (large ducts only) Sarcoidosis Table 7 Bile Ducts: Inflammation by Lymphocytes (Nonsuppurative Cholangitis) Acute viral hepatitis, HCV, HEV Allograft, acute (cellular) rejection >Autoimmune hepatitis (cholangitis) Caroli disease (biliary cyst walls) Chronic viral hepatitis, HCV Cryptosporidiosis Cytomegalovirus >Epstein Barr virus Graft versus host disease Hodgkin s lymphoma (non tumor liver) Human immunodeficiency virus (HIV) associated cholangiopathy) Idiopathic adulthood ductopenia Paucity of ducts syndrome, syndromatic (Alagille s) >Primary biliary cirrhosis >Primary sclerosing cholangitis (also large ducts) Recurrent pyogenic cholangiohepatitis (large ducts only) >Sarcoidosis 26
29 Abetalipoproteinemia Alcoholic hepatitis Alpha 1 antitrypsin deficiency Biliary atresia, extrahepatic Extrahepatic bile duct obstruction, mid/late stage Focal nodular hyperplasia Glycogen storage disease Ia Hepatocellular carcinoma, common patterns Hyperalimentation (TPN), adults Table 15 Mallory Bodies Indian childhood cirrhosis Kwashiorkor Liver cell adenoma Non alcoholic steatohepatitis Perivenular alcoholic fibrosis Primary biliary cirrhosis Primary sclerosing cholangitis Weber Christian disease Wilson disease Abetalipoproteinemia Alcoholic hepatitis Alpha 1 antitrypsin deficiency Biliary atresia, extrahepatic Extrahepatic bile duct obstruction, mid/late stage Focal nodular hyperplasia Glycogen storage disease Ia Hepatocellular carcinoma, common patterns Hyperalimentation (TPN), adults Table 15 Mallory Bodies Indian childhood cirrhosis Kwashiorkor Liver cell adenoma >Non alcoholic steatohepatitis Perivenular alcoholic fibrosis >Primary biliary cirrhosis >Primary sclerosing cholangitis Weber Christian disease >Wilson disease Acute alcoholic fatty liver with/without cholestasis Alcoholic fatty liver Alcoholic hepatitis Chronic granulomatous disease of childhood Eosinophilic gastroenteritis Foreign body giant cell reaction Idiopathic granulomatous hepatitis Infectious: Viral (e.g., acute HCV, CMV, EBV) Fungal (e.g., Cryptococcus, Histoplasma) Bacterial (e.g., Salmonella, Brucella) Mycobacterium Parasitic (e.g., Schistosoma, visceral larva migrans) Inflammatory bowel disease: Crohn s disease Table 14 Granulomas Neoplasms, tumor like lesions: Hepatocellular carcinoma Hodgkin s lymphoma (non tumor liver) Inflammatory pseudotumor Langerhans cell histiocytosis Liver cell adenoma Non alcoholic steatohepatitis Nonspecific reactive hepatitis Polyarteritis nodosa Polymyalgia rheumatica Primary biliary cirrhosis Rheumatoid arthritis Sarcoidosis Systemic lupus erythematosus 27
30 Acute alcoholic fatty liver with/without cholestasis Alcoholic fatty liver Alcoholic hepatitis Chronic granulomatous disease of childhood Eosinophilic gastroenteritis Foreign body giant cell reaction Idiopathic granulomatous hepatitis Infectious: >Viral (e.g., acute HCV, CMV, EBV) Fungal (e.g., Cryptococcus, Histoplasma) Bacterial (e.g., Salmonella, Brucella) Mycobacterium Parasitic (e.g., Schistosoma, visceral larva migrans) Inflammatory bowel disease: Crohn s disease Table 14 Granulomas Neoplasms, tumor like lesions: Hepatocellular carcinoma Hodgkin s lymphoma (non tumor liver) Inflammatory pseudotumor Langerhans cell histiocytosis Liver cell adenoma >Non alcoholic steatohepatitis Nonspecific reactive hepatitis Polyarteritis nodosa Polymyalgia rheumatica >Primary biliary cirrhosis Rheumatoid arthritis >Sarcoidosis Systemic lupus erythematosus Case #1 Differential Diagnoses Five of five parameters Primary biliary cirrhosis Four of five parameters Primary sclerosing cholangitis Three of five parameters Autoimmune hepatitis Epstein Barr virus Non alcoholic steatohepatitis Sarcoidosis Wilson disease Two of five parameters Acute (cellular) rejection Acute viral hepatitis, HCV Alpha 1 antitrypsin deficiency Biliary atresia, extrahepatic Cytomegalovirus Extrahepatic bile duct obstruction Hyperalimentation Idiopathic adult ductopenia Indian childhood cirrhosis Paucity of ducts Four of four parameters Primary biliary cirrhosis Primary sclerosing cholangitis Three of four parameters Autoimmune hepatitis Wilson disease Case #1 Differential Diagnoses (if no granulomas were present) Two of four parameters Acute (cellular) rejection Alpha 1 antitrypsin deficiency Biliary atresia, extrahepatic Epstein Barr virus Extrahepatic bile duct obstruction Hyperalimentation Idiopathic adult ductopenia Indian childhood cirrhosis Non alcoholic steatohepatitis Paucity of ducts Sarcoidosis 28
31 Case #1 Additional Information and Final Diagnosis Serologies for viral hepatitis A, B, C: non reactive Autoimmune serologies ANA: weak positive SMA: non reactive AMA M2: positive ERCP: normal Final diagnosis Primary biliary cirrhosis, stage 3 of 4 What about the differential diagnoses in the list that do not fit? For example, in this case we see Mallory bodies, and Epstein Barr Virus (EBV) induced hepatitis, listed under 3 of 5, does not include Mallory bodies. Why is EBV hepatitis still on the list of differentials? Because of the presence of Mallory bodies, cannot EBV infection automatically be excluded? When a liver biopsy representsonly ONEspecific disease, then EBV could certainly be excluded. However, we do not know that, and in fact co existing liver diseases (e.g., EBV in a patient on a medication that can include Mallory bodies such as amiodarone, or EBV in a patient with a chronic biliary tract stricture that can also show Mallory bodies) may be present in this case, hence these other disorders MUST be included and remain on the list of differentials UNTIL clinical and laboratory correlation is provided. It is important to note that it is not infrequent for co existing liver diseases to be present. An example of co existing diseases will be addressed in this session in Case #4. Case #2 32 year old man with non specific clinical features Liver tests: AST 67 ALT 82 Other liver tests normal Hepatitis serologies: HAV IgM, HBsAg, HCV Ab: non reactive Biopsy performed and showed the following features 29





32 Case #2 Portal lymphocytic infiltrates Case #2 Lobular necroinflammatory change with infiltration by lymphocytes Case #2 Sinusoidal lymphocytosis 30
33 Case #2 Granuloma Case #2 Summary of liver pathology: Portal lymphocytic infiltrates Table 1: Portal Lymphocytes Diffuse necroinflammatory change Table 10: Lobular Necrosis with Inflammation Sinusoidal lymphocytosis Table 19: Sinusoids: Circulating Cells Granuloma formation Table 14: Granulomas Allograft, acute (cellular) rejection Alcoholic cirrhosis Autoimmune hepatitis Biliary atresia, extrahepatic Brucellosis Caroli disease Chronic granulomatous disease of childhood >Cytomegalovirus >Epstein Barr virus Erythropoietic protoporphyria Extrahepatic bile duct obstruction, late stage Graft versus host disease Idiopathic adulthood ductopenia Indian childhood cirrhosis >Inflammatory bowel disease Lassa fever Table 1 Portal Lymphocytes Leukemia, lymphocytic Lymphoma, Hodgkin s (non tumor liver) and non Hodgkin s Neonatal hepatitis >Non alcoholic steatohepatitis >Nonspecific reactive hepatitis Porphyria cutanea tarda >Primary biliary cirrhosis Primary sclerosing cholangitis Q fever >Rheumatoid arthritis Rocky Mountain spotted fever Salmonellosis >Sarcoidosis Tuberculosis >Viral hepatitis, acute and chronic Wilson disease Yellow fever Periportal interface inflammation in active stage of disease 31
34 Table 10 Lobular Necrosis with Inflammation Alcoholic hepatitis PMN * Alcoholic foamy degeneration PMN, L * Allograft, acute (cellular) rejection PMN, L * Alpha 1 antitrypsin deficiency L Autoimmune hepatitis L, PC * Benign recurrent intrahepatic cholestasis L ** Biliary atresia, extrahepatic PMN, L ** Caroli disease PMN, L ** Choledochal cyst (with bile duct obstruction) PMN ** Cystic fibrosis PMN * Extrahepatic bile duct obstruction PMN ** Graft versus host disease L Hemochromatosis L Indian childhood cirrhosis PMN, L *Cholestasis in active disease **Cholestasis as a primary factor in the disease L Lymphocytes PMN Neutrophils PC Plasma cells EO Eosinophils Table 10 Lobular Necrosis with Inflammation Infections, non viral Bacterial (pyogenic abscess) PMN * Bacterial (e.g., salmonellosis) PMN Fungal (e.g., cryptococcosis) L Mycobacterium L Parasitic (e.g., Amebiasis) L, EO >Inflammatory bowel disease L Neonatal hepatitis PMN, L * >Non alcoholic steatohepatitis PMN, L >Primary biliary cirrhosis L, PC Primary sclerosing cholangitis L * Recurrent pyogenic cholangiohepatitis PMN ** >Sarcoidosis L * >Viral hepatitis, acute and chronic >Hepatotropic viruses L * >EBV/CMV hepatitis L Wilson disease L * *Cholestasis in active disease **Cholestasis as a primary factor in the disease L Lymphocytes PMN Neutrophils PC Plasma cells EO Eosinophils Table 19 Sinusoids: Circulating Cells >Acute viral hepatitis, HCV L Alcoholic hepatitis PMN Allograft, acute (cellular) L rejection (severe) >Chronic viral hepatitis, HCV L >Cytomegalovirus L >Epstein Barr virus L Leishmaniasis L Leukemia, CLL L Leukemia, CML PMN Lyme disease L, PMN Malaria (tropical L splenomegaly syndrome ) >Nonspecific reactive L hepatitis Pyogenic abscess PMN Reactive changes, PMN bacterial infections >Rheumatoid arthritis L Rocky Mountain L spotted fever Salmonellosis L Surgical hepatitis PMN L Lymphocytes PMN Neutrophils 32
35 Acute alcoholic fatty liver with/without cholestasis Alcoholic fatty liver Alcoholic hepatitis Chronic granulomatous disease of childhood Eosinophilic gastroenteritis Foreign body giant cell reaction Idiopathic granulomatous hepatitis Infectious: >Viral (e.g., acute HCV, CMV, EBV) Fungal (e.g., Cryptococcus, Histoplasma) Bacterial (e.g., Salmonella, Brucella) Mycobacterium Parasitic (e.g., Schistosoma, visceral larva migrans) >Inflammatory bowel disease: Crohn s disease Table 14 Granulomas Neoplasms, tumor like lesions: Hepatocellular carcinoma Hodgkin s lymphoma (non tumor liver) Inflammatory pseudotumor Langerhans cell histiocytosis Liver cell adenoma >Non alcoholic steatohepatitis >Nonspecific reactive hepatitis Polyarteritis nodosa Polymyalgia rheumatica >Primary biliary cirrhosis >Rheumatoid arthritis >Sarcoidosis Systemic lupus erythematosus Four of four parameters Cytomegalovirus Epstein Barr virus infection Case #2 Differential Diagnoses Three of four parameters Acute and chronic hepatitis (HCV ) Inflammatory bowel disease: Crohn s disease Non alcoholic steatohepatitis Non specific reactive hepatitis Primary biliary cirrhosis Rheumatoid arthritis Sarcoidosis Case #2 Additional Information and Final Diagnosis Monospot test: negative EBV specific IgM, EBV associated nuclear Ag (EBNA): negative CMV IgM, CMV DNA (PCR): positive Serologies for viral lhepatitis i A, B, C: non reactive Final diagnosis CMV induced acute hepatitis 33


36 Case #3 39 year old woman with splenomegaly Liver tests: AST 587 ALT 955 Alkaline phosphatase 665 Total bilirubin/direct 3.2/2.9 Total protein/albumin 8.6/3.5 Biopsy performed and showed the following features Case #3 Portal fibrosis with bridging Case #3 Portal lymphocytes with periportal interface inflammatory activity 34

 Case #3 Lobular")

37 Case #3 Portal plasma cell infiltrates Case #3 Portal tract with interlobular bile duct loss (ductopenia) Case #3 Lobular necroinflammatory change with infiltration by lymphocytes and some plasma cells 35
 Portal plasma cells Table 3: Portal Plasma Cells Duct loss (ductopenia) Table 9:")
: Inflammation Alcoholic cirrhosis Alcoholic hepatitis Alpha 1 antitrypsin deficiency Table 5 Portal Fibrosis, Cirrhosis >Autoimmune hepatitis (cholangitis) * Paucity of")
38 Case #3 Lymphocytic inflammation involving terminal hepatic (central) venules (endothelialitis) Case #3 Summary of liver pathology: Portal fibrosis with bridging Table 5: Portal Fibrosis, Cirrhosis Portal lymphocytes with periportal interface inflammation Table 1: Portal Lymphocytes (with Periportal Inflammation) Portal plasma cells Table 3: Portal Plasma Cells Duct loss (ductopenia) Table 9: Bile Ducts: Cytologic Atypia, Duct Loss (Ductopenia) Diffuse lymphocytic necroinflammatory change Table 10: Lobular Necrosis with Inflammation Endothelialitis of terminal hepatic venules Table 20: Vessels (Excluding Sinusoids): Inflammation Alcoholic cirrhosis Alcoholic hepatitis Alpha 1 antitrypsin deficiency Table 5 Portal Fibrosis, Cirrhosis >Autoimmune hepatitis (cholangitis) * Paucity of ducts syndrome, nonsyndromatic* Autoimmune hepatitis Biliary atresia, extrahepatic * >Primary biliary cirrhosis * Cystic fibrosis * >Primary sclerosing cholangitis * Extrahepatic bile duct obstruction, Progressive familial intrahepatic late stage * Erythropoietic protoporphyria Hereditary hemochromatosis Idiopathic adulthood ductopenia * Hepatic venous outflow obstruction (Budd Chiari syndrome), chronic Hyperalimentation (TPN) Indian childhood cirrhosis Inflammatory bowel disease: Ulcerative colitis Metabolic diseases (e.g., Glycogen storage disease III, Gaucher disease) Non alcoholic steatohepatitis cholestasis (Byler syndrome)* >Sarcoidosis Syphilis, tertiary (hepar lobatum) Veno occlusive disease (VOD), chronic Venous congestion secondary to right sided heart failure, chronic >Viral hepatitis, chronic >Wilson disease (* Biliary type Cardiac type) 36
