R1 orientation 蘇哲萱 2014/10/21
|
|
|
- Aron Morgan
- 5 years ago
- Views:
Transcription
1 R1 orientation 蘇哲萱 2014/10/21
2 I. Decompensated liver cirrhosis & associated complications II. GI Bleeding
3 Liver cirrhosis Compensate liver cirrhosis Decompensate liver cirrhosis
4 Prognosis of Liver cirrhosis Child pugh classification
5 Prognosis of Liver cirrhosis Child pugh classification HE None Gr 1~2 Gr 3~4 Ascites Absent slight Moderate Bilirubin <2 2~3 >3 mg/dl Albumin > ~3.5 <2.8 mg/dl PT prolong <4 s ( INR <1.7) 4~6 s( INR 1.7~2.3) >6 s (INR>2.3) Child A Child B Child C Total 5~6 7~9 10~15 1 year-survival 100 % 80 % 45 %
6 Complications of liver cirrhosis Variceal bleeding Ascites/ Spontaneous bacterial peritonitis Hepatic encephalopathy Hepatorenal syndrome Hepato-pulmonary syndrome / Hepatic hydrothorax
7 SPONTANEOUS BACTERIAL PERITONITIS
8 Spontaneous bacterial peritonitis Ascites fluid infection without an evident intra-abdominal surgically treatable source
9 Clinical manifestations Fever Abdominal pain Altered mental status Diarrhea/ paralytic ileus / Hypotension /Hypothermia
10 Diagnosis Paracentesis Ascites fluid PMN 250 Before any antibiotics What if traumatic paracentesis? Ascites routine: RBC 30 cells/mm3, WBC 500 cells/ mm3, 60 % Neutrophils ; monocyte 10 %, lymphocytes : 20 % SBP? RBC cells/mm3, WBC 500 cells/ mm3, 60 % Neutrophils ; monocyte 10 %, lymphocytes : 20 %, SBP?
11 In traumatic/bloody paracentesis Corrected neutrophil counts= Corrected PMN = PMN counts (RBC counts/250) RBC cells/mm3, WBC 500 cells/ mm3, 60 % Neutrophils ; monocyte 10 %, lymphocytes : 20 %, WBC: 500 * 0.6 = 300 Corrected PMN counts: 300 (60000/250) = 60 PMN/mm3
