Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
|
|
|
- Mervin Berry
- 6 years ago
- Views:
Transcription
1 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton
2 Outline of presentation The melanoma epidemic Benefits of early detection Risks of the second or subsequent melanoma What are atypical and/or dysplastic naevi? Monitoring: what, whom, where, when and why? Future developments




3 Melanoma

4 Ulcerated pigmented nodule on elderly white sun damaged skin-bad news. Male, 80 presented with blue/grey ulcerated nodular melanoma. Dead from brain, liver and lung metastases 6 weeks after this picture was taken in summer 2016
5

6 GP referrals up 41% in 5 years, mainly due to NICE guidance The Independent 1 st September 2014
7 Melanoma now 5 th most common UK cancer excluding BCC+ SCC


8 A tale of two cancers... Change in UK mortality Cervical cancer deaths 957 Melanoma deaths 2,067
9

10 South west skin cancer hub-a great source of data

11 Will education reduce skin cancer incidence?
12 Where s the melanoma?

13 It s not the obvious tumour...

14 Presented with bleeding BCC. This melanoma, of which the patient was unaware was discovered on skin check.


15 If preventable, why not prevented? Thick melanoma Old photo shows a much thinner lesion 5 years earlier
16 Can I have my moles checked, doctor? Should we check individual moles, or the whole skin? Can the NHS fund this or should it be private? Who should be checked? How? By whom? At what intervals? And what are we looking for?
17 Stephen Hayes back! Lots of moles, several are atypical History of blistering sunburn in youth Family history of melanoma The 2 larger ones over the left scapula are dermatofibromas I don t want to die from melanoma.. But I don t like having bits of me cut out thank you very much!

18 What do we mean by atypical or dysplastic moles?

19 Which of his 100+ moles will you cut out?

20 Which of his 100+ moles will you cut out?
21 NEWSFLASH!!!! ATYPICAL NAEVI VERY RARELY DEVELOP INTO MELANOMA 80% OF MELANOMAS ARISE DE NOVO FROM CLEAR SKIN MONITORING IN HIGH RISK PATIENTS IS SAFE AND EFFECTIVE AT CATCHING NEW MELANOMAS AT A PRE-INVASIVE STAGE (IN SITU OR MINIMAL BRESLOW THICKNESS)
22 The Genetic Evolution of Melanoma New England J Med 2016; 374: March 10, 2016 Patients with increased numbers of nevi are at increased risk for melanoma. The potential for nevi to serve as melanoma precursor lesions is controversial.2 The malignant transformation of an individual nevus is estimated to occur at a rate of to 0.003% per year.3 In addition, the majority of melanomas arise de novo, and only 20 to 30% of melanomas are associated with a melanocytic nevus.2 Therefore, we think that prophylactic excision of melanocytic nevi has a low potential to reduce melanoma risk and is not warranted.3,4 Instead, clinical surveillance with periodic skin examinations, dermoscopy, and photography are the strategies we suggest for early detection of melanoma
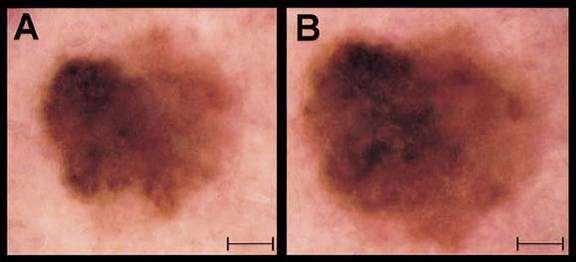
23 Digital dermoscopic monitoring of atypical nevi in patients at risk for melanoma Dermatol Surg October; 33(10): Fuller, Bowen et al Objective : To determine the utility of monitoring dermoscopic photographs of atypical nevi in a high-risk population. Methods :Over a 4.5-year period, digital dermoscopic photographs were taken of clinically atypical nevi at initial and follow-up visits, such that side-by-side comparisons could be made. Results: A total of 5945 lesions were monitored in 297 patients over 3 52 months (median 22 months) and 324 lesions were biopsied. Photographic changes were noted in 96/5945 (1.6%) lesions, which included 64 dysplastic nevi (67%), 25 common nevi (26%), and one melanoma (1.0%). Of six melanomas biopsied during the follow-up period, only one was detected by dermoscopic photographic change at follow-up. Conclusions: Most clinically atypical melanocytic nevi are stable over time, and lesions exhibiting dermoscopic changes are most likely to be dysplastic nevi. While dermoscopy is a useful tool for clinical examination, the sensitivity of dermoscopic monitoring is limited by melanomas that may arise in normal skin or in clinically benign nevi that were not initially photographed. JUST 1 OUT OF ALMOST 6,000 CLINICALLY ATYPICAL NAEVI DEVELOPED INTO A MELANOMA
24
25

26 Atypical naevi indicate increased risk, but are not themselves premalignant. When someone has many atypical naevi, we cannot reasonably cut them all out. Atypical naevi are defined as acquired naevi over 5mm in diameter with asymmetry of shape and colour but no clear cut signs of melanoma. the answer is monitoring.
27 Mole mapping and digital monitoring basic principles The risk of a new melanoma is increased in the following situations -previous history of melanoma -large number of naevi, especially if over or more atypical naevi -severe sun damaged skin -immune suppression (main risk here is squamous cell cancer)
28 How should we monitor patients with atypical moles? -advise patient to observe their own moles? -advise patient to photograph own skin? -professional medical photography individual naevi? -professional medical photography of areas e.g. back, legs, face? -professional medical photography of whole skin? -digital photography of whole skin, with or without digital dermoscopic imaging of particular moles which are atypical? Cost effectiveness and resources must be taken into account in case selection. Currently, practice varies considerably. More research is needed!
29 How to monitor patients with atypical moles? : hierarchy of techniques and cost -advise patient to observe their own moles -advise patient to photograph own skin -professional photography individual naevi -professional photography of areas e.g. back, legs, face -professional photography of whole skin -digital photography of whole skin, with or without digital imaging of particular moles which are atypical Increasing cost
30 How do we do mole mapping and monitoring? Choose the right patients Whole skin photography 2 sets of prints, one to patient, one to notes Show patient (ideally with partner or friend) how to check their skin against the photos Action any new or changed lesions What interval? 3 months is standard, 6 or 12 months may be OK longer term For how long? Debateable, also subject to resources. Technology and research findings are changing-none of this is set in stone!
31
32 How to check the skin with mole mapping At it s simplest, monitoring consists of comparing the patient s whole skin against the photos. If there is no change over time, lesions can be safely assumed to be non malignant, even if they look quite odd.
33 Compare the photos with the patient s skin. We are looking for moles which are new or changed.