39 Allograft, acute (cellular) rejection Alcoholic cirrhosis >Autoimmune hepatitis Biliary atresia, extrahepatic Brucellosis Caroli disease Chronic granulomatous disease of childhood Cytomegalovirus Epstein Barr virus Erythropoietic protoporphyria Extrahepatic bile duct obstruction, late stage Graft versus host disease Idiopathic adulthood ductopenia Indian childhood cirrhosis Inflammatory bowel disease Lassa fever Table 1 Portal Lymphocytes Leukemia, lymphocytic Lymphoma, Hodgkin s (non tumor liver) and non Hodgkin s Neonatal hepatitis Non alcoholic steatohepatitis Nonspecific reactive hepatitis Porphyria cutanea tarda >Primary biliary cirrhosis >Primary sclerosing cholangitis Q fever Rheumatoid arthritis Rocky Mountain spotted fever Salmonellosis >Sarcoidosis Tuberculosis >Viral hepatitis, acute and chronic >Wilson disease Yellow fever Periportal interface inflammation in active stage of disease Table 3 Portal Plasma Cells Acute viral hepatitis, HAV Allograft, acute (cellular) rejection >Autoimmune hepatitis Chronic granulomatous disease of childhood >Chronic viral hepatitis, HBV Chronic viral hepatitis (other than HBV) Echinococcosis (hydatid cyst) Epstein Barr virus Hodgkin s lymphoma (nontumor liver) Leishmaniasis Multiple myeloma >Primary biliary cirrhosis >Primary sclerosing cholangitis Q fever Visceral larva migrans Waldenstrom s macroglobulinemia >Wilson disease Table 9 Bile Ducts: Cytologic Atypia, Duct Loss (Ductopenia) Allograft, hepatic artery thrombosis Allograft, chronic rejection >Autoimmune hepatitis (cholangitis) Cystic fibrosis Cytomegalovirus, adult Extrahepatic bile duct obstruction, late stage (small ducts) Graft versus host disease Hodgkin s lymphoma (non tumor liver) Human immunodeficiency virus (HIV) associated cholangiopathy) Idiopathic adulthood ductopenia Paucity of ducts syndrome, non syndromatic Paucity of ducts syndrome, syndromatic (Alagille s) Polycystic disease, perinatal (infantile) form >Primary biliary cirrhosis >Primary sclerosing cholangitis (small ducts) Progressive familial intrahepatic cholestasis (Byler syndrome) >Sarcoidosis 37
40 Table 10 Lobular Necrosis with Inflammation Alcoholic hepatitis PMN * Alcoholic foamy degeneration PMN, L * Allograft, acute (cellular) rejection PMN, L * Alpha 1 antitrypsin deficiency L >Autoimmune hepatitis L, PC * Benign recurrent intrahepatic cholestasis L ** Biliary atresia, extrahepatic PMN, L ** Caroli disease PMN, L ** Choledochal cyst (with bile duct obstruction) PMN ** Cystic fibrosis PMN * Extrahepatic bile duct obstruction PMN ** Graft versus host disease L Hemochromatosis L Indian childhood cirrhosis PMN, L *Cholestasis in active disease **Cholestasis as a primary factor in the disease L Lymphocytes PMN Neutrophils PC Plasma cells EO Eosinophils Table 10 Lobular Necrosis with Inflammation Infections, non viral Bacterial (pyogenic abscess) PMN * Bacterial (e.g., salmonellosis) PMN Fungal (e.g., cryptococcosis) L Mycobacterium L Parasitic (e.g., Amebiasis) L, EO Inflammatory bowel disease L Neonatal hepatitis PMN, L * Non alcoholic steatohepatitis PMN, L >Primary biliary cirrhosis L, PC >Primary sclerosing cholangitis L * Recurrent pyogenic cholangiohepatitis PMN ** >Sarcoidosis L * >Viral hepatitis, acute and chronic >Hepatotropic viruses L * EBV/CMV hepatitis L >Wilson disease L * *Cholestasis in active disease **Cholestasis as a primary factor in the disease L Lymphocytes PMN Neutrophils PC Plasma cells EO Eosinophils Table 20 Vessels (Excluding Sinusoids): Inflammation Arteries, arterioles Allograft, acute (cellular) rejection Allograft, hyperacute (humoral) rejection Churg Strauss syndrome Hereditary hemorrhagic telangiectasia (OWR) Polyarteritis nodosa Rheumatoid arthritis Rocky Mountain spotted fever Syphilis, secondary Syphilis, tertiary Systemic lupus erythematosus Toxic shock syndrome Veins, venules Acute viral hepatitis Allograft, acute (cellular) rejection >Autoimmune hepatitis Epstein Barr virus Graft versus host disease Hepatic vein phlebitis Non alcoholic steatohepatitis Perivenular alcoholic fibrosis Pylephlebitis Recurrent pyogenic cholangiohepatitis Salmonellosis >Sarcoidosis Schistosomiasis Syphilis, secondary Toxic shock syndrome 38
41 Case #3 Differential Diagnoses Six of six parameters Autoimmune hepatitis (including cholangitis variant) Five of six parameters Primary biliary cirrhosis Primary sclerosing cholangitis Sarcoidosis Three of six parameters Acute (cellular) rejection Chronic viral hepatitis (other than HBV) Epstein Barr virus Graft vs host Non alcoholic steatohepatitis Four of six parameters Chronic viral hepatitis (HBV) Wilson disease Case #3 Additional Information and Final Diagnosis Autoimmune serologic markers ANA 1:1280, SMA 1:640 Negative AMA M2 Negative atypical anti neutrophilic cytoplasmic Ab (ANCA) Serologies for viral hepatitis A, B, C: non reactive Normal ERCP No pulmonary manifestations Final diagnosis Autoimmune hepatitis with ductopenia ( autoimmune cholangitis ) Case # 4 56 year old diabetic woman Liver tests: AST 145 ALT 189 Alkaline phosphatase 289 Biopsy performed and showed the following features 39
 Case # 4 Portal lymphocytic infiltrates with periportal interface")
42 Case # 4 Portal and periportal sinusoidal fibrosis (trichrome) Case # 4 Perivenular (pericentral) sinusoidal fibrosis (trichrome) Case # 4 Portal lymphocytic infiltrates with periportal interface activity 40
 Case # 4 Fatty change with mild predominantly lymphocytic infiltrates Focal liver cell ballooning")


43 Case # 4 Moderate (2+ to 3+) macrovesicular fatty change Rare glycogenated nuclei of hepatocytes (arrows, left) Case # 4 Fatty change with mild predominantly lymphocytic infiltrates Focal liver cell ballooning (arrow, right) Case # 4 Summary of liver pathology Portal fibrosis Table 5: Portal Fibrosis, Cirrhosis Sinusoidal collagen deposition Table 18: Sinusoids: Fibrosis Portal lymphocytes with periportal activity Table 1: Portal Lymphocytes (with Periportal Inflammation) Fatty change (>50% hepatocytes involved), macrovesicular Table 13: Fatty Change Lobular necrosis and lymphocytic inflammation Table 10: Lobular Necrosis with Inflammation 41
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Slide 7 demonstrates acute pericholangitisis with neutrophils around proliferating bile ducts.
 Many of the histologic images and the tables are from MacSween s Pathology of the Liver (5 th Edition). Other images were used from an online source called PathPedia.com. A few images from other sources
Many of the histologic images and the tables are from MacSween s Pathology of the Liver (5 th Edition). Other images were used from an online source called PathPedia.com. A few images from other sources
PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES I HAVE NOTHING TO DISCLOSE CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017
 CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Steatosis/Steatohepatitis
 Prepared by Kurt Schaberg Introduction to Medical Liver Steatosis/Steatohepatitis Alcoholic Hepatitis Hepatocyte injury and inflammation resulting from chronic alcohol consumption AST/ALT ratio typically
Prepared by Kurt Schaberg Introduction to Medical Liver Steatosis/Steatohepatitis Alcoholic Hepatitis Hepatocyte injury and inflammation resulting from chronic alcohol consumption AST/ALT ratio typically
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk @robdgol FATTY LIVER DISEASE Brunt
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk @robdgol FATTY LIVER DISEASE Brunt
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acalculous cholecystitis, postoperative, 190 191 Acute cardiac failure, hypoxic liver injury and, in critically ill and postoperative patients,
Note: Page numbers of article titles are in boldface type. A Acalculous cholecystitis, postoperative, 190 191 Acute cardiac failure, hypoxic liver injury and, in critically ill and postoperative patients,
Biliary tract diseases of the liver
 Biliary tract diseases of the liver Digestive Diseases Course Bucharest 2016 Rob Goldin r.goldin@imperial.ac.uk How important are biliary tract diseases? Hepatology 2011 53(5):1608-17 Approximately 16%
Biliary tract diseases of the liver Digestive Diseases Course Bucharest 2016 Rob Goldin r.goldin@imperial.ac.uk How important are biliary tract diseases? Hepatology 2011 53(5):1608-17 Approximately 16%
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Liver Diseases
 2nd Pannonia Congress of pathology Hepato-biliary pathology Autoimmune Liver Diseases Vera Ferlan Marolt Institute of pathology, Medical faculty, University of Ljubljana Slovenia Siofok, Hungary, May 2012
2nd Pannonia Congress of pathology Hepato-biliary pathology Autoimmune Liver Diseases Vera Ferlan Marolt Institute of pathology, Medical faculty, University of Ljubljana Slovenia Siofok, Hungary, May 2012
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Disorders of the Liver and Pancreas
 Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
AMR in Liver Transplantation: Incidence
 AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
Linda Ferrell, MD Distinguished Professor Vice Chair Director of Surgical Pathology Dept of Pathology
 Linda Ferrell, MD Distinguished Professor Vice Chair Director of Surgical Pathology Dept of Pathology Nonalcoholic steatohepatitis and Fatty Liver Disease Liver manifestations of the obesity epidemic Changes
Linda Ferrell, MD Distinguished Professor Vice Chair Director of Surgical Pathology Dept of Pathology Nonalcoholic steatohepatitis and Fatty Liver Disease Liver manifestations of the obesity epidemic Changes
LIVER SPECIALTY CONFERENCE USCAP Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA
 LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
ACP-BSG meeting The liver in systemic inflammatory disorders. Dr Adrian C Bateman Southampton University Hospitals NHS Trust
 ACP-BSG meeting 10.12.09 The liver in systemic inflammatory disorders Dr Adrian C Bateman Southampton University Hospitals NHS Trust Wide range of diseases General inflammatory disorders Connective tissue
ACP-BSG meeting 10.12.09 The liver in systemic inflammatory disorders Dr Adrian C Bateman Southampton University Hospitals NHS Trust Wide range of diseases General inflammatory disorders Connective tissue
78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP)
 Gene Gulati PhD, SH(ASCP)") 78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP) 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600 Chicago,
78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP) 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600 Chicago,
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries
 ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Paul Y. Kwo, MD, FACG, FAASLD 1, Stanley M. Cohen, MD, FACG, FAASLD 2, and Joseph K. Lim, MD, FACG, FAASLD 3 1 Division of Gastroenterology/Hepatology,
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Paul Y. Kwo, MD, FACG, FAASLD 1, Stanley M. Cohen, MD, FACG, FAASLD 2, and Joseph K. Lim, MD, FACG, FAASLD 3 1 Division of Gastroenterology/Hepatology,
Case n 1 ( B 92 / 4208 ) Case n 2 ( B 00 / 8249 ) Case n 3 ( B 98 / 8352 )
 Case n 2 ( B 00 / 8249 ) Case n 3 ( B 98 / 8352 )") Slide Seminar Case n 1 ( B 92 / 4208 ) 16 month-old girl. HBV serology +. Clinic in favour of chronic hepatitis. 4 portal triads! classification limited Viral B chronic hepatitis Mild activity (Fig. 1
Slide Seminar Case n 1 ( B 92 / 4208 ) 16 month-old girl. HBV serology +. Clinic in favour of chronic hepatitis. 4 portal triads! classification limited Viral B chronic hepatitis Mild activity (Fig. 1
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 6 PURPOSE To establish basic understanding of indications and contraindications for transplantation of various organs. POLICY The N.C. Department of Correction, Division of Prisons, Health Services
PAGE 1 of 6 PURPOSE To establish basic understanding of indications and contraindications for transplantation of various organs. POLICY The N.C. Department of Correction, Division of Prisons, Health Services
Viral Hepatitis (I) Luigi Terracciano Department of Pathology University Hospital Basel. Basel,
 Luigi Terracciano Department of Pathology University Hospital Basel. Basel,") Viral Hepatitis (I) Luigi Terracciano Department of Pathology University Hospital Basel Basel, 19. 04. 2016 Definition Hepatitis means inflammation of the liver characterized by a variable combination
Viral Hepatitis (I) Luigi Terracciano Department of Pathology University Hospital Basel Basel, 19. 04. 2016 Definition Hepatitis means inflammation of the liver characterized by a variable combination
JAUNDICE - INVESTIGATION OF PROLONGED NEONATAL JAUNDICE