12 Diagnosis Paracentesis Routine Culture Gram stain Albumin Protein/Glucose/LDH Amylase Bilirubin
13 SAAG 1.1 g/dl Cirrhosis/ Heart failure, Portal hyperension SAAG < 1.1g/dL Peritoneal carcinomatosis, TB peritonitis, pancreatitis, nephrotic syndrome..
14 Diagnosis Protein/ LDH /Glucose Amylase (?) / Bilirubin (?) Runyon s criteria ( 2/3) Total protein > 1 gm/dl Glucose < 50 mg/dl (2.8 mmol/l) LDH > upper limit of serum
15
16
17 Treatment Antibiotics Tx Cefotaxime /3 rd cephalosporin Fluoroquinolone Discontinue non-selective beta-blocker

18
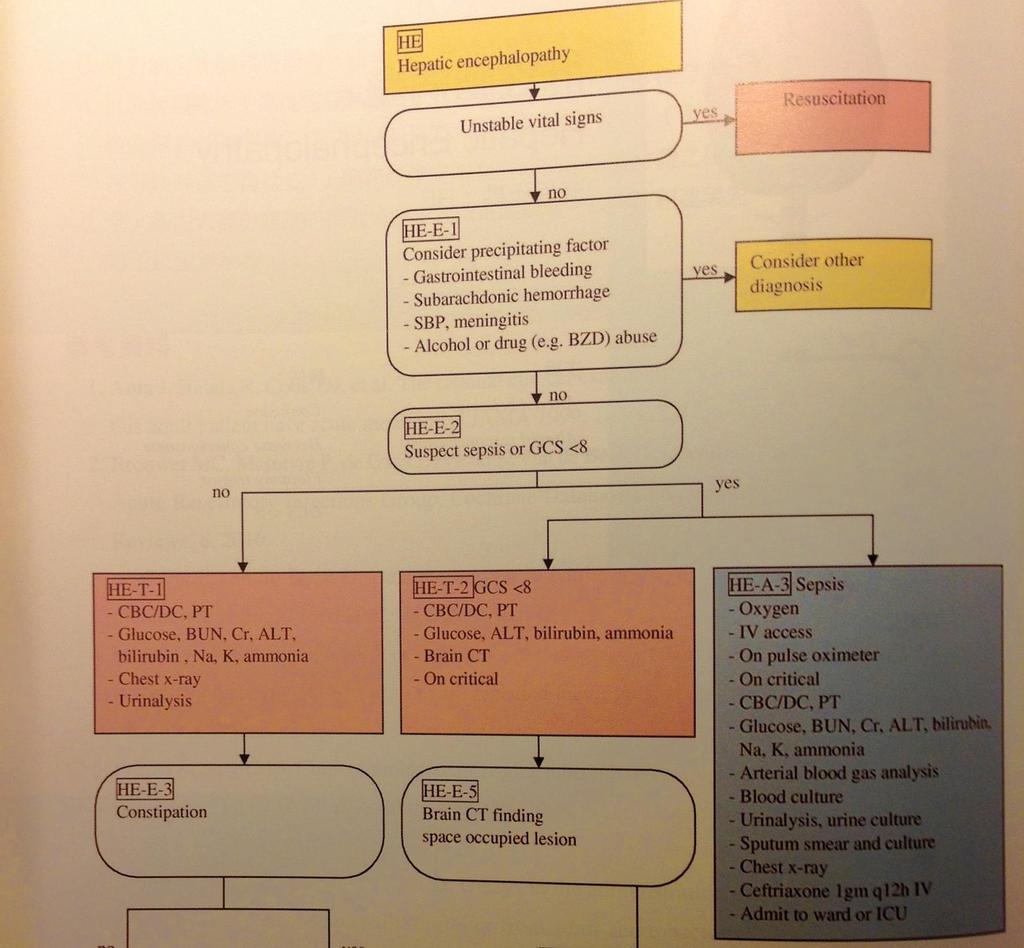
19 HEPATIC ENCEPHALOPATHY
20 Reversible syndrome of impaired brain function in advanced liver failure
21 Severity of HE Stage Mental status Asterixis EEG I Euphoria or depression, mild confusion, slurred speech, disordered sleep +/- Usually normal II Lethargy, moderate confusion + Abnormal III Marked confusion, incoherent speech, sleeping but arousable + Abnormal IV Coma; - Abnormal Delta activity
22 Finding precipitating causes GI bleeding Infection Electrolyte/ fluid status Sedative / transquilizer use Constipation Others
23 Common precipitants of Hepatic Encephalopathy Increase nitrogen load Gastrointestinal bleeding Excess dietary protein Azotemia Constipation Electrolyte and metabolic imbalance Hypokalemia Alkalosis Hypoxia Hyponatremia Hypovolemia Drugs Narcotics, tranquilizers, sedatives, Diuretics Miscellaneous Infection Surgery Superimposed acute liver disease Progressive liver disease Portal-systemic shunts
24 Treatment rationale Ammonia hypothesis Decrease ammoniagenic substrate Inhibition of ammonia production Metabolic ammonia removal False neurotransmitter hypothesis Branched chain amino acid supplementation Increased dopamine GABA hypothesis
