An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors
|
|
|
- Frederick Patterson
- 5 years ago
- Views:
Transcription
1 An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Boston, MA An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors INTRODUCTION 8 FNA CASES WITH CORRESPONDING HISTOLOGY Celeste N. Powers, M.D., Ph.D. Medical College of Virginia Richmond, VA SALIVARY GLAND FNA Because of the wide range of non-neoplastic and neoplastic lesions, and the cytologic overlap between many benign and malignant tumors, salivary gland FNA is probably the MOST CHALLENGING area of cytopathology. Salivary Gland Lesions Non-Neoplastic Acute sialadenitis Chronic sialadenitis LESA HIV-associated lymphoepithelial lesion Reactive lymph nodes Mucocele Mucinous metaplasia Sialadenosis Lipoma Hemangioma Branchial cleft cyst Neoplastic Benign Pleomorphic adenoma Basal cell adenoma Warthin s tumor Oncocytoma Low-Grade Mucoepidermoid carcinoma, low-grade Acinic cell carcinoma Polymorphous low-grade adenocarcinoma Basal cell adenocarcinoma Epithelial-myoepithelial carcinoma MALT lymphoma High-Grade *Adenoid cystic carcinoma Salivary duct carcinoma Mucoepidermoid carcinoma, high-grade Ca-ex-pleomorphic adenoma Clear cell carcinoma Large B-cell Lymphoma SALIVARY GLAND FNA CHALLENGING DIAGNOSTIC ISSUES Matrix-containing tumors Oncocytic lesions Basaloid tumors Lymphoid lesions Cystic and mucinous lesions High-grade carcinomas Clear cell tumors Spindle cell lesions 1


2 SALIVARY GLAND FNA Rationale and Indications for FNA: Any unexplained salivary gland mass Safe, cost-effective, accurate Guide the clinical management/pre-op strategy:» Non-neoplastic» Benign tumor or low-grade carcinoma» High-grade carcinoma SALIVARY GLAND FNA Sample Preparation: Both Romanowsky and Papanicolaou stained preparations are essential! SALIVARY GLAND FNA SALIVARY GLAND FNA Accuracy: High accuracy for non- neoplastic vs neoplastic High accuracy for low-grade vs high-grade Variable accuracy for a specific entity: High for pleomorphic adenoma Low for basal cell adenocarcinoma Usually Specific Diagnosis Pleomorphic adenoma Warthin s tumor Acute and chronic sialadenitis Basal cell adenoma, membranous type Reactive lymph node Lymphoma Sometimes Specific Diagnosis Adenoid cystic carcinoma LG mucoepidermoid carcinoma Carcinoma ex PA Metastasis Small cell carcinoma Mucocele Oncocytoma LESA Usually Descriptive Diagnosis Basal cell adenoma, tubulotrabecular and solid types HG mucoepidermoid carcinoma Salivary duct carcinoma Polymorphous low-grade adenocarcinoma Basal cell adenocarcinoma Epithelial-myoepithelial carcinoma Acinic cell carcinoma SOME SALIVARY GLAND FACTS FEATURES OF THE NORMAL SALIVARY GLAND 3 Major glands (ectodermally derived): Parotid (serous) Submandibular (mixed seromucinous) Sublingual (mucinous) Minor glands: Submucosa of oral cavity Seromucinous glands of the nasal cavity, larynx, and bronchi Tumors: per 100,000 people Older adults, females, parotid gland, approx. 75% are benign Risk of malignancy is inversely proportional to the size of the gland (20% in parotid; 80-89% in oral cavity) 2





3 HISTOLOGIC FEATURES OF THE NORMAL SALIVARY GLAND HISTOLOGIC FEATURES OF THE NORMAL SALIVARY GLAND HISTOLOGIC FEATURES OF THE NORMAL SALIVARY GLAND HISTOLOGIC FEATURES OF THE NORMAL SALIVARY GLAND HISTOLOGIC FEATURES OF THE NORMAL SALIVARY GLAND FNA OF THE NORMAL SALIVARY GLAND Cytologic Features of the Normal Aspirate Serous and mucinous-type acinar cells in lobules Background naked acinar cell nuclei Few admixed small sheets and tubules of ductal epithelium Intercalated ducts Striated ducts Excretory duct Adipose tissue 3






4 FNA OF THE NORMAL SALIVARY GLAND Polarized grape-like clusters of acinar cells NORMAL SALIVARY GLAND FNA Key Pitfall of the Normal Aspirate: Misinterpreting normal acinar cells as acinic cell carcinoma FNA OF THE NORMAL SALIVARY GLAND - PITFALL SALIVARY GLAND FNA CASES Normal Salivary Gland Acinic Cell Carcinoma History: CASE 1 A 31 year old woman with a 1.5 cm nontender right parotid mass that has been slowly enlarging over the past year. 4




5 Case 1 Pleomorphic Adenoma aka Benign Mixed Tumor Diff-Quik Stain Pap Stain Matrix Tumors Pleomorphic Adenoma Adenoid Cystic Carcinoma Monomorphic Adenomas Carcinoma Ex Pleomorphic Adenoma Pleomorphic Adenoma Most common of all salivary gland tumors in both children and adults 75% of parotid tumors & 50% of all salivary tumors Superficial parotid gland is most common site esp. the tail of the parotid at jaw angle Firm, moveable, well demarcated (encapsulated), slow growing, painless 5












6 Cells Biphasic Tumor Epithelial cells arranged in cohesive, honeycomb groups Myoepithelial cells arranged singly and haphazard clusters. Cells may be plasmacytoid, epithelioid, spindled, or clear Matrix Fibrillar with frayed, indistinct margins Chrondromyxoid (Metachromatic) Embedded myoepithelial cells Infarction: Spontaneous vs Aspiration 6
 Epithelial predominant (basaloid tumors) Focal adenoid cystic like areas")

 FNAB is often reported as painful Cribriform, tubular,")

7 Pitfalls Cellular lesions with sparse or absent matrix Myoepithelial predominant (myoepithelioma) Epithelial predominant (basaloid tumors) Focal adenoid cystic like areas Matrix mimics Cytologic atypia Metaplasia Squamous Mucinous Squamous Metaplasia Adenoid Cystic Carcinoma 4-10% of all salivary gland neoplasms Relatively slow growing with perineural invasion and poor long-term survival Submandibular gland, palate, and parotid 4 th to 7 th decade, women > men (3:2) FNAB is often reported as painful Cribriform, tubular, and solid forms Adenoid Cystic Carcinoma Cells Basaloid cells with dark angulated nuclei Variable atypia Matrix 3-D spheres and branching structures Acellular hyaline globules Metachromatic with sharp borders 7




8 Adenoid Cystic Carcinoma Pleomorphic Adenoma vs Adenoid Cystic Carcinoma Pleomorphic Adenoma - predominance of myoepithelial cells - atypia - matrix is fibrillar with ragged edges and myoepithelial cells embedded within Adenoid Cystic Ca - cells more basaloid in appearance - minimal atypia - unique matrix: acellular, smooth edges, homogeneous hyaline globules Pleomorphic Adenoma vs. Adenoid Cystic Carcinoma Final Comments Pleomorphic adenoma Adenoid cystic carcinoma Pleomorphic adenoma, monomorphic adenoma and adenoid cystic carcinoma can overlap significantly History: slow vs rapid growth presence or absence of pain Matrix: fibrillar arrays +/-embedded cells homogenous acellular globules CASE 2 History: A 71 year old man with a l.5 cm right nontender submandibular mass that had been slowly increasing in size for 1.5 years. 8





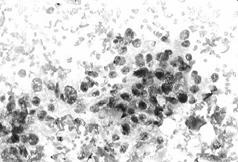
9 Case 2 Acinic Cell Carcinoma Acinic Cell Carcinoma Second most common salivary gland malignancy 2-6% of all salivary gland neoplasms Low-grade malignancy recapitulating growth of normal acinous cells 6.5% of neoplasms, 18% of malignant F>M, 90% parotid Acinic Cell Carcinoma Well demarcated/encapsulated, lobulated, Slow growing Growth patterns Solid & microcystic (common); papillary-cystic; follicular variants Complete surgical excision 12% local recurrence; 8% mets, 6% pts die 9






10 Acinic Cell Carcinoma Cells (high cellularity) Serous type acinar cells, predominate Intercalated duct cells Background Naked nuclei + lymphocytes Clean may be cystic Psammoma bodies (papillary) Capillary meshwork Acinic Cell Carcinoma Serous type acinar cells Sheets and dyshesive 3-D clusters Large polygonal cells with abundant finely vacuolated to granular basophilic cytoplasm PAS+D resistant cytoplasmic zymogen granules Bland nuclear cytologic features some are higher grade. Acinic Cell Carcinoma Intercalated duct cells Cohesive ductal cells with moderate to scant cytoplasm Papanicolaou stain Diff Quik stain Acinic Cell Carcinoma, papillary-papillocystic Pitfalls Misinterpreting normal acinar cells as acinic cell carcinoma Misinterpreting metastatic carcinoma as acinic cell carcinoma 10
 Head")


11 Normal Salivary Gland Normal Salivary Gland vs. Acinic Cell Carcinoma Acinic Cell Carcinoma Metastatic Tumors Uncommon Intraparotid lymph nodes Clinical history in 70% of cases Skin cancers (SCC, basal cell, MM) Head and neck SCC Sebaceous carcinoma Small cell carcinoma Lymphoma Renal cell carcinoma Metastatic Renal Cell Carcinoma vs. Acinic Cell Carcinoma Renal cell carcinoma: Clinical history of cancer Evidence of lymph node involvement CD10+, RCC+, EMA+, CK7-, PAS+ Acinic cell carcinoma: Primary salivary tumor May have lymphocytes CD10-, RCC-, EMA +, CK7+, PAS + D granules Metastatic Renal Cell Carcinoma vs. Acinic Cell Carcinoma Acinic Cell Carcinoma Renal Cell Carcinoma Oncocytic Tumors Acinic Cell Carcinoma Warthin Tumor Oncocytoma Mucoepidermoid carcinoma (oncocytic variant) Metastatic Renal Cell Carcinoma Warthin Tumor Second most common salivary gland tumor 5-10% of all salivary gland neoplasms Bilateral, men> women, fluctuant mass Doughy on palpation Thick brown-green granular fluid machine oil 11


")


12 Warthin Tumor Cells Oncocytic, 2-D sheets Lymphocytes, germinal centers Background Mucoid, mucinous or watery Granular or dirty or machine oil Cholesterol crystals Warthin Tumor Variable cellularity Oncocytes large cells, abundant cytoplasm (squamous/glandular metaplasia eccentric nuclei, prominent nucleoli Lymphocytes heterogeneous (plasma cells, small lymphs) occasional germinal centers, DNA artifact Warthin Tumor Pitfalls Squamous metaplasia in Warthin Tumor may be mistaken for squamous cell carcinoma WT lacks overtly malignant features of SCCa Abundant oncocytes in Warthin Tumor may be mistaken for an oncocytic neoplasm Papanicolaou Stain Diff-Quik Stain 12







13 Squamous Metaplasia Oncocytoma Circumscribed nodule Fibrous capsule Parotid gland May be bilateral Cells Oncocytes 2-D and 3-D groups Homogeneous granular cytoplasm without vacuoles Background No lymphocytes Clean Acinic Cell Carcinoma vs. Oncocytoma Acinic Cell Carcinoma Vacuolated cytoplasm Delicate, slightly basophilic cytoplasm Variable atypia PAS + D granules PTAH negative Oncocytoma No cytoplasmic vacuoles Dense, granular eosinophilic cytoplasm Minimal to absent atypia No PAS + D granules PTAH positive Oncocytoma Final Comments Common problem Normal vs Warthin tumor vs Acinic cell ca Clinical information is very helpful History of primary Fluctuant, recurrent vs firm and fixed Pattern vs cytomorphology Monomorphic vs biphasic population Sheets vs papillae Granular vs vacuolated cytoplasm 13



14 CASE 3 History: A 45 yo man with a 6 month history of a 3.7 cm mildly painful, enlarging left parotid gland mass. An MRI showed a nodular, slightly irregular lesion with variable signal intensity located in the superficial parotid gland just lateral to the facial nerve. An FNA was performed. CASE 3 CYTOLOGIC DIAGNOSIS: BASALOID NEOPLASM WITH MILD ATYPIA, FAVOR BASAL CELL ADENOMA. SEE NOTE. Note: The differential diagnosis includes basal cell adenoma and basal cell adenocarcinoma; however, a more aggressive basaloid neoplasm cannot be entirely excluded. CASE 3 SURGICAL RESECTION: Superficial parotidectomy was performed. A frozen section performed at the time of surgery also favored a basal cell adenoma. 14

 Distinguished by histologic evidence of invasion CANNOT DISTINGUISH BY FNA!")
15 CASE 3 HISTOLOGIC DIAGNOSIS: BASAL CELL ADENOCARCINOMA, 3.7 CM, SOLID TYPE. Clinical follow-up: The patient has been free of disease for 6 years. BASAL CELL ADENOCARCINOMA Rare, low-grade salivary gland neoplasm Approximately 2% of malignant salivary gland tumors Parotid gland, rarely in submandibular gland Average age: 60 years (range: years) Good prognosis: Local recurrence (35%), infrequent metastatic disease (10%), and low mortality (3%) Complete surgical excision with disease-free margins BASAL CELL ADENOCARCINOMA Malignant counterpart of basal cell adenoma (aka monomorphic adenoma) Distinguished by histologic evidence of invasion CANNOT DISTINGUISH BY FNA! 3 Patterns: Solid, tubulotrabecular, and membranous May be associated with synchronous dermal tumors BASAL CELL ADENOMA & ADENOCARCINOMA Histologic Features: Basaloid cells - Small dark cells - usually peripheral Larger pale cells Palisading of the small dark cells Conspicuous hyaline membranes of basal lamina surround nests Intercellular hyaline droplets Small tubules lined by cuboidal cells Squamous morules BASAL CELL ADENOMA & ADENOCARCINOMA: Membranous Type 15





16 BASAL CELL ADENOMA & ADENOCARCINOMA: Membranous Type BASAL CELL ADENOMA & ADENOCARCINOMA: Synchronous Cutaneous Cylindroma BASAL CELL ADENOMA & ADENOCARCINOMA: Tubulotrabecular Type BASAL CELL ADENOMA & ADENOCARCINOMA: BASAL CELL ADENOMA & ADENOCARCINOMA: Solid Type BASAL CELL ADENOMA & ADENOCARCINOMA Peripheral palisading 16




17 BASAL CELL ADENOMA & ADENOCARCINOMA BASAL CELL ADENOMA & ADENOCARCINOMA Squamous morule BASAL CELL ADENOMA & ADENOCARCINOMA BASAL CELL ADENOMA & ADENOCARCINOMA: Myoepithelial Markers Calponin Keratin SM Actin S100 P63 BASAL CELL ADENOMA VS. ADENOCARCINOMA Malignancy is based upon finding histologic evidence of infiltrative growth into salivary gland parenchyma and soft tissue. 25% of carcinomas show perineural or lymphovascular invasion. BASAL CELL ADENOMA & ADENOCARCINOMA Cytologic Features: Two populations of basaloid cells - Small oval cells with scant cytoplasm Bland dark nuclei Haphazard arrangement in cohesive groups Absence of marked nuclear atypia Peripheral palisading Squamous morules Peripheral ribbons & intercellular droplets of dense, nonfibrillary, acellular matrix Metachromatic by Romanowsky stains, cyanophilic by Pap stain 17





18 Basal Cell Adenoma & Adenocarcinoma: 3 Subtypes - Solid, tubulotrabecular and membranous BASAL CELL ADENOMA & ADENOCARCINOMA: Membranous Type BASAL CELL ADENOMA & ADENOCARCINOMA: Solid Type Squamous Morule BASAL CELL ADENOMA & ADENOCARCINOMA DIFFERENTIAL DIAGNOSIS Adenoid cystic carcinoma Polymorphous low-grade adenocarcinoma Cellular pleomorphic adenoma Chronic sialadenitis Cutaneous basal cell carcinoma Metastatic basaloid squamous carcinoma Basal Cell Tumor vs Adenoid Cystic Carcinoma Solid Basal Cell Tumor vs Solid Adenoid Cystic Carcinoma Features favoring basal cell tumor: Peripheral bands of matrix Intercellular matrix globules Dual cell population Peripheral palisading Squamous morules Bland cytology Basal cell adenoma Adenoid cystic carcinoma 18




19 BASAL CELL ADENOMA & ADENOCARCINOMA In the final analysis, it may not always be possible to make a specific diagnosis. Rather, a diagnosis favoring a basal cell tumor with a note explaining the differential diagnosis. Polymorphous Low-Grade Adenocarcinoma Minor salivary glands, esp. palate Circumscribed subepithelial mass Resembles infiltrating lobular breast carcinoma Histologic Features: Diverse architecture: solid, trabecular, cords/single file, ductular, tubular, papillary, cystic, cribriform Concentric whorling appearance Few myoepithelial cells, minimal atypia, & absence of myxochondroid matrix Infiltrative growth Prominent neurotropism without necrosis Polymorphous Low-Grade Adenocarcinoma Polymorphous Low-Grade Adenocarcinoma Polymorphous Low-Grade Adenocarcinoma Polymorphous Low-Grade Adenocarcinoma 19






20 Polymorphous Low-Grade Adenocarcinoma Polymorphous Low-Grade Adenocarcinoma Cellular Pleomorphic Adenoma Chronic Sialadenitis: Kuttner Tumor Features favoring PA: Matrix is fibrillar and contains cells Absence of peripheral palisading Predominance of myoepithelial cells/absence of two basaloid cell populations Chronic Sialadenitis Hypocellular with small basaloid groups and background chronic inflammation. Final Comments Most difficult diagnostic problem in the salivary gland Often a descriptive diagnosis Basal cell adenocarcinoma and adenoma are cytologically indistinguishable: 2 populations of basaloid cells Peripheral matrix ribbons and intercellular globules Squamous morules Palisading The DDX includes adenoid cystic carcinoma. 20


21 CASE 4 History: A 49 year-old woman with a several year history of rheumatoid arthritis presents with a markedly enlarged left parotid gland. By clinical exam, the parotid gland was diffusely firm; however, a discrete mass was not identified. An FNA was performed. The initial working diagnosis based upon rapid interpretation included reactive lymph node, chronic sialadenitis, LESA, and lymphoma. Therefore material for flow cytometry was sent and was negative for lymphoma. CASE 4 Cytologic Diagnosis: LYMPHOEPITHELIAL SIALADENITIS (LESA) 21

 LYMPHOEPITHELIAL SIALADENITIS (LESA) Cytologic Features: Cellular aspirate Mixed population")
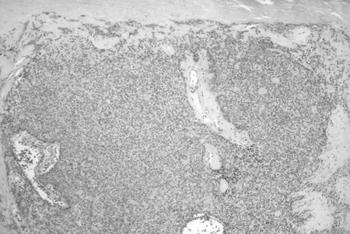
22 LYMPHOEPITHELIAL SIALADENITIS (LESA) Variety of names: Benign lymphoepithelial lesion Myoepithelial sialadenitis (MESA) Mikulicz s disease Often associated with Sjogren s syndrome, rheumatoid arthritis or other autoimmune disorders Can be unilateral, bilateral, solid, or cystic Increased risk of B-cell lymphoma, esp. MALT-type LYMPHOEPITHELIAL SIALADENITIS (LESA) Histologic Features: Lymphocytic infiltration of gland with parenchymal atrophy T-lymphocytes, plasma cells, and monocytoid B-cells Variable germinal center formation Ductal hyperplasia to form lymphoepithelial lesions LYMPHOEPITHELIAL SIALADENITIS (LESA) LYMPHOEPITHELIAL SIALADENITIS (LESA) Cytologic Features: Cellular aspirate Mixed population of lymphocytes and plasma cells Germinal center fragments Tingible body macrophages Lymphoepithelial lesions Absence of acinar cells A key pitfall in the diagnosis of LESA is metastatic squamous cell carcinoma. SCC LESA Differential Diagnosis of LESA Chronic sialadenitis Reactive intraparotid lymph node Lymphoepithelial carcinoma Metastatic squamous cell carcinoma B-cell lymphoma MALT Follicular Diffuse large B-cell 22



23 Epithelial Salivary Gland Tumors with Lymphocytes Warthin tumor Mucoepidermoid carcinoma Acinic cell carcinoma Lymphoepithelial carcinoma Metastatic carcinoma LESA vs. Chronic Sialadenitis Chronic Sialadenitis differs from LESA by: Hypocellularity Fewer lymphocytes and germinal centers Smaller angulated groups rather than sheets Absence of lymphoepithelial lesions LESA vs. Lymphoma Immunophenotyping is essential for distinguishing LESA from lymphoma, especially MALT lymphoma. Salivary Gland Lymphomas 2-5% of salivary gland neoplasms Parotid is most frequently involved Most are B-cell NHL MALT is the most common DLBCL Follicular lymphoma primarily in parotid LNs MALT LYMPHOMA MALT LYMPHOMA 23



24 Salivary Gland Lymphomas MALT Follicular DLBCL Small lymphs, centrocytes, monocytoid B cells Slight nuclear atypia CD20+, 23-, 10-, 5-, cyclin D1-, bcl2+, bcl6- Mixed small & large Notched and grooved nuclei CD20+, 23-, 10+, 5-, bcl2+, bcl-6+ May be CD10- T(14:18) by FISH Large size: Immunoblasts & centroblasts Marked atypia CD20+, keratin -, S-100- Final Comments A characteristic feature of LESA is the lymphoepithelial lesion. The differential diagnosis of lymphoid lesions in the salivary gland includes non-neoplastic and benign conditions, B-cell lymphoma, and carcinoma. Without ancillary studies, LESA can be impossible to distinguish from MALT lymphoma. History: Case 5 A 58 year old man with a 2.0 cm nontender, enlarging left parotid gland mass. 24





 Intermediate cells (low")

25 Case 5 Mucoepidermoid Carcinoma Mucoepidermoid Carcinoma Low Grade Most common salivary gland in children Second only to PA in frequency in adults M=F; Age range: years Usually slow growing and painless Residual mass post aspiration Mucoepidermoid Carcinoma Low Grade Cells (variable cellularity, sheets) Mucous containing epithelial cells Epidermoid cells (squamous features) Intermediate cells (low N/C ratio) Background Mucinous often with cellular debris 25








26 Low-Grade Mucoepidermoid Carcinoma Low-Grade Mucoepidermoid Carcinoma Low-Grade Mucoepidermoid Carcinoma Intermediate cells Cystic Lesions Low grade mucoepidermoid carcinoma Branchial cleft cyst Lymphoepithelial cyst Salivary duct cyst/retention cyst Cystic squamous cell carcinoma 26

 Type I ectodermal only Type II ectodermal and mesodermal (cartilage) Non")

27 Mucocele/Retention Cyst Low-Grade Mucoepidermoid Carcinoma vs Mucocele Low grade mucoepidermoid carcinoma is the most common cause of false negative salivary gland diagnoses: Low cellularity due to cyst Bland cytology of cells Mucin cells resemble foamy histiocytes Branchial Cleft Cyst Branchial Cleft Cyst Usually present in young adults Lateral neck along SCM muscle, around external ear 1st branchial cleft (parotid) Type I ectodermal only Type II ectodermal and mesodermal (cartilage) Non tender fluctuant masses Pap Stain Diff-Quik Stain Final Comments Search for three cell types (mucus, intermediate, squamous) to distinguish LG MEC from Tumors with squamous or mucinous metaplasia Beware making a definitive diagnosis when aspirates are hypocellular 27








28 Case 6 History: 52 year old man presented with a rapidly enlarging right parotid gland mass. The lesion is painful, and the patient has symptoms of facial nerve involvement. Case 6 Salivary Duct Carcinoma Diff-Quik Stain Pap Stain Salivary Duct Carcinoma Uncommon Clinically aggressive Parotid in elderly men Resembles high-grade comedo-type ductal carcinoma of the breast 28






 Clinically")

29 Salivary Duct Carcinoma Cells Overtly malignant cytomorphology Sheets, clusters, papillae, cribriform groupings Polygonal with abundant vacuolated cytoplasm Large hyperchromatic, pleomorphic nuclei Prominent nucleoli Background Necrosis Salivary Gland Duct Ca High-Grade Carcinomas High-grade carcinomas Salivary Duct Carcinoma Mucoepidermoid Carcinoma Carcinoma Ex Pleomorphic Adenoma Squamous Cell Carcinoma Salivary duct ca High-grade MEC Ca Ex PA Mucoepidermoid Carcinoma High- Grade Most common malignant salivary gland tumor (2 nd in frequency to PA) Clinically aggressive: rapidly enlarging and painful Parotid in elderly men Resembles high-grade comedo-type ductal carcinoma of the breast 29

")


")
30 Mucoepidermoid Carcinoma High- Grade Cells High cellularity, obvious malignant features Epithelial cells in clusters and singly Little distinction between squamous and glandular cells Pleomorphism, prominent nucleoli Background Variable necrosis and/or cystic component (mucinous) Malignant Mixed Tumor Rare, occurs in 5-9% of pleomorphic adenomas Pre-existent pleomorphic adenoma Sudden rapid growth in salivary gland mass present for considerable time Three types Carcinoma ex pleomorphic adenoma Carcinosarcoma Metastasizing mixed tumor Carcinoma Ex Pleomorphic Adenoma Cells High-grade carcinoma with pre-existent PA Sheets and aggregates of malignant cells Background Matrix (associated with PA) associated with HG Carcinoma Necrosis 30

 Cells Squamous Cell Carcinoma, High-Grade Sheets and")


")

31 Squamous Cell Carcinoma Rare salivary gland primary Metastases from H&N often cystic High-grade non-keratinizing squamous cell carcinoma often indistiguishable from high-grade primaries (esp. MEC) Cells Squamous Cell Carcinoma, High-Grade Sheets and aggregates of malignant cells Pleomorphic nuclei with coarse chromatin Distinct nucleoli Background Necrosis and cell debris (+/- keratin) Inflammation Squamous Cell Carcinoma, Primary Squamous Cell Carcinoma, Metastatic Final Comments The presence of matrix suggests Ca ex PA The combination of squamoid cells and rare mucin+ cells favors MEC (cell block is useful) Keratinization favors a metastasis over MEC Salivary duct carcinomas resemble high-grade breast cancers with comedo necrosis they can be mucin + 31


32 CASE 7 History: A 69 year-old woman presented with a slowly enlarging, non-tender, 2.0 cm parotid gland mass. An FNA was performed. CASE 7 Cytologic Diagnosis: LOW-GRADE BIPHASIC SALIVARY GLAND NEOPLASM WITH ABUNDANT MYOEPITHELIAL CELLS. SEE NOTE. Note: The DDX includes epithelial-myoepithelial carcinoma and cellular pleomorphic adenoma. The tumor was surgically excised by superficial parotidectomy. 32
 M:F = 1:2 Low-grade")


33 CASE 7 Epithelial-Myoepithelial Carcinoma Histologic Diagnosis: EPITHELIAL-MYOEPITHELIAL CARCINOMA Rare - 1% of all salivary gland tumors Parotid gland Average age: 62 years (range: years) M:F = 1:2 Low-grade malignancy; locally aggressive Excellent prognosis Epithelial-Myoepithelial Carcinoma Epithelial-Myoepithelial Carcinoma Histologic Features: Biphasic: myoepithelial cells and intercalated duct-type cells Multinodular and hyalinized stroma Eosinophilic, PAS+ luminal material Solid, organoid, cystic, and nested patterns Infiltrative growth Variable atypia, necrosis, and mitoses Epithelial-Myoepithelial Carcinoma Epithelial-Myoepithelial Carcinoma 33



34 Epithelial-Myoepithelial Carcinoma Epithelial-Myoepithelial Carcinoma Cytologic Features: Cellular Biphasic: sheets and spheres of cells: Myoepithelial cells -Polygonal with abundant clear cytoplasm -Bland oval nucleus with pale chromatin -Small distinct nucleolus -PAS+ for glycogen Ductal cells -Cuboidal -Round nuclei with dark chromatin -Scant granular cytoplasm Background stripped myoepithelial nuclei Acellular matrix material and proteincaceous secretions In some cases, the clear myoepithelial cells predominate to the near exclusion of the ductal component. Epithelial-Myoepithelial Carcinoma Special Studies: Cell block can be used to demonstrate the biphasic features of the tumor: PAS+ to demonstrate abundant glycogen IPX for WS keratins for ductal cells IPX for smooth muscle actin, calponin, S-100 for myoepithelial cells Epithelial-Myoepithelial Carcinoma: The DDX includes other tumors with clear cells DIFFERENTIAL DIAGNOSIS: Myoepithelioma/carcinoma Acinic cell carcinoma Oncocytoma Sebaceous adenoma/carcinoma Clear cell carcinoma Lipoma Metastatic renal cell carcinoma Mucoepidermoid carcinoma, low-grade 34








35 Epithelial-Myoepithelial Carcinoma: The DDX includes other tumors with clear cells Clear Cell Tumors: Myoepithelioma/Carcinoma What is in the clear cytoplasm?: Glycogen Lipid Condensed mitochondria Mucin Monophasic pattern Less abundant glycogenrich cytoplasm May contain fibrillar matrix with embedded cells High-grade when malignant Myoepithelioma Myoepithelial carcinoma Clear Cell Tumors: Myoepithelioma/Carcinoma Myoepithelioma Myoepithelial Carcinoma Clear Cell Tumors: Sebaceous Adenoma/Lymphadenoma Very rare Clear cells and squamous cells Highly vacuolated cytoplasm Background lymphocytes Cytoplasm contains fat: oil red-o + on air-dried Fat Stain + Sebaceous Lymphadenoma Clear Cell Tumors: Acinic Cell Carcinoma Can be confused with LG MEC, but it lacks mucin. Lacks myoepithelial cells Lacks biphasic pattern Contains PAS + D zyomogen granules 35



36 Clear Cell Tumors: Clear Cell Carcinoma Usually palatal Lacks ductal structures Lacks myoepithelial differentiation Diagnosis of exclusion Final Comments Epithelial-myoepithelial carcinoma is a rare lowgrade biphasic tumor with a predominance of large clear myoepithelial cells. Histology is unique; cytology is more challenging! The DDX includes numerous other clear cell tumors, but none matches the biphasic pattern of epithelialmyoepithelial carcinoma. Ancillary studies can be helpful CASE 8 A 48 year-old female presented with a 1.5 cm tender, rapidly enlarging lesion of the left parotid. An FNA was performed. CASE 8 Cytologic Diagnosis: SPINDLE CELL LESION, FAVOR BENIGN. SEE NOTE. Note: The differential diagnosis includes nodular fasciitis, schwannoma, and pleomorphic adenoma. 36



37 The nodule was surgically excised by superficial parotidectomy. Immunohistochemistry for Vimentin Immunohistochemistry for Smooth Muscle Actin CASE 8 Summary of immunohistochemistry: Vimentin + Smooth muscle actin + S Keratin - CD34 - CASE 8 Histologic Diagnosis: NODULAR FASCIITIS 37
 Reactive myofibroblastic lesion in young adults (20-40 year-old) Rapidly enlarging, often tender subcutaneous nodule (<3 cm) May be associated with trauma Most anatomic sites but")


38 Nodular Fasciitis First reported in 1955 (Konwaler et al.) Reactive myofibroblastic lesion in young adults (20-40 year-old) Rapidly enlarging, often tender subcutaneous nodule (<3 cm) May be associated with trauma Most anatomic sites but predilection for the upper limb, especially forearm less common in the head and neck Self-limiting clinical course; recurrence is uncommon Nodular Fasciitis Histologic Features: Circumscribed but unencapsulated Short interweaving fascicles of myofibroblasts Loose collagenous or myxoid stroma Delicate capillaries with red blood cell extravasation Mild mixed inflammation Mitoses may be frequent May contain osteoclast-type giant cells Absence of atypia Nodular Fasciitis Nodular Fasciitis Nodular Fasciitis Cytology (cellular aspirate): Spindle-shaped myofibroblasts, plump nuclei, pale chromatin, vacuolated cytoplasm, wispy bipolar cytoplasmic processes Small groups often with intercellular collagen Bloody and myxoid background Chronic inflammatory cells Nodular Fasciitis The diagnosis is often suggested by the clinical presentation, and FNA serves to simply confirm the clinical suspicion. 38

 Distinguished by IPX:")


 Myoepithelioma (10) Malignant")
 Neurofibroma (1) Solitary fibrous tumor (1) Angiosarcoma (1) Spindle")
39 Nodular Fasciitis: Differential Diagnosis BENIGN: Myoepithelioma/PA Schwannoma Solitary fibrous tumor Inflammatory pseudotumor Granuloma Fibrous histiocytoma Neurofibroma Leiomyoma Nodular Fasciitis: Benign Differential Diagnosis Schwannoma Wavy nuclei with pointed ends Palisading (Verocay bodies) Distinguished by IPX: Strongly S-100+ Schwannoma Nodular Fasciitis: Benign Differential Diagnosis Granuloma Solitary fibrous tumor Leiomyoma Nodular Fasciitis Immunocytochemistry: Positive:» Vimentin +» Smooth muscle actin + Negative: (Positive)» S-100 Schwannoma» Desmin Leiomyoma» Keratin Pleomorphic adenoma» CD34 Solitary fibrous tumor» CD68 Granuloma FNA of Spindle Cell Lesions of the Head and Neck Spindle cell lesions of the head and neck diagnosed by FNA between : Schwannoma (16) Myoepithelioma (10) Malignant melanoma (6) Medullary carcinoma (4) Hemangiopericytoma (2) Fibrosarcoma (2) Nodular fasciitis (3) Neurofibroma (1) Solitary fibrous tumor (1) Angiosarcoma (1) Spindle cell carcinoma (1) Leiomyosarcoma (1) 39
40 FNA of Spindle Cell Lesions of the Salivary Gland Region Evaluating these difficult lesions: Clinical history including information about the nature of the lesion (size, growth rate, site) is CRITICAL! When possible, additional material for immunocytochemical studies should be obtained, preferably as a paraffin-embedded cell block. Electron microscopy can be an extremely valuable ancillary tool. Benign versus Malignant Spindle Cell Lesions of the Salivary Gland Region It may not always be possible to give a specific diagnosis; however, distinguishing benign from malignant spindle cell lesions is often feasible. Benign versus Malignant Spindle Cell Lesions of the Salivary Gland Region Nonetheless, a note recommending close clinical follow-up and re-biopsy, should the lesion fail to resolve or should it show evidence of growth, is suggested. Benign versus Malignant Spindle Cell Lesions of the Salivary Gland Region Features associated with malignant lesions: Nuclear hyperchromasia Prominent nucleoli Irregular chromatin distribution Nuclear pleomorphism Necrosis Hemorrhage Atypical mitoses High cellularity Nodular Fasciitis: Malignant Differential Diagnosis MALIGNANT: Myoepithelial carcinoma Malignant melanoma Spindle cell carcinoma MPNST Sarcoma:» Fibrosarcoma» Synovial sarcoma» MFH Final Comments Evaluation of spindle cell lesions by FNA can be very challenging. In many cases, distinction between benign and malignant is possible based upon microscopic and clinical features. Clinical correlation and adequate material for ancillary studies are essential for making an accurate evaluation. 40
41 41
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
Salivary gland cytology. Salivary gland cytology. Triage helps the clinician. Salivary gland tumors. Diagnostic difficulties
 Salivary gland cytology Salivary Gland Cytology Pınar Fırat, MD Professor of Pathology İ.U. İstanbul Faculty of Medicine Çapa, İstanbul It is a reliable diagnostic test However, definitive subclassification
Salivary gland cytology Salivary Gland Cytology Pınar Fırat, MD Professor of Pathology İ.U. İstanbul Faculty of Medicine Çapa, İstanbul It is a reliable diagnostic test However, definitive subclassification
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
FNA Biopsy of Salivary Gland
 FNA Biopsy of Salivary Gland Richard M. DeMay, MD Professor of Pathology Director of Cytopathology The University of Chicago Objective: To describe the use of FNA Bx to diagnose salivary gland lesions
FNA Biopsy of Salivary Gland Richard M. DeMay, MD Professor of Pathology Director of Cytopathology The University of Chicago Objective: To describe the use of FNA Bx to diagnose salivary gland lesions
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Salivary gland Workshop Trondheim 31th may 2012
 Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Salivary Gland Pathology
 IN THE NAME OF GOD Salivary Gland Pathology CHAPTER 11 Dr.kheirandish Oral and maxillofacial pathology Sialadenosis Adenomatoid Hyperplasia of the Minor Salivary Glands Necrotizing Sialometaplasia Pleomorphic
IN THE NAME OF GOD Salivary Gland Pathology CHAPTER 11 Dr.kheirandish Oral and maxillofacial pathology Sialadenosis Adenomatoid Hyperplasia of the Minor Salivary Glands Necrotizing Sialometaplasia Pleomorphic
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology
 Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
(CYLINDROMA) ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA
 ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA") (CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
(CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Diagnostic Cytology of Cancer Cases
 Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Diagnostic Cytology of Cancer Cases Somporn Techangamsuwan Companion Animal Cancer Research Unit (CAC-RU) Department of Pathology, Faculty of Veterinary Science, Chulalongkorn University 1 Tumor or Non-tumor
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017
 Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College
Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College
Slide Seminar of the Head and Neck Session of the European Congress of Pathology Bilbao, Spain, 2018.
 Slide Seminar of the Head and Neck Session of the European Congress of Pathology Bilbao, Spain, 2018. Prof Sulen Sarioglu, MD Dokuz Eylul University Faculty of Medicine Department of Pathology Graduate
Slide Seminar of the Head and Neck Session of the European Congress of Pathology Bilbao, Spain, 2018. Prof Sulen Sarioglu, MD Dokuz Eylul University Faculty of Medicine Department of Pathology Graduate
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Oncocytic carcinoma: A rare malignancy of the parotid gland
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS
 NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS Abstract: The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology
NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS Abstract: The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology
Review of the AP Part II Practical Examination. Dr David Clift Co Chief Examiner
 Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
EQA Circulation 43 Educational Cases
 EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Zubair W. Baloch, MD, PhD: Consultant for Veracyyte, INC Tarik M. Elsheikh, MD: Nothing to disclose
 Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair
Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
TYPES and FREQUENCY of SALIVARY GLAND TUMORS in MAJOR and MINOR. Karl Donath Department of Oral Pathology (Director:Prof. Dṛ Dr.
 TYPES and FREQUENCY of SALIVARY GLAND TUMORS in MAJOR and MINOR SALIVARY GLANDS Karl Donath Department of Oral Pathology (Director:Prof. Dṛ Dr. Karl Donath) University of Hamburg, Salivary gland tumors
TYPES and FREQUENCY of SALIVARY GLAND TUMORS in MAJOR and MINOR SALIVARY GLANDS Karl Donath Department of Oral Pathology (Director:Prof. Dṛ Dr. Karl Donath) University of Hamburg, Salivary gland tumors
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors
 Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
DISCUSSION: PLGA accounts for about 2% of all salivary gland tumours and occurs almost exclusively in the minor salivary glands.
 SWELLING ON THE HARD PALATE PRESENTING AS POLYMORPHOUS LOW GRADE ADENOCARCINOMA: A AND REVIEW OF LITERATURE Swapnil D. Chandekar 1, Sunita S. Dantkale 2, Rahul R. Narkhede 3, Snehal V. Chavhan 4, Khushboo
SWELLING ON THE HARD PALATE PRESENTING AS POLYMORPHOUS LOW GRADE ADENOCARCINOMA: A AND REVIEW OF LITERATURE Swapnil D. Chandekar 1, Sunita S. Dantkale 2, Rahul R. Narkhede 3, Snehal V. Chavhan 4, Khushboo
ISPUB.COM. Salivary duct carcinoma of parotid gland. V Kinnera, R Nandyala, M Yootla, K Mandyam INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R Nandyala, M Yootla, K Mandyam.. The Internet Journal of Pathology. 2008 Volume
ISPUB.COM The Internet Journal of Pathology Volume 10 Number 1 V Kinnera, R Nandyala, M Yootla, K Mandyam Citation V Kinnera, R Nandyala, M Yootla, K Mandyam.. The Internet Journal of Pathology. 2008 Volume
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland
 The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
SALIVARY GLAND DISEASES. Omar alnoubani MD,MRCS
 SALIVARY GLAND DISEASES Omar alnoubani MD,MRCS Salivary Glands Overview Parotid gland Sublingual gland Submandibular gland Salivary glands - Types 3 Major Salivary Glands Parotid Submandibular Sublingual
SALIVARY GLAND DISEASES Omar alnoubani MD,MRCS Salivary Glands Overview Parotid gland Sublingual gland Submandibular gland Salivary glands - Types 3 Major Salivary Glands Parotid Submandibular Sublingual
Research Article Transmucosal Fine Needle Aspiration of Oral and Pharyngeal Lesions
 International Scholarly Research Network ISRN Pathology Volume 2011, Article ID 267145, 7 pages doi:10.5402/2011/267145 Research Article Transmucosal Fine Needle Aspiration of Oral and Pharyngeal Lesions
International Scholarly Research Network ISRN Pathology Volume 2011, Article ID 267145, 7 pages doi:10.5402/2011/267145 Research Article Transmucosal Fine Needle Aspiration of Oral and Pharyngeal Lesions
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE
 SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Salivary Gland Imaging. Mary Scanlon MD FACR October 2016
 Salivary Gland Imaging Mary Scanlon MD FACR October 2016 Objectives Recognize normal and abnormal anatomy Discuss work up, management and differential diagnosis of commonly referred clinical scenarios
Salivary Gland Imaging Mary Scanlon MD FACR October 2016 Objectives Recognize normal and abnormal anatomy Discuss work up, management and differential diagnosis of commonly referred clinical scenarios
Pancreas. Atrophy, acinar cell. Pathogenesis: Diagnostic key features:
 Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
Pancreas Atrophy, acinar cell Pathogenesis: Decrease in number and/or size of acinar cells may be due to spontaneous or experimentally induced degenerative changes, apoptosis, or a sequel of chronic inflammation.
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Cytomorphological study of major salivary gland lesions: a 5-year experience at a tertiary care center
 Original article Cytomorphological study of major salivary gland lesions: a 5year experience at a tertiary care center Aruna S, Prathiksha Pai, Shreekant K. Kittur Department of Pathology, Belagavi Institute
Original article Cytomorphological study of major salivary gland lesions: a 5year experience at a tertiary care center Aruna S, Prathiksha Pai, Shreekant K. Kittur Department of Pathology, Belagavi Institute
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Abid Irshad, MD Director Breast Imaging. Medical University of South Carolina Charleston
 Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
CASE year old male with a PET avid nodule in the left adrenal gland
 CASE 1 55 year old male with a PET avid nodule in the left adrenal gland Case 1 Adrenal gland parenchyma partly replaced by a spindle cell tumour with mild nuclear pleomorphism Atypical mitoses present
CASE 1 55 year old male with a PET avid nodule in the left adrenal gland Case 1 Adrenal gland parenchyma partly replaced by a spindle cell tumour with mild nuclear pleomorphism Atypical mitoses present
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
ORIGINAL ARTICLE. Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population
 ORIGINAL ARTICLE Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population Erik G. Cohen, MD; Snehal G. Patel, MD; Oscar Lin, MD; Jay O. Boyle, MD; Dennis H. Kraus, MD; Bhuvanesh
ORIGINAL ARTICLE Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population Erik G. Cohen, MD; Snehal G. Patel, MD; Oscar Lin, MD; Jay O. Boyle, MD; Dennis H. Kraus, MD; Bhuvanesh
Pleomorphic adenoma of breast - a case report and distinction with metaplastic carcinoma D Gupta, S Agrawal, N Trivedi, A Tewari
 of breast - a case report and distinction with metaplastic carcinoma D Gupta, S Agrawal, N Trivedi, A Tewari Introduction, also known as mixed tumour, is a benign tumour which typically presents as a painless,
of breast - a case report and distinction with metaplastic carcinoma D Gupta, S Agrawal, N Trivedi, A Tewari Introduction, also known as mixed tumour, is a benign tumour which typically presents as a painless,
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Pathology Slides. [Pathology]
![Pathology Slides. [Pathology]](/thumbs/94/120604575.jpg "Pathology Slides. [Pathology]") Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Departments of Pathology and *Otorhinolaryngology, Faculty of Medicine, University of Malaya, Kuala Lumpur
 Malaysian J Pathol 2002; 24(2) : 107-112 CASE REPORT Papillary cystic type of acinic cell carcinoma of parotid: fine needle aspiration cytological features of a high grade variant with oncocytic metaplasia
Malaysian J Pathol 2002; 24(2) : 107-112 CASE REPORT Papillary cystic type of acinic cell carcinoma of parotid: fine needle aspiration cytological features of a high grade variant with oncocytic metaplasia
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
Workshop 2. Controversies and Diagnostic Challenges in Head and Neck Cytopathology. Zubair Baloch, MD,PhD. Veracyte, Inc: Consultant
 Workshop 2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair Baloch, MD,PhD Veracyte, Inc: Consultant Tarik Elsheikh, MD There are no disclosures necessary. Controversies and
Workshop 2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair Baloch, MD,PhD Veracyte, Inc: Consultant Tarik Elsheikh, MD There are no disclosures necessary. Controversies and
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
doi: /j.anl
 doi: 10.1016/j.anl.2006.07.001 Synchronous unilateral parotid gland neoplasms of three different histological types Shuho Tanaka 1, Keiji Tabuchi 1, Keiko Oikawa 1, Rika Kohanawa 1, Hideki Okubo 1, Dai
doi: 10.1016/j.anl.2006.07.001 Synchronous unilateral parotid gland neoplasms of three different histological types Shuho Tanaka 1, Keiji Tabuchi 1, Keiko Oikawa 1, Rika Kohanawa 1, Hideki Okubo 1, Dai
Lách
 Lách Lách Lách Lách Splenogonadal fusion. Splenic tissue is attached to testicular tissue. Pseudocyst (false or secondary cyst). A, Outer aspect. Pseudocyst (false or secondary cyst). B, Inner surface.
Lách Lách Lách Lách Splenogonadal fusion. Splenic tissue is attached to testicular tissue. Pseudocyst (false or secondary cyst). A, Outer aspect. Pseudocyst (false or secondary cyst). B, Inner surface.
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no