 Definition Unconjugated hyperbilirubinaemia Conjugated Hyperbilirubinaemia Causes of Neonatal Cholestatsis Flow Chart for Investigation of Neonatal Cholestasis First Line Investigations Second Line Investigations
Definition Unconjugated hyperbilirubinaemia Conjugated Hyperbilirubinaemia Causes of Neonatal Cholestatsis Flow Chart for Investigation of Neonatal Cholestasis First Line Investigations Second Line Investigations
Central role: - Regulating the immune system - Influencing metabolic and endocrine functions
 Spleen Central role: - Regulating the immune system - Influencing metabolic and endocrine functions Anatomy: An encapsulated mass of vascular and lymphatic tissue The largest RES organ 9-11 th ribs 4 impressions
Spleen Central role: - Regulating the immune system - Influencing metabolic and endocrine functions Anatomy: An encapsulated mass of vascular and lymphatic tissue The largest RES organ 9-11 th ribs 4 impressions
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
DR NICKY WIESELTHALER RADIOLOGY CONSULTANT RED CROSS CHILDREN S HOSPITAL
 A CASE BASED APPROACH TO ULTRASOUND IN GIT DR NICKY WIESELTHALER RADIOLOGY CONSULTANT RED CROSS CHILDREN S HOSPITAL Ultrasound= No Radiation!!! 1 CXR= 0.02 msv ( effective dose that calculates dose absorbed)
A CASE BASED APPROACH TO ULTRASOUND IN GIT DR NICKY WIESELTHALER RADIOLOGY CONSULTANT RED CROSS CHILDREN S HOSPITAL Ultrasound= No Radiation!!! 1 CXR= 0.02 msv ( effective dose that calculates dose absorbed)
Special stains in liver pathology
 Current Issues in Surgical Pathology 2014 Special stains in liver pathology Which, why, how Really? Sanjay Kakar, MD University of California, San Francisco Outline Which stains Why the stain is done How
Current Issues in Surgical Pathology 2014 Special stains in liver pathology Which, why, how Really? Sanjay Kakar, MD University of California, San Francisco Outline Which stains Why the stain is done How
How to Approach a Medical Liver Biopsy. 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology. Sarajevo, 6 th -7 th November 2015
 1 A Brief Introduction to the Liver Sessions 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology Sarajevo, 6 th -7 th November 2015 Stefan Hübscher, Institute of Immunology & Immunotherapy,
1 A Brief Introduction to the Liver Sessions 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology Sarajevo, 6 th -7 th November 2015 Stefan Hübscher, Institute of Immunology & Immunotherapy,
Role of Liver Biopsy. Role of Liver Biopsy 9/3/2009. Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging
 Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging for further reference: Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach Neil Theise, MD. Depts of Pathology
Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging for further reference: Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach Neil Theise, MD. Depts of Pathology
Liver Pathology: Cirrhosis, Hepatitis, and Primary Liver Tumors. Update and Diagnostic Problems
 SHORT COURSE Liver Pathology: Cirrhosis, Hepatitis, and Primary Liver Tumors. Update and Diagnostic Problems Linda Ferrell, M.D. Department of Anatomic Pathology, University of California San Francisco,
SHORT COURSE Liver Pathology: Cirrhosis, Hepatitis, and Primary Liver Tumors. Update and Diagnostic Problems Linda Ferrell, M.D. Department of Anatomic Pathology, University of California San Francisco,
Liver National EQA Scheme. Circulation Q Birmingham, March 15 th 2005
 Liver National EQA Scheme Circulation Q Birmingham, March 15 th 2005 Images from circulations Virtualpathology@leeds.ac.uk/uvw View slides from current circulation, Aperio see and navigate whole slide
Liver National EQA Scheme Circulation Q Birmingham, March 15 th 2005 Images from circulations Virtualpathology@leeds.ac.uk/uvw View slides from current circulation, Aperio see and navigate whole slide
Nottingham Patterns of liver fibrosis and their clinical significance
 Nottingham 2006 Patterns of liver fibrosis and their clinical significance Alastair D Burt Professor of Pathology and Dean of Clinical Medicine University of Newcastle upon Tyne Collapse of reticulin
Nottingham 2006 Patterns of liver fibrosis and their clinical significance Alastair D Burt Professor of Pathology and Dean of Clinical Medicine University of Newcastle upon Tyne Collapse of reticulin
Chapter 18 LIVER BILIARY TRACT
 Chapter 18 LIVER & BILIARY TRACT DUCT SYSTEM N O FIBROUS TISSUE PORTAL TRIAD CENTRAL VEIN PATTERNS OF HEPATIC INJURY Degeneration: Balooning, feathery degeneration, fat, pigment Inflammation:
Chapter 18 LIVER & BILIARY TRACT DUCT SYSTEM N O FIBROUS TISSUE PORTAL TRIAD CENTRAL VEIN PATTERNS OF HEPATIC INJURY Degeneration: Balooning, feathery degeneration, fat, pigment Inflammation:
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Evening specialty conference: Liver
 Evening specialty conference: Liver Joseph Misdraji, M.D. Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
Evening specialty conference: Liver Joseph Misdraji, M.D. Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
LIVER DISEASES. Pathology Department, Zhejiang University School of Medicine,
 LIVER DISEASES Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn Viral Hepatitis Cirrhosis of liver Liver cancer Viral Hepatitis DEFINITION Primary hepatic infections
LIVER DISEASES Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn Viral Hepatitis Cirrhosis of liver Liver cancer Viral Hepatitis DEFINITION Primary hepatic infections
Chronic Biliary Disease. Dr Susan Davies & Dr Bill Griffiths
 Chronic Biliary Disease Dr Susan Davies & Dr Bill Griffiths Chronic Biliary Disease Terminology is confusing with pathologists and hepatologists using the same language BUT with different meanings. Chronic
Chronic Biliary Disease Dr Susan Davies & Dr Bill Griffiths Chronic Biliary Disease Terminology is confusing with pathologists and hepatologists using the same language BUT with different meanings. Chronic
Nordic Liver Transplant Registry
 Nordic Liver Transplant Registry Revised version 18. December 2007 Data from almost 4000 patients have now been entered to the NLTR. This represents a unique dataset spanning the years 1984 up until today.
Nordic Liver Transplant Registry Revised version 18. December 2007 Data from almost 4000 patients have now been entered to the NLTR. This represents a unique dataset spanning the years 1984 up until today.