25 Treament Control predisposing factors Decrease NH3 Lactulose / lactitol / rifaxim General supportive tx Fluid : adequate, avoid dehydration Electrolyte Pharmacologic restrain (haloperidol safer then BZD )
26 Lower Blood [NH3] Lactulose /lactitol / 30~45 ml BID ~ QID / day 2~3 stools / day Lactulose enemas Rifaximin (Gr 2C, 本院目前無藥 ) rifampin 400 mg TID / 550 mg BID in addition to lactulose Neomycin Ototoxicity / nephrotoxicity ; 500 mg TID / 1 gm BID ; metronidazole
27
28
29 Bar code HE IVF with D5W 1000 ml run 60ml/hr F/S stat CBC/DC Bun/Cr/Na/K/ Bil(T)/AST/ALT/NH3 CXR
30 HEPATORENAL SYNDROME
31 Diagnosis Renal failure in patient with advanced liver disease Type I Rapid decline renal function Cr elevated >2X (from baseline) to > 2.5 mg/dl <=2WKS Usually triggered by precipitating event with other organ dysfuction Type II Steady & progressive Characterized by refractory ascites & Na retension Average Cr around 2 mg/dl
32 Epidemiology Who is most affected With decompensated cirrhosis, precipitating as alcohol, hepatitis, or infection Incidence/Prevalence 4 % PT with decompensated cirrhosis 30 % PT with cirrhosis & SBP 45.8 % of PT with cirrhosis & renal failure
33 Pathogenesis Peripheral arterial vasodilation theory by cirrhosis/portal hypertension Splanchnic vasodilation, reduced arterial blood volume, decreased MAP RAA system activitaty renal vasoconstriction --< shift in renal autoregulatory curve Impaired CO due to cirrhosis cardiomyopathy Increased synthesis of vasoactive mediators affects renal blood flow or glomerular microcirculatory hemodynamics
34 Diagnosis Excluding other causes of AKD with advanced liver disease Major diagnositc criteria Cirrhosis with ascites Cr > 1.5 mg/dl No sustained improvement in Cr after 2 days of diuretic withdrawal and plasma volume expansion with albumin Absence of shock No current/recent use of nephrotoxic drugs No parenchymal renal disease (Proteinuria < 0.5g/d, no microhematuria, normal renal ultrasound
35 Tx Fluid restriction of 1L/day Prevent progression of dilutional hyponatremia in Type I hepatorenal dz Liver transplant / liver & renal transplant Tx prior to liver transplant Vasoconstriction + albumin Terlipressin level I» May increase CV events Large-volume paracentesis + albumin TIPS (transjugular intrahepatic portacaval shunts)
36 R1 orientation II GI Bleeding
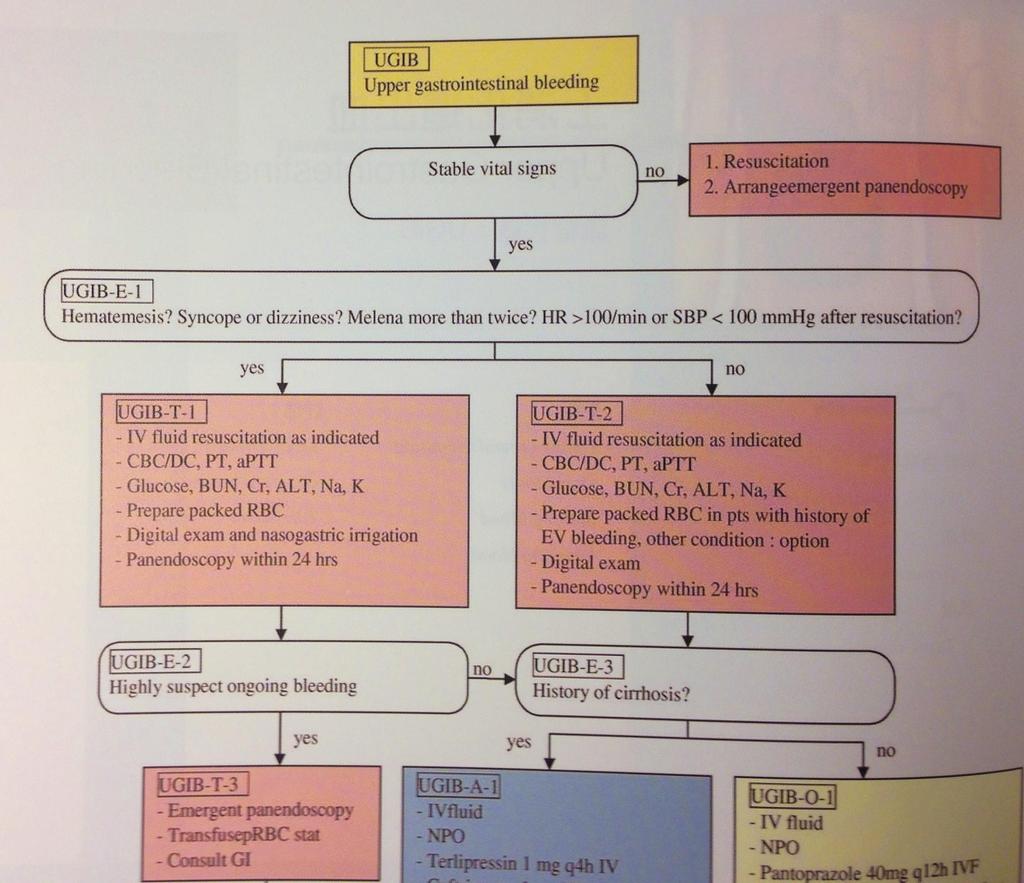
37 UGIB
38 Definitions Upper GI bleeding; Above Ligament of Treitz s
39 Symptoms/signs Melena Black, tarry, foul-smelling stools Hematemesis Vomitus of red blood of coffee-ground Hematochezia Passage of bright red/maroon blood from rectum
40 Etiology UGIB Varices Non-varices Ulcer, mallory-weiss tear, erosive lesion, gastritis, dieulafoy lesion.etc
41 Etiology UGIB Mimic Mimics LGIB Extra-intestinal blood loss /Epistaxis / gingival bleeding/ hemoptysis False positive fecal OB test
42 Approach to the patient Symptoms /signs; Shock sign, volume status Conscious /Pale/Cold sweating/weakness Abdominal pain Dizziness, palpitation, faintness, syncope others?
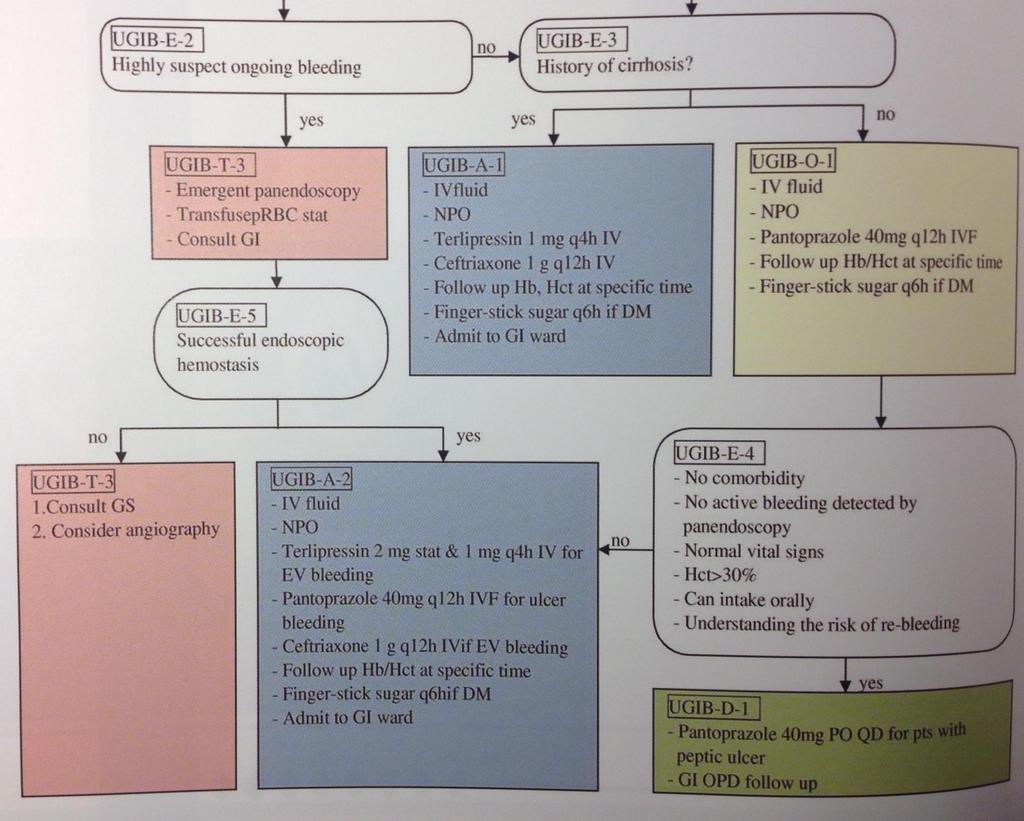
43 Evaluation/ tx plan Support & Stability Finding the DZ & treat it Others
44 Evaluation/ tx plan - UGIB Support & Stability Restoring volume loss/blood loss Correct bleeding tendency Finding the bleeding area & stop bleeding Medications Endoscopy Image study Others Electrolyte, nutrition, associated comorbidities
45 ABC Volume status Initial assessment

46 ABC Volume status Initial assessment
47 Evaluation and Tx Resuscitation / survey Barcode( UGIB) ; Medications tx PPI/ Terlipressin. PES Angiography Surgery
48 Barcode --UGIB Recheck BP 30 mins later NPO CBC/ DC/ PT/ Sugar / Bun/Cr/ALT/ Na/K IVF with N/S 1000 ml run 500 ml stat then run 120 ml/hr On NG tube with saline irrigation CXR Panendoscopy
49 Acid suppression Proton pump inhibitor (PPI) High dose with IV form rebleeding rate, length of stay, rebleeding rate, need for B/T with highrisk ulcers tx with endoscopy Barcode: HI LOSEC, HI PANTO (for hi-dose PPI) H2 blocker not been shown to significantly lower the rate of ulcer rebleeding
50 Terlipressin Vasoconstrictor therapy splanchnic blood flow Terlipressin Only agents improving control of bleeding/ survival in RCT & meta-analysis Regimen 2mg stat, 1mg Q4h~Q6H
51 Somatostatin analog Somatostatin & analogue gastroduodenal mucosal blood flow Octreotide 20~50 mcg bolus, then 25~50 mcg/hr drip x 3 ~5 days Somatostatin 2 amp in 500ml; 20 ml loading 2~3 mins, then 3.5 mg/kg/hr for 24 hrs;
52 Antibiotics Bacterial infection occurs in 20~50 % of patient with cirrhosis & GI bleeding; Prophylatic antibiotics reduce incidence of bacterial infection Ceftriaxone 1 gm/ QD 5~7 days Norfloxacin 400 mg BID
53 Evaluation and Tx Resuscitation / survey Barcode( UGIB/LGIB) ; fluid ; X-ray Medications tx PPI/ Terlipressin. PES Angiography Surgery
54 Prokinetics before PES Erythromycin Metoclopramide Improve gastric visualization at time of endoscopy, 30~ 90 mins before PES Usually with large amounts of blood in the stomach
55 Forrest Classification High risk A: spurting (Gr IA) B: Oozing (IB) C: Non-bleedling visible vessels (IIA) D: Adherent clot (IIB)
 F: Clean base (III)")
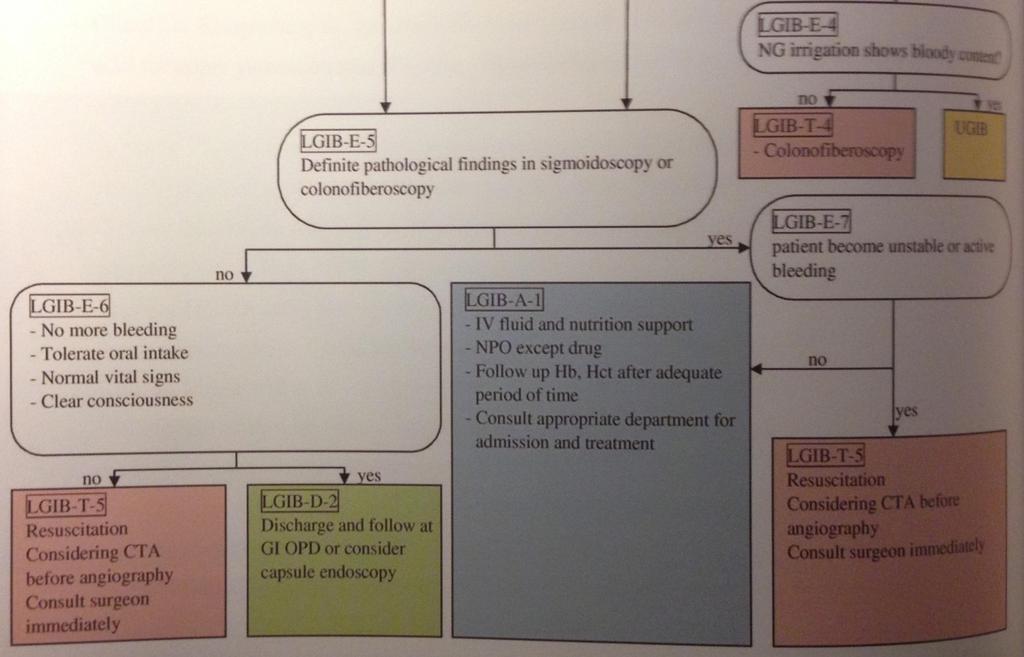
56 Forrest Classification Low risk E: flat, pigmented spot (IIC) F: Clean base (III)

 100 80")



57 Risk of re-bleeding by Forrest grade Patients with endoscopic or clinical re-bleeding (%) Forrest I* Forrest IIa Forrest IIb Forrest IIc Forrest III *Patients did not receive endoscopic therapy Laine L & Peterson WL. N Engl J Med 1994;331:717 27
58

59 Variceal Bleeding Occurs in 1/3 of patients with cirrhosis 1/3 initial bleeding episodes are fatal Among survivors, 1/3 will rebleed within 6 weeks Only 1/3 will survive 1 year or more
60 Tx of GI bleeding Resuscitation / survey Barcode( UGIB/LGIB) ; fluid ; X-ray Medications tx PPI/ Terlipressin. PES Angiography Surgery
61 UGIB
62
63 LGIB
64 Definition Lower GI bleeding; Below Ligament of Treitz s
65 Symptoms/signs Melena Black, tarry, foul-smelling stools Hematemesis Vomitus of red blood of coffee-ground Hematochezia Passage of bright red/maroon blood from rectum
66 Common Etiology LGIB Colonic diverticular bleeding GI Angiodysplasia Hemorrhoid Intestinal dieulafoy Colitis (IBD/infection/ischemic ) Neoplasm Dieulafoy lesion
67 Approach to the patient Symptoms /signs; Shock sign, volume status Conscious /Pale/Cold sweating/weakness Dizziness, palpitation, faintness, syncope Abdominal pain / back pain Others : Hx, associated cormobidity..
68 Evaluation / Tx of LGIB ABC, stable vital sign;
69 Current Barcode - LGIB CBC / PT ; Cr/ ALT/ Na/ K On BP monitor & EKG monitor ; O2 N/C 5L/min Admission to GI ward IVF with N/S 1000 ml run stat then run 120 ml/hr Sigmoidscopy, flexible Fleet enema 2 PC before sigmoid
70 Evaluation & Tx of LGIB Sigmoidscopy Colonfiberscopy Need bowel preparation
71 Tx of LGIB Colonfiberscopy Angiography Surgery Others Hormone tx, angiogenesis inhibitors (thalidomide) Octreotide Long-acting form of octreotide (IM/month)
72 LGIB
73
74 CASE
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Program Disclosure. This program is supported by an educational grant from Salix Pharmaceuticals.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis
 The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/enlarged/ Daniel Giddings,
The Use of Albumin for the Prevention of Hepatorenal Syndrome in Patients with Spontaneous Bacterial Peritonitis and Cirrhosis http://www.funnyjunk.com/funny_pictures/1743659/enlarged/ Daniel Giddings,
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
CHAPTER 7. End Stage Liver Disease in the ICU: Walking a Tightrope. Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing
 CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CONTROLLED DOCUMENT. Cirrhosis Care Bundle CATEGORY: Clinical Guidelines. CLASSIFICATION: Clinical. Controlled Document CG201 Number:
 Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Gastrointestinal bleeding definitions (I)
") definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
Optimal management of ascites
 Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Care of the Patient With Cirrhosis
 REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Management of Hepatic Encephalopathy
 Management of Hepatic Encephalopathy Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH
Management of Hepatic Encephalopathy Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH
Complications of Cirrhosis
 What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
What is Cirrhosis? Complications of Cirrhosis Paul J. Gaglio, MD Center for Liver Disease and Transplantation Columbia University College of Physicians and Surgeons NAFLD 1 PHYSICAL EXAM FINDINGS Decreased
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Sign up to receive ATOTW weekly -
 HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
Guidelines for the Management of Upper gastrointestinal bleeding
 Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS
 INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS Yoshida H et al (1993)* Deschenes M et al (1999)** Strauss E et al (1993) Borzio M et al (2002) PATIENTS 1140 140 170 405 INFECTIONS 15.4% 20% 47% 34% * Many
INCIDENCE OF BACTERIAL INFECTIONS IN CIRRHOSIS Yoshida H et al (1993)* Deschenes M et al (1999)** Strauss E et al (1993) Borzio M et al (2002) PATIENTS 1140 140 170 405 INFECTIONS 15.4% 20% 47% 34% * Many
Topics to be covered
 Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Management of Hospitalized Patients with Cirrhosis
 Disclosure Management of Hospitalized Patients with Cirrhosis Research Support: Gilead, Genfit, Conatus and Intercept Advisory: Gilead Bilal Hameed, MD Associate Professor of Medicine Division of Transplant
Disclosure Management of Hospitalized Patients with Cirrhosis Research Support: Gilead, Genfit, Conatus and Intercept Advisory: Gilead Bilal Hameed, MD Associate Professor of Medicine Division of Transplant
REVIEW. Ariel W. Aday, M.D.,* Nicole E. Rich, M.D.,* Arjmand R. Mufti, M.D., and Shannan R. Tujios, M.D.
 REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
REVIEW CON ( The Window Is Closed ): In Patients With Cirrhosis With Ascites, the Clinical Risks of Nonselective beta-blocker Outweigh the Benefits and Should NOT Be Prescribed Ariel W. Aday, M.D.,* Nicole
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
Pharmacology in Liver Disease. Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant
 Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
Pharmacology in Liver Disease Sandeep Whitehead Advanced Clinical Pharmacist Hepatology and Liver Transplant Objectives Outline the drug management for patients with: Ascites Spontaneous Bacterial Peritonitis
Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A Retrospective Study
 Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
CLIF Consortium. Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study
 Core Study") CLIF Consortium Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study Case Report Form (Final) Center: Investigator: Investigator s Signature: The highlighted information
CLIF Consortium Protocol of the CLIF Acute-oN-ChrONic LIver Failure in Cirrhosis (CANONIC) Core Study Case Report Form (Final) Center: Investigator: Investigator s Signature: The highlighted information
Colon ischemia. Bible class 12 September Stefan Christen. ACG Clinical Guideline: Am J Gastroenterol 2015
 Colon ischemia Bible class 12 September 2018 Stefan Christen ACG Clinical Guideline: Am J Gastroenterol 2015 Definition Definition Imbalance between blood supply and metabolic demands of the colonocytes
Colon ischemia Bible class 12 September 2018 Stefan Christen ACG Clinical Guideline: Am J Gastroenterol 2015 Definition Definition Imbalance between blood supply and metabolic demands of the colonocytes
PALLIATIVE CARE IN END-STAGE LIVER DISEASE
 PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
PALLIATIVE CARE IN END-STAGE LIVER DISEASE Ken S. Ota, DO Family Medicine Banner Good Samaritan Medical Center Learning Objectives: Describe the common bio-psycho-social issues in end-stage liver disease
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
GASTROINTESTINAL BLEEDING. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding
 ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington