PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
|
|
|
- Daisy Walsh
- 5 years ago
- Views:
Transcription

1 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN
2 DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg ( kPa), which is sufficient to maintain a portal flow through the hepatic sinusoids of approximately 1 liter/min.
3 CLASSIFICATION AND CAUSES Presinusoidal Thrombosis of the extrahepatic portal vein or one of its major tributaries extrahepatic Pathologic processes that affect the terminal portal venules in the presinusoidal position intrahepatic Liver function is well preserved Variceal bleeding

4 Sinusoidal caused by cirrhosis, and viral hepatitis and ethanol abuse,autoimmune liver disease, hemochromatosis Hepatocellular damage, destroyed sinusoidal anatomy, regenerative nodules form, fibrosis further obstructs portal venous flow and the normal metabolic processes are disrupted. Evaluate liver function, assess the activity of the underlying liver disease
5 Postsinusoidal Results from hepatic venous outflow obstruction Budd Chiari syndrome. The least common cause of portal hypertension, but may be reversible if identified and treated early
")
6 Etiologies of portal hypertension. These are divided into those associated with normal liver function (presinusoidal) and those associated with liver damage (sinusoidal).

7 SURGICAL ANATOMY Portal venous anatomy in portal hypertension. The superior mesenteric, splenic and inferior mesenteric veins unite behind the neck of the pancreas to form the portal vein. The right and left gastric and gastroepiploic veins enter the portal and superior mesenteric veins

8 PATHOPHYSIOLOGY Stages in the development of portal hypertension.
9 HEMODYNAMIC PATHOPHYSIOLOGIC CHANGES Portal venous pressure increases to 20mmHg or greater, and blood is transmitted back into the whole splanchnic bed. The major sites for collateral pathway development are the natural watersheds for portosystemic collaterals: Gastroesophageal; Hemorrhoidal; Periumbilical; Retroperitoneal. Increased portal venous pressure, dilatation of the splanchnic venous bed and the development of collaterals all act as stimuli for splanchnic hyperemia. The clinical consequences are that a hyperdynamic systemic circulation develops with a high cardiac output and a low total systemic vascular resistance and a low normal blood pressure.
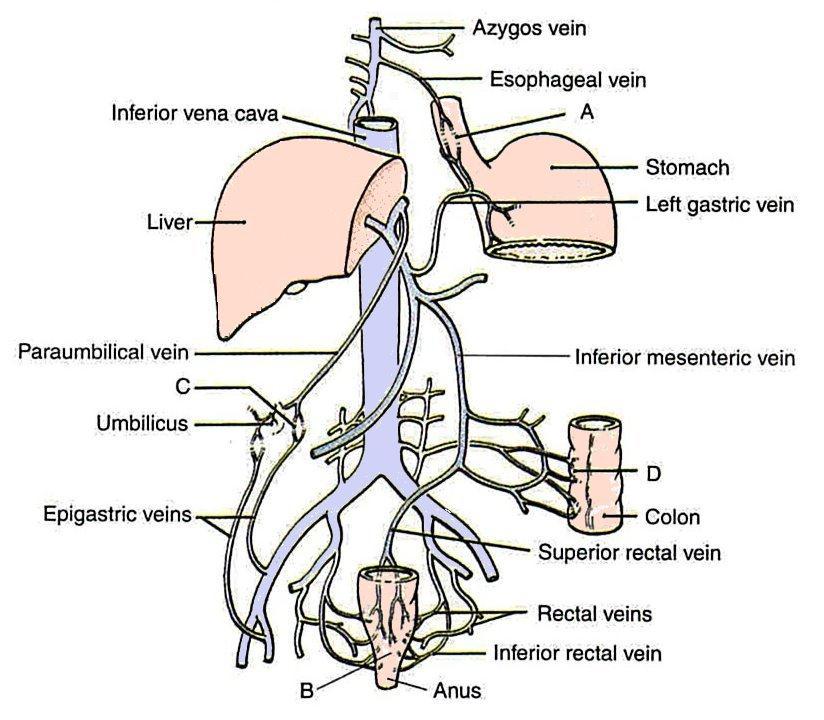
10 Portal-Systemic Anastomosis
11 At the lower third of the esophagus, the esophageal branches of the left gastric vein (portal tributary) anastomose with the esophageal veins draining the middle third of the esophagus into the azygos veins (systemic tributary)
12 Half way down the anal canal, the superior rectal veins (portal tributary) draining the upper half of the anal canal anastomose with the middle and inferior rectal veins (systemic tributaries).
13 The paraumbilical veins connect the left branch of the portal vein with the superficial veins of the anterior abdominal wall (systemic tributaries). The paraumbilical veins travel in the falciform ligament and accompany the ligamentum teres.
14 The veins of the ascending colon, descending colon, duodenum, pancreas, and liver (portal tributaries) anastomose with the renal, lumbar, and phrenic veins (systemic tributaries).

15 CLINICAL PRESENTATION Fig Presenting features of portal hypertension.
16 Classification of the severity of the underlying liver disease at the time of presentation of a patient who has portal hypertension is important. Child s classification has stood the test of time. Child s original classification used the three clinical parameters of ascites, encephalopathy and nutrition plus the two biochemical parameters of bilirubin and albumin with a grading of 1 3 for each. The Child s classification modification most commonly used is that of Pugh, in which nutritional status is replaced by prothrombin time.

17 Child Pugh classification Fig.27-6 Child Pugh classification. The grades are A for 5 6 points, B for7 9 points and C for points.
18 INVESTIGATION HISTORY Exposure to hepatitis, a history of excessive alcohol ingestion or a family history of liver disease are relevant in history taking. Any history of upper gastrointestinal bleeding should be clarified in detail, with particular emphasis on the severity, occurrence of multiple episodes and management modalities used.
19 PHYSICAL EXAMINATION General physical examination should include a visual inspection for muscle wasting, jaundice and spider angiomas, and in males for gynecomastia and testicular atrophy. Abdominal examination focuses on hepatosplenomegaly and ascites, but may also reveal prominent abdominal wall veins. Systemic hemodynamic changes, which are manifested as a mild persistent tachycardia and a low blood pressure.
20 HEMATOLOGY Hematocrit is often reduced, either secondary to chronic bleeding or as a result of the expanded plasma volume; platelet count may be less than /mm 3 and the white cell count less than /mm 3 because of hypersplenism. Prolongation of the prothrombin time and decrease of plasma fibrinogen level indicates moderate liver impairment. The therapeutic implication is an increased risk of bleeding and the need to give fresh frozen plasma to patients who are bleeding or require any interventional procedure.
21 BIOCHEMISTRY Serum electrolytes, blood urea nitrogen and serum creatinine Serum bilirubin, albumin, aminotransferases, alkaline phosphatase and γ-glutamyltranspeptidase. These indices assess the severity and activity of the underlying liver disease
22 SEROLOGY Hepatitis A, B and C serologies should be carried out routinely Antimitochondrial antibody (primary biliary cirrhosis); Antinuclear antibody (for evidence of autoimmune hepatitis); Ceruloplasmin for Wilson s disease; and α 1 -antitrypsin to reveal deficiency.
23 ENDOSCOPY All patients confirmed or suspected of having cirrhosis should have a screening upper gastrointestinal endoscopy. If varices are identified at screening, patients should be started on appropriate prophylactic pharmacologic therapy to reduce the risk of an initial bleed. For a patient who has cirrhosis and has an upper gastrointestinal bleed, endoscopy is the first step in evaluation of the bleeding site and in making decisions on further management. The classification of the severity of varices is based on size, extent and the color signs.
24 RADIOLOGIC IMAGING The initial imaging study is ultrasound with Doppler evaluation of the major vessels. An ultrasound scan of the liver should inspect overall morphology; it is the initial screening procedure for focal intrahepatic lesions that may suggest hepatocellular carcinoma. The vessel imaging focuses on the main portal vein, the splenic vein, the hepatic veins and the infraand intrahepatic inferior vena cava. It identifies most of the extrahepatic causes of portal hypertension. A CT scan or MRI of the abdomen may be indicated for some patients who have portal hypertension to evaluate the liver morphology in greater detail and to image the intra-abdominal venous system.
25

26

27
28

29

30

31
32 ANGIOGRAPHY Fig Venous phase imaging of superior mesenteric artery injection demonstrating the superior mesenteric and portal veins.
33 LIVER BIOPSY Percutaneous biopsy Transjugular biopsy Laparoscopic biopsy

34 Fig Treatment strategies for esophagastric varices. MANAGEMENT OF ESOPHAGOGASTRIC VARICES

35 Fig Time points in the treatment of esophogastric varices.
36 PHARMACOLOGIC THERAPY The patient who has acute variceal bleeding may be treated initially with intra- venous vasopressin and nitroglycerin or somatostatin or one of its analogs. Acute pharmacologic therapy is most easily administered using octreotide infused at 50mg/h. This agent is as effective as vasopressin and nitroglycerin given in combination, has fewer side effects and requires less monitoring. In the elective situation, noncardioselective β- blockers and the long-acting nitrates are the main drugs used to lower portal pressure. Portal pressure could be lowered by about 20% with propranolol (Oral pharmacologic therapy). A similar effect can be obtained with the long-acting nitrates.
37 ENDOSCOPIC THERAPY Endoscopic therapy has a definite role in acute variceal bleeding and is the first-line therapy in preventing rebleeding. The two main techniques are sclerotherapy or variceal banding (1) Sclerotherapy involves the use of one of several agents to directly thrombose a varix or to create fibrosis in the mucosa overlying a varix; (2) In banding the varix is sucked into an applicator on the end of the flexible endoscope and a rubber band is fired to strangulate the varix; the bands slough off in 7 10 days with minimal scarring and less ulceration than with sclerotherapy. Endoscopic banding is more effective, resulting in earlier obliteration of varices and fewer complications than endoscopic sclerotherapy.
38 TAMPONADE This is rarely indicated in the 1990s, but may be needed for the 10% of patients whose acute bleeding is not controlled endoscopically. The Sengstaken Blakemore tube has both gastric and esophageal balloons. The tube must first be fully introduced into the stomach. The gastric balloon should then be inflated to ml and pulled up into the gastric fundus. Occasionally, persistent bleeding may occur in the esophagus, requiring inflation of the esophageal balloon to 40mmHg. The tube should not be left in place for more than hours and should only be used as a temporary measure while the patient is resuscitated and prepared for either repeat endoscopic therapy or decompression.

39 DECOMPRESSION Fig Methods of decompression for portal hypertension and gastroesophageal varices.

40 Fig TIPS. The metallic shunt maintains the transparenchymal track, which has been made through the liver between the portal and hepatic veins.

41 Fig Side-to-side portacaval shunt with direct vein-to-vein anastomosis. The portal vein is dissected from the right side, posterior to the bile duct. The intrahepatic vena cava is fully mobilised. If there is a larger caudate lobe, an interposition graft may be used.

42 Fig Partial portosystemic shunt with an 8mm graft between the portal vein and inferior vena cava. Exposure is the same as for the total portacaval shunt.

43 Fig Distal splenorenal shunt, with anastomosis of the splenic to the left renal vein. The gastric fundus, esophagus and spleen are decompressed. Portal hypertension and prograde portal flow are maintained.
44 DEVASCULARIZATION PROCEDURES These have the components of splenectomy, gastric and esophageal devascularization, and esophageal transection, with the goal of reducing inflow to bleeding varices. Their success depends upon the extent of the devascularization: the more extensive, the lower the subsequent rebleeding rate. Sufficient exposure: easy to perform splenectomy and to immobilize fully both the stomach and at least 7cm of the distal esophagus. pyloroplasty is necessary The upper two-thirds of the lesser curve of the stomach should be devascularized. The whole of the greater curve should be devascularized from the pylorus to the gastroesophageal junction.

45 Fig Gastroesophageal devascularization interrupts all variceal inflow to most of the stomach and the distal 7cm of the esophagus. Splenectomy and desvascularization of the greater curve of the stomach complete the procedure.
46 LIVER TRANSPLANTATION This is part of the surgical repertoire of managing patients who have portal hypertension and variceal bleeding. The indication for transplant remains end-stage liver disease, and for Child s class C patients this treatment has altered the long-term outcome.

47 MANAGEMENT OF VARICEAL BLEEDING AT DEFINED TIME POINTS PROPHYLACTIC THERAPY Pharmacologic therapy to prevent the first bleed has been most widely studied using b-blockers. ACUTE VARICEAL BLEEDING Balloon tamponade Decompression
48 PREVENTION OF RECURRENT VARICEAL BLEEDING The principles for prevention of rebleeding can be summarized as: first-line treatment with pharmacologic and endoscopic therapy; second-line treatment with variceal decompression; and liver transplantation for end-stage liver disease.

49 summary of the management of variceal bleeding Fig Management of variceal bleeding. DSRS, distal splenorenal shunt.
50 MANAGEMENT OF EXTRAHEPATIC PORTAL VEIN THROMBOSIS normal liver function; control bleeding:endoscopic therapy ; decompression; devascularization; splenectomy identify the etiology: angiography is more important
51 ASCITES PATHOGENESIS Ascites results from a combination of: portal hypertension; altered renal sodium and water handling; hypoalbuminemia.
52 MANAGEMENT Ascites is managed primarily by medical therapy If ascites is refractory to medical management, the next line of therapy is paracentesis. Large-volume paracentesis The primary surgical treatment for intractable ascites is liver transplantation because the patient has decompensated liver disease.

53 BUDD CHIARI SYNDROME Fig Causes of the Budd Chiari syndrome.
54 PATHOPHYSIOLOGY The sequence of outflow obstruction, sinusoidal dilatation and congestion, hepatocyte necrosis from the increased pressure and progressive liver damage produce the syndrome. CLINICAL PRESENTATION This is usually subacute with relatively mild symptoms and signs of ascites, hepatomegaly and right upper quadrant abdominal pain.

55 MANAGEMENT Fig Evaluation and management of Budd Chiari syndrome. OLT, orthotopic liver transplantation.

56
Portogram shows opacification of gastroesophageal varices.
 Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Spontaneous portosystemic venous shunts in liver cirrhosis: Anatomy, pathophysiology, hemodynamic changes and imaging findings
 Spontaneous portosystemic venous shunts in liver cirrhosis: Anatomy, pathophysiology, hemodynamic changes and imaging findings Poster No.: C-3193 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular
Spontaneous portosystemic venous shunts in liver cirrhosis: Anatomy, pathophysiology, hemodynamic changes and imaging findings Poster No.: C-3193 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Patrick S. Kamath, MD, and David M. Nagorney, MD
 gastrointestinal tract and abdomen PORTAL HYPERTENSION Patrick S. Kamath, MD, and David M. Nagorney, MD Portal hypertension is diagnosed when the hepatic veinpressure gradient (HVPG), which reflects hepatic
gastrointestinal tract and abdomen PORTAL HYPERTENSION Patrick S. Kamath, MD, and David M. Nagorney, MD Portal hypertension is diagnosed when the hepatic veinpressure gradient (HVPG), which reflects hepatic
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Liver Failure. The most severe clinical consequence of liver disease is liver failure:
 Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Obliterative hepatocavopathy ultrasound and cavography findings
 doi:10.2478/v10019-008-0020-6 case report Obliterative hepatocavopathy ultrasound and cavography findings Ramazan Kutlu Department of Radiology, Inonu University School of Medicine, Malatya, Turkey ackgound.
doi:10.2478/v10019-008-0020-6 case report Obliterative hepatocavopathy ultrasound and cavography findings Ramazan Kutlu Department of Radiology, Inonu University School of Medicine, Malatya, Turkey ackgound.
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما
 بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
Portal hypertension and ascites
 Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Transjugular Intrahepatic
 Transjugular Intrahepatic Portosystemic Shunt (TIPS): A Clinical and Procedural Review Mark R. Werley, M.D. and John Briguglio, M.D. Lancaster Radiology Associates, Ltd. INTRODUCTION This article reviews
Transjugular Intrahepatic Portosystemic Shunt (TIPS): A Clinical and Procedural Review Mark R. Werley, M.D. and John Briguglio, M.D. Lancaster Radiology Associates, Ltd. INTRODUCTION This article reviews
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL
 DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
DISEASE LEVEL MEDICAL EVIDENCE PROTOCOL 1. This Protocol sets out the medical evidence that must be delivered to the Administrator for proof of Disease Level. It is subject to such further and other Protocols
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein
: Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein") Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم **As we remember from the last lecture: The arterial supply which comes from the single branches of the aorta drains in the portal vein (venous drainage of the gut = portal vein).
بسم هللا الرحمن الرحيم **As we remember from the last lecture: The arterial supply which comes from the single branches of the aorta drains in the portal vein (venous drainage of the gut = portal vein).
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
Tranjugular Intrahepatic Portosystemic Shunt
 Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Development of the Liver and Pancreas
 Development of the Liver and Pancreas Professor Alfred Cuschieri Department of Anatomy University of Malta Three glandular buds arise from the distal end of the foregut during the fourth week Day 22 -The
Development of the Liver and Pancreas Professor Alfred Cuschieri Department of Anatomy University of Malta Three glandular buds arise from the distal end of the foregut during the fourth week Day 22 -The
SUMMARY AND CONCLUSION
 - 100 - SUMMARY AND CONCLUSION The problem of portal hypertension and its alarming complications is still attracting the attentions of surgeons and physicians all over the world. Portal hypertension usually
- 100 - SUMMARY AND CONCLUSION The problem of portal hypertension and its alarming complications is still attracting the attentions of surgeons and physicians all over the world. Portal hypertension usually
Thrombocytopenia and Chronic Liver Disease
 Thrombocytopenia and Chronic Liver Disease Severe thrombocytopenia (platelet count
Thrombocytopenia and Chronic Liver Disease Severe thrombocytopenia (platelet count
Central role: - Regulating the immune system - Influencing metabolic and endocrine functions
 Spleen Central role: - Regulating the immune system - Influencing metabolic and endocrine functions Anatomy: An encapsulated mass of vascular and lymphatic tissue The largest RES organ 9-11 th ribs 4 impressions
Spleen Central role: - Regulating the immune system - Influencing metabolic and endocrine functions Anatomy: An encapsulated mass of vascular and lymphatic tissue The largest RES organ 9-11 th ribs 4 impressions
Netter's Anatomy Flash Cards Section 4 List 4 th Edition
 Netter's Anatomy Flash Cards Section 4 List 4 th Edition https://www.memrise.com/course/1577335/ Section 4 Abdomen (31 cards) Plate 4-1 Bony Framework of Abdomen 1.1 Costal cartilages 1.2 Iliac crest 1.3
Netter's Anatomy Flash Cards Section 4 List 4 th Edition https://www.memrise.com/course/1577335/ Section 4 Abdomen (31 cards) Plate 4-1 Bony Framework of Abdomen 1.1 Costal cartilages 1.2 Iliac crest 1.3
Surgical Rescue of Surgical Failures
 HPB Surgery, 1999, Vol. 11, pp. 151-155 Reprints available directly from the publisher Photocopying permitted by license only (C) 1999 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 1999, Vol. 11, pp. 151-155 Reprints available directly from the publisher Photocopying permitted by license only (C) 1999 OPA (Overseas Publishers Association) N.V. Published by license under
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
BY DR NOMAN ULLAH WAZIR
 BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Liver Transplantation
 1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12:
 Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Subject Review. Pathophysiology and Treatment of Variceal Hemorrhage M.D., AND PATRICK S. KAMATH, M.D.
 Subject Review Pathophysiology and Treatment of Variceal Hemorrhage LEWIS R. ROBERTS, M.D., AND PATRICK S. KAMATH, M.D. Portal hypertension results from increases in portal flow and portal vascular resistance.
Subject Review Pathophysiology and Treatment of Variceal Hemorrhage LEWIS R. ROBERTS, M.D., AND PATRICK S. KAMATH, M.D. Portal hypertension results from increases in portal flow and portal vascular resistance.
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011
 Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Job Task Analysis for ARDMS Abdomen Data Collected: June 30, 2011 Reported: Analysis Summary for: Abdomen Examination Survey Dates 06/13/2011-06/26/2011 Invited Respondents 6,000 Surveys with Demographics
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Portal hypertension is the main complication of cirrhosis
 GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Omran Saeed. Mohammad Al-muhtaseb. 1 P a g e
 13 Omran Saeed Mohammad Al-muhtaseb 1 P a g e Posterior abdominal wall - The diaphragm separates between thoracic cavity and abdominal cavity. Structures of posterior abdominal wall: (below diaphragm)
13 Omran Saeed Mohammad Al-muhtaseb 1 P a g e Posterior abdominal wall - The diaphragm separates between thoracic cavity and abdominal cavity. Structures of posterior abdominal wall: (below diaphragm)
Left-sided portal hypertension with a patent splenic vein: An impossible or a not-so-uncommon scenario?
 Khan et al. 108 CASE REPORT PEER REVIEWED OPEN ACCESS Left-sided portal hypertension with a patent splenic vein: An impossible or a not-so-uncommon scenario? Iftikhar Khan, Ghassan Ramahi, Saif Zaabi,
Khan et al. 108 CASE REPORT PEER REVIEWED OPEN ACCESS Left-sided portal hypertension with a patent splenic vein: An impossible or a not-so-uncommon scenario? Iftikhar Khan, Ghassan Ramahi, Saif Zaabi,
INCREASED resistance to blood flow in the liver or portal venous system results
 EFFECTIVE SPONTANEOUS PORTACAVAL VENOUS SHUNT Report of Two Cases B. H. SULLIVAN, JR., M.D., CHARLES H. BROWN, M.D., Department of Gastroenterology THOMAS F. MEANEY, M.D., Division of Radiology and EARL
EFFECTIVE SPONTANEOUS PORTACAVAL VENOUS SHUNT Report of Two Cases B. H. SULLIVAN, JR., M.D., CHARLES H. BROWN, M.D., Department of Gastroenterology THOMAS F. MEANEY, M.D., Division of Radiology and EARL
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 16, 2015
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
Alpha-1 Antitrypsin Deficiency: Liver Disease
 Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Copy Right- Hongqi ZHANG-Department of Anatomy-Fudan University. Systematic Anatomy. Angiology Part 4. Veins. Dr.Hongqi Zhang ( 张红旗 )
") Systematic Anatomy Angiology Part 4 Veins Dr.Hongqi Zhang ( 张红旗 ) Email: zhanghq58@126.com 1 General introduction of the veins Vessel which return the blood back to atrium No pulsation,veneous blood, metabolic
Systematic Anatomy Angiology Part 4 Veins Dr.Hongqi Zhang ( 张红旗 ) Email: zhanghq58@126.com 1 General introduction of the veins Vessel which return the blood back to atrium No pulsation,veneous blood, metabolic
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
CT appearance of collateral pathways in portal hypertension
 CT appearance of collateral pathways in portal hypertension Poster No.: C-0972 Congress: ECR 2011 Type: Educational Exhibit Authors: F. Mihai, C. Bar, M. L. Savin, B. Cucuteanu, D. Negru ; Iasi/ 1 2 2
CT appearance of collateral pathways in portal hypertension Poster No.: C-0972 Congress: ECR 2011 Type: Educational Exhibit Authors: F. Mihai, C. Bar, M. L. Savin, B. Cucuteanu, D. Negru ; Iasi/ 1 2 2
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
1 Right & left Hepatic ducts Gastric Impression of spleen
 Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
DR. DO NGUYEN TIN CHILDREN HOSPITAL 1
 DR. DO NGUYEN TIN CHILDREN HOSPITAL 1 BACKGROUND Congenital extrahepatic porto-systemic shunt (CEPS), known as Abernethy malformation, is a rare malformation. Intestinal and/or splenic venous blood bypasses
DR. DO NGUYEN TIN CHILDREN HOSPITAL 1 BACKGROUND Congenital extrahepatic porto-systemic shunt (CEPS), known as Abernethy malformation, is a rare malformation. Intestinal and/or splenic venous blood bypasses
The Leeds Teaching Hospitals NHS Trust Transjugular Intrahepatic Portosystemic Shunt (TIPS)
") n The Leeds Teaching Hospitals NHS Trust Transjugular Intrahepatic Portosystemic Shunt (TIPS) Information for patients Your liver doctor has recommended that you have a Transjugular Intrahepatic Portosystemic
n The Leeds Teaching Hospitals NHS Trust Transjugular Intrahepatic Portosystemic Shunt (TIPS) Information for patients Your liver doctor has recommended that you have a Transjugular Intrahepatic Portosystemic
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Vascular Technology Examination Content Outline
 Vascular Technology Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Normal Anatomy, Perfusion, and Function Evaluate normal anatomy, perfusion, function 2 Pathology, Perfusion,
Vascular Technology Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Normal Anatomy, Perfusion, and Function Evaluate normal anatomy, perfusion, function 2 Pathology, Perfusion,
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Portal Venous Thrombosis: Tumor VS Bland Thrombus
 June 2015 Portal Venous Thrombosis: Tumor VS Bland Thrombus SERGIO ALFARO, HARVARD MEDICAL SCHOOL YEAR III GILLIAN LIEBERMAN, MD Overview 2 Index Patient History Portal Venous Thrombosis (PVT) Imaging
June 2015 Portal Venous Thrombosis: Tumor VS Bland Thrombus SERGIO ALFARO, HARVARD MEDICAL SCHOOL YEAR III GILLIAN LIEBERMAN, MD Overview 2 Index Patient History Portal Venous Thrombosis (PVT) Imaging
CARDIOVASCULAR DANIL HAMMOUDI.MD
 CARDIOVASCULAR DANIL HAMMOUDI.MD 18 Systemic Circulation Figure 19.19 Pulmonary Circulation Figure 19.18b 1. Thyroid gland 2. Trachea 3. Brachiocephalic 4. Common carotid 5. Internal jugular 6. Superior
CARDIOVASCULAR DANIL HAMMOUDI.MD 18 Systemic Circulation Figure 19.19 Pulmonary Circulation Figure 19.18b 1. Thyroid gland 2. Trachea 3. Brachiocephalic 4. Common carotid 5. Internal jugular 6. Superior
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
AASLD PRACTICE GUIDELINE. The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension. Preamble.
 AASLD PRACTICE GUIDELINE The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension Thomas D. Boyer 1 and Ziv J. Haskal 2 Preamble The recommendations in this article
AASLD PRACTICE GUIDELINE The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension Thomas D. Boyer 1 and Ziv J. Haskal 2 Preamble The recommendations in this article
Case Report Inferior Vena Cava Torsion and Stenosis Complicated by Compressive Pericaval Regional Ascites following Orthotopic Liver Transplantation
 Case Reports in Radiology Volume 2013, Article ID 576092, 4 pages http://dx.doi.org/10.1155/2013/576092 Case Report Inferior Vena Cava Torsion and Stenosis Complicated by Compressive Pericaval Regional
Case Reports in Radiology Volume 2013, Article ID 576092, 4 pages http://dx.doi.org/10.1155/2013/576092 Case Report Inferior Vena Cava Torsion and Stenosis Complicated by Compressive Pericaval Regional
Abdomen Sonography Examination Content Outline
 Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality prese
 Hepatopulmonary syndrome (HPS) By Alaa Haseeb, MS.c Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality presenting
Hepatopulmonary syndrome (HPS) By Alaa Haseeb, MS.c Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality presenting
PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES I HAVE NOTHING TO DISCLOSE CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017
 CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS
 BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
3 Circulatory Pathways
 40 Chapter 3 Circulatory Pathways Systemic Arteries -Arteries carry blood away from the heart to the various organs of the body. -The aorta is the longest artery in the body; it branches to give rise to
40 Chapter 3 Circulatory Pathways Systemic Arteries -Arteries carry blood away from the heart to the various organs of the body. -The aorta is the longest artery in the body; it branches to give rise to
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant