Endovascular Techniques for Symptomatic Portal Hypertension. Michael Meuse, M.D. Vascular and Interventional Radiology
|
|
|
- Kelley Todd
- 5 years ago
- Views:
Transcription
1 Endovascular Techniques for Symptomatic Portal Hypertension Michael Meuse, M.D. Vascular and Interventional Radiology
2 Objectives Review indications and contraindications for TIPS Define a treatment algorithm for acutely bleeding varicies Evaluation of Elective TIPS for ascites TIPS followup and management Role of Balloon-Occluded Retrograde Transvenous Obliteration (BRTO) of splenorenal gastric varicies
3 TIPS An intra-hepatic portal-systemic shunt usually created by advancing a needle, via a right jugular venous access, from the right hepatic vein to the right portal vein CO2 gas is used as an intravascular contrast agent rarely need iodinated contrast A covered stent is placed to maintain the track created with the needle and provides long term patency

4 TIPS Track

5 48 y/o WM with hepatitis B & C, cirrhosis, refractory ascities, and recurrent GI bleed 10F sheath already in place in right jugular vein


6 AP and Lateral CO2 Wedge Venograms LPV RPV PV LPV RPV PV

7 Colopinto Needle Exiting Right Hepatic Vein


8 Upon Getting Blood Return a Guidewire is Advanced

9 Stent Deployed and Dilated for Desired Gradient
10 Completion Venogram
11 General Indications for TIPS Management of symptoms related to portal hypertension Variceal bleeding Ascites Pleural effusion secondary to portal hypertension Hepatorenal syndrome Hepatopulmonary syndrome Ectopic Varicies Access for other portal vein interventions
12 TIPS For Acute Variceal Bleeding
13 Medical Management of Acute Variceal Bleeding Judicious volume replacement FFP and VIIa Lactulose Airway management (if heading to TIPS they will be intubated anyway) Vasopressin or somatostatin (terlipressin and octreotide)
14 Endoscopic Management Early EGD to exclude Mallory Weiss, etc. (up to 30% of presumed variceal bleeds are something else) Banding>sclerotherapy Hemostasis in 80% 25-30% continue or recur Otherwise move on to Sengstaken-Blakemore or Linton-Nachlas which are 90% effective 50% bleed on deflation May consider one more EGD
15 Surgical Options Esophageal transection 79% 30 day mortality 26% rebleeding rate Surgical portocaval shunt % mortality in acute setting with Child A or C respectively Liver Transplantation best option, but not usually available in acute setting
16 Emergent TIPS Uncontrolled bleeding or early (<48 hour) rebleeding after two EGD therapies Bypass endoscopic therapy in esophageal strictures bleeding gastric (??) and unusual GI varicies TIPS is not used as primary treatment encephalopathy risk is high survival no better than successful sclerotherapy/banding
17 Management We Look For Prior to Emergent TIPS EGD to confirm variceal bleeding some outside studies are OK and some are not Pharmacologic therapy tried first? Intubate Balloon tamponade if actively bleeding Try to defer if infected (20% of active bleeders have an in-hospital infection)
18 Work-up Prior to Emergent TIPS MR, CT or U/S (r/o tumors, polycystic disease and PV thrombosis) Cardiac history to exclude CHF, pulmonary HTN, and tricuspid valve disease (TTE) Correct INR to 1.8 and PLT to 50 per microliter
19 Emergent TIPS Outcomes 90% effective in controlling bleeding 40 day mortality is 25% if done within 48 hours of first failed endoscopic treatment
20 Survival Varies Widely If they have ascites, are on catecholamines, and if they have a balloon up, their mortality is 96% at 60 days If they don t have any of these three risk factors then 60 day mortality is only 2%
21 Acute Bleeding Mortality Markers of poor survival with or without TIPS APACHE II>18 On pressors Acute renal failure ALT >100 or bilirubin >3 Encephlaopathy or requiring ventilation After TIPS mortality related to Liver failure Sepsis Multi-organ failure Azoulay D. J Hepatol 2001; 35: 590
22 Other Tools to Predict Mortality of Acutely Bleeding TIPS Predictive index= 1.54 x (1 or 0 for ascites) x (1 or 0 for ventilation) x ln(wbc) x ln(ptt) x ln(cr) ln(PLT) Predictive index > 18.3 has 100% mortality Patch D. J Hepatol 1988; 114: 981)
23 Emergent versus Non-Emergent TIPS Survival If acutely bleeding at time of TIPS 34% die within 30 days If elective TIPS 16% 30 day mortality if not bleeding at time of TIPS 2.9 x greater odds of death if bleeding at times of TIPS Rajan DK, Haska ZJ. Am J Gastroenterol 1995; 108: 1143


24 Coronary Vein Embolization
25 Adjunctive Embolization Only done in conjunction with TIPS Embolize any veins still visible after TIPS placed and gradient dropped to 8 mmhg Stops acute bleeding Prevents competition with TIPS for systemic shunting Embolization also done if bleeding persists after TIPS Usually done with coils. Can use sotradecol, alcohol, glue, and other devices
26 Elective TIPS
27 Additional Evaluation Prior to Elective TIPS Age greater than 65 higher risk of post procedure encephalopathy Indications: bleeding recurring despite aggressive endoscopic treatment ascites refractory to medical management Are symptoms likely related to intrahepatic portal or hepatic vein obstruction? Does patient have signs or symptoms of encephalopathy Cardiac history?
28 Work Up Prior to Elective TIPS Liver function and kidney function not more than 1 week prior to procedure Coagulation not more than 48 hours prior to procedure (if previously abnormal) MRI If can t have MRI then do a CTA If can t have MRI or CTA then do an U/S Echo and EKG (may skip if no cardiac history and patient is <50)
29 MELD Model for end stage liver disease MELD=9.6 x ln(cr) x ln(bilirubin) x ln(inr) +6.4 >25 has 35% 3 month survival >18 has 40% 3 month survival <=18 has a 90% 3 month survival <10 has 100% 3 month survival Angermayr B. Gut 2003; 52: 879

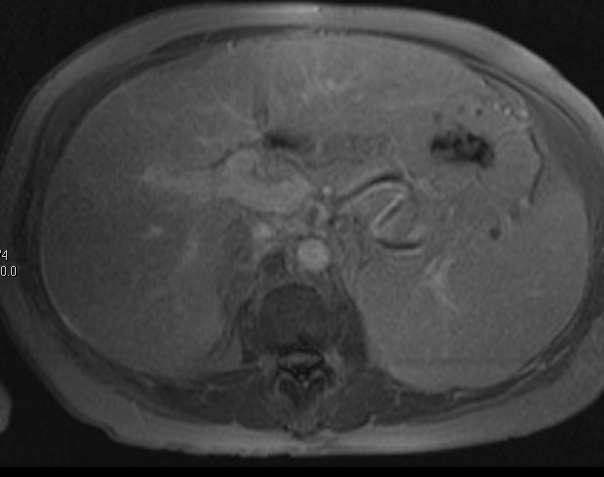
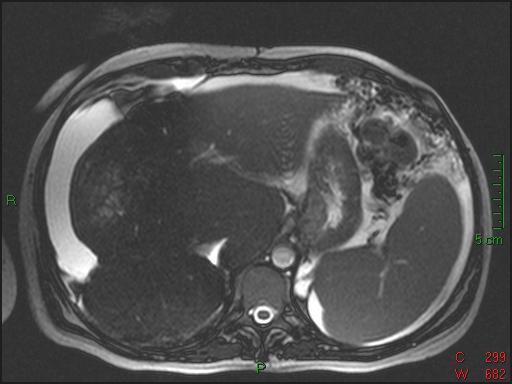
30 MRI in Patient with Bleeding Rectal Varicies
31 Elective TIPS for Varicies Esophageal varicies refractory to endoscopic treatment Gastric Varicies that cannot be glued Varicies in areas usually not amenable to endoscopic or surgical management Stoma Rectal


