Cath Lab Essentials: Pericardial effusion & tamponade
|
|
|
- Stuart Farmer
- 5 years ago
- Views:
Transcription





1 Cath Lab Essentials: Pericardial effusion & tamponade Pranav M. Patel, MD, FACC, FSCAI Chief, Division of Cardiology Director, Cardiac Cath Lab & CCU University of California, Irvine Division of Cardiology


2 Acknowledgments No financial disclosures
3 Case A 52-year-old man with a 3-day history of progressively worsening dyspnea on exertion to the point that he is unable to walk more than one block without resting. He has had sharp intermittent pleuritic chest pain and a nonproductive cough. He is taking no medications.
4 Case Temp is 37.7 C (99.9 F), blood pressure is 88/44 mm Hg, pulse is 125/min, and respiration rate is 29/min; BMI is 27. Oxygen saturation is 95%. Pulsus paradoxus is 15 mm Hg. JVP is 12 cm H 2 O. Cardiac examination discloses muffled heart sounds with no rubs. Lung auscultation reveals normal breath sounds and no crackles. There is 2+ pedal edema.

5 ECG-electrical alternans

6 Chest X-ray

7 Question What is the most appropriate treatment? A. Dobutamine to increase BP B. Broad spectrum antibiotics C. Pericardiocentesis D.Surgical pericardiectomy

8 Echocardiogram: RV collapse in diastole Most commonly involves the RV outflow tract (more compressible area of RV) Occurs in early diastole, immediately after closure of the pulmonary valve, at the time of opening of the tricuspid valve When collapse extends form outflow tract to the body of the right ventricle, this is evidence that intrapericardial pressure is elevated more substantially FN Delling

9 Subcostal view FN Delling 2007

10 M-mode Beginning of systole ES DC RV wall Pericardial space FN Delling 2007

11 Parasternal long axis view FN Delling 2007

12 M-mode Beginning of systole ES DC FN Delling 2007
13 Pericardial Effusion Can occur rapidly or slowly Pulmonary compression-cough, dyspnea, and tachypnea Phrenic nerve compression-hiccups Heart sounds distant, muffled Slow fluid build-up; no immediate effects; Rapid fluid build up --> compression of heart --> tamponade FN Delling 2007

14
15 Cardiac Tamponade Compression of heart Occur acutely (trauma) or sub-acutely (malignancy) Symptoms- chest pain, confusion, anxious, elevated CVP/JVD, restless, muffled heart sounds Later- tachypnea, tachycardia, and decrease CO, and pulsus paradoxus With slow onset- dyspnea may be only symptom If rapid compression-medical Emergency


16 Original heart size Excess pericardial fluid
17 Summary of physiologic changes in tamponade. RV, right ventricle. (From Shoemaker WC, Carey JS, Yao ST, et al: Hemodynamic monitoring for physiological evaluation, diagnosis, and therapy of acute hemopericardial tamponade from penetrating wounds. J Trauma 13:36, 1973; and Spodick D: Acute cardiac tamponade: Pathologic physiology, diagnosis, and management. Prog Cardiovasc Dis 10:65, 1967.)
18 Grade Pericardial Volume (ml) Cardiac Index MAP CVP HR Beck's Triad I <200 Normal or Normal usually not present II 200 Normal or ( 12 cm H 2 O) May or may not be present III >200 ( cm H 2 O) Usually present From Shoemaker WC, Carey SJ, Yao ST, et al: Hemodynamic monitoring for physiologic evaluation, diagnosis, and therapy of acute hemopericardial tamponade from penetrating wounds. J Trauma 13:36, 1973.