34 No change over 6 months is very reassuring Most melanomas change visually over 3 months
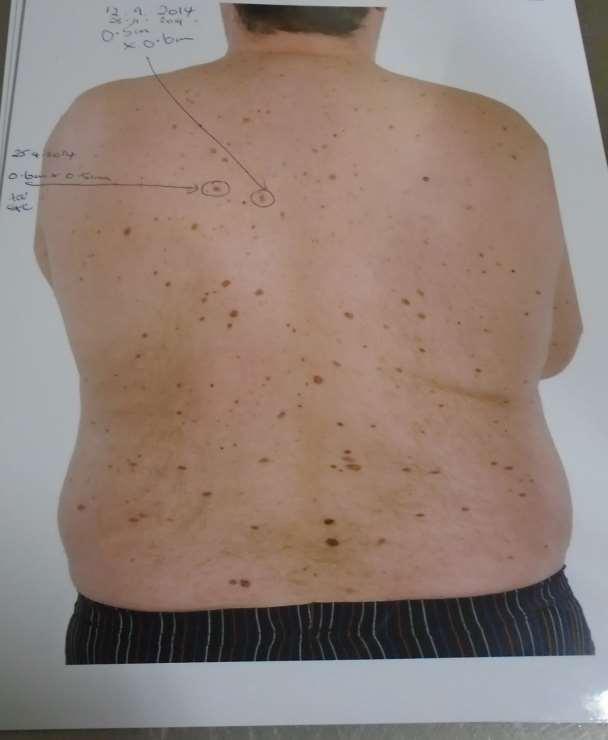
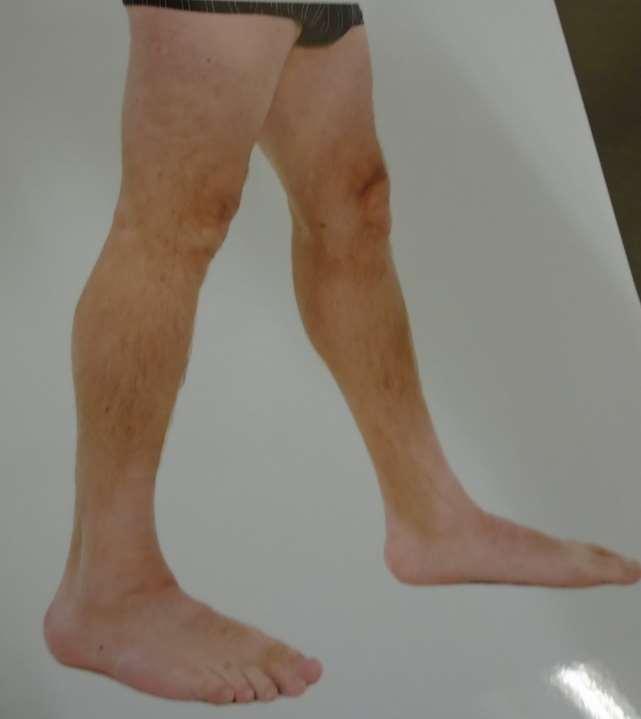
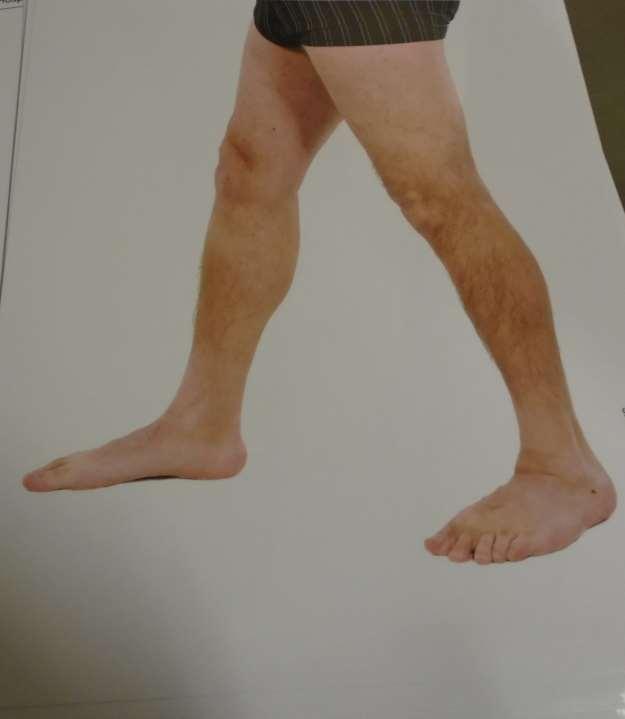
35 Mole mapping and monitoringdiscussion and an example This patient gave written permission for these images to be shared for the purpose of education. He was mole mapped and followed up after the excision of a thin melanoma. Several other naevi have been excised, all proved to be benign (labelled mildly dysplastic.)
36

37

38
39
40

41

42
43

44 These moles were unchanged over 3 years Failure to change over this length of time is strong evidence that they are all completely harmless and should NOT be excised as a precaution
45

46
47

48

49

50

51
52
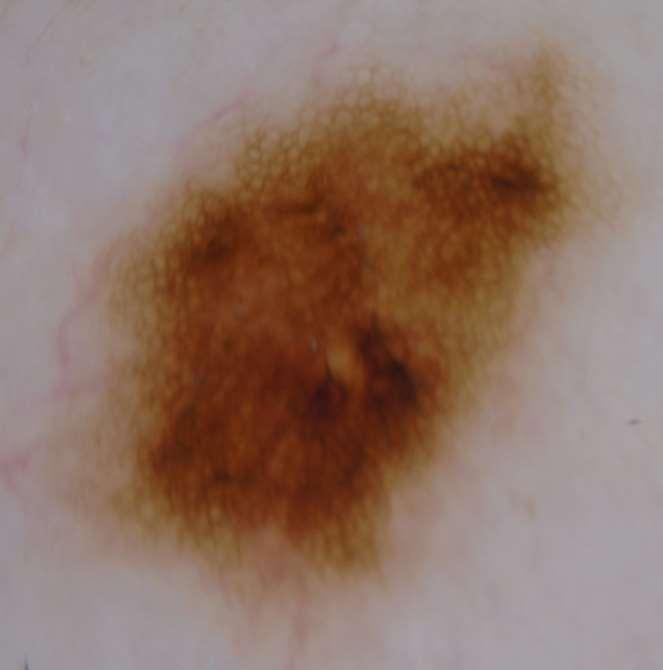
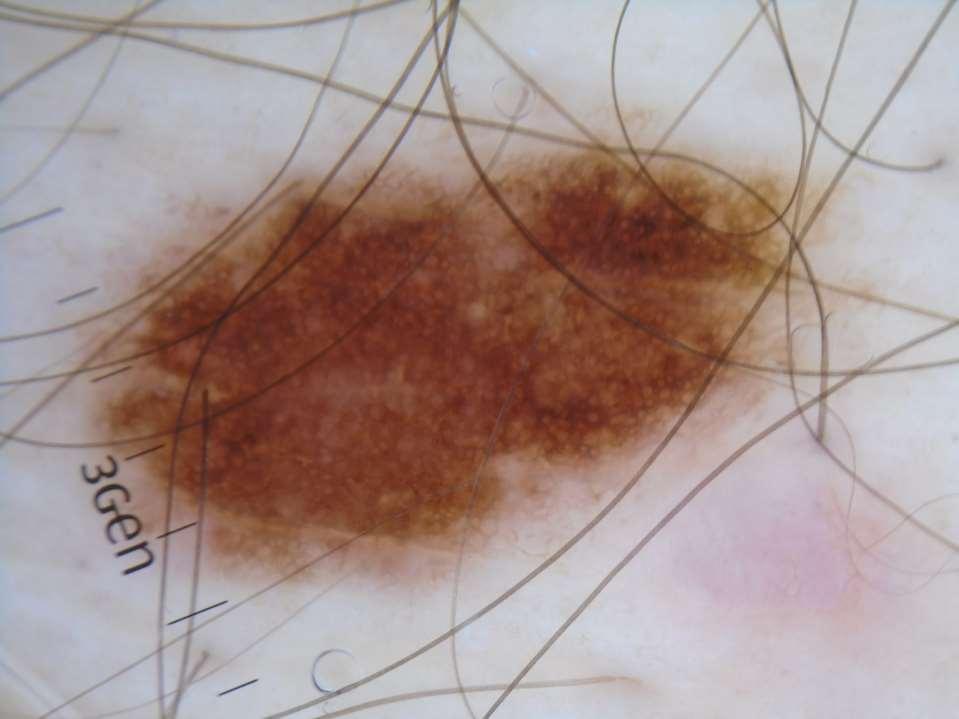
53 These atypical naevi are non symmetrical with variable brown colour and patterns, but lack Argenziano s 7 features of melanoma Atypical pigment network Blue grey areas Radial streaming (streaks/pseudopods) Irregular black blotches Irregular dots and globules Atypical vessels Regression structures (I would add shiny white streaks)

54 No moles had changed over 3 years of monitoring, we can therefore safely say they are harmless NB this is a case study of one but agrees with and illustrates the published trial evidence mentioned earlier (hyperlinks to these studies in final slide, included on your delegate memory drive)

55 How to use mole mapping spot the difference At it s simplest, monitoring consists of comparing the patient s whole skin against the photos. If there is no change over time, lesions can be safely assumed to be non malignant, even if they look quite odd.


56 Just like star spotting in the night sky
57 Following up high risk patients detects thinner melanomas Multiple primary melanoma: the impact of atypical naevi and follow up. BJD [2010, 163(6): ] De Georgi et al Melanoma patients in Florence, Italy between 2000 and 2004 had their records evaluated The presence of atypical naevi was associated with a greater risk of getting a new melanoma, odds ration 3.28 Those who were followed up and had a new melanoma had an average Breslow thickness of 0.36mm Those who did not attend follow up, when they presented with new melanomas the average Breslow thickness was three times thicker at 1.22mm This study provides objective evidence that careful follow up of high risk melanoma patients is associated with the detection of significantly thinner and therefore much more survivable melanomas Conclusion: Follow up of high risk melanoma patients is effective in detecting new melanomas at an earlier stage.
58 Short term or long term monitoring? Short term monitoring Suitable for individual lesions Only monitor flat lesions, which are a bit odd but have no positive features for melanoma Dermoscopic photography is essential 90% of early melanomas will have changed over 12 weeks (beware, some are very slow growing) Long term monitoring Suitable for patients at high risk due to multiple naevi, atypical mole syndrome, personal history of melanoma Immune suppressed? TBP (total body photography) with or without dermoscopy of selected naevi Most melanomas picked up are on monitoring are in situ or very thin.
 There is now strong international evidence that all high risk patients")
59 Internationally, people are encouraged to get their skin checked annually. Germany has rolled out universal skin screening for the over 40s (evidence of benefit is awaited) There is now strong international evidence that all high risk patients should be monitored. The risk is life long and may increase with age, so when should monitoring end?


60 DIGITAL DERMATOSCOPY Digital dermoscopic monitoring Professor Harald Kittler University of Vienna COMPARISON OF SEQUENTIAL IMAGES

61 Follow-up : 7 months, Melanoma in situ 2 Follow-up adds diagnostic information

62

63 Digital dermoscopic monitoring images by kind permission of Professor Harald Kittler, University of Vienna


64 NB the change is usually at the periphery of the naevus

65 How close to the wind dare we sail?
66 Aged 80, lesion had changed over several years.
67 Aged 80, lesion had changed over several years. Fingerprint pattern (fine parallel curved lines)? Blue clods near centre? Mildly chaotic 6mm punch biopsy taken- Diagnosis = solar lentigo, no malignant features Could lesions like this be safely monitored?

68 What about apps and commercial mole mapping?
69 Skinvision.com
 but there is likely to be some value.")
70 There are MANY mole watching Smartphone apps out there, new ones are being created all the time. We don t endorse any (the jury is out) but there is likely to be some value. Potential down side: may be tie ins with skin surgeons (overdiagnosis + monetisation) and patients may not select the right lesions to photograph.
71 Patient performed dermoscopy with Teledermatology Manahan MN, Soyer HP, et al. BJD November 21, doi: /bjd Fifty-eight Australian adults aged years performed skin self-examination and photography using a cheap Smartphone dermoscope at home A total of 309 lesions were patient-photographed and ed to a dermatologist. The patient=-performed dermoscopic images were of adequate quality and telediagnosis of the lesions correlated well with clinical diagnosis The sensitivity of skin self-examination plus mobile teledermoscopy was 81.8% with the patient as denominator and 41.9% with the lesion as denominator. However, patients photographed many banal lesions and missed some suspicious ones CONCLUSION: the details may require some work, but patient performed skin self examination (SSE) with Smartphone dermoscopy is feasible.
72 Mole monitoring-in conclusion We have a melanoma epidemic Public demand for screening and monitoring will increase Monitoring of high risk patients is safe and cost effective. Based on the evidence, it should be happening routinely. The benefits of monitoring lower risk patients are uncertain Self monitoring by patients using Smartphone apps is feasible There are likely to be further developments in this area
73 Hyperlinks to studies cited in this presentation rentissue&
The GP s approach to the patient who is worried about sun, skin and moles. Dr Stephen Hayes
 The GP s approach to the patient who is worried about sun, skin and moles Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Dr Stephen Hayes DECLARATION OF INTERESTS
The GP s approach to the patient who is worried about sun, skin and moles Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Dr Stephen Hayes DECLARATION OF INTERESTS
Dr Stephen Hayes Associate Specialist in Dermatology University Hospital Southampton
 South East Dermatology Transformation and Sustainability Network Guildford, 19 th April 2018 Dermoscopy as an effective skin lesion triage tool in GP surgeries Dr Stephen Hayes Associate Specialist in
South East Dermatology Transformation and Sustainability Network Guildford, 19 th April 2018 Dermoscopy as an effective skin lesion triage tool in GP surgeries Dr Stephen Hayes Associate Specialist in
Skin Cancer A Personal Approach. Dr Matthew Strack Dunedin New Zealand
 Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Cancer Council Australia Wiki Guidelines 2017
 WHAT IS THE ROLE OF SEQUENTIAL DIGITAL DERMOSCOPY IMAGING IN MELANOMA DIAGNOSIS? Cancer Council Australia Wiki Guidelines 2017 SHORT-TERM MONITORING 3 months Any change leads to excision Any melanocytic
WHAT IS THE ROLE OF SEQUENTIAL DIGITAL DERMOSCOPY IMAGING IN MELANOMA DIAGNOSIS? Cancer Council Australia Wiki Guidelines 2017 SHORT-TERM MONITORING 3 months Any change leads to excision Any melanocytic
50 interactive dermoscopic case discussions Dr Stephen Hayes
 50 interactive dermoscopic case discussions Dr Stephen Hayes Annotations will be found on your memory drive, as will 100 case discussions and other learning material Melanoma 2mm thick Ugly duckling-one
50 interactive dermoscopic case discussions Dr Stephen Hayes Annotations will be found on your memory drive, as will 100 case discussions and other learning material Melanoma 2mm thick Ugly duckling-one
Total body photography in high risk patients
 Total body photography in high risk patients Doug Grossman, MD, PhD Department of Dermatology Huntsman Cancer Institute University of Utah Summer AAD F032 Practical Considerations for Patients with Melanoma
Total body photography in high risk patients Doug Grossman, MD, PhD Department of Dermatology Huntsman Cancer Institute University of Utah Summer AAD F032 Practical Considerations for Patients with Melanoma
Dermoscopy-a BRIEF introduction
 Dermoscopy-a BRIEF introduction Aim of presentation -to tell you what dermoscopy is -to show some of what it can do -point the interested learner to further resources Overview of dermoscopy Dermoscopy
Dermoscopy-a BRIEF introduction Aim of presentation -to tell you what dermoscopy is -to show some of what it can do -point the interested learner to further resources Overview of dermoscopy Dermoscopy
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Apps and Telemedicine H. Peter Soyer Dermatology Research Centre
 Apps and Telemedicine H. Peter Soyer Dermatology Research Centre p.soyer@uq.edu.au https://twitter.com/hpsoyer William Gibson The future is already here it's just not very evenly distributed Vision 3D
Apps and Telemedicine H. Peter Soyer Dermatology Research Centre p.soyer@uq.edu.au https://twitter.com/hpsoyer William Gibson The future is already here it's just not very evenly distributed Vision 3D
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Regression 2/3/18. Histologically regression is characterized: melanosis fibrosis combination of both. Distribution: partial or focal!
 Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
6/17/2018. Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things. Bad?
 Dermoscopy of Brown(ish) Things. Bad?") Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things Jennie T. Clarke, MD ssociate Professor of Dermatology University of Utah School of Medicine Bad? 1 Brown(ish) Things Bad Melanoma Pigmented basal
Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things Jennie T. Clarke, MD ssociate Professor of Dermatology University of Utah School of Medicine Bad? 1 Brown(ish) Things Bad Melanoma Pigmented basal
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
22/04/2015. Dermoscopy of Melanoma. Ilsphi Browne. Overview
 Dermoscopy of Melanoma Ilsphi Browne Overview The device Dermoscopic criteria (terminology) Colour Patterns Global features Local features Approach to diagnosing pigmented lesions Other uses in general
Dermoscopy of Melanoma Ilsphi Browne Overview The device Dermoscopic criteria (terminology) Colour Patterns Global features Local features Approach to diagnosing pigmented lesions Other uses in general
Management of Atypical Pigmented Lesions
 Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper:
 This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
Finding Melanoma. Is not easy!
 Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
It can be helpful in some cases of actinic keratosis, Bowen s disease and squamous cell carcinoma
 Dermoscopy Introduction, Terminology and Structures (to be read in conjunction with the Diagnostic Dermoscopic Algorithm) Copyright to Cunliffe TP (Jan. 2017) All rights reserved Introduction Dermoscopy
Dermoscopy Introduction, Terminology and Structures (to be read in conjunction with the Diagnostic Dermoscopic Algorithm) Copyright to Cunliffe TP (Jan. 2017) All rights reserved Introduction Dermoscopy
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Malignant non-melanocytic lesions
 Malignant non-melanocytic lesions Course C023: Fundamentals of Dermoscopy March 4, 2019, 11:20 AM - 11:50 PM Room: 146B Jason B. Lee, MD Professor & Vice Chair Director of Dermatopathology & Pigmented
Malignant non-melanocytic lesions Course C023: Fundamentals of Dermoscopy March 4, 2019, 11:20 AM - 11:50 PM Room: 146B Jason B. Lee, MD Professor & Vice Chair Director of Dermatopathology & Pigmented
INTRODUCTION HOUSEKEEPING June 11 th Dr John Adams Dermatologist/Dermoscopist MOLEMAP NZ/Australia MOLESAFE USA
 INTRODUCTION HOUSEKEEPING June 11 th 2015 Dr John Adams Dermatologist/Dermoscopist MOLEMAP NZ/Australia MOLESAFE USA Program Skin cancer statistics. Dermoscopy description and usefulness. Patient /lesion
INTRODUCTION HOUSEKEEPING June 11 th 2015 Dr John Adams Dermatologist/Dermoscopist MOLEMAP NZ/Australia MOLESAFE USA Program Skin cancer statistics. Dermoscopy description and usefulness. Patient /lesion
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
Histopathological and SIAscopic Correlation of Pigmented Skin Lesions
 Histopathological and SIAscopic Correlation of Pigmented Skin Lesions Professor Sujatha Fernando MBBS(Hon), MSc(London, Distinction), FRSTM&H, FRCPA, FIAC, FACTM Senior Consultant in Anatomical Pathology,
Histopathological and SIAscopic Correlation of Pigmented Skin Lesions Professor Sujatha Fernando MBBS(Hon), MSc(London, Distinction), FRSTM&H, FRCPA, FIAC, FACTM Senior Consultant in Anatomical Pathology,
The impact of GP sub-specialisation and dermatoscopy use on diagnostic accuracy for melanomas in Australia
 The impact of GP sub-specialisation and dermatoscopy use on diagnostic accuracy for melanomas in Australia Cliff Rosendahl, Gail Williams, Diann Eley, Tobias Wilson, Greg Canning, Jeffrey Keir, Ian McColl,
The impact of GP sub-specialisation and dermatoscopy use on diagnostic accuracy for melanomas in Australia Cliff Rosendahl, Gail Williams, Diann Eley, Tobias Wilson, Greg Canning, Jeffrey Keir, Ian McColl,
Disclosure. Objectives. PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016
 PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016 1 Disclosure The speaker has no conflict of interest, financial agreement, or working affiliation with any group or organization.
PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016 1 Disclosure The speaker has no conflict of interest, financial agreement, or working affiliation with any group or organization.
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
MODULE 1. LOCAL AND GENERAL CRITERIA IN PIGMENTED MELANOCYTIC LESIONS.
 DERMOSCOPY TEACHING PROGRAMME Dermoscopy Teaching Programme Module 1 MODULE 1. LOCAL AND GENERAL CRITERIA IN PIGMENTED MELANOCYTIC LESIONS. Dermoscopy is a non-invasive in vivo technique that provides
DERMOSCOPY TEACHING PROGRAMME Dermoscopy Teaching Programme Module 1 MODULE 1. LOCAL AND GENERAL CRITERIA IN PIGMENTED MELANOCYTIC LESIONS. Dermoscopy is a non-invasive in vivo technique that provides
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
DERMATOLOGY PRACTICAL & CONCEPTUAL. Gabriel Salerni 1,2, Teresita Terán 3, Carlos Alonso 1,2, Ramón Fernández-Bussy 1 ABSTRACT
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com The role of dermoscopy and digital dermoscopy follow-up in the clinical diagnosis of melanoma: clinical and dermoscopic features of 99 consecutive primary
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com The role of dermoscopy and digital dermoscopy follow-up in the clinical diagnosis of melanoma: clinical and dermoscopic features of 99 consecutive primary
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
STUDY. Identification of Clinically Featureless Incipient Melanoma Using Sequential Dermoscopy Imaging
 STUDY Identification of Clinically Featureless Incipient Melanoma Using Sequential Dermoscopy Imaging Harald Kittler, MD; Pascale Guitera, MD; Elisabeth Riedl, MD; Michelle Avramidis, MD; Ligia Teban,
STUDY Identification of Clinically Featureless Incipient Melanoma Using Sequential Dermoscopy Imaging Harald Kittler, MD; Pascale Guitera, MD; Elisabeth Riedl, MD; Michelle Avramidis, MD; Ligia Teban,
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Hauora Maori. Map. Non-Melanoma Skin Lesion. Clinically Seborrhoeic Keratosis. Management Options. Punch Biopsy. Refer to Public Skin Lesion Service
 Care map information Information resources for patients and carers Updates to this Care Map Hauora Maori Pacific Skin lesion history Clinical examination and diagnostic test Suspicious of Melanoma Non-Melanoma
Care map information Information resources for patients and carers Updates to this Care Map Hauora Maori Pacific Skin lesion history Clinical examination and diagnostic test Suspicious of Melanoma Non-Melanoma
MELANOMA. 4 Fitzroy Square, London W1T 5HQ Tel: Fax: Registered Charity No.
 MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Dermoscopy in everyday practice. What and Why? When in doubt cut it out? Trilokraj Tejasvi MD
 Dermoscopy in everyday practice Trilokraj Tejasvi MD Assistant Professor, Department of Dermatology, Director Teledermatology services, University of Michigan, Faculty Associate, GLOBAL REACH, Michigan
Dermoscopy in everyday practice Trilokraj Tejasvi MD Assistant Professor, Department of Dermatology, Director Teledermatology services, University of Michigan, Faculty Associate, GLOBAL REACH, Michigan
Digital monitoring by whole body photography and sequential digital dermoscopy detects thinner melanomas
 Digital monitoring by whole body photography and sequential digital dermoscopy detects thinner melanomas Marius Rademaker BM, FRCP(Edin), FRACP, DM; Amanda Oakley MBChB, FRACP, DipHealInf Dermatology Department,
Digital monitoring by whole body photography and sequential digital dermoscopy detects thinner melanomas Marius Rademaker BM, FRCP(Edin), FRACP, DM; Amanda Oakley MBChB, FRACP, DipHealInf Dermatology Department,
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2
 MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/22172 holds various files of this Leiden University dissertation. Author: Rhee, Jasper Immanuel van der Title: Clinical characteristics and management of
Cover Page The handle http://hdl.handle.net/1887/22172 holds various files of this Leiden University dissertation. Author: Rhee, Jasper Immanuel van der Title: Clinical characteristics and management of
The Leeds Teaching Hospitals NHS Trust Looking after your moles
 n The Leeds Teaching Hospitals NHS Trust Looking after your moles Information for patients This leaflet is designed to help you look after your own moles. It is hoped that it will be useful for everyone
n The Leeds Teaching Hospitals NHS Trust Looking after your moles Information for patients This leaflet is designed to help you look after your own moles. It is hoped that it will be useful for everyone
BLINCK A diagnostic algorithm for skin cancer diagnosis combining clinical features with dermatoscopy findings
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com BLINCK A diagnostic algorithm for skin cancer diagnosis combining clinical features with dermatoscopy findings Peter Bourne, MBBS 1, Cliff Rosendahl,
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com BLINCK A diagnostic algorithm for skin cancer diagnosis combining clinical features with dermatoscopy findings Peter Bourne, MBBS 1, Cliff Rosendahl,
Fundamentals of dermoscopy
 Fundamentals of dermoscopy Learning objectives Upon completion of this session, participants should be able to: describe the basic principles of dermoscopy identify features associated with pigmented and
Fundamentals of dermoscopy Learning objectives Upon completion of this session, participants should be able to: describe the basic principles of dermoscopy identify features associated with pigmented and
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Phoebe Rich MD Adjunct Professor OHSU Portland, Oregon
 Nail Tips for Diagnosis and Management of Nail Disorders Winter Clinical Dermatology Conference 2017 Hawaii Phoebe Rich MD Adjunct Professor OHSU Portland, Oregon Objectives diagnostic clues for benign
Nail Tips for Diagnosis and Management of Nail Disorders Winter Clinical Dermatology Conference 2017 Hawaii Phoebe Rich MD Adjunct Professor OHSU Portland, Oregon Objectives diagnostic clues for benign
The diagnostic accuracy of the mobile phone teledermatoscopy
 original research article doi: 10.18282/jsd.v3.i2.178 The diagnostic accuracy of the mobile phone teledermatoscopy Hamza Yildiz 1*, Memet Ersan Bilgili 1, Hasan Aktug Simsek 2 1 Department of Dermatology,
original research article doi: 10.18282/jsd.v3.i2.178 The diagnostic accuracy of the mobile phone teledermatoscopy Hamza Yildiz 1*, Memet Ersan Bilgili 1, Hasan Aktug Simsek 2 1 Department of Dermatology,
ORIGINAL ARTICLE. 980 Journal of Investigative Dermatology (2006), Volume 126 & 2006 The Society for Investigative Dermatology
, Volume 126 & 2006 The Society for Investigative Dermatology") ORIGINAL ARTICLE Results from an Observational Trial: Digital Epiluminescence Microscopy Follow-Up of Atypical Nevi Increases the Sensitivity and the Chance of Success of Conventional Dermoscopy in Detecting
ORIGINAL ARTICLE Results from an Observational Trial: Digital Epiluminescence Microscopy Follow-Up of Atypical Nevi Increases the Sensitivity and the Chance of Success of Conventional Dermoscopy in Detecting
Key factors in successfully integrating dermoscopy into your clinical practice
 Key factors in successfully integrating dermoscopy into your clinical practice S051 Dilemmas and challenges in skin cancer therapies and management Monday, March 4 th 2019 (9AM-12PM) Room 209A 10:56-11:09AM
Key factors in successfully integrating dermoscopy into your clinical practice S051 Dilemmas and challenges in skin cancer therapies and management Monday, March 4 th 2019 (9AM-12PM) Room 209A 10:56-11:09AM
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
=C 0= C8E4 <4;0=><0 3806=>B8B
 4558284=C 0=3 45542C8E4 B8B Wednesday 20 th November 2002 Centenary Institute of Cancer Medicine & Cell Biology Royal Prince Alfred Hospital Missenden Road Camperdown NSW WORKSHOP SUMMARY
4558284=C 0=3 45542C8E4 B8B Wednesday 20 th November 2002 Centenary Institute of Cancer Medicine & Cell Biology Royal Prince Alfred Hospital Missenden Road Camperdown NSW WORKSHOP SUMMARY
Introduction to Dermoscopy. Nicholas Compton, MD June 16, 2010
 Introduction to Dermoscopy Nicholas Compton, MD June 16, 2010 Overview What is dermoscopy Brief history Types of dermoscopy General approach to lesion of interest 2 step algorithm 3-point checklist Practice
Introduction to Dermoscopy Nicholas Compton, MD June 16, 2010 Overview What is dermoscopy Brief history Types of dermoscopy General approach to lesion of interest 2 step algorithm 3-point checklist Practice
Associate Professor Amanda Oakley. Professor H. Peter Soyer. Academic Dermatologist The University of Queensland Brisbane. Dermatologist Hamilton
 Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-10:30 WS #3: Dermoscopy Workshop Part 1 11:00-13:00 WS
Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-10:30 WS #3: Dermoscopy Workshop Part 1 11:00-13:00 WS
Dermoscopy Quiz 3-Point Checklist Algorithm
 Dermoscopy Quiz 3-Point Checklist Algorithm GLOBAL PATTERN Globular LOCAL CRITERIA Aggregated globules Milia-like cysts 3 POINT CHECK LIST Symmetrical No abnormal net Slight Blue-white veil BENIGN MELANOCYTIC
Dermoscopy Quiz 3-Point Checklist Algorithm GLOBAL PATTERN Globular LOCAL CRITERIA Aggregated globules Milia-like cysts 3 POINT CHECK LIST Symmetrical No abnormal net Slight Blue-white veil BENIGN MELANOCYTIC
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
STUDY. Risks and Benefits of Sequential Imaging of Melanocytic Skin Lesions in Patients With Multiple Atypical Nevi
 Risks and Benefits of Sequential Imaging of Melanocytic Skin Lesions in Patients With Multiple Atypical Nevi Harald Kittler, MD; Michael Binder, MD STUDY Objective: To evaluate the utility of sequential
Risks and Benefits of Sequential Imaging of Melanocytic Skin Lesions in Patients With Multiple Atypical Nevi Harald Kittler, MD; Michael Binder, MD STUDY Objective: To evaluate the utility of sequential
Growth rate of melanoma in vivo and correlation with dermatoscopic and dermatopathologic findings
 Dermatology Practical & Conceptual www.derm101.com Growth rate of melanoma in vivo and correlation with dermatoscopic and dermatopathologic findings Jürgen Beer, M.D. 1, Lina Xu, M.D. 1, Philipp Tschandl,
Dermatology Practical & Conceptual www.derm101.com Growth rate of melanoma in vivo and correlation with dermatoscopic and dermatopathologic findings Jürgen Beer, M.D. 1, Lina Xu, M.D. 1, Philipp Tschandl,
Revised Pattern Analysis: a method for the accurate diagnosis of pigmented skin lesions
 Dermatoscopy for Students A concise outline of: Revised Pattern Analysis: a method for the accurate diagnosis of pigmented skin lesions And Chaos and Clues: a decision algorithm for routine practice to
Dermatoscopy for Students A concise outline of: Revised Pattern Analysis: a method for the accurate diagnosis of pigmented skin lesions And Chaos and Clues: a decision algorithm for routine practice to
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Multispectral Digital Skin Lesion Analysis. Summary
 Subject: Multispectral Digital Skin Lesion Analysis Page: 1 of 8 Last Review Status/Date: March 2016 Multispectral Digital Skin Lesion Analysis Summary There is interest in noninvasive devices that will
Subject: Multispectral Digital Skin Lesion Analysis Page: 1 of 8 Last Review Status/Date: March 2016 Multispectral Digital Skin Lesion Analysis Summary There is interest in noninvasive devices that will
CANCER INSIGHT. FOR GPs. Summer 2018 WHAT YOU NEED TO KNOW ABOUT SKIN CANCER VISIT. our Skin Cancer Recognition Toolkit at
 CANCER INSIGHT FOR GPs Summer 2018 WHAT YOU NEED TO KNOW ABOUT SKIN CANCER VISIT our Skin Cancer Recognition Toolkit at www.doctors.net. uk/sct Cancer Research UK, Angel Building, 407 St John Street, London
CANCER INSIGHT FOR GPs Summer 2018 WHAT YOU NEED TO KNOW ABOUT SKIN CANCER VISIT our Skin Cancer Recognition Toolkit at www.doctors.net. uk/sct Cancer Research UK, Angel Building, 407 St John Street, London
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Professor Michael Eccles
 Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines
 CLINICAL GUIDANCE The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines Julia Newton Bishop, Veronique Bataille, Alice Gavin, Marko Lens, Jerry Marsden, Tania Mathews
CLINICAL GUIDANCE The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines Julia Newton Bishop, Veronique Bataille, Alice Gavin, Marko Lens, Jerry Marsden, Tania Mathews
Abrupt Intralesional Color Change on Dermoscopy as a New Indicator of Early Superficial Spreading Melanoma in a Japanese Woman
 Published online: June 24, 2015 1662 6567/15/0072 0123$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: June 24, 2015 1662 6567/15/0072 0123$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Dermoscopy STFM Richard Usatine, MD 5/2/16. Disclosure Statement: Some Dermatoscopes. Dermoscopy Video. Thanks to Dr.
 Disclosure Statement: Dermoscopy STFM 2016 Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, Clinic University of Texas
Disclosure Statement: Dermoscopy STFM 2016 Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, Clinic University of Texas
Dermatology pilots. Ram Patel GPwSI Dermatology Gateway lead for Dermatology.
 Dermatology pilots Ram Patel GPwSI Dermatology Gateway lead for Dermatology Assessing needs Extent of skin disease: Study of 1500 people age 15 years and over 54% reported a skin condition 14% seek advice
Dermatology pilots Ram Patel GPwSI Dermatology Gateway lead for Dermatology Assessing needs Extent of skin disease: Study of 1500 people age 15 years and over 54% reported a skin condition 14% seek advice
Features Causing Confusion between Basal Cell Carcinoma and Squamous Cell Carcinoma in Clinical Diagnosis
 TH Ryu, et al pissn 1013-9087ㆍeISSN 2005-3894 Ann Dermatol Vol. 30, No. 1, 2018 https://doi.org/10.5021/ad.2018.30.1.64 ORIGINAL ARTICLE Features Causing Confusion between Basal Cell Carcinoma and Squamous
TH Ryu, et al pissn 1013-9087ㆍeISSN 2005-3894 Ann Dermatol Vol. 30, No. 1, 2018 https://doi.org/10.5021/ad.2018.30.1.64 ORIGINAL ARTICLE Features Causing Confusion between Basal Cell Carcinoma and Squamous
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Looking after your moles
 Who is at increased risk? This leaflet is designed to help you look after your own moles. It is hoped that it will be useful for everyone but it may be especially valuable for people who are at increased
Who is at increased risk? This leaflet is designed to help you look after your own moles. It is hoped that it will be useful for everyone but it may be especially valuable for people who are at increased
Talking to Your Clients About Skin Cancer. Objectives 9/9/2017. Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017
 Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Dermoscopy. Enhanced Diagnostic Ability: Pigmented Lesions. Ted Rosen, MD Baylor College of Medicine Houston, Texas
 Dermoscopy Enhanced Diagnostic Ability: Pigmented Lesions Ted Rosen, MD Baylor College of Medicine Houston, Texas Faculty Disclosure Statement No conflicts relevant to this workshop! Sir William Osler
Dermoscopy Enhanced Diagnostic Ability: Pigmented Lesions Ted Rosen, MD Baylor College of Medicine Houston, Texas Faculty Disclosure Statement No conflicts relevant to this workshop! Sir William Osler
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Nonmelanoma skin cancers
 Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Dr Amanda Oakley. Dermatologist Dept of Dermatology, Health Waikato Adjunct Associate Professor, Waikato Clinical Campus
 Dr Amanda Oakley Dermatologist Dept of Dermatology, Health Waikato Adjunct Associate Professor, Waikato Clinical Campus 14:00-16:00 WS #14: Dermoscopy Part 1 Skin Lesions and Dermatoscopy 16 August 2018
Dr Amanda Oakley Dermatologist Dept of Dermatology, Health Waikato Adjunct Associate Professor, Waikato Clinical Campus 14:00-16:00 WS #14: Dermoscopy Part 1 Skin Lesions and Dermatoscopy 16 August 2018
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Imaging Technologies to Assist in Melanoma Detec3on Prac3cal Considera3ons for Pa3ents with Melanoma/Dysplas3c Nevi
 Imaging Technologies to Assist in Melanoma Detec3on Prac3cal Considera3ons for Pa3ents with Melanoma/Dysplas3c Nevi Michael A. Marche@, MD Assistant ABending, Dermatology Service Memorial Sloan KeBering
Imaging Technologies to Assist in Melanoma Detec3on Prac3cal Considera3ons for Pa3ents with Melanoma/Dysplas3c Nevi Michael A. Marche@, MD Assistant ABending, Dermatology Service Memorial Sloan KeBering
Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report
 Case Reports in Oncological Medicine, Article ID 206260, 4 pages http://dx.doi.org/10.1155/2014/206260 Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report Sharad P. Paul 1,2,3 1 Skin
Case Reports in Oncological Medicine, Article ID 206260, 4 pages http://dx.doi.org/10.1155/2014/206260 Case Report Micromelanomas: A Review of Melanomas 2mmand a Case Report Sharad P. Paul 1,2,3 1 Skin
p16 Genetic Test Reporting Counseling Protocol Flip Chart
 p16 Genetic Test Reporting Counseling Protocol Flip Chart Chromosomes, Gene, & Protein Cell Nucleus Chromosomes Gene Protein Adapted from Understanding Gene Testing,, NIH, 1995 Cancer Normal cell Disease
p16 Genetic Test Reporting Counseling Protocol Flip Chart Chromosomes, Gene, & Protein Cell Nucleus Chromosomes Gene Protein Adapted from Understanding Gene Testing,, NIH, 1995 Cancer Normal cell Disease
Professor Peter Soyer. Academic Dermatologist Brisbane, Australia
 Professor Peter Soyer Academic Dermatologist Brisbane, Australia What s New in Melanoma Dermatology Research Centre, The University of Queensland, School of Medicine, Translational Research Institute &
Professor Peter Soyer Academic Dermatologist Brisbane, Australia What s New in Melanoma Dermatology Research Centre, The University of Queensland, School of Medicine, Translational Research Institute &
Non-melanocytic Patterns
 Non-melanocytic Lesions Non-melanocytic Patterns Michelle Tarbox, MD Assistant Professor of Dermatology and Dermatopathology Texas Tech University Health Sciences Center 2018 Seborrheic keratoses Acanthotic
Non-melanocytic Lesions Non-melanocytic Patterns Michelle Tarbox, MD Assistant Professor of Dermatology and Dermatopathology Texas Tech University Health Sciences Center 2018 Seborrheic keratoses Acanthotic
BJD British Journal of Dermatology. Summary. What s already known about this topic? CLINICAL AND LABORATORY INVESTIGATIONS
 CLINICAL AND LABORATORY INVESTIGATIONS BJD British Journal of Dermatology Pigmented nodular melanoma: the predictive value of dermoscopic features using multivariate analysis M.A. Pizzichetta, 1 H. Kittler,
CLINICAL AND LABORATORY INVESTIGATIONS BJD British Journal of Dermatology Pigmented nodular melanoma: the predictive value of dermoscopic features using multivariate analysis M.A. Pizzichetta, 1 H. Kittler,
Associate Professor Amanda Oakley. Professor H. Peter Soyer. Academic Dermatologist The University of Queensland Brisbane. Dermatologist Hamilton
 Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-9:25 WS #94: Teledermatology Case Reports 9:35-10:30
Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-9:25 WS #94: Teledermatology Case Reports 9:35-10:30
comedo-like openings (clods, brown or orange & circles) milia-like cysts (dots or clods, white) 1/29/18 Dotted vessels are also commonly seen in SCC
 milia-like cysts (dots or clods, white) 1/29/18 Dotted vessels are also commonly seen in SCC") Brown circles Dotted vessels are also commonly seen in SCC Step1 1. Nevus (unequivocal) 2. DF/IDN 3. BCC 4. SCC Network Patchy network Peripheral network & central hypopigmentation DF: network with central
Brown circles Dotted vessels are also commonly seen in SCC Step1 1. Nevus (unequivocal) 2. DF/IDN 3. BCC 4. SCC Network Patchy network Peripheral network & central hypopigmentation DF: network with central
MELANOMA: HANDS-ON OR HANDS-OFF?
 MELANOMA: HANDS-ON OR HANDS-OFF? M SCHAMM MBChB (Pret), FCS (SA) Endocrine and Transplant Surgeon, Department of Surgery, University of the Witwatersrand; and Clinical Head Transplant Surgery, Charlotte
MELANOMA: HANDS-ON OR HANDS-OFF? M SCHAMM MBChB (Pret), FCS (SA) Endocrine and Transplant Surgeon, Department of Surgery, University of the Witwatersrand; and Clinical Head Transplant Surgery, Charlotte
Clinical and Dermoscopic Features of Thin Nodular Melanoma
 Clinical and Dermoscopic Features of Thin Nodular Melanoma A study of the International Dermoscopy Society Coordinator: Dr. Alexander J. Stratigos and colleagues, alstrat2@gmail.com ** Extended to May
Clinical and Dermoscopic Features of Thin Nodular Melanoma A study of the International Dermoscopy Society Coordinator: Dr. Alexander J. Stratigos and colleagues, alstrat2@gmail.com ** Extended to May
Skin Cancer. Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts Dr Elizabeth Ogden
 Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
What is melanoma? Melanoma dealing with the diagnosis. What is melanoma?
 Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Yes. Breaking Bad II: Dermoscopy of Pink-ish Things. Does it Fit? Yes 6/17/2018. Yes. Joslyn Kirby, MD, MS, MEd
 Breaking Bad II: Dermoscopy of Pink-ish Things Joslyn Kirby, MD, MS, MEd Yes Observe Yes Step 2. Fit a Benign Nevus Pattern? Does it Fit? Step 1: Melanocytic? pigment network, globules, homogeneous? No
Breaking Bad II: Dermoscopy of Pink-ish Things Joslyn Kirby, MD, MS, MEd Yes Observe Yes Step 2. Fit a Benign Nevus Pattern? Does it Fit? Step 1: Melanocytic? pigment network, globules, homogeneous? No