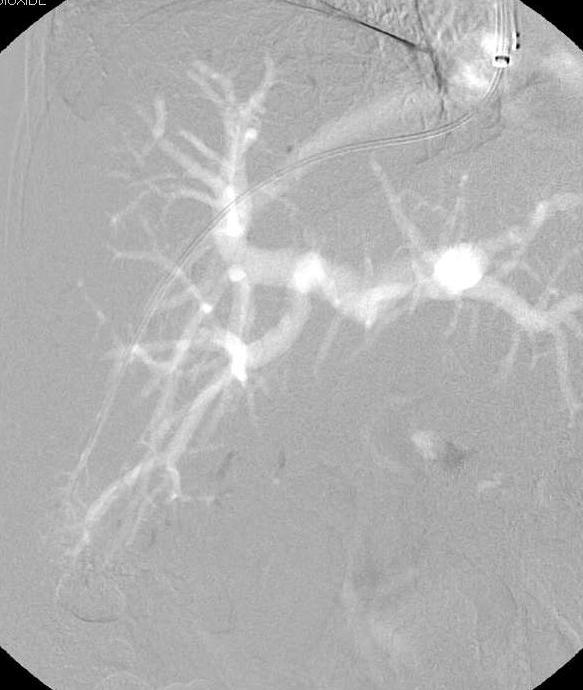
32 Hepatic Venogram Poor Reflux with CO2

33 Occlusion Balloon Still No Reflux into Portal Vein

34 Portal Venogram

35 Portal Decompressed
36 Etiology of Ascites Portal hypertension PS gradient > 12 mmhg Sodium retention Decreased intravascular volume Lymphatic leakage from liver
37 Treatment of Ascites Diuretics 10-20% of ascites is refractory to diuretics LVP next line therapy Patients requiring frequent LVP (>2 times a month) should be considered for TIPS Peritoneal venous shunt too many occlusions to be widely used LTX
38 Outcome of TIPS for Ascites 95% technical success 9% complication rate 3% hemorrhage 3% ARF 1.5% sepsis 1.2% hemolysis 11% heart failure 33% encephalopathy Not reduced by prophylactic lactulose Biggest predictor is baseline encephalopathy
39 Mortality in TIPS for Ascites Analysis of 16 studies Pooled estimate for complete response at 6 months was 45% and for any response (complete and partial) was 63%. Pooled 6-month mortality after TIPS was 36%. Risk factors for mortality Renal insufficiency (serum creatinine >1.5 mg/dl) Hyperbilirubinemia (total bilirubin >3 mg/dl) Advanced age (>60 yr) Poor response to TIPS Refractory cases associated with 100% mortality New or worsening encephalopathy after TIPS was 32% Improvement in creatinine clearance and urinary sodium excretion Am J Gastroenterol Nov;98(11):2521-7
40 Target PSG Mean pressure gradient from PV to RA Post TIPS gradient: >16 is no help 8-12 recommended <5 lead to high incidence of encephalopathy
41 Summary of TIPS for Ascites Most have improvement Many still require diruretics Most demonstrate improving nutrition Probably does not change mortality High creatinine and high bilirubin Encephalopathy usually well controlled medically If not controlled, TIPS reduction a must
42 Occluded hepatic veins Difficult Cases Wedge catheter and needle in a small branch and proceed as usual Directly enter liver through intra-hepatic portion of IVC (DIPS) Portal Vein Thrombosis Recannalize PV and stent open Reverse TIPS Very shrunken livers Reverse TIPS Other ways to make a target in the PV
43
44 Budd-Chiari Syndrome Hepatic vein obstruction raises portal pressure Hypertrophied caudate lobe (short hepatic veins) TIPS normally uses hepatic vein as starting point Work in small hepatic vein remnant Direct puncture from intrahepatic IVC


45 No Hepatic Vein Branches


46 Wire in Hepatic Artery


47 CO2 Injections Guide Needle Advancement

48 3 Dimensional Imaging of Portal


49 Track Dilated

50 TIPS Stented and Dilated

51 TIPS Completed Portal-Atrial Gradient=8 mmhg
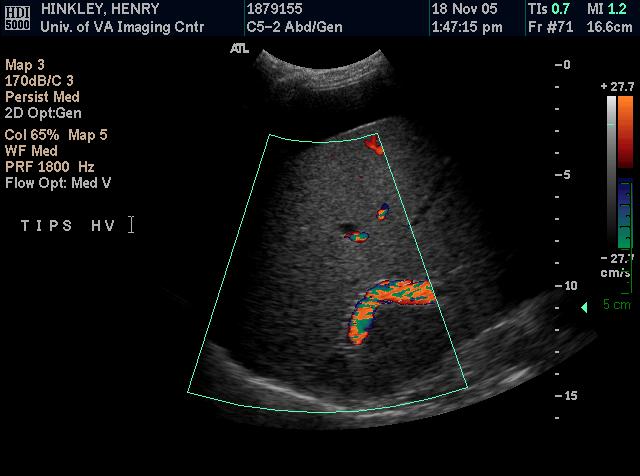
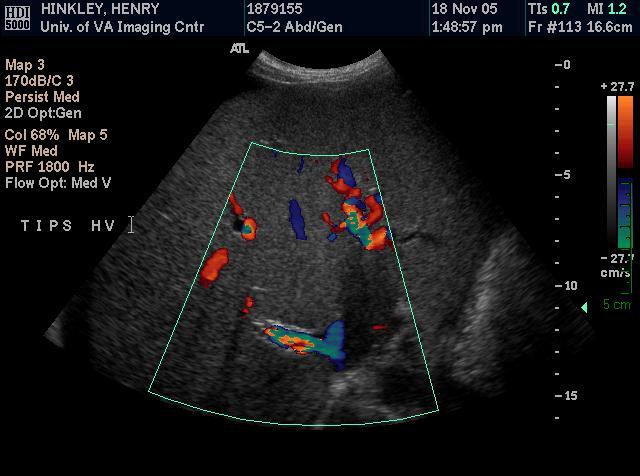
52 Follow-Up of TIPS
53 Refractory Ascites Despite TIPS
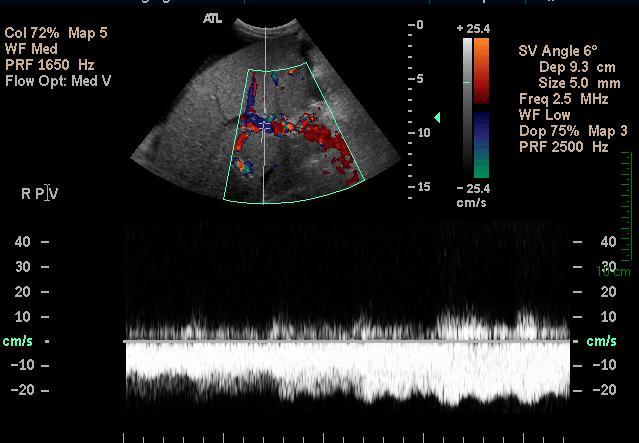
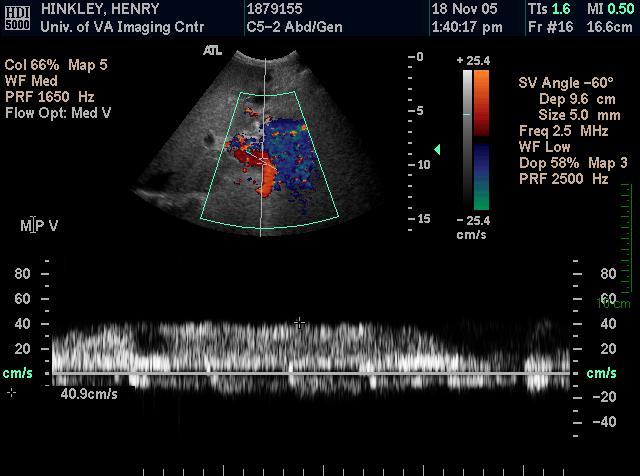
54 Ultrasound Surveillance TIPS with PPG <12 mmhg (n = 60) TIPS Dysfunction (n = 57) Mean TIPS Vmax (cm/s) 99.1 ± ± 55.9 NS p Mean PV Vmax (cm/s) 29.8 ± ± 6.3 < Change in Mean TIPS Vmax (%) 18 ± ± 46 NS Change in mean PV Vmax (%) 19 ± ± 23 NS Flow Direction 52/8 31/26 < JG Abraldes, Utility of Color Doppler Ultrasonography Predicting TIPS Dysfunction. Am J Gastro. 2005; 100:


55 Once TIPS Stent Encorporated We Can Visualize Stent Lumen


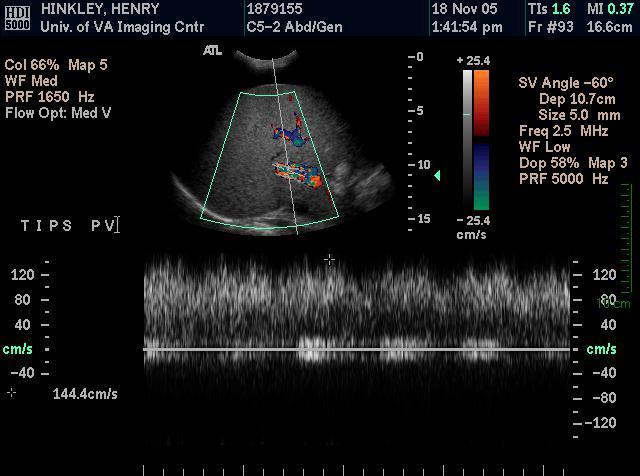
56 TIPS Check P-S gradient 14 mm Hg


57 Prepare to Place Second TIPS

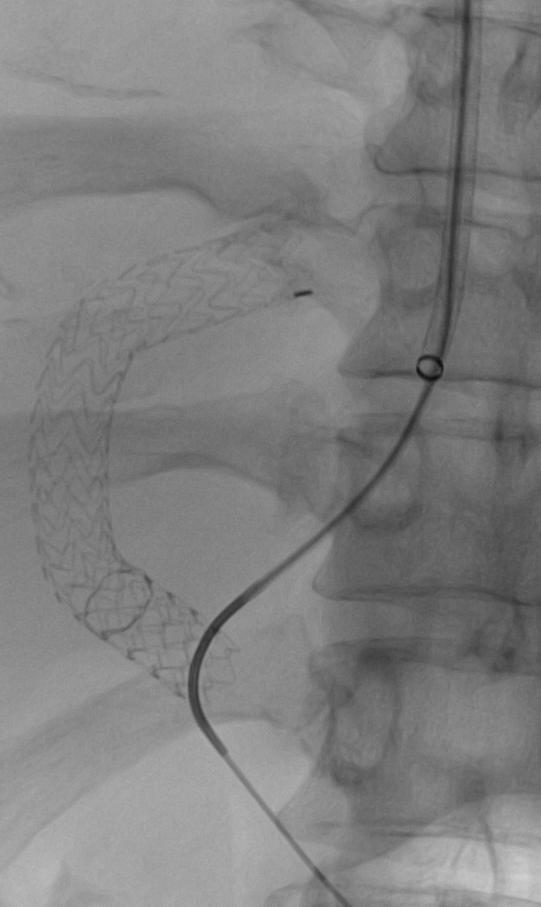
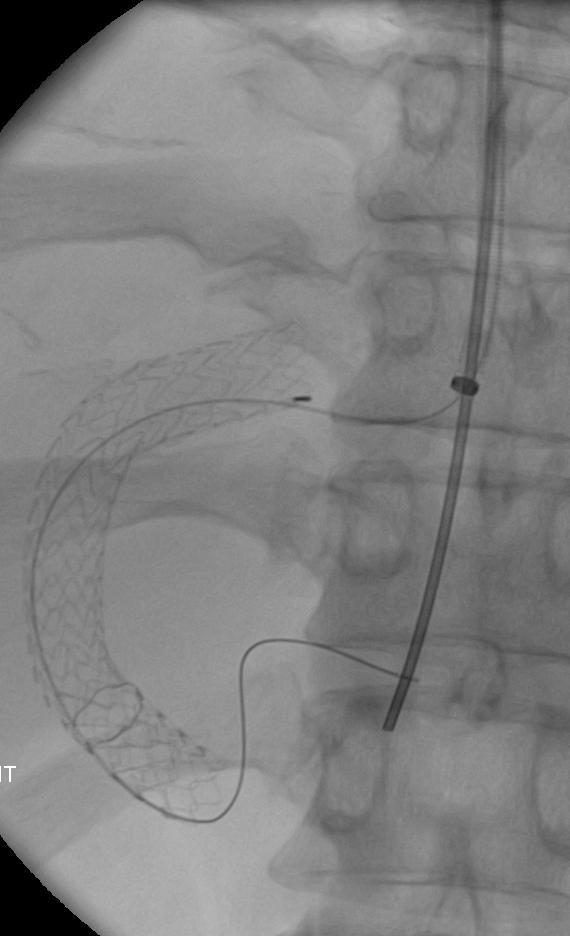
58 Second Wire Was A Target


59 Track Dilated and Stent Deployed

60 Second TIPS to Increase Flow P-S gradient down to 8 mm Hg
61 Contraindications to TIPS Right heart cannot handle extra flow Tricuspid disease CHF Severe (systolic >45 mmhg) pulmonary hypertension Technical blockages Bilateral jugular vein or SVC obstruction Hepatic vein obstruction Portal vein obstruction Liver tumor in between the hepatic veins and portal veins Very poor liver function Uncorrectable coagulopathy Severe encephalopathy

62 Other Structures Opacified
63 Access site Complications of TIPS Bleeding Carotid artery or jugular vein injury Chest Cardiac injury Pneumothorax Liver Bleeding Abscess Bile leak Infarction Portal thrombosis
64 Systemic Effects of TIPS Sepsis Encephalopathy Tumor spread
65 Etiology of Encephalopathy Nitrogenous compounds allowed to bypass the liver Gamma-Aminobutyric acid and benzodiazepines (neurotransmitters)
66 Management of post TIPS Encephalopathy Restrict protein (<.5gm/kg/day) Catharsis Control GI bleeds Review medications Return to alcohol? Lactulose (15-45 ml q8-12 for 2-3 stools/day) Neomycin or metronidazole Branched chain amino acid diet Flumazenil, bromocriptine to block GABA
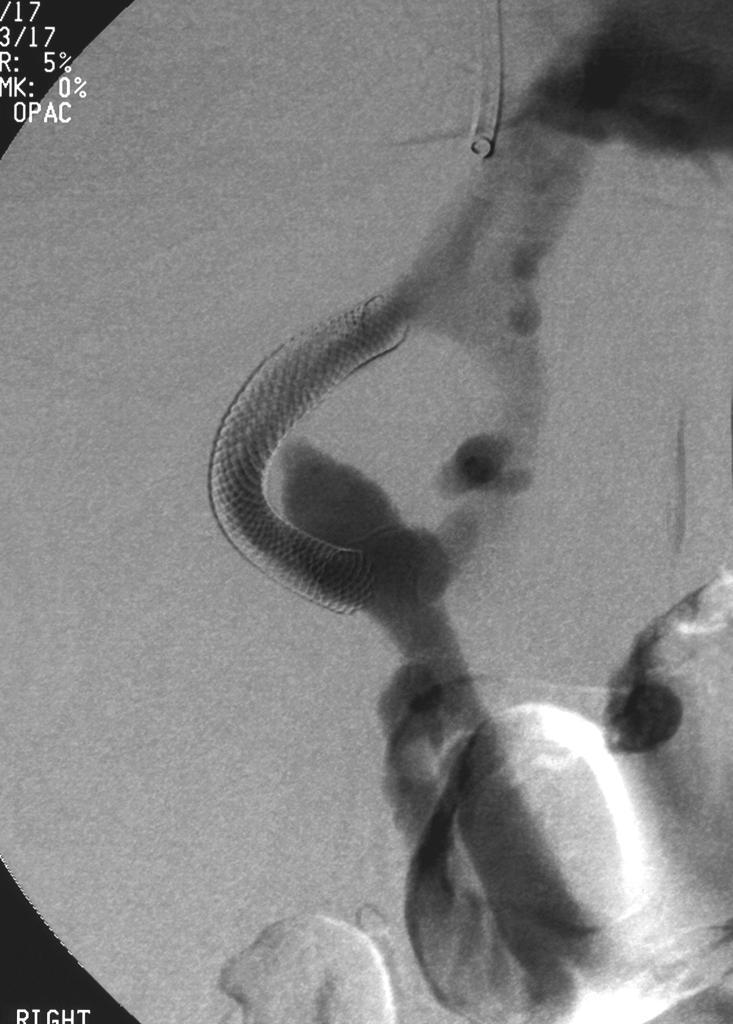
67 Reducing a TIPS Hemolysis Uncontrollable encephalopathy Avoid occluding the TIPS leads to severe ill effects (hemorrhage, hypotension, acidosis) Additional hour-glass shaped stent placed
68 BRTO

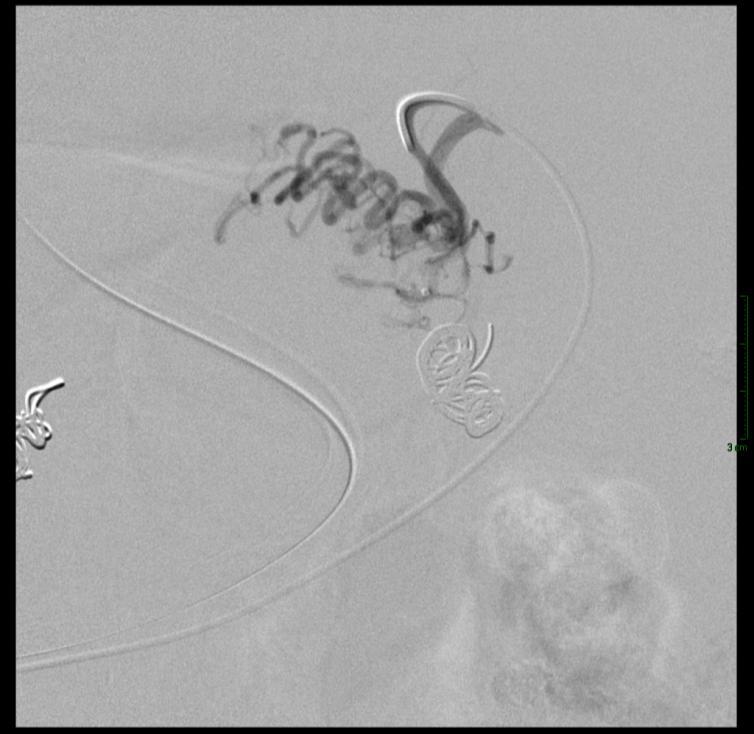
69 TIPS Check for UGI Bleeding

70

 PSG")
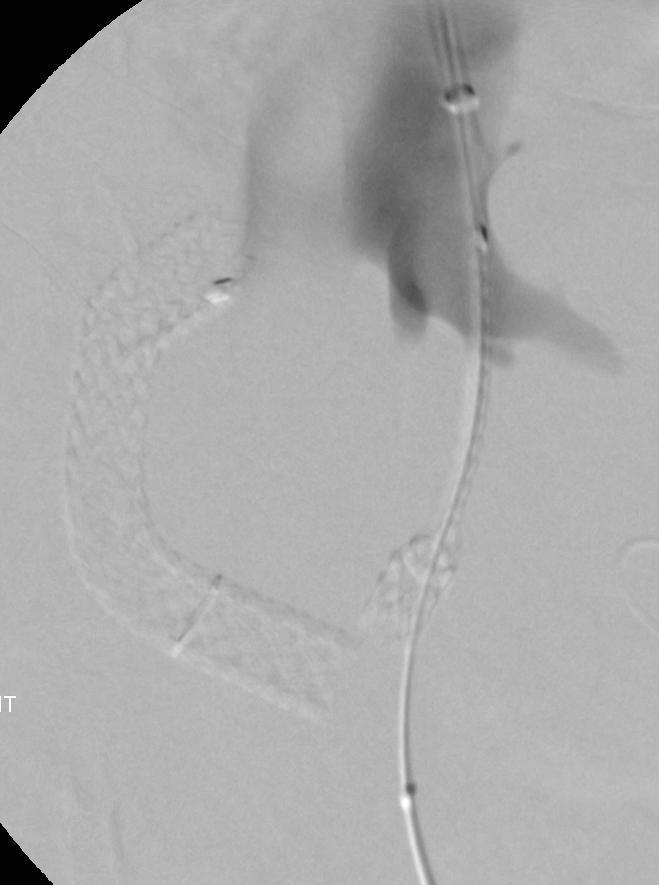
71 TIPS Recanalization With Distal End Revision Bard self expanding stent placed (Fluency) PSG 13mmHg

72

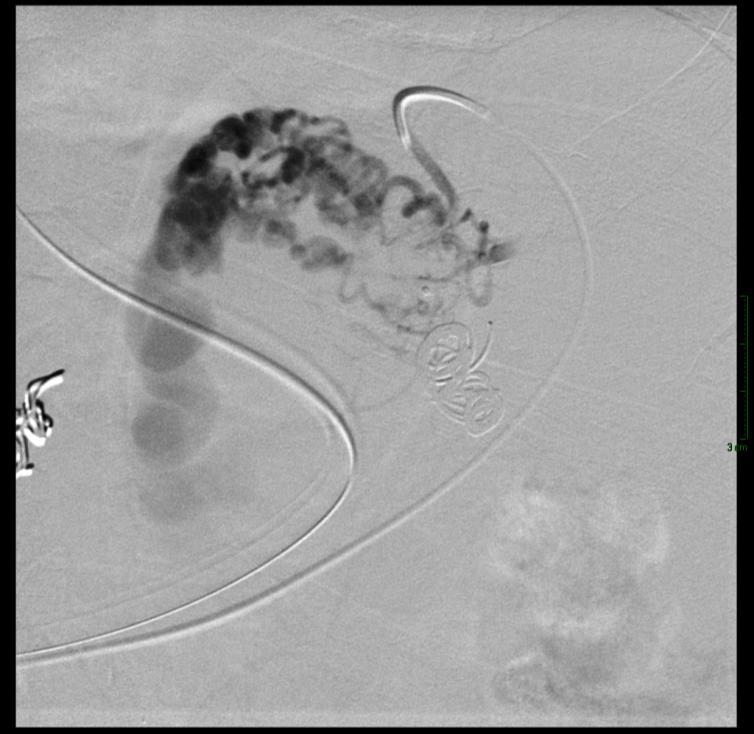
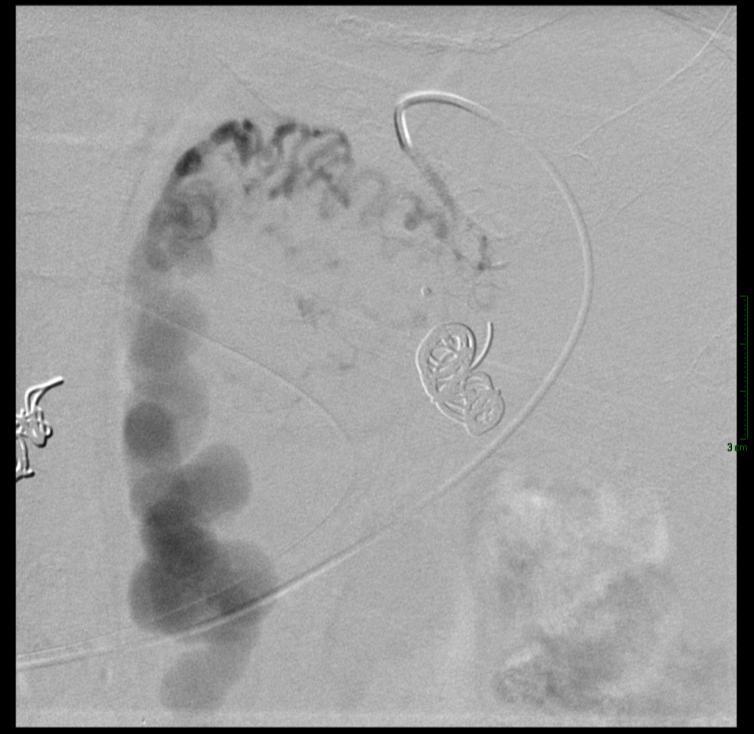
73 TIPS Check For Recurrent Massive UGI Bleeding
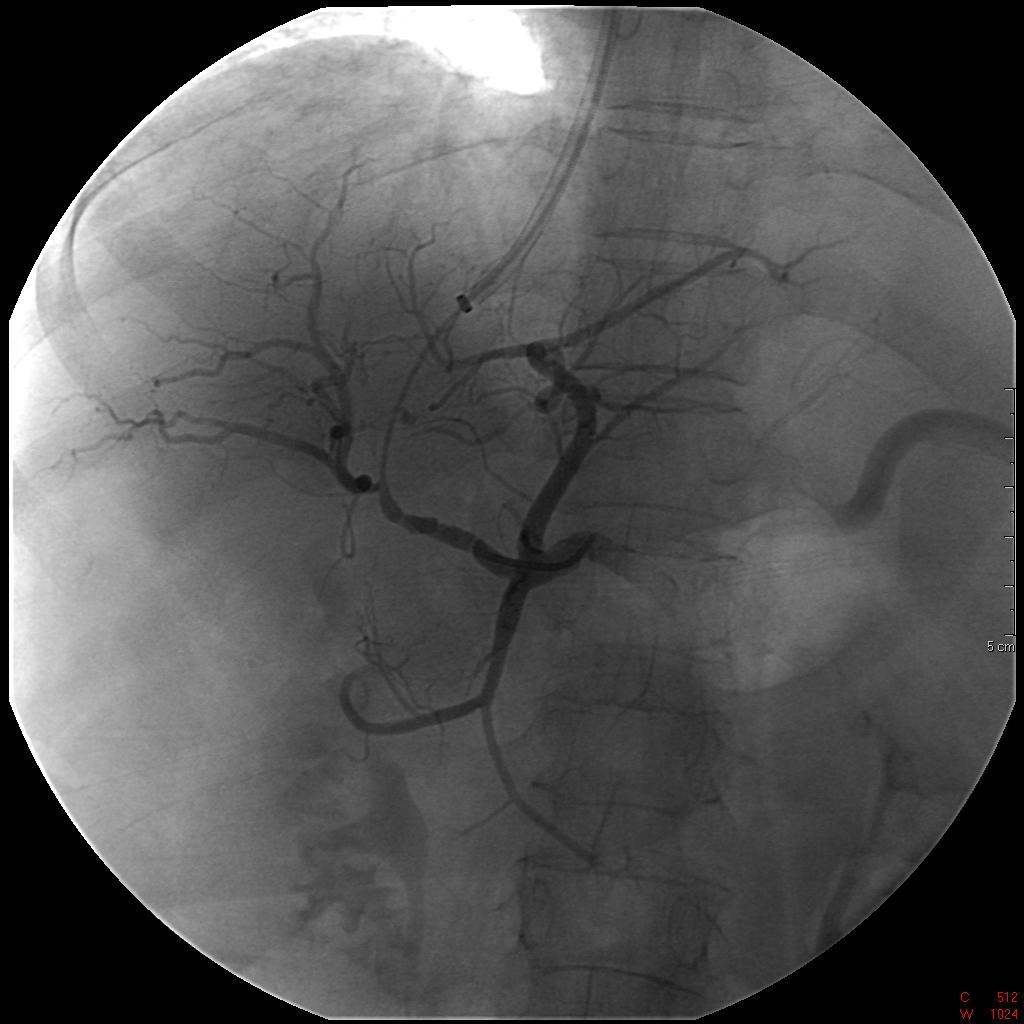
74 Spleno-Renal Shunt Catheter in short gastric vein branch of splenic vein
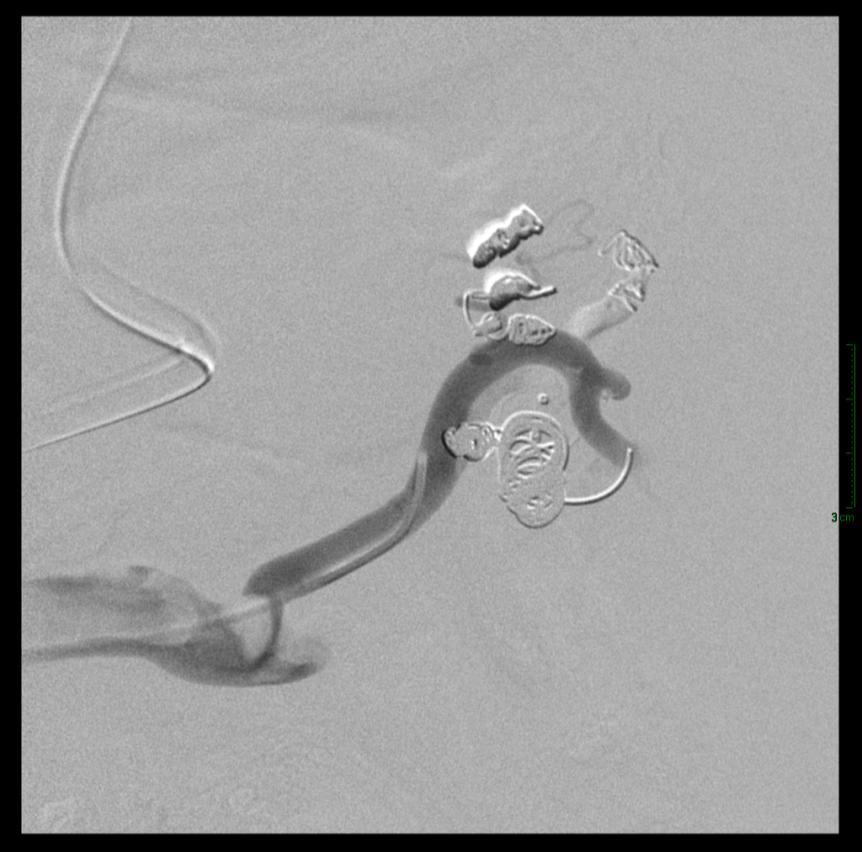
75 Aggressive Embolization

76 Parallel TIPS Created PSG 6-7 mmhg


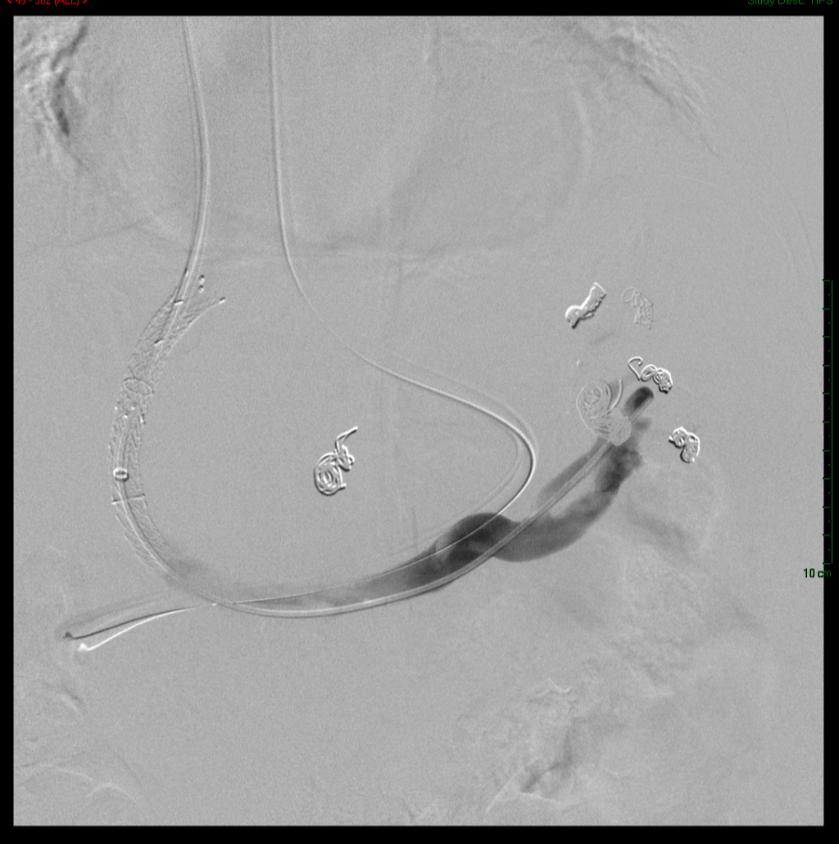
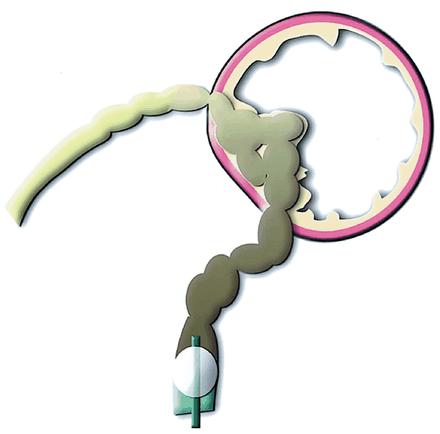
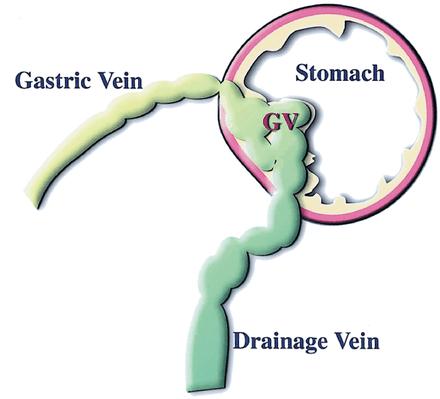
77 Gastric Variceal Anatomy Afferent Gastric Veins Potential Draining Veins
")
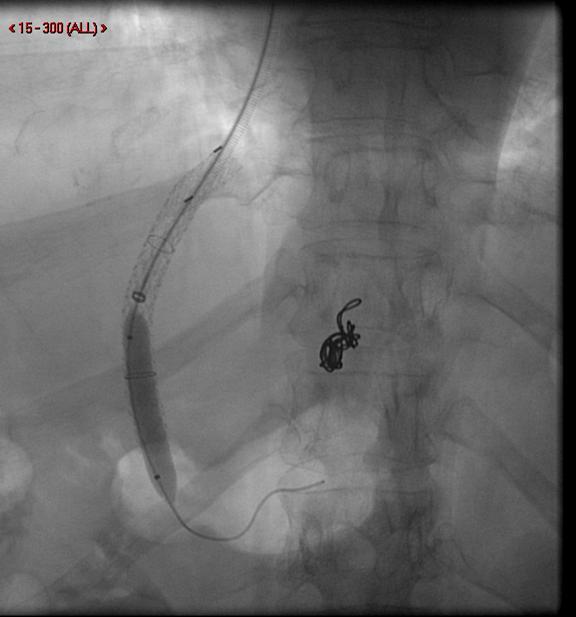
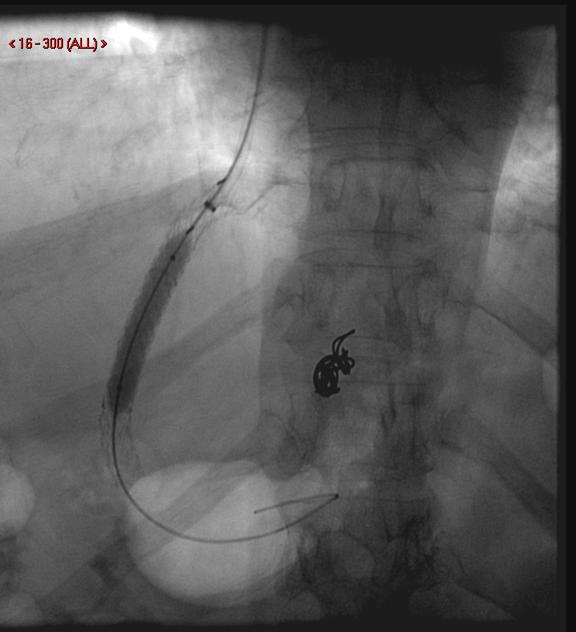
78 B-RTO (Balloon Retrograde Transvenous Obliteration)
79 B-RTO Appearance on Endoscopy

80 Catheterized Spleno-Renal Shunt

81

82
83
84
85
86

87
88

89
")

90 CORONAL PLANE (DYNA CT) Gastro-renal Shunt TIPS Occlusion Balloon


91 SAGITTAL PLANE (DYNA CT) Stomach Gastric Varix


92 CT PRE and Post BRTO PRE B-RTO 72 HRS POST B-RTO Bleeding Gastric Varices Thrombosed Gastric Varices


93 CT PRE and Post BRTO PRE B-RTO 72 HRS POST B-RTO SAGITTAL (MDCT) Patent Gastrorenal Shunt Thrombosed Gastrorenal Shunt
94 B-RTO Indications Indications Gastric Varices Prophylactic Management High Risk GV Poor TIPS candidates (B-RTO alone) B-RTO as adjunct to TIPS Acute Management Bleeding GV Adjunct (to TIPS and Endoscopic Glue Therapy) Refractory Hepatic Encephalopathy B-RTO alone B-RTO with partial splenic artery embolization
95 B-RTO Outcomes Procedural success (>90%) Recurrent bleeding (<10%) Complications Worsening esophageal varices (10-30%) Non-target embolization (rare) Gastric Ulceration (rare - case report) Hemoglobinurin (50%)
96 Conclusions TIPS a valuable adjunct in the management of symptomatic portal hypertension Procedure provides high technical success with good clinical outcomes in carefully selected patient population
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Tranjugular Intrahepatic Portosystemic Shunt
 Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Portogram shows opacification of gastroesophageal varices.
 Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Transjugular Intrahepatic
 Transjugular Intrahepatic Portosystemic Shunt (TIPS): A Clinical and Procedural Review Mark R. Werley, M.D. and John Briguglio, M.D. Lancaster Radiology Associates, Ltd. INTRODUCTION This article reviews
Transjugular Intrahepatic Portosystemic Shunt (TIPS): A Clinical and Procedural Review Mark R. Werley, M.D. and John Briguglio, M.D. Lancaster Radiology Associates, Ltd. INTRODUCTION This article reviews
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Transjugular Intrahepatic Portosystemic Shunt Reduction for Management of Recurrent Hepatic Encephalopathy
 CLINICAL IMAGES Ochsner Journal 17:311 316, 2017 Ó Academic Division of Ochsner Clinic Foundation Transjugular Intrahepatic Portosystemic Shunt Reduction for Management of Recurrent Hepatic Encephalopathy
CLINICAL IMAGES Ochsner Journal 17:311 316, 2017 Ó Academic Division of Ochsner Clinic Foundation Transjugular Intrahepatic Portosystemic Shunt Reduction for Management of Recurrent Hepatic Encephalopathy
BRTO /PARTO Indications and outcomes
 BRTO /PARTO Indications and outcomes Saher Sabri, MD Associate Professor of Radiology and Surgery Division of Interventional Radiology University of Virginia Health System Saher Sabri, M.D. Speakers Bureau:
BRTO /PARTO Indications and outcomes Saher Sabri, MD Associate Professor of Radiology and Surgery Division of Interventional Radiology University of Virginia Health System Saher Sabri, M.D. Speakers Bureau:
TIPS. D Patch Royal Free Hospital London UK
 TIPS D Patch Royal Free Hospital London UK TIPS Technique Ascites Budd Chiari Variceal Bleeding Historical Experimental Development 1967 Piccone Shunt between recanalized umbilical vein and saphenous
TIPS D Patch Royal Free Hospital London UK TIPS Technique Ascites Budd Chiari Variceal Bleeding Historical Experimental Development 1967 Piccone Shunt between recanalized umbilical vein and saphenous
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
Direct Intrahepatic Porta-Caval Shunt Technique & Tips-Tricks. Pierre GOFFETTE, MD, St-Luc University Hospital University of Leuven Brussels
 Direct Intrahepatic Porta-Caval Shunt Technique & Tips-Tricks Pierre GOFFETTE, MD, St-Luc University Hospital University of Leuven Brussels Pierre Goffette, M.D. Consultant/Advisory Board: Covidien (Neuro)
Direct Intrahepatic Porta-Caval Shunt Technique & Tips-Tricks Pierre GOFFETTE, MD, St-Luc University Hospital University of Leuven Brussels Pierre Goffette, M.D. Consultant/Advisory Board: Covidien (Neuro)
AASLD PRACTICE GUIDELINE. The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension. Preamble.
 AASLD PRACTICE GUIDELINE The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension Thomas D. Boyer 1 and Ziv J. Haskal 2 Preamble The recommendations in this article
AASLD PRACTICE GUIDELINE The Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension Thomas D. Boyer 1 and Ziv J. Haskal 2 Preamble The recommendations in this article
Barbara Rus Gadžijev Peter Popovič Klinični inštitut za radiologijo UKC Ljubljana
 STROKOVNI SESTANEK ZDRUŽENJA HEMATOLOGOV SLOVENIJE IN ZDRUŽENJA ZA TRANSFUZIJSKO MEDICINO, Terme Zreče, 17.-18.4.2015 Barbara Rus Gadžijev Peter Popovič Klinični inštitut za radiologijo UKC Ljubljana goals,
STROKOVNI SESTANEK ZDRUŽENJA HEMATOLOGOV SLOVENIJE IN ZDRUŽENJA ZA TRANSFUZIJSKO MEDICINO, Terme Zreče, 17.-18.4.2015 Barbara Rus Gadžijev Peter Popovič Klinični inštitut za radiologijo UKC Ljubljana goals,
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Manejo Actual del Sangrado por Varices Gástricas
 Manejo Actual del Sangrado por Varices Gástricas Juan Carlos Garcia-Pagán Barcelona Hepatic Hemodynamic Laboratory. Liver Unit. IMDIM. Hospital Clinic. IDIBAPS. Ciberehd. XXIV Congreso de la Asociación
Manejo Actual del Sangrado por Varices Gástricas Juan Carlos Garcia-Pagán Barcelona Hepatic Hemodynamic Laboratory. Liver Unit. IMDIM. Hospital Clinic. IDIBAPS. Ciberehd. XXIV Congreso de la Asociación
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap. Simon McPherson, Vascular Interventional Radiologist, Leeds
 Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Acute TIPS occlusion due to iatrogenic arteriovenous shunt in a cirrhotic patient with total portal vein thrombosis
 Interventional Medicine & Applied Science, Vol. 7 (4), pp. 166 170 (2015) CASE REPORT Acute TIPS occlusion due to iatrogenic arteriovenous shunt in a cirrhotic patient with total portal vein thrombosis
Interventional Medicine & Applied Science, Vol. 7 (4), pp. 166 170 (2015) CASE REPORT Acute TIPS occlusion due to iatrogenic arteriovenous shunt in a cirrhotic patient with total portal vein thrombosis
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12:
 Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Virtual Mentor American Medical Association Journal of Ethics December 2008, Volume 10, Number 12: 805-809. CLINICAL PEARL Indications for Use of TIPS in Treating Portal Hypertension Elizabeth C. Verna,
Obliterative hepatocavopathy ultrasound and cavography findings
 doi:10.2478/v10019-008-0020-6 case report Obliterative hepatocavopathy ultrasound and cavography findings Ramazan Kutlu Department of Radiology, Inonu University School of Medicine, Malatya, Turkey ackgound.
doi:10.2478/v10019-008-0020-6 case report Obliterative hepatocavopathy ultrasound and cavography findings Ramazan Kutlu Department of Radiology, Inonu University School of Medicine, Malatya, Turkey ackgound.
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Noncirrhotic Portal Hypertension: Imaging, Hemodynamics, and Endovascular Therapy
 REVIEW Noncirrhotic Portal Hypertension: Imaging, Hemodynamics, and Endovascular Therapy Venkatesh P. Krishnasamy, M.D.,* Michael J. Hagar, M.D., Albert K. Chun, M.D., M.B.A., and Elliot Levy, M.D. Patients
REVIEW Noncirrhotic Portal Hypertension: Imaging, Hemodynamics, and Endovascular Therapy Venkatesh P. Krishnasamy, M.D.,* Michael J. Hagar, M.D., Albert K. Chun, M.D., M.B.A., and Elliot Levy, M.D. Patients
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
BRTO: Updates to Techniques
 Session XIV: BRTO, PARTO and Portal Hypertension GEST2016 BRTO: Updates to Techniques Hiro Kiyosue Oita University Hospital, Japan Hiro Kiyosue, MD Royalty: Cook, Medkit Consulting Fee: Stryker Japan,
Session XIV: BRTO, PARTO and Portal Hypertension GEST2016 BRTO: Updates to Techniques Hiro Kiyosue Oita University Hospital, Japan Hiro Kiyosue, MD Royalty: Cook, Medkit Consulting Fee: Stryker Japan,
Transcaval TIPS in Patients with Failed Revision of Occluded Previous TIPS
 Transcaval TIPS in Patients with Failed Revision of Occluded Previous TIPS Chang Kyu Seong, MD Yong Joo Kim, MD Tae Beom Shin, MD Hyo Yong Park, MD Tae Hun Kim, MD Duk Sik Kang, MD Index terms: Hypertension,
Transcaval TIPS in Patients with Failed Revision of Occluded Previous TIPS Chang Kyu Seong, MD Yong Joo Kim, MD Tae Beom Shin, MD Hyo Yong Park, MD Tae Hun Kim, MD Duk Sik Kang, MD Index terms: Hypertension,
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Patrick S. Kamath, MD, and David M. Nagorney, MD
 gastrointestinal tract and abdomen PORTAL HYPERTENSION Patrick S. Kamath, MD, and David M. Nagorney, MD Portal hypertension is diagnosed when the hepatic veinpressure gradient (HVPG), which reflects hepatic
gastrointestinal tract and abdomen PORTAL HYPERTENSION Patrick S. Kamath, MD, and David M. Nagorney, MD Portal hypertension is diagnosed when the hepatic veinpressure gradient (HVPG), which reflects hepatic
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Use of transjugular intrahepatic portosystemic shunt in liver disease
 Vol. XVIII No. 3 JOURNAL OF VASCULAR NURSING PAGE 83 Use of transjugular intrahepatic portosystemic shunt in liver disease Patricia Ann Radovich, RN, MSN, CCRN, FCCM Persons with cirrhosis have many complications.
Vol. XVIII No. 3 JOURNAL OF VASCULAR NURSING PAGE 83 Use of transjugular intrahepatic portosystemic shunt in liver disease Patricia Ann Radovich, RN, MSN, CCRN, FCCM Persons with cirrhosis have many complications.
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CHAPTER 7. End Stage Liver Disease in the ICU: Walking a Tightrope. Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing
 CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
Left-sided portal hypertension with a patent splenic vein: An impossible or a not-so-uncommon scenario?
 Khan et al. 108 CASE REPORT PEER REVIEWED OPEN ACCESS Left-sided portal hypertension with a patent splenic vein: An impossible or a not-so-uncommon scenario? Iftikhar Khan, Ghassan Ramahi, Saif Zaabi,
Khan et al. 108 CASE REPORT PEER REVIEWED OPEN ACCESS Left-sided portal hypertension with a patent splenic vein: An impossible or a not-so-uncommon scenario? Iftikhar Khan, Ghassan Ramahi, Saif Zaabi,
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Portal Venous Thrombosis: Tumor VS Bland Thrombus
 June 2015 Portal Venous Thrombosis: Tumor VS Bland Thrombus SERGIO ALFARO, HARVARD MEDICAL SCHOOL YEAR III GILLIAN LIEBERMAN, MD Overview 2 Index Patient History Portal Venous Thrombosis (PVT) Imaging
June 2015 Portal Venous Thrombosis: Tumor VS Bland Thrombus SERGIO ALFARO, HARVARD MEDICAL SCHOOL YEAR III GILLIAN LIEBERMAN, MD Overview 2 Index Patient History Portal Venous Thrombosis (PVT) Imaging
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Review Article Self-Expandable Metal Stents in the Treatment of Acute Esophageal Variceal Bleeding
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2011, Article ID 910986, 6 pages doi:10.1155/2011/910986 Review Article Self-Expandable Metal Stents in the Treatment of Acute
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2011, Article ID 910986, 6 pages doi:10.1155/2011/910986 Review Article Self-Expandable Metal Stents in the Treatment of Acute
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments
 CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) In CY2015 and in an effort to help pay providers for quality, not
CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) In CY2015 and in an effort to help pay providers for quality, not
Sclerosing Agents: Tips & Tricks Session: Liquid Embolics
 Sclerosing Agents: Tips & Tricks Session: Liquid Embolics Jeffrey S. Pollak, M.D. Robert I. White, Jr., M.D. Professor of Interventional Radiology Yale University School of Medicine Department of Radiology
Sclerosing Agents: Tips & Tricks Session: Liquid Embolics Jeffrey S. Pollak, M.D. Robert I. White, Jr., M.D. Professor of Interventional Radiology Yale University School of Medicine Department of Radiology
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Variceal bleeding. Mainz,
 Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
DR. DO NGUYEN TIN CHILDREN HOSPITAL 1
 DR. DO NGUYEN TIN CHILDREN HOSPITAL 1 BACKGROUND Congenital extrahepatic porto-systemic shunt (CEPS), known as Abernethy malformation, is a rare malformation. Intestinal and/or splenic venous blood bypasses
DR. DO NGUYEN TIN CHILDREN HOSPITAL 1 BACKGROUND Congenital extrahepatic porto-systemic shunt (CEPS), known as Abernethy malformation, is a rare malformation. Intestinal and/or splenic venous blood bypasses
Portal hypertension and ascites
 Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Portal hypertension and ascites Muhammad S Mirza Guruprasad P Aithal Abstract Portal pressure is the product of portal blood flow and resistance; an increase in either leads to increased portal pressure.
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Portal hypertension is the main complication of cirrhosis
 GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
GASTROENTEROLOGY 2001;120:726 748 Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis GUADALUPE GARCIA TSAO
Follow this and additional works at:
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Comparison of transjugular intrahepatic portosystemic shunt with covered stent and balloon-occluded retrograde
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Comparison of transjugular intrahepatic portosystemic shunt with covered stent and balloon-occluded retrograde
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما
 بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
CY2015 Hospital Outpatient: Endovascular Procedure APCs and Complexity Adjustments
 CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis
 Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Gastric fundal varices with hemorrhage are
 alloon-occluded Retrograde Transvenous Obliteration of Gastric Varices review of the anatomy, technique, and outcomes. Y SHER S. SRI, MD; ULKU C. TUR, MD; WEL E.. SD, MD; UH WHN PRK, MD; ND JOHN F. NGLE,
alloon-occluded Retrograde Transvenous Obliteration of Gastric Varices review of the anatomy, technique, and outcomes. Y SHER S. SRI, MD; ULKU C. TUR, MD; WEL E.. SD, MD; UH WHN PRK, MD; ND JOHN F. NGLE,
INTRAHEPATIC PSS: AN INTERVENTIONALIST S PERSPECTIVE
 INTRAHEPATIC PSS: AN INTERVENTIONALIST S PERSPECTIVE Matthew W. Beal, DVM, DACVECC College of Veterinary Medicine, Michigan State University, East Lansing, MI Key Points: Percutaneous transjugular coil
INTRAHEPATIC PSS: AN INTERVENTIONALIST S PERSPECTIVE Matthew W. Beal, DVM, DACVECC College of Veterinary Medicine, Michigan State University, East Lansing, MI Key Points: Percutaneous transjugular coil
Title: Cholestasis after TIPS placement in a patient with primary sclerosing cholangitis: an uncommon complication
 Title: Cholestasis after TIPS placement in a patient with primary sclerosing cholangitis: an uncommon complication Authors: Alejandro Salagre García, Carolina Muñoz Codoceo, Elena Gómez Domínguez, Inmaculada
Title: Cholestasis after TIPS placement in a patient with primary sclerosing cholangitis: an uncommon complication Authors: Alejandro Salagre García, Carolina Muñoz Codoceo, Elena Gómez Domínguez, Inmaculada
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Complications of Cirrhosis
 What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
MINIMALLY INVASIVE MANAGEMENT OF RENOVASCULAR COMPLICATIONS AFTER RENAL GRAFT TRANSPLANTATION
 MINIMALLY INVASIVE MANAGEMENT OF RENOVASCULAR COMPLICATIONS AFTER RENAL GRAFT TRANSPLANTATION Gortes, Francisco Javier B.S; Salsamendi, Jason Thomas M.D LEARNING OBJECTIVES Educate physicians on the prompt
MINIMALLY INVASIVE MANAGEMENT OF RENOVASCULAR COMPLICATIONS AFTER RENAL GRAFT TRANSPLANTATION Gortes, Francisco Javier B.S; Salsamendi, Jason Thomas M.D LEARNING OBJECTIVES Educate physicians on the prompt
The SplitWire Percutaneous Transluminal Angioplasty Scoring Device. Instructions for Use
 The SplitWire Percutaneous Transluminal Angioplasty Scoring Device Instructions for Use Contents Contains one (1) SplitWire device. Sterile. Sterilized with ethylene oxide gas. Radiopaque. For single use
The SplitWire Percutaneous Transluminal Angioplasty Scoring Device Instructions for Use Contents Contains one (1) SplitWire device. Sterile. Sterilized with ethylene oxide gas. Radiopaque. For single use
Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality prese
 Hepatopulmonary syndrome (HPS) By Alaa Haseeb, MS.c Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality presenting
Hepatopulmonary syndrome (HPS) By Alaa Haseeb, MS.c Definition: HPS is a disease process with a triad of: 1- Liver disease. 2- Widespread intrapulmonary vasodilatation. 3- Gas exchange abnormality presenting
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein
: Portal HTN and Derivatives for the USMLE Step One Exam. Ultrasound (w/ doppler) Reversal of flow Portal Vein") Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Podcast (Video Recorded Lecture Series): Portal HTN and Derivatives for the USMLE Step One Exam Hepatic Vein (Budd Chiari) Ultrasound (w/ doppler) Reversal of flow Portal Vein Howard J. Sachs, MD www.12daysinmarch.com
Occlusion: A New Technique Antegrade wiring i with retrograde ballooning and stenting
 How To Treat Resistant Central Venous Occlusion: A New Technique Antegrade wiring i with retrograde ballooning and stenting Dafsah A Juzar T. Santoso National Heart Center, Harapan Kita, & Medistra Hospital
How To Treat Resistant Central Venous Occlusion: A New Technique Antegrade wiring i with retrograde ballooning and stenting Dafsah A Juzar T. Santoso National Heart Center, Harapan Kita, & Medistra Hospital
Sample page. POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
 2018 Complete Guide for Interventional Radiology An in-depth guide to interventional radiology coding, billing, and reimbursement for facilities and physicians POWER UP YOUR CODING with Optum360, your
2018 Complete Guide for Interventional Radiology An in-depth guide to interventional radiology coding, billing, and reimbursement for facilities and physicians POWER UP YOUR CODING with Optum360, your
Clinical Study Transjugular Intrahepatic Portosystemic Shunt for the Treatment of Portal Hypertension in Noncirrhotic Patients with Portal Cavernoma
 Gastroenterology Research and Practice, Article ID 659726, 8 pages http://dx.doi.org/10.1155/2014/659726 Clinical Study Transjugular Intrahepatic Portosystemic Shunt for the Treatment of Portal Hypertension
Gastroenterology Research and Practice, Article ID 659726, 8 pages http://dx.doi.org/10.1155/2014/659726 Clinical Study Transjugular Intrahepatic Portosystemic Shunt for the Treatment of Portal Hypertension
Originally Posted: November 15, 2014 BRUIT IN THE GROIN
 Originally Posted: November 15, 2014 BRUIT IN THE GROIN Resident(s): Donald ML Tse, MD Attending(s): KT Tan, MD Program/Dept(s): University Health Network/Mount Sinai Hospital, Toronto, ON, Canada CHIEF
Originally Posted: November 15, 2014 BRUIT IN THE GROIN Resident(s): Donald ML Tse, MD Attending(s): KT Tan, MD Program/Dept(s): University Health Network/Mount Sinai Hospital, Toronto, ON, Canada CHIEF
Management of Cirrhotic Patients Undergoing Non-Transplant Surgery
 Management of Cirrhotic Patients Undergoing Non-Transplant Surgery Jason S. Wakakuwa, M.D. Assistant Professor of Anesthesia Director, Transplant Anesthesia Beth Israel Deaconess Medical Center I have
Management of Cirrhotic Patients Undergoing Non-Transplant Surgery Jason S. Wakakuwa, M.D. Assistant Professor of Anesthesia Director, Transplant Anesthesia Beth Israel Deaconess Medical Center I have
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year