19 Increased venous pressure Decreased arterial pressure Muffled heart sounds


20 Swinging heart-electrical alternans F N Delling

21 Pulsus Paradoxus >20mmHg drop RA pressure =Pericardial pressures with blunted wave forms
22 Nursing Care 1. Dyspnea: from hypoxia, decreased CO and decreased lung expansion. 2. Retrosternal chest pain that increases when patients are supine and decreases when leaning forward because of compression of the heart 3. Cough, hoarseness, or hiccups caused by mechanical compression of nerves of the esophagus, bronchi, and trachea 4. Weakness, fatigue, and malaise resulting from decreased cardiac output 5. Vague gastrointestinal complaints because of visceral congestion and venous stasis
23 Nursing Care 1. Monitor for dysrhythmia which may result of myocardial ischemia from epicardial coronary artery compression. 2. Monitor the BP every 5 to 15 minutes during acute phase 3. Monitor for pulsus paradoxus via arterial tracing or during manual BP reading. Monitor for increased JVP 4. A drop in urine output indicates decreased renal perfusion as a result of decreased stroke volume secondary to cardiac compression. 5. Assess level of consciousness for changes that may indicate decreased cerebral perfusion Cardiac Tamponade nursingcrib.com

24 Technologist: Equipment required Pericardiocentesis 1. Pericardiocentesis kit (contains equipment to perform drain placement via Seldinger technique) 1. If kit unavailable: 18ga spinal needle, 20mL syringe 2. Can also use micro puncture needle and kit 2. Ultrasound/echocardiogram if available; or, 3. Equipment ready to measure pericardial pressure if needed 4. Swan Ganz catheter to measure chamber pressure A Seldinger technique pericardiocentesis set (Wood set by Cook Critical Care Co.)- calsprogram.org
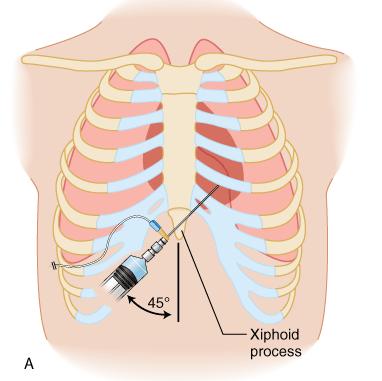
25 Technologist: Patient preparation- subxyphoid approach 1. Bed to angle if patient condition allows (brings heart/pericardium closer to anterior chest wall) 2. Skin prep with iodine or chlorhexidine, followed by sterile drape 3. Consider sedation or local anesthesia but do not delay procedure 4. Continuous monitoring (BP, HR, spo2, etc) during procedure. Art-line preferable, but do not delay procedure. 5. Atropine may be helpful to prevent vasovagal reaction

26 Pericardial pressure is an external pressure which pushes on the cardiac chambers.... An effusion is equally distributed and thus equalize filling/diastole pressures across chambers. Therefore no gradient for flow exists except during atrial contraction. In early diastole filling does not occur = absence of the y descent. Bojan Paunovic, MD and Sat Sharma, MD, FRCPC,
27 Case Temp is 37.7 C (99.9 F), blood pressure is 88/44 mm Hg, pulse is 125/min, and respiration rate is 29/min; BMI is 27. Oxygen saturation is 95%. Pulsus paradoxus is 15 mm Hg. JVP is 12 cm H 2 O. Cardiac examination discloses muffled heart sounds with no rubs. Lung auscultation reveals normal breath sounds and no crackles. There is 2+ pedal edema.

28 Pericardiocentesis From Custalow CB: Color Atlas of Emergency Department Procedures. Philadelphia, Elsevier Saunders, 2005, p 123.

29
30
31

32



33
34 expiration inspiration Femoral artery pressure

35 RA- mean pressure 18 mmhg

36 RV diastolic pressure mmhg

37 PA diastoilic pressure mm Hg

38 PCW Mean PCW mmhg

39 Pericardial pressure RA pressure

40 Removal of 60 ml of pericadial fluid - RA and pericardial pressures are equal and falling
41 Removal of 120 ml of fluid pericardial pressure < RA pressure

42 Femoral artery pressure no pulses paradoxus Mean RA pressure = 10 mm Hg after 240 ml fluid removed
43 Pericardial effusion impending tamponade

44 Removed 3ml of pericardial fluid and then added 3ml of agitated saline in pericardial space but before that the needle had entered the RV


45 Now increased pericardial effusion fall in HR and BP loss of consciousness TAMPONADE imminent death


46 Removal of bloody pericardial fluid


47 Pericardial drain in place more fluid removed patient doing well and talking one hour after procedure


48 Seen under fluroscopy after pericardiocentesis Initial Pericardiocentesis What is seen after Pericardiocentesis
49 End questions? Thanks!
We are now going to review the diagnosis and management of pericardial collections and tamponade
 We are now going to review the diagnosis and management of pericardial collections and tamponade FEEL COURSE PAGE 1 Paying particular attention to the difference between a collection and cardiac tamponade
We are now going to review the diagnosis and management of pericardial collections and tamponade FEEL COURSE PAGE 1 Paying particular attention to the difference between a collection and cardiac tamponade
Palpable Pulsus Paradoxus in the Setting of Malignant Pericardial Effusion and Tamponade Akshay Pendyal, MD
 Palpable Pulsus Paradoxus in the Setting of Malignant Pericardial Effusion and Tamponade Akshay Pendyal, MD University of Colorado Department of Internal Medicine None Conflicts of Interest Objectives
Palpable Pulsus Paradoxus in the Setting of Malignant Pericardial Effusion and Tamponade Akshay Pendyal, MD University of Colorado Department of Internal Medicine None Conflicts of Interest Objectives
PERICARDIAL DIAESE. Kaijun Cui Associated professor Sichuan University
 PERICARDIAL DIAESE Kaijun Cui Associated professor Sichuan University CLASSIFICATION acute pericarditis pericardial effusion cardiac tamponade constrictive pericarditis congenitally absent pericardium
PERICARDIAL DIAESE Kaijun Cui Associated professor Sichuan University CLASSIFICATION acute pericarditis pericardial effusion cardiac tamponade constrictive pericarditis congenitally absent pericardium
Technique. Technique. Technique. Monitoring 1. Local anesthetic? Aseptic technique Hyper-extend (if radial)
") Critical Care Monitoring Hemodynamic Monitoring Arterial Blood Pressure Cannulate artery Uses 2 Technique Sites Locate artery, prep 3 1 Technique Local anesthetic? Aseptic technique Hyper-extend (if radial)
Critical Care Monitoring Hemodynamic Monitoring Arterial Blood Pressure Cannulate artery Uses 2 Technique Sites Locate artery, prep 3 1 Technique Local anesthetic? Aseptic technique Hyper-extend (if radial)
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU
 Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU Ailin Barseghian El-Farra, MD, FACC Assistant Professor, Interventional Cardiology University of California, Irvine Department of Cardiology
Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU Ailin Barseghian El-Farra, MD, FACC Assistant Professor, Interventional Cardiology University of California, Irvine Department of Cardiology
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
THE PERICARDIUM: LOOKING OUTSIDE THE HEART
 THE PERICARDIUM: LOOKING OUTSIDE THE HEART DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate
THE PERICARDIUM: LOOKING OUTSIDE THE HEART DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate
Cardiac tamponade and Pericardiocentesis Made Easy
 Cardiac tamponade and Pericardiocentesis Made Easy www.cardiconcept.com Etiology of pericardial diseases. Non Infectious cause Infectious cause European Heart Journal (2015) 36, 2921 2964 Recommendations
Cardiac tamponade and Pericardiocentesis Made Easy www.cardiconcept.com Etiology of pericardial diseases. Non Infectious cause Infectious cause European Heart Journal (2015) 36, 2921 2964 Recommendations
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
LeMone & Burke Ch 30-32
 LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
Pericardial Diseases. Smonporn Boonyaratavej, MD. Division of Cardiology, Department of Medicine Chulalongkorn University
 Pericardial Diseases Smonporn Boonyaratavej, MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital 21 AUGUST 2016 Pericardial
Pericardial Diseases Smonporn Boonyaratavej, MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital 21 AUGUST 2016 Pericardial
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Background & Indications Probe Selection
 Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Unit 4 Problems of Cardiac Output and Tissue Perfusion
 Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
Cardiology. Objectives. Chapter
 1:44 M age 1121 Chapter Cardiology Objectives art 1: Cardiovascular natomy and hysiology, ECG Monitoring, and Dysrhythmia nalysis (begins on p. 1127) fter reading art 1 of this chapter, you should be able
1:44 M age 1121 Chapter Cardiology Objectives art 1: Cardiovascular natomy and hysiology, ECG Monitoring, and Dysrhythmia nalysis (begins on p. 1127) fter reading art 1 of this chapter, you should be able
TAMPONADE CARDIAQUE. Dr Cédrick Zaouter TUSAR 15 décembre 2015
 TAMPONADE CARDIAQUE Dr Cédrick Zaouter TUSAR 15 décembre 2015 OUTLINE History Incidence Definition Pathophysiology Aetiologies Investigations - Echocardiography Treatment of cardiac tamponade Pericardial
TAMPONADE CARDIAQUE Dr Cédrick Zaouter TUSAR 15 décembre 2015 OUTLINE History Incidence Definition Pathophysiology Aetiologies Investigations - Echocardiography Treatment of cardiac tamponade Pericardial
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Outline. Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials
 Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials John R Schairer DO FACC Henry Ford Heart and Vascular Institute No Disclosures Outline Normal Anatomy and Physiology Pathophysiology
Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials John R Schairer DO FACC Henry Ford Heart and Vascular Institute No Disclosures Outline Normal Anatomy and Physiology Pathophysiology
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Acute Pericardial Tamponade
 Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Pericardial diseases
 Pericardial diseases Anatomy of the pericardium Consists of parietal and visceral membranes. The space between them(pericardial space is normally filled by a lymph like fluid. The fluid s normal quantity
Pericardial diseases Anatomy of the pericardium Consists of parietal and visceral membranes. The space between them(pericardial space is normally filled by a lymph like fluid. The fluid s normal quantity
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade
 Symposium The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade Adam Goodman, Phillips Perera, Thomas Mailhot, Diku Mandavia Department of Emergency Medicine, Los
Symposium The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade Adam Goodman, Phillips Perera, Thomas Mailhot, Diku Mandavia Department of Emergency Medicine, Los
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Heart Failure with Johnny Crash: LEFT VENTRICULAR EJECTION FRACTION (LVEF) SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:
 SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:") Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
Integrative Clinical Hemodyamics
 Integrative Clinical Hemodyamics James A. Goldstein, MD Director, Research & Education Division of Cardiology William Beaumont Hospital Disclosure Information Integrative Clinical Hemodyamics James A.
Integrative Clinical Hemodyamics James A. Goldstein, MD Director, Research & Education Division of Cardiology William Beaumont Hospital Disclosure Information Integrative Clinical Hemodyamics James A.
CATCH A WAVE.. INTRODUCTION NONINVASIVE HEMODYNAMIC MONITORING 4/12/2018
 WAVES CATCH A WAVE.. W I S C O N S I N P A R A M E D I C S E M I N A R A P R I L 2 0 1 8 K E R I W Y D N E R K R A U S E R N, C C R N, E M T - P Have you considered that if you don't make waves, nobody
WAVES CATCH A WAVE.. W I S C O N S I N P A R A M E D I C S E M I N A R A P R I L 2 0 1 8 K E R I W Y D N E R K R A U S E R N, C C R N, E M T - P Have you considered that if you don't make waves, nobody
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Interventional Imaging Cases
 Interventional Imaging Cases Steven A. Goldstein MD Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Tuesday, October 10, 2017 DISCLOSURE I
Interventional Imaging Cases Steven A. Goldstein MD Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Tuesday, October 10, 2017 DISCLOSURE I
Pericardial Disease: Case Examples. Echo Fiesta 2017
 Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
The Cardiac Cycle Clive M. Baumgarten, Ph.D.
 The Cardiac Cycle Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe periods comprising cardiac cycle and events within each period 2. Describe the temporal relationships between pressure, blood flow,
The Cardiac Cycle Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe periods comprising cardiac cycle and events within each period 2. Describe the temporal relationships between pressure, blood flow,
Lab 16. The Cardiovascular System Heart and Blood Vessels. Laboratory Objectives
 Lab 16 The Cardiovascular System Heart and Blood Vessels Laboratory Objectives Describe the anatomical structures of the heart to include the pericardium, chambers, valves, and major vessels. Describe
Lab 16 The Cardiovascular System Heart and Blood Vessels Laboratory Objectives Describe the anatomical structures of the heart to include the pericardium, chambers, valves, and major vessels. Describe
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: CARDIAC EMERGENCIES Revised: 11/2013
 DEFINITIONS: Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: CARDIAC EMERGENCIES Revised: 11/2013 Chain of survival (adult) - early activation, early
DEFINITIONS: Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: CARDIAC EMERGENCIES Revised: 11/2013 Chain of survival (adult) - early activation, early
February 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Cardiac Cycle MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Cycle MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 1- Regarding the length of systole and diastole: a- At heart rate 75 b/min, the duration of
Cardiac Cycle MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 1- Regarding the length of systole and diastole: a- At heart rate 75 b/min, the duration of
Disclosures. Cardiac Ultrasound. Introductory Case. 80 y/o male Syncope at home Emesis x 3 in ambulance Looks sick. No pain.
 Disclosures Cardiac Ultrasound Justin A Davis, MD MPH RDMS Subchief for Emergency Ultrasound Kaiser Permanente East Bay Medical Center I have nothing to disclose. Introductory Case HR 118 BP 65/43 RR 27
Disclosures Cardiac Ultrasound Justin A Davis, MD MPH RDMS Subchief for Emergency Ultrasound Kaiser Permanente East Bay Medical Center I have nothing to disclose. Introductory Case HR 118 BP 65/43 RR 27
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
#6 - Cardiovascular III Heart Sounds, Pulse Rate, Hemoglobin Saturation, and Blood Pressure
 #6 - Cardiovascular III Heart Sounds, Pulse Rate, Hemoglobin Saturation, and Blood Pressure Objectives: Observe slide of artery and vein cross-section Auscultate heart sounds using a stethoscope Measure
#6 - Cardiovascular III Heart Sounds, Pulse Rate, Hemoglobin Saturation, and Blood Pressure Objectives: Observe slide of artery and vein cross-section Auscultate heart sounds using a stethoscope Measure
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
efferent fibers from t.. Heart Surface anatomy and heart sounds -Dry lecture -Gray s 169,
 A patient is diagnosed with ischemia (i.e., lack of blood flow) in a left lobar pulmonary vein. The attending physician determines that the ischemia is due to a vasospastic episode. Constriction of this
A patient is diagnosed with ischemia (i.e., lack of blood flow) in a left lobar pulmonary vein. The attending physician determines that the ischemia is due to a vasospastic episode. Constriction of this
BACHELOR OF SCIENCE IN CARDIO VASCULAR TECHNOLOGY
 BACHELOR OF SCIENCE IN CARDIO VASCULAR TECHNOLOGY BCVT 101 Eco Cardiography BCVT 102 ECG-Stream-Holter BCVT 103 Cat lab BCVT 104 Anatomy 1 st YEAR BCVT 105 Physiology BCVT 106 Pathology & Pathophysiology
BACHELOR OF SCIENCE IN CARDIO VASCULAR TECHNOLOGY BCVT 101 Eco Cardiography BCVT 102 ECG-Stream-Holter BCVT 103 Cat lab BCVT 104 Anatomy 1 st YEAR BCVT 105 Physiology BCVT 106 Pathology & Pathophysiology
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Brief View of Calculation and Measurement of Cardiac Hemodynamics
 Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy
 A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
Normal Pericardial Physiology
 Normal Pericardial Physiology Normal pericardium contains 20-30 ml of lymphoid fluid lubricating function that facilitates normal myocardial rotation and translation during each cardiac cycle in that the
Normal Pericardial Physiology Normal pericardium contains 20-30 ml of lymphoid fluid lubricating function that facilitates normal myocardial rotation and translation during each cardiac cycle in that the
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
10/16/2014. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular
 Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
Cardiovascular Images
 Cardiovascular Images Pulmonary Embolism Diagnosed From Right Heart Changes Seen After Exercise Stress Echocardiography Brian C. Case, MD; Micheas Zemedkun, MD; Amarin Sangkharat, MD; Allen J. Taylor,
Cardiovascular Images Pulmonary Embolism Diagnosed From Right Heart Changes Seen After Exercise Stress Echocardiography Brian C. Case, MD; Micheas Zemedkun, MD; Amarin Sangkharat, MD; Allen J. Taylor,
12 th Annual West Virginia ACC Meeting April 8, 2017
 12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
Cardiovascular Practice Quiz
 Cardiovascular Practice Quiz 1. When caring for a patient following a cardiac catheterization with coronary angiography, which of the following findings would be of most concern to the nurse? a. Swelling
Cardiovascular Practice Quiz 1. When caring for a patient following a cardiac catheterization with coronary angiography, which of the following findings would be of most concern to the nurse? a. Swelling
For more information about how to cite these materials visit
 Project: Ghana Emergency Medicine Collaborative Document Title: Case Presentation- Pericarditis Author(s): Kwaku Nyame License: Unless otherwise noted, this material is made available under the terms of
Project: Ghana Emergency Medicine Collaborative Document Title: Case Presentation- Pericarditis Author(s): Kwaku Nyame License: Unless otherwise noted, this material is made available under the terms of
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
suggested by Katz and Gauchat (3) for the ex- diaphragm during inspiration, traction is applied Dornhorst, Howard, and Leathart (2), using an
 for the ex- diaphragm during inspiration, traction is applied Dornhorst, Howard, and Leathart (2), using an") Journal of Clinical Investigation Vol. 42, No. 2, 1963 THE MECHANISM OF PULSUS PARADOXUS DURING ACUTE PERICARDIAL TAMPONADE * By RICHARD J. GOLINKO,t NEVILLE KAPLAN, AND ABRAHAM M. RUDOLPH t (From the
Journal of Clinical Investigation Vol. 42, No. 2, 1963 THE MECHANISM OF PULSUS PARADOXUS DURING ACUTE PERICARDIAL TAMPONADE * By RICHARD J. GOLINKO,t NEVILLE KAPLAN, AND ABRAHAM M. RUDOLPH t (From the
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
9/10/2012. Chapter 49. Learning Objectives. Learning Objectives (Cont d) Thoracic Trauma
 Thoracic Trauma") Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH
 Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Salt Lake Regional Medical Center, Cardiology. Terron Arbon, Stacy Tukuafu, Dean Porcelli, Paul Allred
 Salt Lake Regional Medical Center, Cardiology Terron Arbon, Stacy Tukuafu, Dean Porcelli, Paul Allred Superior Vena Cava (SVC) Inferior Vena Cava (IVC) Right Atrium (RA) Atrial Appendage Crista Terminalis
Salt Lake Regional Medical Center, Cardiology Terron Arbon, Stacy Tukuafu, Dean Porcelli, Paul Allred Superior Vena Cava (SVC) Inferior Vena Cava (IVC) Right Atrium (RA) Atrial Appendage Crista Terminalis
Echo in Pulmonary HTN
 Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Department of Cardiac, Thoracic and Vascular Sciences University of Padua Cardiac Tamponade. Echocardiography in Diagnosis and Management
 Department of Cardiac, Thoracic and Vascular Sciences University of Padua Cardiac Tamponade. Echocardiography in Diagnosis and Management Luigi P. Badano, MD, FESC, FACC Declaration of interest **Dr. Badano
Department of Cardiac, Thoracic and Vascular Sciences University of Padua Cardiac Tamponade. Echocardiography in Diagnosis and Management Luigi P. Badano, MD, FESC, FACC Declaration of interest **Dr. Badano
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
10. Thick deposits of lipids on the walls of blood vessels, called, can lead to serious circulatory issues. A. aneurysm B. atherosclerosis C.
 Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Πνευμονική υπέρταση και περικαρδιακή συλλογή. Τρόποι αντιμετώπισης
 Πνευμονική υπέρταση και περικαρδιακή συλλογή. Τρόποι αντιμετώπισης Γεώργιος Λάζαρος Καρδιολόγος, Διευθυντής ΕΣΥ Α Πανεπιστημιακή Καρδιολογική Κλινική Ιπποκράτειο Γ.Ν. Αθηνών Pericardial syndromes o Acute
Πνευμονική υπέρταση και περικαρδιακή συλλογή. Τρόποι αντιμετώπισης Γεώργιος Λάζαρος Καρδιολόγος, Διευθυντής ΕΣΥ Α Πανεπιστημιακή Καρδιολογική Κλινική Ιπποκράτειο Γ.Ν. Αθηνών Pericardial syndromes o Acute
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Performance Enhancement. Cardiovascular/Respiratory Systems and Athletic Performance
 Performance Enhancement Cardiovascular/Respiratory Systems and Athletic Performance Functions of the Cardiovascular System Deliver oxygen & nutrients to body tissues Carry wastes from the cells Anatomy
Performance Enhancement Cardiovascular/Respiratory Systems and Athletic Performance Functions of the Cardiovascular System Deliver oxygen & nutrients to body tissues Carry wastes from the cells Anatomy
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
PHYSIOLOGY MeQ'S (Morgan) All the following statements related to blood volume are correct except for: 5 A. Blood volume is about 5 litres. B.
 All the following statements related to blood volume are correct except for: 5 A. Blood volume is about 5 litres. B.") PHYSIOLOGY MeQ'S (Morgan) Chapter 5 All the following statements related to capillary Starling's forces are correct except for: 1 A. Hydrostatic pressure at arterial end is greater than at venous end.
PHYSIOLOGY MeQ'S (Morgan) Chapter 5 All the following statements related to capillary Starling's forces are correct except for: 1 A. Hydrostatic pressure at arterial end is greater than at venous end.
Echocardiography Conference
 Echocardiography Conference David Stultz, MD Cardiology Fellow, PGY-6 September 20, 2005 Atrial Septal Aneurysm Bulging of Fossa Ovalis Associated commonly with Atrial septal defect or small perforations
Echocardiography Conference David Stultz, MD Cardiology Fellow, PGY-6 September 20, 2005 Atrial Septal Aneurysm Bulging of Fossa Ovalis Associated commonly with Atrial septal defect or small perforations
Copyright 2017 American College of Emergency Physicians. All rights reserved.
 POLICY Approved April 2017 Guidelines for the Use of Transesophageal Echocardiography (TEE) in the ED for Cardiac Arrest Approved by the ACEP Board of Directors April 2017 1. Introduction The American
POLICY Approved April 2017 Guidelines for the Use of Transesophageal Echocardiography (TEE) in the ED for Cardiac Arrest Approved by the ACEP Board of Directors April 2017 1. Introduction The American
POCUS for the Internist: Lungs & Pericardial Effusions
 POCUS for the Internist: Lungs & Pericardial Effusions Jeremy S. Boyd, MD, FACEP Asst. Professor of Emergency Medicine Vanderbilt University Medical Illustrations courtesy of Robinson Ferre, MD, FACEP
POCUS for the Internist: Lungs & Pericardial Effusions Jeremy S. Boyd, MD, FACEP Asst. Professor of Emergency Medicine Vanderbilt University Medical Illustrations courtesy of Robinson Ferre, MD, FACEP
An Uncommon Cardiac Etiology of Liver Cirrhosis, Recurrent Ascites, Atrial Fibrillation and Congestive Heart Failure
 Cronicon OPEN ACCESS EC CARDIOLOGY Case Report An Uncommon Cardiac Etiology of Liver Cirrhosis, Recurrent Ascites, Atrial Fibrillation and Congestive Heart Failure Montaser Y Ismail 1 *, Mohammed I Nassar
Cronicon OPEN ACCESS EC CARDIOLOGY Case Report An Uncommon Cardiac Etiology of Liver Cirrhosis, Recurrent Ascites, Atrial Fibrillation and Congestive Heart Failure Montaser Y Ismail 1 *, Mohammed I Nassar
Means failure of heart to pump enough blood to satisfy the need of the body.
 Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased