General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
|
|
|
- Charity Walton
- 5 years ago
- Views:
Transcription
1 General History 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious for minutes in the morning.
2 General History DM under regular medical control for 10 years. Blurred vision, intermittent bilateral costal margin pain and leg muscle spasm many times in recent years. Dizziness when changing from lying to sitting position recently.
3 General History Three days ago, she began to have mild cough with whitish sputum. She also felt fatigue, anorexia, dry mouth and back soreness. She denied fever, chillness or shortness of breath.
4 General History She was doing morning exercise with her husband in a park when she suddenly lost her conscious and fell down. Her husband mentioned that she looked pale, but no vomiting, clonic movement or cold sweating was noted. She denied any pre-syncope aura, headache, chest tightness, dyspnea,, palpitation, abdominal pain and digital numbness.
5 General History At our ER, Physical Examination revealed mild fever, hypertension and tachycardia. Two ablation wounds were found on her right elbow and occipital area. Neurological functions are normal. Routine chest x-ray x showed numerous lung masses. There were rales over bilateral lung fields on auscultation. She was admitted to our ward for work up of her syncope and lung masses.
6 Laboratory Data Blood WBC [ /uL] ] : Neutrophil [40-74%] : 82.9 Lymphocyte [19-48%] : 8.5 Left shift : ++ RBC [ /uL] ] : 3.53 Hb [12-18g 18g/dL] ] : 11.3 Hct [37-52%] : 33.1
7 Laboratory Data Biochemistry Glucose [80-140mg 140mg/dL] ] : 209 CK [ IU/L] : 158 LDH [ IU/L] : 191 Na [ meq/L] 158meq/L] : 133

8
9 Imaging findings:chest x-rayx Multiple, ill-defined radio-opaque opaque densities over both lungs : -Infarction -Pneumonia -Lung Abscesses staphylococci, staphylococci, klebsiella,, TB, anaerobic bacteria and various fungi -Metastatic carcinoma -Granuloma caused by collagen vascular disease Blunting of right CP angle : -Pleural effusion -Pneumonia of RLL

10

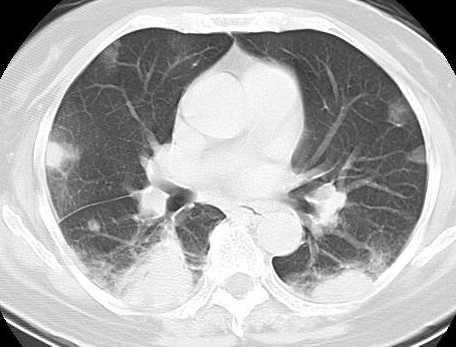
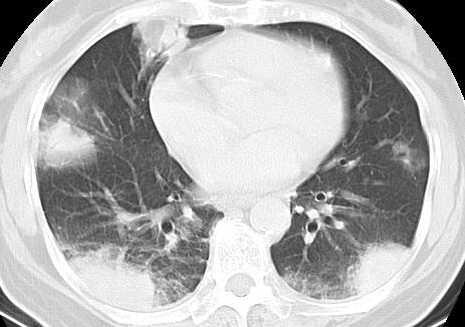
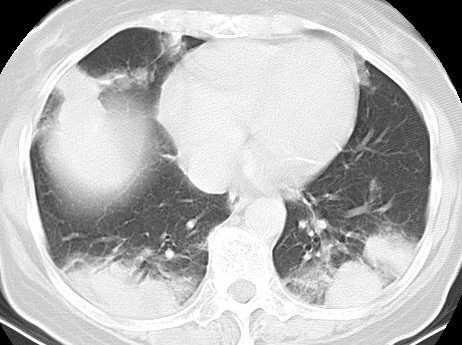
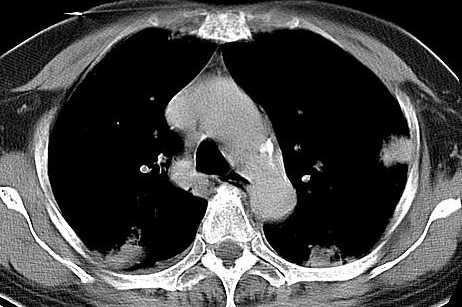
11 Lung window
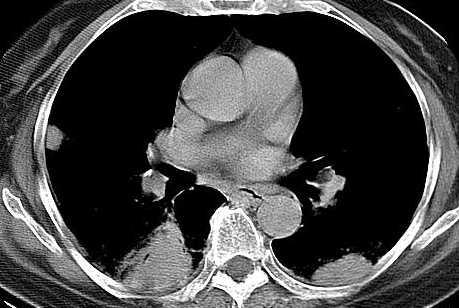
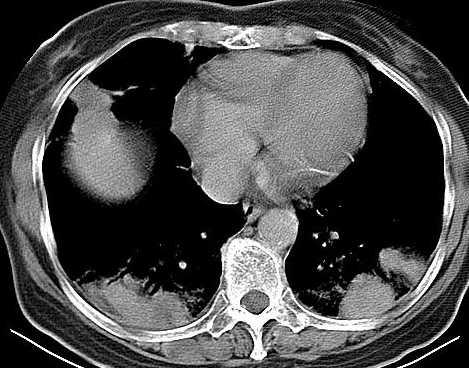
12 Imaging findings:chest CT Multiple, wedge-shaped and lobulated hyperdense masses at the periphery of both lungs: a) Originates from the lung -Metastatic carcinoma -Pneumonia -Lung abscesses a) Originates from the pleura -Metastatic carcinoma -Malignant mesothelioma


13 Brain CT:Grossly normal, no specific findings.
14 Differential Diagnosis Pneumonia Metastatic carcinoma Lung abscesses Infarction Granuloma Malignant Mesothelioma
15 Pathological findings CT guided biopsy of RLL mass Cryptococcosis was proved by PAS and mucicarmine stain.
16 Discussion Cryptococcosis is an opportunistic infection caused by inhaling the fungus Cryptococcus neoformans. C. neoformans is found worldwide in soil contaminated with pigeon or other bird droppings. Cryptococcosis may be limited to the lungs,but frequently spreads throughout the body. It is often fatal if it infects the central nervous system.
17 Discussion Most pulmonary infections are asymptomatic or self-limiting limiting in healthy individuals. Cryptococcal pneumonia has symptoms similar to other pneumonias (cough, chest pain, difficulty breathing), making it difficult to accurately diagnose. Most patients are not diagnosed as having cryptococcosis until they show signs of cryptococcal meningitis.
18 Discussion Pulmonary Cryptococcosis : cough, low-grade fever, pleuritic pain, difficulty breathing. CNS Cryptococcosis: Symptoms usually develop slowly over several months, and include headache, drowsiness, dizziness, irritability, confusion, nausea, vomiting, neck stiffness and focal neurological defects, such as ataxia.
19 Discussion Laboratory Diagnosis A) Direct microscopy : India Ink staining of sputum, bronchial washings or CSF. PAS+ Mucicarmine for staining tissue sections. B) Culture : blood or CSF C) Serology : detection of cryptococcal antigen by latex agglutination.

20 India ink preparation of CSF showing a typical yeast cell of C. neoformans surrounded by a characteristic wide gelatinous capsule.
21 Discussion:Radiographic appearances of pulmonary cryptococcal disease Major features on chest x-ray x and CT: -bilateral more common than unilateral -irregular airspace opacities -segmental or lobar consolidation -discrete nodules or masses(up to 3 cm)with or without adjacent tiny satellite nodules -tiny subpleural or peripheral interstitial nodules with adjacent interstitial thickening or pleural thickening
22 Discussion:Radiographic appearances of pulmonary cryptococcal disease Minor features on chest x-ray x and CT: pleural effusions lymph nodes enlargement Cavitation or calcification within nodules

![lobe].](/docs-images/94/121316561/images/23-1.jpg "Marked interval progression")
23 X-ray showing lobar consolidation [right upper lobe]. Marked interval progression of air-space consolidation.


24 Initial posteroanterior chest radiograph shows ill-defined vaguely nodular air-space opacities (arrows). PA chest radiograph shows 1.5-cm cavitary RUL nodule.



25 CT shows subpleural location and polygonal shape of the mass. CT shows multiple irregular airspace opacities in bilateral lungs, predominant in RLL.
26 Discussion Treatment Intravenous Amphotericin B, with or without 5-Flucytosine, 5 is given several weeks until the patient is stable, after which the patient is given oral fluconazole to prevent the relapse of cryptococcosis.
27 Discussion Prognosis 1. Untreated cryptococcosis is always fatal. 2. Most deaths are attributable to cryptococcal meningitis and occur within two weeks after diagnosis. 3. Once the cryptococcosis infection has been successfully treated, individuals may be left with a variety of neurologic symptoms.
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Cryptococcal Meningitis
 Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
KAP conference 19 th March 2008: Dr Mohamed Hussein Jin.
 SENSITIVITY PATTERNS, SEROTYPES OF CRYPTOCOCCUS NEOFORMANS AND DIAGNOSTIC VALUE OF INDIA INK IN PATIENTS WITH CRYPTOCOCCAL MENINGITIS AT KENYATTA NATIONAL HOSPITAL. KAP conference 19 th March 2008: Dr
SENSITIVITY PATTERNS, SEROTYPES OF CRYPTOCOCCUS NEOFORMANS AND DIAGNOSTIC VALUE OF INDIA INK IN PATIENTS WITH CRYPTOCOCCAL MENINGITIS AT KENYATTA NATIONAL HOSPITAL. KAP conference 19 th March 2008: Dr
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Neurosciences- Lecture 2 Virus associated meningitis Polio Virus
 Al- Balqa Applied University Faculty of Medicine Neurosciences- Lecture 2 Virus associated meningitis Polio Virus Dr. Hala Al Daghistani The most important Enteroviruses are the three poliovirus serotypes
Al- Balqa Applied University Faculty of Medicine Neurosciences- Lecture 2 Virus associated meningitis Polio Virus Dr. Hala Al Daghistani The most important Enteroviruses are the three poliovirus serotypes
NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C.
 NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C. Past Medical History AIDS/HIV disease Anemia Asthma Bronchitis Cancer Date of last Chest X-ray Diabetes Mellitus, Type I Diabetes Mellitus,
NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C. Past Medical History AIDS/HIV disease Anemia Asthma Bronchitis Cancer Date of last Chest X-ray Diabetes Mellitus, Type I Diabetes Mellitus,
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
SWABCHA Fact Sheet: Tuberculosis (TB)
") SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Bacterial pneumonia with associated pleural empyema pleural effusion
 EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
EMPYEMA Synonyms : - Parapneumonic effusion - Empyema thoracis - Bacterial pneumonia - Pleural empyema, pleural effusion - Lung abscess - Complicated parapneumonic effusions (CPE) 1 Bacterial pneumonia
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
HASPI Medical Biology Lab 03
 Patient 1001 is a 42-year-old female that is experiencing severe heartburn, abdominal pain, bloating, nausea, and vomiting. Ulcers Bleeding sores in the stomach or intestine Gallbladder Disease Gallstones
Patient 1001 is a 42-year-old female that is experiencing severe heartburn, abdominal pain, bloating, nausea, and vomiting. Ulcers Bleeding sores in the stomach or intestine Gallbladder Disease Gallstones
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Case Presentation. Intern Tutor VS 2007/01/26
 Case Presentation Intern 8931150 Tutor VS 2007/01/26 About The Patient 38 years old worker ID: M120794700 Admission date: 2006/12/28 C.C.: Fever with headache for 2 days Present Illness Smoker, alcoholism
Case Presentation Intern 8931150 Tutor VS 2007/01/26 About The Patient 38 years old worker ID: M120794700 Admission date: 2006/12/28 C.C.: Fever with headache for 2 days Present Illness Smoker, alcoholism
Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD
 Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Pulmonary Cryptococcosis in Patients Without HIV Infection* Judith A. Aberg, MD; Linda M. Mundy, MD; and William G. Powderly, MD Purpose: To further elucidate the diagnostic and therapeutic approaches
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 5: Cough
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 5: Cough This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. So Ms. Chen, tell me what is your average
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 5: Cough This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. So Ms. Chen, tell me what is your average
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
RAPIDLY PROGRESSIVE PULMONARY CRYPTOCOCCOSIS WITH CAVITATION IN AN IMMUNOCOMPETENT WOMAN: A CASE REPORT AND LITERATURE REVIEW
 RAPIDLY PROGRESSIVE PULMONARY CRYPTOCOCCOSIS WITH CAVITATION IN AN IMMUNOCOMPETENT WOMAN: A CASE REPORT AND LITERATURE REVIEW Junyan Qu, Xiaohui Wang, Yanbin Liu and Xiaoju Lv Center of Infectious Disease,
RAPIDLY PROGRESSIVE PULMONARY CRYPTOCOCCOSIS WITH CAVITATION IN AN IMMUNOCOMPETENT WOMAN: A CASE REPORT AND LITERATURE REVIEW Junyan Qu, Xiaohui Wang, Yanbin Liu and Xiaoju Lv Center of Infectious Disease,
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland
 The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland Principle of Harm Reduction First Do No Harm Hippocratic Oath I will use treatment
The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland Principle of Harm Reduction First Do No Harm Hippocratic Oath I will use treatment
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Review Article Correlation between Clinical Characteristics and Chest Computed Tomography Findings of Pulmonary Cryptococcosis
 Pulmonary Medicine Volume 2015, Article ID 703407, 7 pages http://dx.doi.org/10.1155/2015/703407 Review Article Correlation between Clinical Characteristics and Chest Computed Tomography Findings of Pulmonary
Pulmonary Medicine Volume 2015, Article ID 703407, 7 pages http://dx.doi.org/10.1155/2015/703407 Review Article Correlation between Clinical Characteristics and Chest Computed Tomography Findings of Pulmonary
MENINGITIS CRYPTOCOCCAL. learn about the symptoms, diagnosing and treating this disease
 CRYPTOCOCCAL MENINGITIS learn about the symptoms, diagnosing and treating this disease A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS JANAURY 2007 Cryptococcal
CRYPTOCOCCAL MENINGITIS learn about the symptoms, diagnosing and treating this disease A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS JANAURY 2007 Cryptococcal
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Pulmonary Cryptococcosis in an HIV-infected Patient
 Case Report Vol. 28 No. 3 Pulmonary Cryptococcosis:- Wongkulab P, et al. 203 Pulmonary Cryptococcosis in an HIV-infected Patient Panuwat Wongkulab, M.D., Nontakan Nuntachit, M.D., Romanee Chaiwarith, M.D.,
Case Report Vol. 28 No. 3 Pulmonary Cryptococcosis:- Wongkulab P, et al. 203 Pulmonary Cryptococcosis in an HIV-infected Patient Panuwat Wongkulab, M.D., Nontakan Nuntachit, M.D., Romanee Chaiwarith, M.D.,
Opportunistic Infections BHIVA Guidelines
 Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Bronchioloalveolar Carcinoma Mimicking DILD:
 Bronchioloalveolar Carcinoma Mimicking DILD: A Case Report 1 Ju Young Lee, M.D., In Jae Lee, M.D., Dong Gyu Kim, M.D. 2, Soo Kee Min, M.D. 3, Min-Jeong Kim, M.D., Sung Il Hwang, M.D., Yul Lee, M.D., Sang
Bronchioloalveolar Carcinoma Mimicking DILD: A Case Report 1 Ju Young Lee, M.D., In Jae Lee, M.D., Dong Gyu Kim, M.D. 2, Soo Kee Min, M.D. 3, Min-Jeong Kim, M.D., Sung Il Hwang, M.D., Yul Lee, M.D., Sang
Fungal Meningitis. Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse Bern
 Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
A Case of Pediatric Plasma Cell Granuloma
 August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
Morbidity Conference. Presented by 肝膽腸胃科張瀚文
 Morbidity Conference Presented by 肝膽腸胃科張瀚文 Chief Complaint General weakness for three days Present Illness This 63-year-old female with diabetes and on oral hypoglycemic agents presented with 3-day history
Morbidity Conference Presented by 肝膽腸胃科張瀚文 Chief Complaint General weakness for three days Present Illness This 63-year-old female with diabetes and on oral hypoglycemic agents presented with 3-day history
Fungal Diseases of the Respiratory System
 Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Scedosporium apiospermum
 223 Scedosporium apiospermum 1 1) 2) 3) 4) 5) 1) 2) 3) 4) 5) 16 7 14 16 10 12 Candida Aspergillus 82 2000 10 2001 1 12 MRI 2 1 Scedosporium apiospermum Key words: Scedosporium apiospermum, Aspergillus,
223 Scedosporium apiospermum 1 1) 2) 3) 4) 5) 1) 2) 3) 4) 5) 16 7 14 16 10 12 Candida Aspergillus 82 2000 10 2001 1 12 MRI 2 1 Scedosporium apiospermum Key words: Scedosporium apiospermum, Aspergillus,
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Thoracoscopy for Lung Cancer
 Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
Thrombotic Microangiopathies
 Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Past Medical History. Chief Complaint: Patient Name: Appointment Date: Page 1
 Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Case 5 15-year-old male
 Case 5 15-year-old male Present illness: Six months ago, abnormality of ECG was incidentally detected by annual health check. His blood level of γ-gtp, HbA1c and norepinephrine were elevated; however,
Case 5 15-year-old male Present illness: Six months ago, abnormality of ECG was incidentally detected by annual health check. His blood level of γ-gtp, HbA1c and norepinephrine were elevated; however,
Viruses, bacteria, fungus, parasites (in rare cases) or other organisms can cause pneumonia.
 or other organisms can cause pneumonia.") 1 Pneumonia Pneumonia is an infection which inflames the air sacs either in one or both of the lungs. The air sacs are generally filled with fluid or pus, causing cough along with phlegm or pus, fever,
1 Pneumonia Pneumonia is an infection which inflames the air sacs either in one or both of the lungs. The air sacs are generally filled with fluid or pus, causing cough along with phlegm or pus, fever,
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Broward Oncology Associates, P.A. PATIENT INFORMATION
 NAME: BIRTHDATE: AGE: LOCAL ADDRESS (Street city state zip): HOME TELEPHONE# CELL # SOCIAL SECURITY #: - - SEX MARITAL STATUS WHAT IS YOUR HT? WHAT IS YOUR WT? EMPLOYER WORK# SPOUSE'S NAME SPOUSE'S EMPLOYER
NAME: BIRTHDATE: AGE: LOCAL ADDRESS (Street city state zip): HOME TELEPHONE# CELL # SOCIAL SECURITY #: - - SEX MARITAL STATUS WHAT IS YOUR HT? WHAT IS YOUR WT? EMPLOYER WORK# SPOUSE'S NAME SPOUSE'S EMPLOYER
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
*Monitor for significant side effects, especially symptoms of neurological or cardiovascular events.
 Assessment Prior to administration: Obtain complete health history including allergies, drug history, and possible drug reactions Assess reason for drug administration such as presence/history of anemia
Assessment Prior to administration: Obtain complete health history including allergies, drug history, and possible drug reactions Assess reason for drug administration such as presence/history of anemia
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Challenges in Management of Cryptococcal Meningitis. Yunus Moosa Department of ID NRMSM Durban
 Challenges in Management of Cryptococcal Meningitis Yunus Moosa Department of ID NRMSM Durban Overview Epidemiology Pathogenesis Clinical presentation Diagnosis Prognostic factors Antifungal Treatment
Challenges in Management of Cryptococcal Meningitis Yunus Moosa Department of ID NRMSM Durban Overview Epidemiology Pathogenesis Clinical presentation Diagnosis Prognostic factors Antifungal Treatment
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology Zeina Alkudmani
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
The exact cause of sarcoidosis is unknown. However, gender, race, and genetics can increase the risk of developing the condition:
 What is sarcoidosis? Sarcoidosis is an inflammatory disease in which granulomas, or clumps of inflammatory cells, form in various organs. This causes organ inflammation. Sarcoidosis may be triggered by
What is sarcoidosis? Sarcoidosis is an inflammatory disease in which granulomas, or clumps of inflammatory cells, form in various organs. This causes organ inflammation. Sarcoidosis may be triggered by
Index No. All five (05) questions should be answered. All questions carry equal marks.
 questions should be answered. All questions carry equal marks.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Medical monitoring: tests available at central hospitals
 medial monitoring: tests available at central hospitals: 1 medical monitoring: tests available at central hospitals Medical monitoring: tests available at central hospitals medial monitoring: tests available
medial monitoring: tests available at central hospitals: 1 medical monitoring: tests available at central hospitals Medical monitoring: tests available at central hospitals medial monitoring: tests available
Panel Discussion: What s New with DRGs and ICD?
 Panel Discussion: What s New with DRGs and ICD? Moderator: Angie Comfort, RHIA, CDIP, CCS, CCS-P Thilo Koepfer, MD Wilbur Lo, MD, CDIP, CCA Objectives Get updated on the current status of ICD- 11 IR-DRG
Panel Discussion: What s New with DRGs and ICD? Moderator: Angie Comfort, RHIA, CDIP, CCS, CCS-P Thilo Koepfer, MD Wilbur Lo, MD, CDIP, CCA Objectives Get updated on the current status of ICD- 11 IR-DRG
LADIS Case of the Month
 November 2018 LADIS Case of the Month Drs Valentin Janvier and Brieuc Cossic Hospital for Animals and Animal Health Diagnostic Center Signalment and presenting complaint 13 year old Thoroughbred gelding
November 2018 LADIS Case of the Month Drs Valentin Janvier and Brieuc Cossic Hospital for Animals and Animal Health Diagnostic Center Signalment and presenting complaint 13 year old Thoroughbred gelding
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome
 Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome Jeong Joo Woo, Dong Hyun Lee, Jin Kyung An Department
Community-Acquired Acinetobacter baumannii Pneumonia: Initial Chest Radiographic Findings and Follow-up CT Findings in Helping Predict Patient Outcome Jeong Joo Woo, Dong Hyun Lee, Jin Kyung An Department
Sleep History Questionnaire
 Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Web Chapter 3. Image Gallery: Lesion detection on low dose chest CT
 Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Drug Resistant Tuberculosis Self-reporting of Drugrelated. During Treatment
 Drug Resistant Tuberculosis Self-reporting of Drugrelated Adverse Events During Treatment Introduction This information has been prepared for people with tuberculosis (TB) that is resistant to the commonly
Drug Resistant Tuberculosis Self-reporting of Drugrelated Adverse Events During Treatment Introduction This information has been prepared for people with tuberculosis (TB) that is resistant to the commonly
CASE-BASED SMALL GROUP DISCUSSION
 MHD II, Session XII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION Session XII MHD II April 21, 2014 STUDENT COPY Helpful Resource: ACP Medicine online available through LUHS Library Infectious
MHD II, Session XII, STUDENT Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION Session XII MHD II April 21, 2014 STUDENT COPY Helpful Resource: ACP Medicine online available through LUHS Library Infectious
Radiological syndroms. Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome
 Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Fungal Infections. Fungal Infections
 Fungal Infection in the Immune Competent Host Steven L. Primack, MD Fungal Infection in the Immune Competent Host Steven L. Primack, MD Department of Radiology Oregon Health & Science University Fungal
Fungal Infection in the Immune Competent Host Steven L. Primack, MD Fungal Infection in the Immune Competent Host Steven L. Primack, MD Department of Radiology Oregon Health & Science University Fungal
2:39 2: Dizziness and nausea Cerebral. 2:57 1: Vomiting Gastro-intestinal
 Supplemental: Table B: Detailed description of adverse events by time, treatment group and procedure T-spinal to incident T-spinal to PACU discharge Group THA/TKA Adverse event description Adverse event
Supplemental: Table B: Detailed description of adverse events by time, treatment group and procedure T-spinal to incident T-spinal to PACU discharge Group THA/TKA Adverse event description Adverse event
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)