2014 CURRENT ISSUES IN PATHOLOGY
 2014 CURRENT ISSUES IN PATHOLOGY SPECIAL STAINS IN LIVER BIOPSY PATHOLOGY Sanjay Kakar, MD University of California, San Francisco Trichrome stain : (1) Assess degree of fibrosis. H&E stain is not reliable
2014 CURRENT ISSUES IN PATHOLOGY SPECIAL STAINS IN LIVER BIOPSY PATHOLOGY Sanjay Kakar, MD University of California, San Francisco Trichrome stain : (1) Assess degree of fibrosis. H&E stain is not reliable
Key Points: Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective. Jenny Heathcote, MD. University of Toronto
 Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
EVALUATION OF ABNORMAL LIVER TESTS
 EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
Dhanpat Jain Yale University School of Medicine, New Haven, CT
 Dhanpat Jain Yale University School of Medicine, New Haven, CT Case history 15 years old female presented with fatigue. Found to have features suggestive of cirrhosis with esophageal varices, splenomegaly
Dhanpat Jain Yale University School of Medicine, New Haven, CT Case history 15 years old female presented with fatigue. Found to have features suggestive of cirrhosis with esophageal varices, splenomegaly
DILI PATHOLOGY. PHILIP KAYE November 2017 BSG Pathology Winter Meeting
 DILI PATHOLOGY PHILIP KAYE November 2017 BSG Pathology Winter Meeting General Mechanisms Role of Liver Biopsy Outline Kleiner Categories Pathology! Differentials Severity Finally Drugs/Toxins may cause
DILI PATHOLOGY PHILIP KAYE November 2017 BSG Pathology Winter Meeting General Mechanisms Role of Liver Biopsy Outline Kleiner Categories Pathology! Differentials Severity Finally Drugs/Toxins may cause
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Histology. The pathology of the. bile ducts. pancreas. liver. The lecture in summary. Vt-2006
 Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Steatotic liver disease
 Steatotic liver disease Fatty liver disease Prof. Dr. ANNE HOORENS Non-Neoplastic Liver Pathology December 8th 2018 Working Group of Digestive Pathology Belgian Society of Pathology OUTLINE NAFLD = Non-Alcoholic
Steatotic liver disease Fatty liver disease Prof. Dr. ANNE HOORENS Non-Neoplastic Liver Pathology December 8th 2018 Working Group of Digestive Pathology Belgian Society of Pathology OUTLINE NAFLD = Non-Alcoholic
Overall Goals and Objectives for Transplant Hepatology EPAs:
 Overall Goals and Objectives for Transplant Hepatology EPAs: 1. DIAGNOSTIC LIST During the one-year Advanced Pediatric Transplant Hepatology Program, fellows are expected to develop comprehensive skills
Overall Goals and Objectives for Transplant Hepatology EPAs: 1. DIAGNOSTIC LIST During the one-year Advanced Pediatric Transplant Hepatology Program, fellows are expected to develop comprehensive skills
National Liver EQA Scheme. Open meeting, Glasgow March 24th 2004
 National Liver EQA Scheme Open meeting, Glasgow March 24th 2004 Participants meeting SOP8 Case discussion Are we quorate All please sign attendance sheet There were 20 EQA participants and 7 non-members
National Liver EQA Scheme Open meeting, Glasgow March 24th 2004 Participants meeting SOP8 Case discussion Are we quorate All please sign attendance sheet There were 20 EQA participants and 7 non-members
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
British Liver Transplant Group Pathology meeting September Leeds cases
 British Liver Transplant Group Pathology meeting September 2014 Leeds cases Leeds Case 1 Male 61 years Liver transplant for HCV cirrhosis with HCC in January 2014. Now raised ALT and bilirubin,? acute
British Liver Transplant Group Pathology meeting September 2014 Leeds cases Leeds Case 1 Male 61 years Liver transplant for HCV cirrhosis with HCC in January 2014. Now raised ALT and bilirubin,? acute
Plan. Sarcoidosis 21/07/2017. Sarcoidosis Liver involvement. Sarcoidosis GI involvement. Sarcoidosis Diagnosis
 Belfast Pathology 2017 Gastrointestinal tract involvement by systemic disease 21.6.17 Dr Adrian C. Bateman University Hospital Southampton NHS Foundation Trust, UK Plan Dermatological conditions Chronic
Belfast Pathology 2017 Gastrointestinal tract involvement by systemic disease 21.6.17 Dr Adrian C. Bateman University Hospital Southampton NHS Foundation Trust, UK Plan Dermatological conditions Chronic
Interpretation of Biopsy Findings in the Transplant Liver
 Interpretation of Biopsy Findings in the Transplant Liver Kirk D. Jones, MD and Linda D. Ferrell, MD W i several thousand liver transplants being performed each year and many patients being managed in
Interpretation of Biopsy Findings in the Transplant Liver Kirk D. Jones, MD and Linda D. Ferrell, MD W i several thousand liver transplants being performed each year and many patients being managed in
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
PBC and PSC: Back to Basics
 Disclosure No financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in this presentation. PBC and PSC: Back to Basics
Disclosure No financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in this presentation. PBC and PSC: Back to Basics
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids. Cholestasis
 Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Extrahepatic Biliary Obstruction. Ductal Diseases: Stones Tumors. Acute Injury: Viral Hepatitis Toxin (APAP/Etoh) Reye s Shock.
 Reye s Shock.") Extrahepatic Biliary Obstruction Stones Tumors Ductal Diseases: Ductal Diseases: Primary Biliary Primary Biliary Cirrhosis Cirrhosis Sclerosing Cholangitis Sclerosing Cholangitis Acute Injury: Viral Hepatitis
Extrahepatic Biliary Obstruction Stones Tumors Ductal Diseases: Ductal Diseases: Primary Biliary Primary Biliary Cirrhosis Cirrhosis Sclerosing Cholangitis Sclerosing Cholangitis Acute Injury: Viral Hepatitis
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Resident, PGY1 David Geffen School of Medicine at UCLA. Los Angeles Society of Pathology Resident and Fellow Symposium 2013
 Resident, PGY1 David Geffen School of Medicine at UCLA Los Angeles Society of Pathology Resident and Fellow Symposium 2013 85 year old female with past medical history including paroxysmal atrial fibrillation,
Resident, PGY1 David Geffen School of Medicine at UCLA Los Angeles Society of Pathology Resident and Fellow Symposium 2013 85 year old female with past medical history including paroxysmal atrial fibrillation,
I have no disclosures relevant to this presentation LIVER TESTS: WHAT IS INCLUDED? LIVER TESTS: HOW TO UTILIZE THEM OBJECTIVES
 LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
Internal Medicine End of Rotation
 Internal Medicine End of Rotation EXAM TOPIC LIST CARDIOVASCULAR Angina pectoris Cardiac arrhythmias/conduction disorders Cardiomyopathy Congestive heart failure Coronary vascular disease Endocarditis
Internal Medicine End of Rotation EXAM TOPIC LIST CARDIOVASCULAR Angina pectoris Cardiac arrhythmias/conduction disorders Cardiomyopathy Congestive heart failure Coronary vascular disease Endocarditis
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases Harrison s Principles of Internal Medicine 18-19 Ed. 2012 e seguenti Chronic hepatitis classification by cause
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases Harrison s Principles of Internal Medicine 18-19 Ed. 2012 e seguenti Chronic hepatitis classification by cause
REGISTRATION FORMS THE NORDIC LIVER TRANSPLANT REGISTRY 18-JAN-2017 ACCEPTANCE. Basic
 FORM A ACCEPTANCE Basic Scandia number: Surname: Person number: First name: Weight: kg Height: cm Events (at any time up to acceptance): Encephalopathy Variceal bleeding Ascites (1: Grade 1/ 2: Grade 2/
FORM A ACCEPTANCE Basic Scandia number: Surname: Person number: First name: Weight: kg Height: cm Events (at any time up to acceptance): Encephalopathy Variceal bleeding Ascites (1: Grade 1/ 2: Grade 2/
Non-Cirrhotic Portal Hypertension and Incomplete Septal Cirrhosis. Stefan Hübscher, University of Birmingham, Birmingham B15 2TT, U.K.
 Non-Cirrhotic Portal Hypertension and Incomplete Septal Cirrhosis Stefan Hübscher, University of Birmingham, Birmingham B15 2TT, U.K. Non-Cirrhotic Portal Hypertension Problems with Liver Biopsy Diagnosis
Non-Cirrhotic Portal Hypertension and Incomplete Septal Cirrhosis Stefan Hübscher, University of Birmingham, Birmingham B15 2TT, U.K. Non-Cirrhotic Portal Hypertension Problems with Liver Biopsy Diagnosis
Liver Cancer Causes, Risk Factors, and Prevention
 Liver Cancer Causes, Risk Factors, and Prevention Risk Factors A risk factor is anything that affects your chance of getting a disease such as cancer. Learn more about the risk factors for liver cancer.
Liver Cancer Causes, Risk Factors, and Prevention Risk Factors A risk factor is anything that affects your chance of getting a disease such as cancer. Learn more about the risk factors for liver cancer.
Circulation T. Manchester July 5 th 2006
 Circulation T Manchester July 5 th 2006 Case 242 8 year old female with polycystic disease Section from explanted liver. Case 242 Case 242 Case 242 Case 242 Case 242 Case 242 31 Congenital hepatic fibrosis
Circulation T Manchester July 5 th 2006 Case 242 8 year old female with polycystic disease Section from explanted liver. Case 242 Case 242 Case 242 Case 242 Case 242 Case 242 31 Congenital hepatic fibrosis
Autoimmune Hepatitis: Histopathology
 REVIEW Autoimmune Hepatitis: Histopathology Stephen A. Geller M.D.*, Autoimmune hepatitis (AIH), a chronic hepatic necroinflammatory disorder, occurs mostly in women. AIH is characterized by prominent
REVIEW Autoimmune Hepatitis: Histopathology Stephen A. Geller M.D.*, Autoimmune hepatitis (AIH), a chronic hepatic necroinflammatory disorder, occurs mostly in women. AIH is characterized by prominent
Liver, Pancreas and Gall Bladder Pathology
 Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Alpha-fetoprotein
 Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
-sheet 3. -Waseem Alhaj. Maha Shomaf
 -sheet 3 -Basheer egbaria -Waseem Alhaj Maha Shomaf 1 P a g e Viral hepatitis have many types each type is associated with different outcomes complication, some can result in acute one,others result in
-sheet 3 -Basheer egbaria -Waseem Alhaj Maha Shomaf 1 P a g e Viral hepatitis have many types each type is associated with different outcomes complication, some can result in acute one,others result in
Liver Pathology Symposium - medical livers
 Liver Pathology Symposium - medical livers London, April 13 th 2018 Dr Susan E Davies, Addenbrooke s Hospital, Case 1 SED 65/F Diabetic. Raised ALT, USS fatty. Fibroscan? cirrhosis Reticulin (untoned),
Liver Pathology Symposium - medical livers London, April 13 th 2018 Dr Susan E Davies, Addenbrooke s Hospital, Case 1 SED 65/F Diabetic. Raised ALT, USS fatty. Fibroscan? cirrhosis Reticulin (untoned),
ACCME/Disclosures. The Overlap Syndromes: Do They Exist? Key Points and Questions 4/6/2016. Hans Popper Hepatopathology Society
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
AAIM: GI Workshop Follow Up to Case Studies. Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease
 AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
Alpha-fetoprotein
 Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
IN THE NAME OF GOD. D r. MANIJE DEZFULI AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL INFECTIOUS DISEASES SPECIALIST
 IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract. Shannon Martinson, March 2017
 Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Alpha-fetoprotein
 Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Other Names/Abbreviations AFP 190.25 - Alpha-fetoprotein Alpha-fetoprotein (AFP) is a polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring the response of certain
Acute Hepatitis: An Approach to Infectious and Other Causes. Mary Anne Cooper MSc, MD, MEd, FRCPC
 : An Approach to Infectious and Other Causes Mary Anne Cooper MSc, MD, MEd, FRCPC Faculty: Dr. Mary Anne Cooper Relationships with commercial interests: Consulting Fees: Lupin Pharmaceuticals, Canada Objectives
: An Approach to Infectious and Other Causes Mary Anne Cooper MSc, MD, MEd, FRCPC Faculty: Dr. Mary Anne Cooper Relationships with commercial interests: Consulting Fees: Lupin Pharmaceuticals, Canada Objectives
Approach to a case of Neonatal Cholestasis
 Approach to a case of Neonatal Cholestasis Ira Shah (Co-Incharge, Consultant Pediatrician, Pediatric Liver Clinic) Gunjan Narkhede (Resident in Pediatric Liver Clinic) Pediatric Hepatobiliary Clinic, B.J.Wadia
Approach to a case of Neonatal Cholestasis Ira Shah (Co-Incharge, Consultant Pediatrician, Pediatric Liver Clinic) Gunjan Narkhede (Resident in Pediatric Liver Clinic) Pediatric Hepatobiliary Clinic, B.J.Wadia
Supplemental Tables. Parasitic Schistosomiasis increase < 1. Genetic Hemochromatosis increase < 1. autoimmune Autoimmune hepatitis (AIH) increase < 1
 increase < 1") Supplemental Tables Supplemental Table 1 Various etiologies of liver cirrhosis and their association with liver stiffness and AST/ALT ratio Disease category Cause Example LS AST/ALT Inflammatory liver
Supplemental Tables Supplemental Table 1 Various etiologies of liver cirrhosis and their association with liver stiffness and AST/ALT ratio Disease category Cause Example LS AST/ALT Inflammatory liver
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
EVALUATION & LISTING. Your Child s Liver Transplant Evaluation. What is the Liver?
 EVALUATION & LISTING Your Child s Liver Transplant Evaluation The University of Michigan is a national leader in liver transplantation, as well as the surgical and medical management of patients with liver
EVALUATION & LISTING Your Child s Liver Transplant Evaluation The University of Michigan is a national leader in liver transplantation, as well as the surgical and medical management of patients with liver
Acute Hepatitis in a Patient with NASH and Elevation of CMV-IgM
 Acute Hepatitis in a Patient with NASH and Elevation of CMV-IgM Uta Drebber, MD Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the
Acute Hepatitis in a Patient with NASH and Elevation of CMV-IgM Uta Drebber, MD Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Special stains in liver pathology
 Current Issues in Surgical Pathology 2014 Special stains in liver pathology Which, why, how Really? Sanjay Kakar, MD University of California, San Francisco Outline Which stains Why the stain is done How
Current Issues in Surgical Pathology 2014 Special stains in liver pathology Which, why, how Really? Sanjay Kakar, MD University of California, San Francisco Outline Which stains Why the stain is done How
What s new in liver transplantation? Romil Saxena, MD, FRCPath (UK) Indiana University School of Medicine, Indianapolis
 Indiana University School of Medicine, Indianapolis") What s new in liver transplantation? Romil Saxena, MD, FRCPath (UK) Indiana University School of Medicine, Indianapolis A combination of improved surgical techniques, donor organ preservation, selection
What s new in liver transplantation? Romil Saxena, MD, FRCPath (UK) Indiana University School of Medicine, Indianapolis A combination of improved surgical techniques, donor organ preservation, selection
Malignant Focal Liver Lesions
 Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Hepatitis A Hepatitis D Hepatitis E HSV CMV EBV
 Ammar Hassan PGY-4 Hepatotropic Viruses Nominal Viruses Hepatitis A Hepatitis D Hepatitis E HSV CMV EBV HEPATITIS A *Non-enveloped, single-stranded RNA virus. *Only one known serotype. *The primary route
Ammar Hassan PGY-4 Hepatotropic Viruses Nominal Viruses Hepatitis A Hepatitis D Hepatitis E HSV CMV EBV HEPATITIS A *Non-enveloped, single-stranded RNA virus. *Only one known serotype. *The primary route
Autoimmune hepatitis
 Autoimmune hepatitis: Autoimmune hepatitis a spectrum within a spectrum Alastair Burt Professor of Pathology and Dean of Clinical Medicine Newcastle University Spectrum of autoimmune liver disease Autoimmune
Autoimmune hepatitis: Autoimmune hepatitis a spectrum within a spectrum Alastair Burt Professor of Pathology and Dean of Clinical Medicine Newcastle University Spectrum of autoimmune liver disease Autoimmune
PATHOLOGY OF LIVER & BILIARY TRACT. Lecture 5. Idiopathic & proliferative conditions; diseases of the biliary tract
 PATHOLOGY OF LIVER & BILIARY TRACT Lecture 5 Idiopathic & proliferative conditions; diseases of the biliary tract Enrique Aburto Winter 2015 IX. Diseases of uncertain origin Equine serum hepatitis Idiopathic
PATHOLOGY OF LIVER & BILIARY TRACT Lecture 5 Idiopathic & proliferative conditions; diseases of the biliary tract Enrique Aburto Winter 2015 IX. Diseases of uncertain origin Equine serum hepatitis Idiopathic
FUO or FKO? Andrew Beany May 2017 Bnai Zion MC, Haifa
 FUO or FKO? Andrew Beany May 2017 Bnai Zion MC, Haifa M. G. 19 yo female Obesity Fever 6 months Weight loss Weakness Dry cough Diffuse non-specific (abdominal) pain November 2016 August 2016 Work-up in
FUO or FKO? Andrew Beany May 2017 Bnai Zion MC, Haifa M. G. 19 yo female Obesity Fever 6 months Weight loss Weakness Dry cough Diffuse non-specific (abdominal) pain November 2016 August 2016 Work-up in
Acute and Chronic Hepatitis John Hart, M.D. University of Chicago Medical Center
 Acute and Chronic Hepatitis John Hart, M.D. University of Chicago Medical Center Acute Hepatitis Clinical Features Classically acute hepatitis is defined clinically as a significant (at least 2X elevation
Acute and Chronic Hepatitis John Hart, M.D. University of Chicago Medical Center Acute Hepatitis Clinical Features Classically acute hepatitis is defined clinically as a significant (at least 2X elevation
Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland
 Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland Sanjiv Chopra, MD, MACP Professor of Medicine Harvard Medical School Editor In Chief Hepatology Section Up To Date Serum
Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland Sanjiv Chopra, MD, MACP Professor of Medicine Harvard Medical School Editor In Chief Hepatology Section Up To Date Serum
Non-reproductive tissues and cells Recommending authority/ association
 Colour key Minimum requirements as set out in Directive 2004/23/EC More stringent - legy binding More stringent - recommended Not legy binding and not recommended Tested pathogen Donor test/ technique
Colour key Minimum requirements as set out in Directive 2004/23/EC More stringent - legy binding More stringent - recommended Not legy binding and not recommended Tested pathogen Donor test/ technique
Vasculitides in Surgical Neuropathology Practice
 Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Fibrosis & Structural Decline of Liver Allografts: what and how to measure & potential underlying causes. Carla Venturi Monteagudo MD, PhD
 Fibrosis & Structural Decline of Liver Allografts: what and how to measure & potential underlying causes Carla Venturi Monteagudo MD, PhD THE NORMAL LIVER ARCHITECTURE Parenchymal Cells -Hepatocytes -Cholangiocytes
Fibrosis & Structural Decline of Liver Allografts: what and how to measure & potential underlying causes Carla Venturi Monteagudo MD, PhD THE NORMAL LIVER ARCHITECTURE Parenchymal Cells -Hepatocytes -Cholangiocytes
Drug therapy in patient with hepatic impairment
 Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
A Systematic Approach to Medical Liver Disease
 A Systematic Approach to Medical Liver Disease Laura W. Lamps, M.D. Godfrey D. Stobbe Professor and Director of Gastrointestinal Pathology University of Michigan Health System Ann Arbor, MI Why do people
A Systematic Approach to Medical Liver Disease Laura W. Lamps, M.D. Godfrey D. Stobbe Professor and Director of Gastrointestinal Pathology University of Michigan Health System Ann Arbor, MI Why do people
Mesenchymal Tumors. Cavernous Hemangioma (CH) VASCULAR TUMORS MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE)
 VASCULAR TUMORS MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE)") Mesenchymal Tumors MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE) CURRENT ISSUES IN ANATOMIC PATHOLOGY MAY 23, 2014 Linda Ferrell, MD, UCSF Focus on Vascular Tumors Benign and
Mesenchymal Tumors MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE) CURRENT ISSUES IN ANATOMIC PATHOLOGY MAY 23, 2014 Linda Ferrell, MD, UCSF Focus on Vascular Tumors Benign and