ACUTE VARICEAL BLEEDING MULTIMODAL APPROACH
|
|
|
- Adele Rose
- 5 years ago
- Views:
Transcription

1 FALK symposium. Liver Cirrhosis: from pathophysiology to disease management Dresden, October ACUTE VARICEAL BLEEDING MULTIMODAL APPROACH Professor Andrew K Burroughs Hepato-biliary biliary-pancreatic and Liver Transplantation Unit Royal Free Hospital
2
3


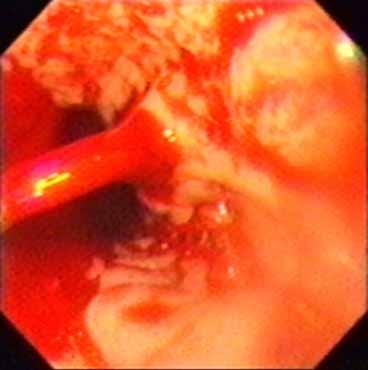
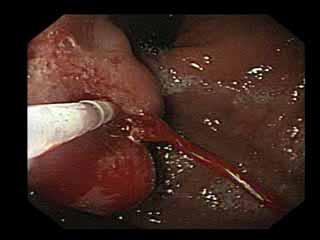
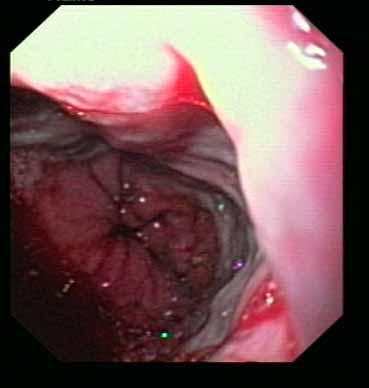
4 White nipple sign varix varix Platelet/fibrin plug Platelet/fibrin plug
5 Prognostic significance of the white nipple sign (Siringo 1989) Prospective study: white nipple no white nipple admissions active bleeding at endoscopy 39% 44% failure to control bleeding 24 hours 11% 24% cumulative at 5 days 39% 49%
6 Diagnosis of upper GI bleeding in cirrhosis Endoscopy as soon as resuscitation adequate It is a high risk endoscopy - adequate support staff (suction) - assess risk of aspiration - pulse oximetry - nasal oxygen - will need endotracheal intubation/ga in several cases Look at fundus, other lesions NB 50% DGH do not have an adequately supported on call system
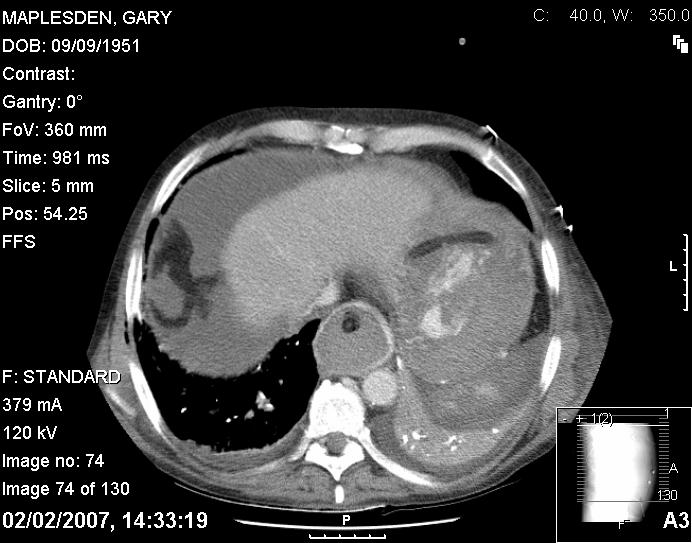
7 Rapid imaging in UGI bleeding in cirrhosis Establish patency portal vein Look for hepatocellular carcinoma Use ultrasound/ doppler
8 MORTALITY FROM VARICEAL BLEEDING McCormick et al 2001
9 Mortality from variceal bleeding in a single centre (Carbonell 2004) Child Pugh A/B Child Pugh C
10 PROSPECTIVE STUDY OF UPPER GI BLEEDING IN CIRRHOTICS (D Amico 2003) cirrhotics patients 5 day failure Rebleed 5d varices % 4.8% P=0.03 Non-variceal 114 7% 1.8% Deaths 5d 9.2% P= % Rebleed 6w 19% P= % Deaths 6 w 20.8% P= %
11 Acute variceal bleeding Factors associated with failure to control bleeding severity of liver disease (many authors) active bleeding at endoscopy (Ben Ari 1999) portal pressure (Ready 1991, Moitinho 1999) infection (Bernard 1995, Goulis 1998)? haemostasis (? independent of severity of liver disease)
12 PREDICTIVE MODEL for FAILURE to CONTROL ACUTE VARICEAL BLEEDING (BenAri 1999) Continued bleeding 24h / early rebleeding 5 days 385 patients vasoactive drugs sclerotherapy if failure MV analysis: failure to control bleeding 30 days mortality * active bleeding at endoscopy PSE urea (log) bleeding started at hospital haematemesis platelets failure to control bleeding PSE urea (log) bleeding started at hospital pulse PT (log) bilirubin Irrespective of interval from admission * Interaction with Child-Pugh, transfusion need, bleeding in hospital and transfusion need, active bleeding and transfusion need
13 PREDICTIVE MODEL for FAILURE to CONTROL ACUTE VARICEAL BLEEDING (BenAri 1999) Time to failure (hrs) < No failure Number failed to control bleeding % death 30 days 24 % 12 % 21 % 33 % 50 % 6 %


14 Portal Pressure and Variceal Bleeding (Moitinho 1999) Outcome according to HPVG at admission 20 mmhg < 20 mmhg
15 HVPG PREDICTION of 5 DAY FAILURE in ACUTE VARICEAL BLEEDING (Albraldes 2006) 117 patients HVPG measured 48 h ( 4 centres) 18 (15%) failure at 5 days (vasoactive drugs,endoscopic therapy, antibiotics) HVPG 20 mmhg OR 5.2 ( ) Systolic BP 100mmHg OR 3.6 ( ) Non-alcoholic cirrhosis OR 4.0 ( ) c statistic 0.79 HVPG 20 mmhg strongly related to CP (p=0.0002) Child A 33% Child B 57% Child C 84% Without HVPG c statistic 0.8
16 HVPG PREDICTION of 5 DAY FAILURE in ACUTE VARICEAL BLEEDING (Albraldes 2006) Allocation points score % failure Systolic B 100 mm Hg points 8 % Systolic B > 100 mm Hg 0 Non-alcoholic cirrhosis 1 Alcoholic cirrhosis 0 Child B points 39 % Child C 2 p =
17 HVPG and SEVERITY of CIRRHOSIS and SIZE of VARICES (Wadhawan 2006) HVPG mmhg ± ±6.9 19± ± ± ± ±6.2 0 Child A Child B Child C small large bleeders non-bleeders
18 Volume change and HVPG in human cirrhosis 12 cirrhotics 600 ml venesected 600 ml restituted Vlavianos 1999
19 Do you obtain blood cultures routinely in known cirrhotic patients, or those suspected of being so, if presenting with upper GI bleeding? Yes No
20 Frequency of bacterial infection in cirrhosis prospective study (Borzio 2001) In hospital mortality 15% v 7% non infected % fever GI bld jaund asc PSE HCC others admission to hospital
21 ACUTE VARICEAL BLEEDING - PROPHYLACTIC ANTIBIOTICS AND BACTERIAL INFECTIONS
22 ACUTE VARICEAL BLEEDING PROPHYLACTIC ANTIBIOTICS AND MORTALITY
23 Complications of portal hypertension Sepsis Bacterial translocation Renal failure Liver failure
24 RANDOMIZED TRIALS of PROPHYLACTIC vs ON DEMAND ANTIBIOTICS for ACUTE VARICEAL BLEEDING Grade C 22.5% Grade C c. 20% iv ofloxacin 200mg qds 2d iv cefotaxime 1gr tds 7d po ofloxacin 200mg bd 5d Frequency of infection on demand prophylaxis % patients % 15.5% 5 0 Hou 2004 Jun 2006 no evidence infection 3.4% 3.2% consecutive admissions
25 EARLY REBLEEDING in RANDOMIZED TRIALS of PROPHYLACTIC vs ON DEMAND ANTIBIOTICS Frequency of bleeding on demand prophylaxis days 6 weeks Hou2004 Jun.2006 Hou2004 Jun.2006
26 QUINOLONES vs CEPHALOSPORINS in the MANAGEMENT of UPPER GI BLEEDING in CIRRHOSIS Included 33% ASC/PSE/shock/ascites Included 9% 2 of PSE/Bil 3mg+/ severe malnutrition Infections: during hospitalization 10 days % infections quinolones 46 patients 65% varices 24% grade C ceftriaxone±quinolones severe infections total infections quinolones Fernandez 2006 Sabat 1998 Antibiotics given: all<6 hours at 6.8±2.9 hours 111 patients 69% varices 53% grade C ceftriaxone
27 QUINOLONES VERSUS CEPHALOSPORINS FOR MANAGEMENT OF UPPER GI BLEEDING IN CIRRHOSIS Failure to control bleeding < 5 days <24 hours failure to control bleeding ceftriaxone±quinolones quinolones quinolones ceftriaxone Sabat 1998 Fernandez 2006
28 WHICH ANTIBIOTIC FOR PROPHYLAXIS IN UPPER GI BLEEDING IN CIRRHOSIS? IV 3 rd generation cephalosporins Start at admission before endoscopy Active against quinolone resistant bacteria gram negative bacteria non enterococcal streptococci No issue of poor absorption due to bleeding, pseudo-ileus etc. Many cirrhotics receive quinolone prophylaxis Will treat infections already present 20% culture positive at admission 50% of infections in cirrhotics are culture negative
29 MORTALITY and ADRENAL INSUFFICIENCY in CIRRHOTIC PATIENTS with SEPSIS Fernandez 2006 Septic shock (n=25) Hydrocortisone 50 mg qds improved survival compared to historical controls (64% vs 32%, p=0.003) Tsai 2006 Critically ill/severe sepsis (n=101) Adrenal insufficiency in 51.5% - associated with: increased mortality 81% vs 37% bacteraemia
30 FREQUENCY of ADRENAL INSUFFICIENCY in CIRRHOTIC PATIENTS with SEPSIS % Adrenal insufficiency Critically ill/sepsis n= 101 (Tsai 2006) Septic shock n= 25 (Fernandez 2006) % Total < CP 11 > Tsai Total B CP C Fernandez
31 Transfusion Airway Kidneys Electrolytes BAVENO III TAKE CARE IN OGV Coagulation Alcohol withdrawal Resuscitation Encephalopathy Infection Nutrition Oxygen Gastric Varices
32 Treatment strategies used in acute variceal bleeding: randomised trials Vasoactive drugs (±( tamponade) ) v. vasoactive drugs (±( tamponade) ) + sclerotherapy Vasoactive drugs v. sclerotherapy Vasoactive drugs + therapeutic endoscopy v. therapeutic endoscopy Sclerotherapy v. ligation Recombinant factor VII + therapeutic endoscopy v. placebo + therapeutic endoscopy
33 VASOACTIVE DRUGS IN ACUTE VARICEAL BLEEDING ( Cochrane reviews) Patients Studies Mortality 95% CI Early rebleeding failure initial haemostasis Transfusion need Terlipressin (Ioannou 2002) ( ) 0.88) Somatostatin analogues ( Gotzche 2001) ( ) 0.61( ) 1.09) 0.68( ) 0.92) Reduction of 1 unit blood
34 RANDOMISED TRIAL OF SOMATOSTATIN SCHEDULES FOR ACUTE VARICEAL BLEEDING (Moitinho( 2001) Bolus 250µg g 250µgX3 250µgX3 infusion 250µg/hr 250µg/hr 500µg/hr Active bleeding at endoscopy Control bleeding+ 58% 61% 82%* Early rebleeding 25% 15% 15% 6week mortality 33% 26% 7% + assessed at 48hrs *p=0.13 p=0.05 Endoscopic therapy if failure of drug therapy
35 RCT 250 vs 500 mg somatostatin for acute variceal bleeding with sclerotherapy (Palazon 2006) Sclerotherapy and 5 days ST: Patients Initial haemostasis Early rebleeding Early rebleeding Child B or C 6 week mortality 250 mg 29 90% 35% 39% 24% 500 mg 33 85% 15% 13% 15%
36 Early administration of Terlipressin and GTN for GI bleeding in cirrhotics (Levacher 1995) double blind:12hrs placebo terlipressin/gtn /GTN episodes persistent bleeding 28% 17% rebleeding 26% 12% mortality 4% 2% blood:units/patient/hr control of bleeding: all 47% 71%* control of bleeding: varices 42% 78%º 1-2mg T/10mg/24h GTN *p< %: 72%º p=0.017
37 Do you use sclerotherapy at diagnostic endoscopy if oesophageal varices are diagnosed as the source of bleeding? Yes No
38 Acute variceal bleeding Drugs vs sclerotherapy Failure to control bleeding (all papers)
39 Acute variceal bleeding Drugs vs sclerotherapy Mortality
40 Acute variceal bleeding Endotherapy + drugs vs endotherapy Failure to control bleeding
41 Acute variceal bleeding Endotherapy + drugs vs endotherapy Mortality
42 RCT OCTREOTIDE + SCLEROTHERAPY vs SCLEROTHERAPY (Morales 2007) 48 hours octreotide Patients 7 day mortality Rebleeding Mean units transfused ITU support Scl 28 18% 21% % Scl+oct 40 20% 20% %
43 If you see actively bleeding oesophageal varices at diagnostic endoscopy, do you remove the scope and (a) arrange for immediate endotracheal intubation? Yes No (b) attach a ligating device, and pass the scope again and ligate varices? Yes No (c) place balloon tamponade and consider referral? Yes No
44 ACUTE VARICEAL BLEEDING LIGATION vs SCLEROTHERAPY FAILURE to CONTROL BLEEDING
45 ACUTE VARICEAL BLEEDING LIGATION vs SCLEROTHERAPY - MORTALITY
46 RCT LIGATION vs SCLEROTHERAPY (Villaneuva 2006) SOM + SCL SOM + EVL Patients Failure 5 days 24 % * p= % * Child C Failure 5 days 33 % NS 25 % Active bleeding Failure 5 days 24 % NS 18 % Deaths at 5 days 3 % NS 3 % Deaths at 6 weeks 21 % NS 13% * amongst failures 50% died compared to 11 % successes * * HVPG > 16 mm Hg associated with failure
47 Control of variceal bleeding with emergency sclerotherapy (Triantos 2005) % median % 83% 69% 95% 5 trials trials trials trials 1309 S+d v.drugs v. drugs v. S+drugs v. ligation* * At the end of endoscopy
48 ACUTE VARICEAL BLEEDING RCT OF rviia (Bosch 2004) 10/119 6/120 10/116 9/116 variceal bleeders variceal bleeders placebo rfviia placebo rfviia Failure to control acute bleeding (within 24h) Failure to prevent rebleeding (24h - day 5)
49 ACTIVE VARICEAL BLEEDING in CHILD B and C CHIRRHOSIS DOUBLE BLIND PLACEBO CONTROLLED TRIAL of rf.viia Bosch doses <24h Placebo 600mg rfviia 300mg rfviia Patients Failure to control bleeding 8% 9% 8% Failure to prevent rebleeding (24h to 5d) 8% 4% 4% Mortality 5d 13% 12% 5% Mortality 42d 29% 15% 31%

50
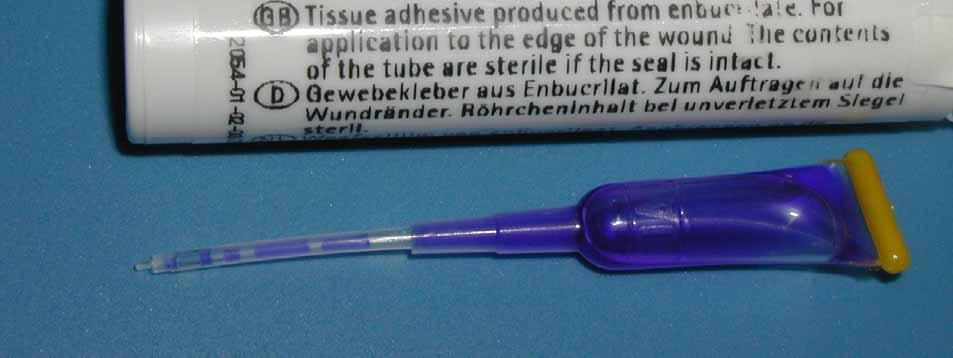
51 Histoacryl glue Flush biopsy channel with lipiodol Mix 1ml glue with 1-2mls 1 lipiodol Flush sclerotherapy needle with saline Wear glasses/goggles Plentiful supply of needles Preparation Consent?
52 RCT standard endoscopic therapy vs glues Haemostasis: no. 114 Thakeb Feretis Zimmer Sung % scl scl + hist acryl 56 scl scl + hist acryl lig cyano acryl
53 RCT standard endoscopic therapy vs glues rebleeding: no. 114 Thakeb Feretis Zimmer Sung % scl 25 scl + hist acryl scl glue lig cyano acryl
54 RCT standard endoscopic therapy vs glues mortality: Thakeb no Feretis Zimmer Sung % scl 4 scl + hist acryl 9 scl 14 glue 28 lig cyano acryl
55 Acutely bleeding Gastric Varices High early rebleeding with sclerotherapy and ligation (Jansen 1995, Tan 2006) Glues effective (Hou Hou 1998, Sarin 2002, Greenwald 2003, Milson 2003, Tan 2006 ) TIPS effective (Chau 90% control Chau 1998, Barange 1999, Azoulay 2001)
56
57 RCT BAND LIGATION vs N BUTYL-2 CYANOACRYLATE (Tan 2006) gastric varices ligation glue Patients Active bleeding controlled 14 of of 15 Rebleeding 44% p< % + Cumulative rebleeding 72% p< % at 3 years + use of ligation was independently associated with rebleeding

58
59 RCT TIPS vs CYANOACRYLATE INJECTION for PREVENTION of GASTRIC REBLEEDING (Lo 2007) Patients Rebleeding TIPS (43%) GLUE (59%) Rebleeding gastric varices Survival 4 (11%) same 14 (38%)

60 Sengstaken Blakemore Bridge TIPS Liver Transplant
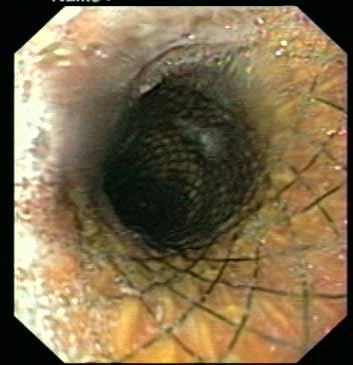
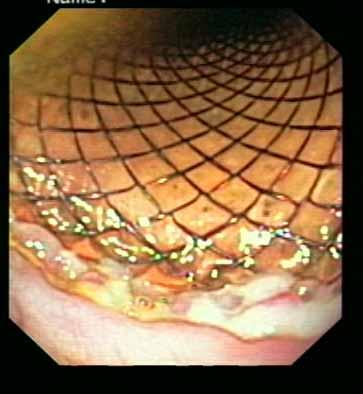
61 SELF-EXPANDING METAL STENTS TO TREAT ACUTE BLEEDING FROM OESOPHAGEAL VARICES (Hubmann 2006) 15 from 143 patients (+5 referred) new type of stent (Ella-Denis) in % successful deployment radiological screening 100% haemostasis 100% successful endoscopic removal between 2-14 days 20% migration into stomach-endoscopic adjustment no local complications
62 The correct positioning is ensured by a balloon at the end of the set.

63 Course

64
65 When sclerotherapy or ligation with vasoactive drugs have failed, do you (a) use tissue adhesives? Yes No (b) refer for TIPS? Yes No

66
67 DEFINITION of UNCONTROLLED VARICEAL HAEMORRHAGE at RFH Continued/early variceal rebleeding (within 5 days) despite 2 sessions of therapeutic endoscopy Continued variceal bleeding despite correctly placed balloon tamponade Continued/early gastric or ectopic variceal bleeding despite vasoconstrictor therapy
68 Emergency salvage TIPS for variceal bleeding (Chau 1998) varices oesophageal gastric fundal patients (%Child s C) 84 (75%) 28 (60%) early rebleeding <7 days 11 4 varices 3 (3.5%) 1 (6%) oesophageal ulcer 4 1 PHG 1 1 not identified 3 1 mortality 31 (37%) 12 (43%)
69 Emergency TIPS series: immediate control of bleeding no c.bleed % LaBerge 93 Hang 93 Rubin 95 Jalan 95 Jabour 96 Sanayal 96 Perarnau 97 Banares 98 Gerbes 98 Chau 98 Barange 99 Bizollon 01 Azoulay 01
70 Emergency TIPS series: mortality no mortal. % Hang 93 Helton 93 Jalan 95 Jabour 96 Sanayal 96 Perarnau 97 Banares 98 Gerbes 98 Chau 98 Barange 99 Bizollon 01 Azoulay 01
71 RCT OF EARLY TIPS IN ACUTE VARICEAL BLEEDERS WITH HVPG 20 mmhg (Monescillo 2004) HVPG 20 mmhg ( 24 hr) Patients Non TIPS 26 TIPS 26 Treatment failure 50% 0 12% Transfusion (units) Mortality at 6 weeks 38% 17% o 77% of these (n=10) within 48 hours of admission 38% (n=5) could not receive 2 nd sclerotherapy or TIPS. Predictive accuracy for treatment failure of 20 mmhg - 77% - ROC curve HVPG , Pugh s

72 TIPS technique

73 TIPS technique

74 TIPS technique
75

76 Colonic Varices


77 TIPS FOR PORTAL VEIN THROMBOSIS AT RFH Senzolo et al 2005


78 TIPS FOR PORTAL VEIN THROMBOSIS AT RFH Senzolo et al 2005
79 TIPS FOR PORTAL VEIN THROMBOSIS AT RFH Senzolo et al patients portal vein thrombosis - 12 with cirrhosis Total Complete PVT Cavernoma Successful 65% 61% 62% Complications Mechanical thrombectomy 53% * Variceal bleeding in 14, pre OLT 3, Budd Chiari 2, Ascites 5, portal biliopathy 2
80 BLEEDING FROM ECTOPIC VARICES TREATMENT WITH TIPS AND EMBOLISATION (Vangeli 2004) Ectopic variceal bleeding 5% cause of bleeding in cirrhotics Endoscopic treatment is ineffective (especially for rectal varices) Patients Total TIPS 19* Rebleeding Further successful embolisation TIPS alone 12 42% (48h) 80% TIPS + Embolisation 6 28% 100% * 2 technical failure

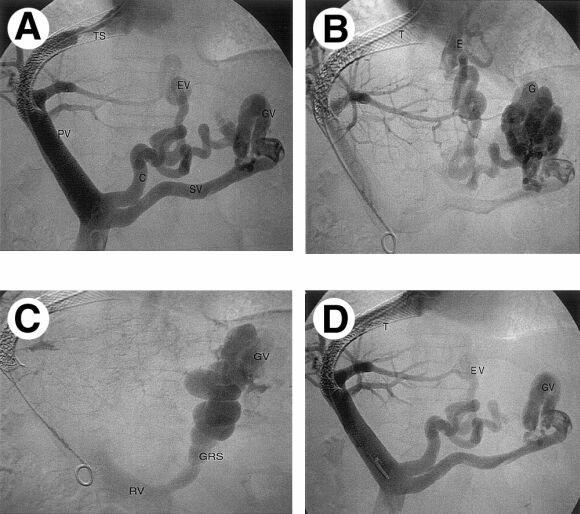
81 RETROGRADE BALLOON OCCLUSION of GASTRIC VARICES
82 POTENTIAL AREAS of CLINICAL STUDY in ACUTE VARICEAL BLEEDING Prophylactic antibiotics given at admission not after diagnosis High risk of failure to control bleeding - glue as first line therapy - TIPS as first line therapy Assess risks of double intubation - diagnostic endoscopy and then ligation Routine endotracheal intubation in high risk patients - aspiration pneumonia Steroids in infected patients
83 ACUTE VARICEAL BLEEDING BAVENO CONSENSUS IV (2005) blood restitution to 8g/dL prophylactic antibiotic mandatory endoscopy within 12 hours vasoactive drugs before diagnostic endoscopy - maintained 2-5 days - no preference indicated - combined with endoscopic therapy ligation preferred, sclerotherapy not excluded tissue adesive for gastric varices failures use TIPS (covered stents) ATLANTA CONSENSUS (2006)
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
TIPS. D Patch Royal Free Hospital London UK
 TIPS D Patch Royal Free Hospital London UK TIPS Technique Ascites Budd Chiari Variceal Bleeding Historical Experimental Development 1967 Piccone Shunt between recanalized umbilical vein and saphenous
TIPS D Patch Royal Free Hospital London UK TIPS Technique Ascites Budd Chiari Variceal Bleeding Historical Experimental Development 1967 Piccone Shunt between recanalized umbilical vein and saphenous
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
th Annual AISF Meeting 44 th th th, 2011 Rome, February 23 rd -26
 44 th 44 th Annual AISF Meeting Rome, February 23 rd -26 th th, 2011 Update on the Baveno Consensus Conference Roberto de Franchis Department of of Clinical Sciences, University of of Milan, Head, Gastroenterology
44 th 44 th Annual AISF Meeting Rome, February 23 rd -26 th th, 2011 Update on the Baveno Consensus Conference Roberto de Franchis Department of of Clinical Sciences, University of of Milan, Head, Gastroenterology
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Portogram shows opacification of gastroesophageal varices.
 Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France
 Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Blood and guts.. Haemodynamics / resuscitation. Haemodynamics / resuscitation. Blood and guts. Dr Jonathan Hoare
 Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Review Article Self-Expandable Metal Stents in the Treatment of Acute Esophageal Variceal Bleeding
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2011, Article ID 910986, 6 pages doi:10.1155/2011/910986 Review Article Self-Expandable Metal Stents in the Treatment of Acute
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2011, Article ID 910986, 6 pages doi:10.1155/2011/910986 Review Article Self-Expandable Metal Stents in the Treatment of Acute
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Variceal bleeding. Mainz,
 Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation
 Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation Siwaporn Chainuvati, MD Faculty of Medicine Siriraj Hospital Outline Natural history of esophageal varices Which
Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation Siwaporn Chainuvati, MD Faculty of Medicine Siriraj Hospital Outline Natural history of esophageal varices Which
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Manejo Actual del Sangrado por Varices Gástricas
 Manejo Actual del Sangrado por Varices Gástricas Juan Carlos Garcia-Pagán Barcelona Hepatic Hemodynamic Laboratory. Liver Unit. IMDIM. Hospital Clinic. IDIBAPS. Ciberehd. XXIV Congreso de la Asociación
Manejo Actual del Sangrado por Varices Gástricas Juan Carlos Garcia-Pagán Barcelona Hepatic Hemodynamic Laboratory. Liver Unit. IMDIM. Hospital Clinic. IDIBAPS. Ciberehd. XXIV Congreso de la Asociación
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12:
 Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
V ariceal haemorrhage is a major cause of mortality and
 270 LIVER DISEASE The role of the transjugular intrahepatic portosystemic stent shunt (TIPSS) in the management of bleeding gastric : clinical and haemodynamic correlations D Tripathi, G Therapondos, E
270 LIVER DISEASE The role of the transjugular intrahepatic portosystemic stent shunt (TIPSS) in the management of bleeding gastric : clinical and haemodynamic correlations D Tripathi, G Therapondos, E
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
Gastrointestinal bleeding is one of the most important
 Prospective Validation of Baveno V Definitions and Criteria for Failure to Control Bleeding in Portal Hypertension Sun Young Ahn, 1 Soo Young Park, 1 Won Young Tak, 1 Yu Rim Lee, 1 Eun Jeong Kang, 1 Jung
Prospective Validation of Baveno V Definitions and Criteria for Failure to Control Bleeding in Portal Hypertension Sun Young Ahn, 1 Soo Young Park, 1 Won Young Tak, 1 Yu Rim Lee, 1 Eun Jeong Kang, 1 Jung
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Picking up their Pieces: Emergency Management of GI Bleeds
 Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Endovascular Techniques for Symptomatic Portal Hypertension. Michael Meuse, M.D. Vascular and Interventional Radiology
 Endovascular Techniques for Symptomatic Portal Hypertension Michael Meuse, M.D. Vascular and Interventional Radiology Objectives Review indications and contraindications for TIPS Define a treatment algorithm
