Radiological syndroms. Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome
|
|
|
- Adam Chase
- 5 years ago
- Views:
Transcription



1 Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome

2 Alveolar syndrome


3 Pulmonary architecture : Morphological unit is the lobule 15-25mm

4 Acinus & lobule Lobule : morphological unit, smallest anatomical unit, ventilated by the centro lobular bronchiole accompanied by the centro lobular artery dimension: 1 à 2,5 cm composed of 3 to 5 acinus Perilobular interstitial tissue Lobule Acinus : functional unit 14 divisions between the trachea and the terminal bronchiole 1 et 1 bronchiole & centro lobular artery 2. bronchiole & terminal artery 3. respiratory bronchiole 4. Alveolar duct 5. Alveolar bag 6. Alveolus 7. Perilobular vein + lymphatic vessels Acinus
5 Features of alveolar syndrome Blurred, heterogeneous opacity Not well limited (except if there is contact with one fissure, then the consolidation is systematised ) With sometimes aeric bronchogram No retraction in acute phase (but retraction is possible if chronic evolution)



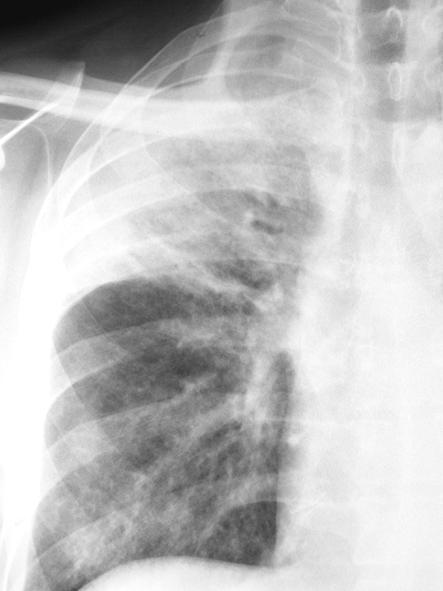
6 Alveolar consolidation Blurred, heterogeneous Not well limited But sharp boundary if contact with a fissure Small fissure Small fissure Right Upper Lobe Pneumonia
7 Systematised opacity with aeric bronchogram
8 Acute* alveolar syndrome - Main etiologies *The more frequent Located Diffuse Infections (bacterial, viral) Tuberculosis Localized pulmonary oedema Lung infarctus and embolism Lung traumatism Post radiotherapy (acute phase ) Mycosis Loeffler syndrome Alveolar sarcoidosis Broncho alveolar cancer > 90 % of cases Infections (bacterial,viral,opportunistic) Tuberculosis Pulmonary oedema > 90 % of cases Traumatism (contusion, fat embolism) Angeitis Pulmonary haemorrhage Loeffler syndrome, eosinophilic lung Hypersensibility pneumonia (allergic alveolitis)
9 Chronic* alveolar syndrome - Main etiologies * Much less common than acute should be referred to a pulmonologist Located Chronic pneumonia Chronic pneumonia with eosinophilia Bronchiolo-alveolar cancer Lymphoma and haemopathy Diffuse Diffuse bronchiolo-alveolar damage Lymphoma and haemopathy Sarcoidosis Pulmonary alveolar proteinosis Lipidic pneumonia desquamative interstitial pneumonia
 Heterogeneous Sharp boundary in contact with a fissure Aeric bronchogramme No retraction in acute phase")
10 Young man with no medical history Fever, chills, sudden onset with right chest pain and purulent sputum Right upper lobe pneumonia (Streptoccocus pneumoniae) Heterogeneous Sharp boundary in contact with a fissure Aeric bronchogramme No retraction in acute phase

")
11 Right lower lobe pneumonia (S. pneumoniae)



12 Bacterial pneumonia are often caused by ear-nose-throat and dental infections and by Flu


13 Right upper lobe pneumonia F. 50 y Day 6 of a Flu t 40, cough and sore spot right chest very limited area of crackles in right scapular region


14 Evolution day 10 Rapid clinical improvement with Amoxicillin Slower radiological improvement


15 Bifocal infection : RUL external segment and left lower lobe


16 Cough, asthenia, loss of weight since 4 weeks AFB (acid fast bacilli) + in sputum Bilateral tuberculosis pneumonia

17 Retractile evolution with treatment



18 RUL Excavated pneumonia Pneumonia + adenopathies RLL pneumonia + adenopathies HIV - H V+ HIV+ TB pneumonia is frequent in countries with high incidence of TB in HIV + patients, but also in HIV - In case of AIDS : mediastinal adenopathies are often associated and TB pneumonia is often located in the lower lobes If the immunosuppression is severe, the cavities are rare
 : AFB + Fistulised node on endoscopic view This image is typical")
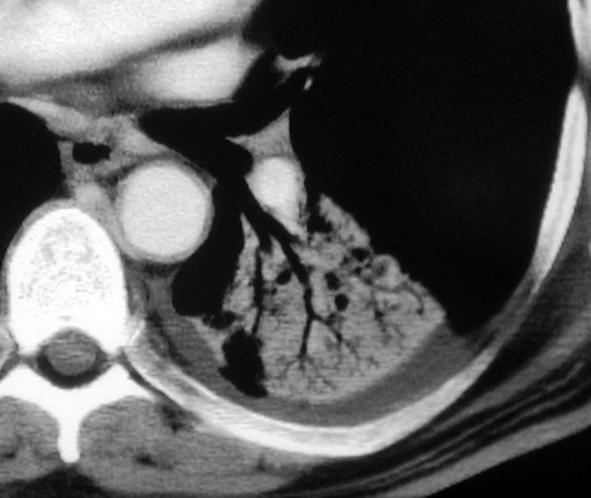
19 Man 30 y old HIV+ Right upper lobe and middle lobe pneumonia Hilar and mediastinum adenopathies AFB sputum negative Bronchial aspiration and BAL (bronchiolo alveaolar lavage) : AFB + Fistulised node on endoscopic view This image is typical of TB/HIV


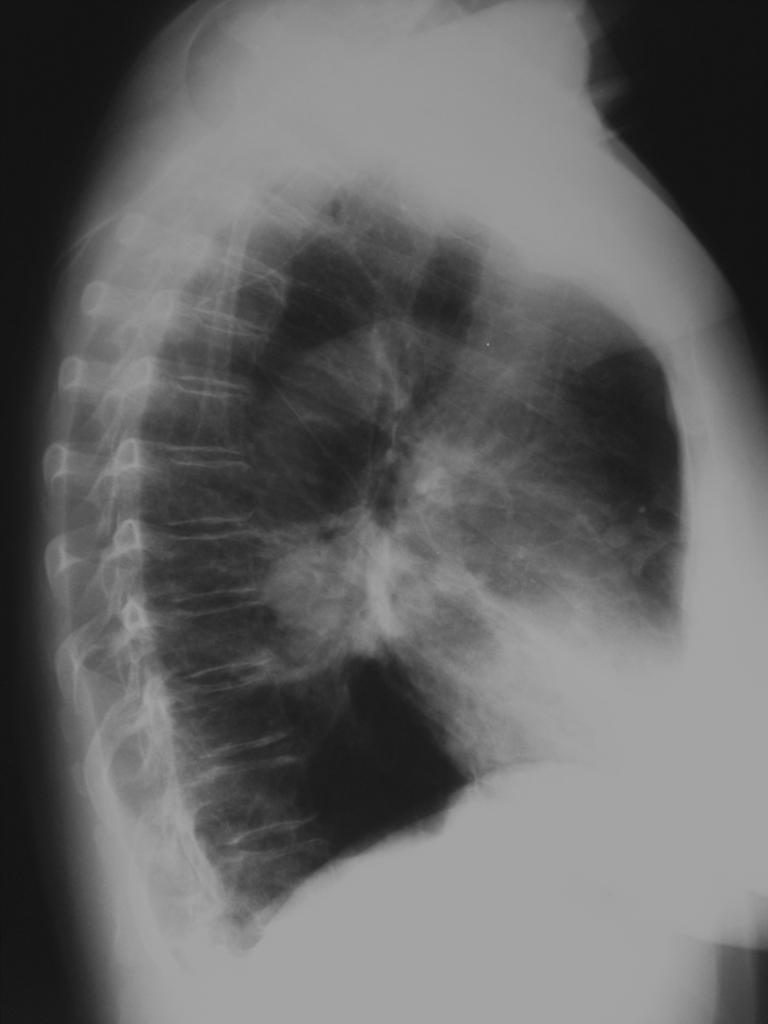
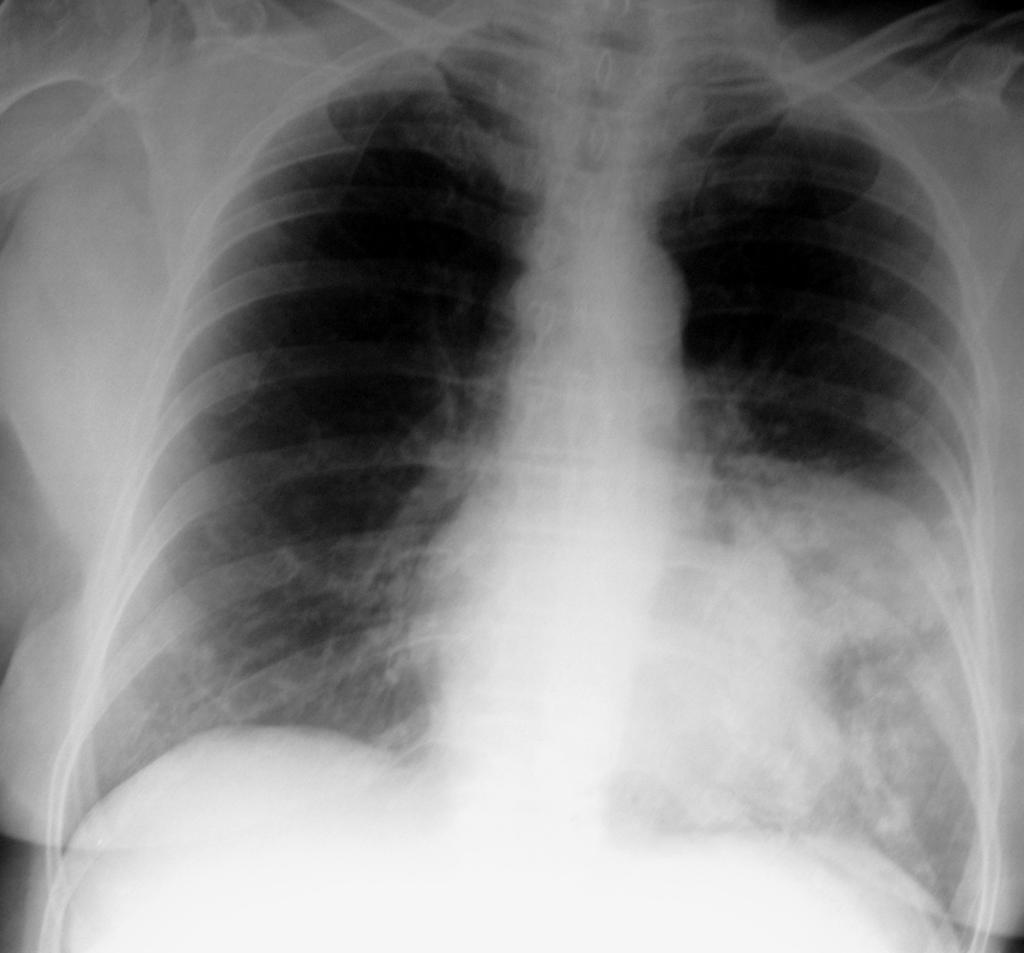
20 African officer in internship in France, t 37 8C, stable condition, no functional or respiratory signs Excavated opacity of the inferior lobe, apical segment, AFB+

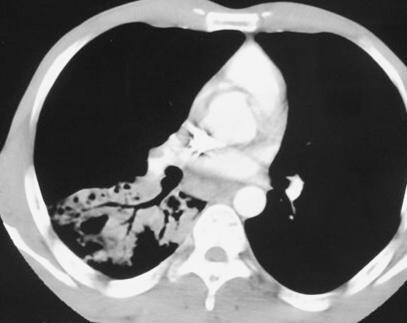
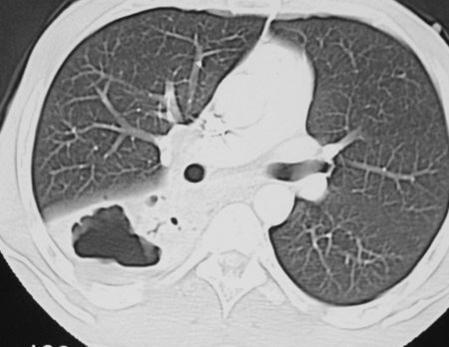

21 Pneumonia with Aeric bronchogramme Micro nodules Cavern


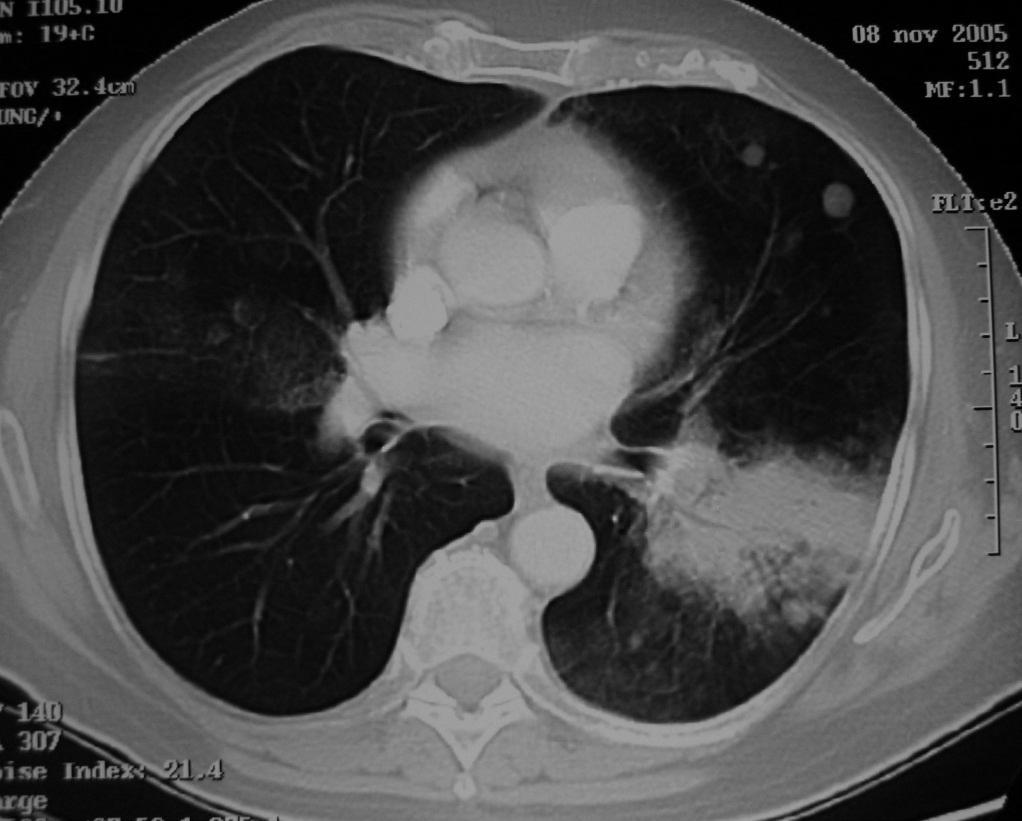
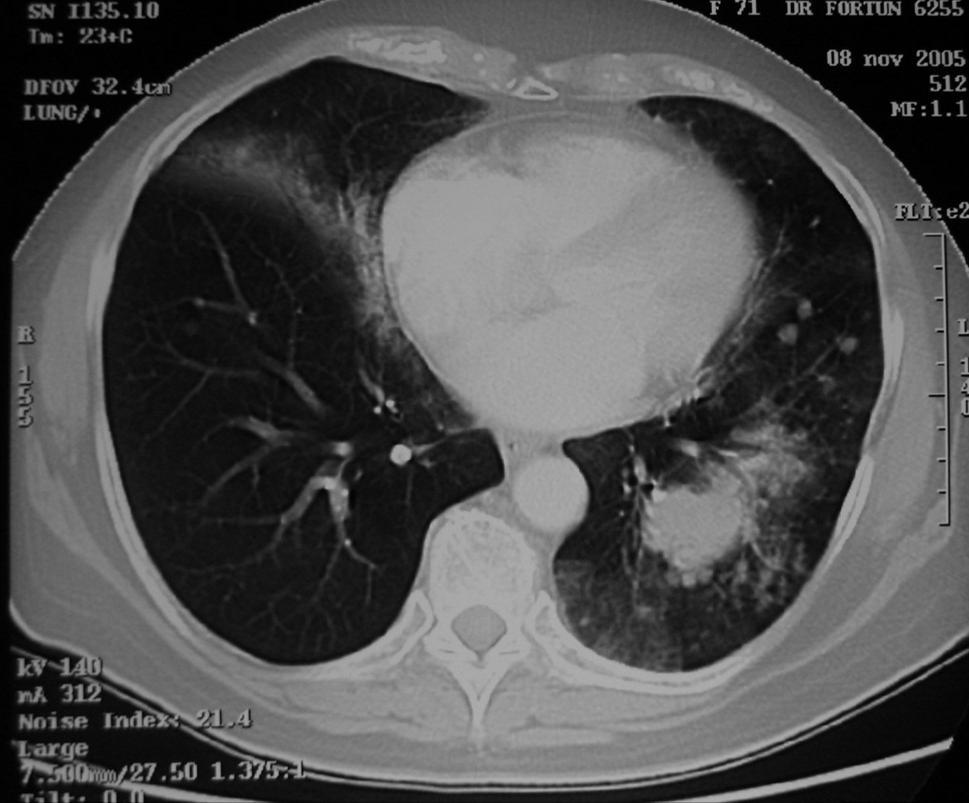
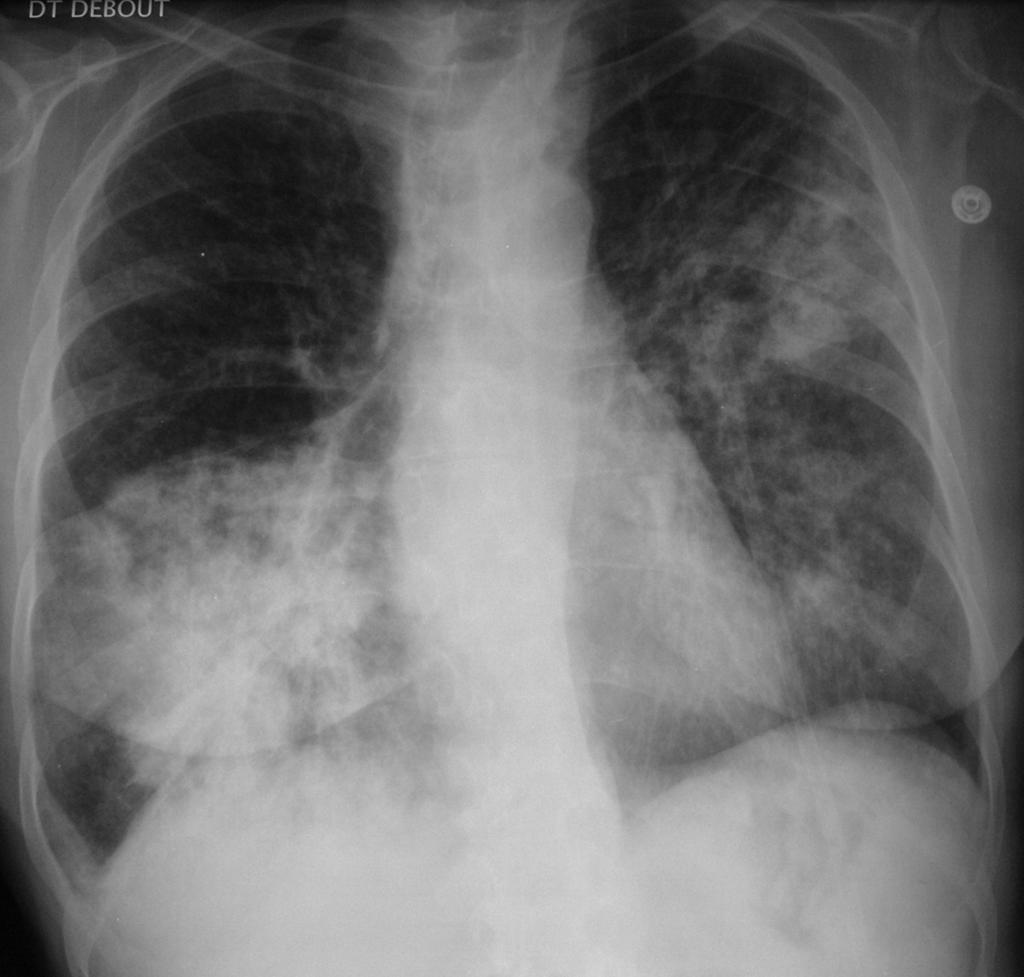
22 Man, 50 years old, fever, cough, dyspnea, headache, abdominal pain. Worsening despite amoxicillin treatment Legionnaires disease Legionella pneumophila

23 Man, 35 years old, dyspnea and severe hypoxemia. Treatment by amoxicilline 3 g per day. (1)


24 Worsening at J4. Modification of treatment and introduction of erythromicin IV 3g/24h. Improvement in few days : Mycoplasma pneumoniae (2)

25 F 30 y HIV + Central African Rep. Bilateral pneumonia unimproved under Amoxycillin


26 Broncho Alveolar Lavage : PJP Aeric bronchogramme Alveolar form of pneumocystosis RARE PJP - Allergy to Bactrim => dapsone Improvement S3
27 If patient does not improve under amoxicilline and has not evident TB (AFB neg in sputum +/- Xpert negative) Consider to switch to macrolides Do not use fluoroquinolones Ask for HIV status If the alveolar syndrome is chronic You must consider an alternative diagnosis Lymphoma, bronchiolo-alveolar carcinoma,. and refer to a pulmonology ward
28 Bronchiolo-alveolar carcinoma
29
30 Bronchiolo-alveolar carcinoma

 There is no anatomic lesion of the alveolar capillary barrier Lesional edema")

 toxic (for example inhalation of toxic gases) complication of")
31 Pulmonary oedema alveolar syndrome 2 physiopathological mechanisms : Hemodynamic oedema : result of left ventricular failure with pulmonary arterial hypertension, of post-capillar type. Medical treatment is usually effective (O2, diuretic, TNT..) There is no anatomic lesion of the alveolar capillary barrier Lesional edema also called Acute Respiratory Distress Syndrom ARDS): The alveolar capillary barrier is more or less irreversibly altered. The prognosis is most often dismal. Death may occur by refractory hypoxemia The etiologies are varied : infectious (viral or bacterial) toxic (for example inhalation of toxic gases) complication of shock whatever the cause

32 Typical pulmonary cardiogenic oedema
33 Hemodynamic pulmonary edema radiological features Alveolar picture Perihilar predominent Bilateral but sometimes assymetric Always with accute dyspnea, cough and clear sputum (although sometimes blood in sputum) Crepitant rales ( crackles ) at the auscultation

34 Acute pulmonary oedema : butterfly wings image

35 Acute pulmonary oedema After furosemide


36 Acute pulmonary oedema Note the asymmetry of the image

37 Asymetric cardiogenic edema
38 Two exemples of ARDS

39 Case Woman, 7 1/2 months pregnant. Fever and dyspnea with rapid deterioration in few days. No improvement despite amoxicilline then erythromycin

40 Worsening at D2 then D3 : lesionnal oedema probably with a viral origin

41 F 27 y., fever, dyspnea and diffuse pain with quick onset. No improvment with antibiotherapy - D1 : admission in intensive care unit. Tamiflu treatment Bronchial and nasopharyngeal sample for H5N1 virus PCR Case 2

42 D2 : no improvment => Non invasive ventilation - PCR + for H5N1 Typical ARDS


43 D4: mecanical ventilation with intra tracheal tube; Note chest tube for left pneumothorax drainage Progressive improvement D 8 to D25 D 4 D 8


44 ARDS lesionnal edema during a H5N1 flu in a young woman Slow improvement after management in ICU D 12 D 25
45 Alveolar syndrome Easy to diagnose : Blurred opacity, heterogeneous, ill-defined, except in contact with a fissure (systematized) non retractile with air bronchogram Must especially evoke : Localized : Bacterial pneumonia, TB pneumonia Diffuse : acute pulmonary edema, infection (bacteria, TB, virus, fungus)
Alveolar condensation syndrome
 Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images
 Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Interstitial syndrome
 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible?
 Chapter 10 Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible? The opacity of the left upper lobe is not cavited and looks like a tissular mass, not
Chapter 10 Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible? The opacity of the left upper lobe is not cavited and looks like a tissular mass, not
Key messages. CXR interpretation in TB/HIV setting. Training course
 Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum.
 Chapter 7 Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum. Auscultation: crepitant bilateral rales. Chest Xray: cardiomegaly
Chapter 7 Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum. Auscultation: crepitant bilateral rales. Chest Xray: cardiomegaly
Case N 1. Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds. Courtesy Dr Van den Homberg-Tanzania
 Case N 1 Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds Courtesy Dr Van den Homberg-Tanzania Case N 1 Enlargment of cardiac silhouette. Notice the symetry
Case N 1 Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds Courtesy Dr Van den Homberg-Tanzania Case N 1 Enlargment of cardiac silhouette. Notice the symetry
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Case N 1. Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available. Courtesy Dr Van Den Homberg
 Case N 1 Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available Courtesy Dr Van Den Homberg Case N 1 CXR: Right abundant pleural effusion. Notice the typical concave aspect of the superior
Case N 1 Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available Courtesy Dr Van Den Homberg Case N 1 CXR: Right abundant pleural effusion. Notice the typical concave aspect of the superior
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
CARDIO-VASCULAR SYNDROME
 CARDIO-VASCULAR SYNDROME Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) OFCP Right pulmonary artery Left pulmonary artery
CARDIO-VASCULAR SYNDROME Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) OFCP Right pulmonary artery Left pulmonary artery
I particularly want to thank: -Pr Pierre L Her who has been my nearest partner in this adventure which began in Cambodia many years ago.
 Introduction and advices for users: CXR interpretation in TB/HIV high burden settings Clinical and radiological cases for training to positive and differential diagnosis Here are collected 144 clinical
Introduction and advices for users: CXR interpretation in TB/HIV high burden settings Clinical and radiological cases for training to positive and differential diagnosis Here are collected 144 clinical
Cardio-vascular syndrome. Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
 Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Pleural syndrome Tuberculous pleurisy
 Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Pleural syndrome. Tubercular pleurisy
 Pleural syndrome. Tubercular pleurisy Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Pleurisy: Findings of fluid between visceral
Pleural syndrome. Tubercular pleurisy Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Pleurisy: Findings of fluid between visceral
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Dr Marie Bruyneel and Deborah Konopnicki. BVIKM/SBMIC November 8th, 2012
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
 Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Exam 2 Respiratory Disorders
 Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
Respiratory diseases in Ostrołęka County
 Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Radiation Pneumonitis Joseph Junewick, MD FACR
 Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Avian Influenza Clinical Picture, Risk profile & Treatment
 Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Describe regional differences in pulmonary blood flow in an upright person. Describe the major functions of the bronchial circulation
 OBJECTIVES Describe regional differences in pulmonary blood flow in an upright person Define zones I, II, and III in the lung, with respect to pulmonary vascular pressure and alveolar pressure Describe
OBJECTIVES Describe regional differences in pulmonary blood flow in an upright person Define zones I, II, and III in the lung, with respect to pulmonary vascular pressure and alveolar pressure Describe
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Case Report Chronic Lipoid Pneumonia in a 9-Year-Old Child Revealed by Recurrent Chest Pain
 Case Reports in Pediatrics Volume 2015, Article ID 402926, 4 pages http://dx.doi.org/10.1155/2015/402926 Case Report Chronic Lipoid Pneumonia in a 9-Year-Old Child Revealed by Recurrent Chest Pain A. Hochart,
Case Reports in Pediatrics Volume 2015, Article ID 402926, 4 pages http://dx.doi.org/10.1155/2015/402926 Case Report Chronic Lipoid Pneumonia in a 9-Year-Old Child Revealed by Recurrent Chest Pain A. Hochart,
Pulmonary Alveolar Proteinosis
 January 2001 Pulmonary Alveolar Proteinosis Brady Case, Harvard Medical School 1 Our Patient Nelson is a 40 year-old male who presents with a 6 month history of: progressive dyspnea on exertion dry cough
January 2001 Pulmonary Alveolar Proteinosis Brady Case, Harvard Medical School 1 Our Patient Nelson is a 40 year-old male who presents with a 6 month history of: progressive dyspnea on exertion dry cough
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Respiratory System. Respiratory System Overview. Component 3/Unit 11. Health IT Workforce Curriculum Version 2.0/Spring 2011
 Component 3-Terminology in Healthcare and Public Health Settings Unit 11-Respiratory System This material was developed by The University of Alabama at Birmingham, funded by the Department of Health and
Component 3-Terminology in Healthcare and Public Health Settings Unit 11-Respiratory System This material was developed by The University of Alabama at Birmingham, funded by the Department of Health and
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology Zeina Alkudmani
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases
 Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
THE GOOFY ANATOMIST QUIZZES
 THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
Acute pneumonia Simple complement
 Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
Acute pneumonia Simple complement 1. Clinical variants of acute pneumonia in children are, except: A. Bronchopneumonia B. Lobar confluent pneumonia C. Viral pneumonia D. Interstitial pneumonia E. Chronic
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
About the Respiratory System. Respiratory System. Human Respiratory System. Cellular Respiration. Nostrils. Label diagram
 Respiratory System Human Respiratory System A system to deliver oxygen (O2) to body cells & get rid of carbon dioxide (CO2) as a waste through cellular respiration. Two systems involved: Respiratory &
Respiratory System Human Respiratory System A system to deliver oxygen (O2) to body cells & get rid of carbon dioxide (CO2) as a waste through cellular respiration. Two systems involved: Respiratory &
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Disclosure. Clinical Chest Radiography Interpretation Part II
 Clinical Chest Radiography Interpretation Part II Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma
Clinical Chest Radiography Interpretation Part II Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma
100 Chest X Rays for Study Group. by Dr. Suneet Khurana
 100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH. Leonard E. Swischuk, M.D. University of Texas Medical Branch
 ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
ACUTE PULMNARY INFECTIONS: UNDERSTANDING THE CHEST RADIOGRAPH Leonard E. Swischuk, M.D. University of Texas Medical Branch AUTHOR HAS NOTHING TO DECLARE LEARNING OBJETIVES Understand the pathophysiology
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Unilateral pulmonary oedema, a forgotten presentation.
 Unilateral pulmonary oedema, a forgotten presentation. Poster No.: C-2146 Congress: ECR 2018 Type: Educational Exhibit Authors: C. A. Arboleda Vallejo, M. I. carvajal, M. Perez ; Medellin, 1 2 1 1 2 Antioquia/CO,
Unilateral pulmonary oedema, a forgotten presentation. Poster No.: C-2146 Congress: ECR 2018 Type: Educational Exhibit Authors: C. A. Arboleda Vallejo, M. I. carvajal, M. Perez ; Medellin, 1 2 1 1 2 Antioquia/CO,
Accurate Diagnosis Of Postoperative Pneumonia Requires Objective Data
 Accurate Diagnosis Of Postoperative Pneumonia Requires Objective Data David Ebler, MD David Skarupa, MD Andrew J. Kerwin, MD, FACS Jhun de Villa, MD Michael S. Nussbaum, MD, FACS J.J. Tepas III, MD, FACS
Accurate Diagnosis Of Postoperative Pneumonia Requires Objective Data David Ebler, MD David Skarupa, MD Andrew J. Kerwin, MD, FACS Jhun de Villa, MD Michael S. Nussbaum, MD, FACS J.J. Tepas III, MD, FACS
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Respiratory tract infections. Krzysztof Buczkowski
 Respiratory tract infections Krzysztof Buczkowski Etiology Viruses Rhinoviruses Adenoviruses Coronaviruses Influenza and Parainfluenza Viruses Respiratory Syncitial Viruses Enteroviruses Etiology Bacteria
Respiratory tract infections Krzysztof Buczkowski Etiology Viruses Rhinoviruses Adenoviruses Coronaviruses Influenza and Parainfluenza Viruses Respiratory Syncitial Viruses Enteroviruses Etiology Bacteria
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Particle Size and Dust Inhalation
 Pneumoconiosis A disease of the lungs characterized by fibrosis and caused by the chronic inhalation of mineral dusts, especially silica and asbestos. Helen Lang Dept. Geology & Geography West Virginia
Pneumoconiosis A disease of the lungs characterized by fibrosis and caused by the chronic inhalation of mineral dusts, especially silica and asbestos. Helen Lang Dept. Geology & Geography West Virginia