Endovascular Techniques for Symptomatic Portal Hypertension Michael Meuse, M.D. Vascular and Interventional Radiology Objectives Review indications and contraindications for TIPS Define a treatment algorithm
CLINICAL LIVER, PANCREAS, AND BILIARY TRACT
 GASTROENTEROLOGY 2003;124:1277 1291 CLINICAL LIVER, PANCREAS, AN BILIARY TRACT Emergency Sclerotherapy Versus Vasoactive rugs for Variceal Bleeding in Cirrhosis: A Cochrane Meta-Analysis GENNARO AMICO,*
GASTROENTEROLOGY 2003;124:1277 1291 CLINICAL LIVER, PANCREAS, AN BILIARY TRACT Emergency Sclerotherapy Versus Vasoactive rugs for Variceal Bleeding in Cirrhosis: A Cochrane Meta-Analysis GENNARO AMICO,*
Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine -
 Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Treatment of portal hypertension in the light of the Baveno VI Consensus Conference
 r e v I E w A R T I C l e S Curierul medical, December 2015, Vol. 58, No 6 Treatment of portal hypertension in the light of the Baveno VI Consensus Conference E. Tcaciuc Department of Internal Medicine,
r e v I E w A R T I C l e S Curierul medical, December 2015, Vol. 58, No 6 Treatment of portal hypertension in the light of the Baveno VI Consensus Conference E. Tcaciuc Department of Internal Medicine,
Risk factors for 5-day bleeding after endoscopic treatments for gastroesophageal varices in liver cirrhosis
 Original Article Page 1 of 9 Risk factors for 5-day bleeding after endoscopic treatments for gastroesophageal varices in liver cirrhosis Rui Sun*, Xingshun Qi* #, Deli Zou, Xiaodong Shao, Hongyu Li, Xiaozhong
Original Article Page 1 of 9 Risk factors for 5-day bleeding after endoscopic treatments for gastroesophageal varices in liver cirrhosis Rui Sun*, Xingshun Qi* #, Deli Zou, Xiaodong Shao, Hongyu Li, Xiaozhong
PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS
 PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS Dr. J. Fernández. Head of the Liver Unit Hospital Clinic Barcelona, Spain AEEH Postgraduate Course, Madrid, February 15 2017 Prevalence of
PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS Dr. J. Fernández. Head of the Liver Unit Hospital Clinic Barcelona, Spain AEEH Postgraduate Course, Madrid, February 15 2017 Prevalence of
King Abdul-Aziz University Hospital (KAUH) is a tertiary
 is a tertiary") Modelling Factors Causing Mortality in Oesophageal Varices Patients in King Abdul Aziz University Hospital Sami Bahlas Abstract Objectives: The objective of this study is to reach a model defining factors
Modelling Factors Causing Mortality in Oesophageal Varices Patients in King Abdul Aziz University Hospital Sami Bahlas Abstract Objectives: The objective of this study is to reach a model defining factors
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Clinical guideline Published: 13 June 2012 nice.org.uk/guidance/cg141
 Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
ABDOMINAL PAIN (SEE ALSO ABDOMINAL AORTIC ANEURYSM)
") ABDOMINAL PAIN (SEE ALSO ABDOMINAL AORTIC ANEURYSM) Evaluating abdominal pain is difficult misdiagnosis of this symptom generates more formal complaints than any other clinical mistake made in our department.
ABDOMINAL PAIN (SEE ALSO ABDOMINAL AORTIC ANEURYSM) Evaluating abdominal pain is difficult misdiagnosis of this symptom generates more formal complaints than any other clinical mistake made in our department.
Portal hypertension and ascites
 Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Patrick S. Kamath, MD, and David M. Nagorney, MD
 gastrointestinal tract and abdomen PORTAL HYPERTENSION Patrick S. Kamath, MD, and David M. Nagorney, MD Portal hypertension is diagnosed when the hepatic veinpressure gradient (HVPG), which reflects hepatic
gastrointestinal tract and abdomen PORTAL HYPERTENSION Patrick S. Kamath, MD, and David M. Nagorney, MD Portal hypertension is diagnosed when the hepatic veinpressure gradient (HVPG), which reflects hepatic
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
Management of variceal bleeding Rachael Harry, MA, MRCP, and Julia Wendon, FRCP
 Management of variceal bleeding Rachael Harry, MA, MRCP, and Julia Wendon, FRCP Variceal hemorrhage complicates cirrhosis in as many as 50% of patients and results in considerable morbidity and mortality.
Management of variceal bleeding Rachael Harry, MA, MRCP, and Julia Wendon, FRCP Variceal hemorrhage complicates cirrhosis in as many as 50% of patients and results in considerable morbidity and mortality.
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Emergency Medical Retrieval Service (EMRS) Standard Operating Procedure
 Standard Operating Procedure") Emergency Medical Retrieval Service (EMRS) www.emrs.scot.nhs.uk Standard Operating Procedure Title Oesophagogastric Tamponade Tube Version 4 Related Documents SOP-Upper GI Haemorrhage Author G Cowan, C
Emergency Medical Retrieval Service (EMRS) www.emrs.scot.nhs.uk Standard Operating Procedure Title Oesophagogastric Tamponade Tube Version 4 Related Documents SOP-Upper GI Haemorrhage Author G Cowan, C
Cyanoacrylate Glue versus Band Ligation for Acute Gastric Variceal Hemorrhage - A randomized controlled trial at Services Hospital, Lahore
 ORIGINAL ARTICLE Cyanoacrylate Glue versus Band Ligation for Acute Gastric Variceal Hemorrhage - A randomized controlled trial at Services Hospital, Lahore ISMAIL HASSAN 1, ASMA SIDDIQUE 2, MUHAMMAD IBRAR
ORIGINAL ARTICLE Cyanoacrylate Glue versus Band Ligation for Acute Gastric Variceal Hemorrhage - A randomized controlled trial at Services Hospital, Lahore ISMAIL HASSAN 1, ASMA SIDDIQUE 2, MUHAMMAD IBRAR
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Critical care and cirrhosis: outcome and benefit Julia Wendon, William Bernal, Chris Willars and Georg Auzinger
 Critical care and cirrhosis: outcome and benefit Julia Wendon, William Bernal, Chris Willars and Georg Auzinger Institute of Liver Studies, Kings College Hospital, Denmark Hill, London, UK Correspondence
Critical care and cirrhosis: outcome and benefit Julia Wendon, William Bernal, Chris Willars and Georg Auzinger Institute of Liver Studies, Kings College Hospital, Denmark Hill, London, UK Correspondence
Original Article INTRODUCTION. pissn eissn X
 pissn 2287-2728 eissn 2287-285X Original Article Clinical and Molecular Hepatology 2016;22:466-476 Emergency endoscopic variceal ligation in cirrhotic patients with blood clots in the stomach but no active
pissn 2287-2728 eissn 2287-285X Original Article Clinical and Molecular Hepatology 2016;22:466-476 Emergency endoscopic variceal ligation in cirrhotic patients with blood clots in the stomach but no active
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap. Simon McPherson, Vascular Interventional Radiologist, Leeds
 Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Service provision for liver disease in the UK: a national questionnaire-based survey
 PROFESSIONAL ISSUES Clinical Medicine 2012, Vol 12, No 2: 114 8 Service provision for liver disease in the UK: a national questionnaire-based survey R Scott, M Williams, A Lawson, A Austin and J Freeman
PROFESSIONAL ISSUES Clinical Medicine 2012, Vol 12, No 2: 114 8 Service provision for liver disease in the UK: a national questionnaire-based survey R Scott, M Williams, A Lawson, A Austin and J Freeman
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما
 بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
PROGRAMME AT A GLANCE
 PROGRAMME AT A GLANCE Hotel Hyatt Andaz Hotel Pullman Date Hall-H1 Hall-H2 Hall-P1 Hall-P2 Hall-P3 Hall-P4 Hall-P5 Hall-P6 Basic science workshop 1 Basic Science Workshop 2 Postgraduate Course - Liver
PROGRAMME AT A GLANCE Hotel Hyatt Andaz Hotel Pullman Date Hall-H1 Hall-H2 Hall-P1 Hall-P2 Hall-P3 Hall-P4 Hall-P5 Hall-P6 Basic science workshop 1 Basic Science Workshop 2 Postgraduate Course - Liver
Review Article Role of Self-Expandable Metal Stents in Acute Variceal Bleeding
 Hindawi Publishing Corporation International Journal of Hepatology Volume 2012, Article ID 418369, 6 pages doi:10.1155/2012/418369 Review Article Role of Self-Expandable Metal Stents in Acute Variceal
Hindawi Publishing Corporation International Journal of Hepatology Volume 2012, Article ID 418369, 6 pages doi:10.1155/2012/418369 Review Article Role of Self-Expandable Metal Stents in Acute Variceal
CONTROLLED DOCUMENT. Cirrhosis Care Bundle CATEGORY: Clinical Guidelines. CLASSIFICATION: Clinical. Controlled Document CG201 Number:
 Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Thrombocytopenia and Chronic Liver Disease
 Thrombocytopenia and Chronic Liver Disease Severe thrombocytopenia (platelet count
Thrombocytopenia and Chronic Liver Disease Severe thrombocytopenia (platelet count
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
King s College Hospital NHS Foundation Trust. Acute on Chronic Liver Failure: Practical management outside the tertiary centre.
 King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
Terlipressin: An Asset for Hepatologists!
 DIAGNOSTIC AND THERAPEUTIC ADVANCES IN HEPATOLOGY Terlipressin: An Asset for Hepatologists! S.K. Sarin and Praveen Sharma One Case Scenario A 48-year-old male with alcoholic cirrhosis who was abstinent
DIAGNOSTIC AND THERAPEUTIC ADVANCES IN HEPATOLOGY Terlipressin: An Asset for Hepatologists! S.K. Sarin and Praveen Sharma One Case Scenario A 48-year-old male with alcoholic cirrhosis who was abstinent
Practical Approach to Endoscopic Management for Bleeding Gastric Varices
 Review Article http://dx.doi.org/10.3348/kjr.2012.13.s1.s40 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2012;13(S1):S40-S44 Practical Approach to Endoscopic Management for Bleeding Gastric Varices
Review Article http://dx.doi.org/10.3348/kjr.2012.13.s1.s40 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2012;13(S1):S40-S44 Practical Approach to Endoscopic Management for Bleeding Gastric Varices
BRTO /PARTO Indications and outcomes
 BRTO /PARTO Indications and outcomes Saher Sabri, MD Associate Professor of Radiology and Surgery Division of Interventional Radiology University of Virginia Health System Saher Sabri, M.D. Speakers Bureau:
BRTO /PARTO Indications and outcomes Saher Sabri, MD Associate Professor of Radiology and Surgery Division of Interventional Radiology University of Virginia Health System Saher Sabri, M.D. Speakers Bureau:
Gastrointestinal bleeding definitions (I)
") definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Clinical practice guidelines on the management of variceal bleeding
 ecommons@aku Department of Medicine Department of Medicine January 2016 Clinical practice guidelines on the management of variceal bleeding Javed Iqbal Farooqi Hasnain Ali Shah Aga Khan University, hasnain.alishah@aku.edu
ecommons@aku Department of Medicine Department of Medicine January 2016 Clinical practice guidelines on the management of variceal bleeding Javed Iqbal Farooqi Hasnain Ali Shah Aga Khan University, hasnain.alishah@aku.edu
V ariceal bleeding is a serious complication of portal
 431 LIVER Randomised controlled trial of long term portographic follow up versus variceal band ligation following transjugular intrahepatic portosystemic stent shunt for preventing oesophageal variceal
431 LIVER Randomised controlled trial of long term portographic follow up versus variceal band ligation following transjugular intrahepatic portosystemic stent shunt for preventing oesophageal variceal
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
Upper GI Bleeds. AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM
 Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Management of critically-ill cirrhotic patients
 Management of critically-ill cirrhotic patients Pere Ginès 1,2, *, Javier Fernández 1,François Durand 2, Faouzi Saliba 3 1 Liver Unit, IMDiM, Hospital Clinic Barcelona, University of Barcelona and IDIBAPS
Management of critically-ill cirrhotic patients Pere Ginès 1,2, *, Javier Fernández 1,François Durand 2, Faouzi Saliba 3 1 Liver Unit, IMDiM, Hospital Clinic Barcelona, University of Barcelona and IDIBAPS
Tranjugular Intrahepatic Portosystemic Shunt
 Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complication of Portal Hypertension: should the patients in the waiting list be treated differently?
 Wilma Debernardi Venon Gastroepatologia, Az. Osp. San Giovanni Battista ditorino Complication of Portal Hypertension: should the patients in the waiting list be treated differently? Il sottoscritto dichiara
Wilma Debernardi Venon Gastroepatologia, Az. Osp. San Giovanni Battista ditorino Complication of Portal Hypertension: should the patients in the waiting list be treated differently? Il sottoscritto dichiara
TIPS in the Management of Portal Hypertension Clinician s Opinion
 TIPS in the Management of Portal Hypertension Clinician s Opinion Oliviero Riggio 5 th AISF post meeting course Diagnostic and Therapeutic Procedures in Hepatology 2012 Oliviero Riggio Dipartimento di
TIPS in the Management of Portal Hypertension Clinician s Opinion Oliviero Riggio 5 th AISF post meeting course Diagnostic and Therapeutic Procedures in Hepatology 2012 Oliviero Riggio Dipartimento di
Management of Portal Vein Thrombosis With and Without Cirrhosis
 Management of Portal Vein Thrombosis With and Without Cirrhosis Dominique-Charles Valla Service d Hépatologie,Hôpital Beaujon, APHP, Université Paris-Diderot, Inserm CRB3 Extrahepatic Portal Vein Obstruction
Management of Portal Vein Thrombosis With and Without Cirrhosis Dominique-Charles Valla Service d Hépatologie,Hôpital Beaujon, APHP, Université Paris-Diderot, Inserm CRB3 Extrahepatic Portal Vein Obstruction
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Luis S. Marsano, MD March 2013
 Portal HTN: Variceal Bleed, Portal Gastropathy, Hepatopulmonary Syndrome, Porto Pulmonary Hypertension, Cardiomyopathy, and Acute on Chronic Liver Failure Luis S. Marsano, MD March 2013 Variceal Hemorrhage
Portal HTN: Variceal Bleed, Portal Gastropathy, Hepatopulmonary Syndrome, Porto Pulmonary Hypertension, Cardiomyopathy, and Acute on Chronic Liver Failure Luis S. Marsano, MD March 2013 Variceal Hemorrhage
INTRODUCTION. Chung-Hwan Jun, Chang-Hwan Park, Wan-Sik Lee, Young-Eun Joo, Hyun-Soo Kim, Sung-Kyu Choi, Jong-Sun Rew, Sei-Jong Kim, Young-Dae Kim*
 J Korean Med Sci 2006; 21: 883-90 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences Antibiotic Prophylaxis Using Third Generation Cephalosporins Can Reduce the Risk of Early Rebleeding in
J Korean Med Sci 2006; 21: 883-90 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences Antibiotic Prophylaxis Using Third Generation Cephalosporins Can Reduce the Risk of Early Rebleeding in
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Bleeding from Oesophageal Varices,
 HPB Surgery, 1996, Vol. 10, pp. 1-6 Reprints available directly from the publisher Photocopying permitted by license only 1996 OPA (Overseas Publishers Association) (C) Amsterdam B.V. Published in The
HPB Surgery, 1996, Vol. 10, pp. 1-6 Reprints available directly from the publisher Photocopying permitted by license only 1996 OPA (Overseas Publishers Association) (C) Amsterdam B.V. Published in The
Prevention and treatment of variceal haemorrhage in 2017
 Received: 12 October 2016 Accepted: 19 October 2016 DOI: 10.1111/liv.13277 REVIEW ARTICLE Prevention and treatment of variceal haemorrhage in 2017 Felix Brunner 1 Annalisa Berzigotti 1 Jaime Bosch 1,2
Received: 12 October 2016 Accepted: 19 October 2016 DOI: 10.1111/liv.13277 REVIEW ARTICLE Prevention and treatment of variceal haemorrhage in 2017 Felix Brunner 1 Annalisa Berzigotti 1 Jaime Bosch 1,2
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Portal hypertension is the main complication of cirrhosis
 GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
Online Supplement for:
 Online Supplement for: INFLUENCE OF COMBINED INTRAVENOUS AND TOPICAL ANTIBIOTIC PROPHYLAXIS ON THE INCIDENCE OF INFECTIONS, ORGAN DYSFUNCTIONS, AND MORTALITY IN CRITICALLY ILL SURGICAL PATIENTS A PROSPECTIVE,
Online Supplement for: INFLUENCE OF COMBINED INTRAVENOUS AND TOPICAL ANTIBIOTIC PROPHYLAXIS ON THE INCIDENCE OF INFECTIONS, ORGAN DYSFUNCTIONS, AND MORTALITY IN CRITICALLY ILL SURGICAL PATIENTS A PROSPECTIVE,
Risk assessment in UGIB: recent PCI & ACS. Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass
 Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual