I have no relevant conflicts of interest to disclose
|
|
|
- Cody Green
- 5 years ago
- Views:
Transcription



1
2 I have no relevant conflicts of interest to disclose
3 Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures HRCT Approach Pattern of Disease Location in the secondary lobule HRCT Approach Upper versus lower lung zone predominance Central versus peripheral predominance Idiopathic Interstitial Pneumonias NSIP, COP, RB-ILD, DIP, LIP, and AIP IPF Teaching Points
4 Common Clinical Problem Diffuse/widespread infiltrates on a chest radiograph Diffuse does not imply uniformity of involvement Diffuse infiltrates are non-specific radiographic findings that do not diagnose causation
5 Causes of Widespread/Diffuse Infiltrates on Chest Radiograph Edema (water) Pulmonary hemorrhage (blood) Infection (pus) Inflammation Fibrosis Neoplasm
6 Important Associations with DPLD Drug induced injury Environmental induced injury Occupational induced injury Relationship to other systemic illness (collagen vascular disease and/or autoimmune disease) Genetic relationships
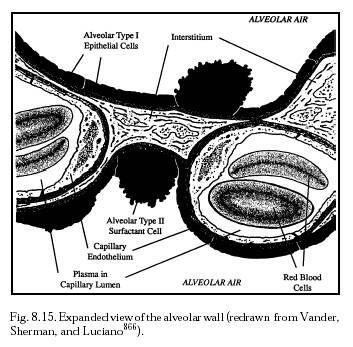
7 Descriptive term for diffuse lung diseases that affect the interstitium or alveolar space There are shared physiologic, radiographic, and pathologic features
8
9 Understanding of lung anatomy is essential for approach to DPLD especially with the widespread use of HRCT The secondary lobule is the basic anatomic unit of pulmonary structure and function Interpretation of DPLD is based upon the type of involvement of the secondary lobule

10 Smallest lung unit surrounded by connective tissue septa Measures 1-2 cm and is made up of 5-15 pulmonary acini, that contain the alveoli for gas exchange Supplied by the terminal bronchiole in the center, that is paralleled by the centrilobular artery Pulmonary veins and lymphatics run in the periphery within the interlobular septa

11 Centrilobular Area Central part of the secondary lobule Site of diseases that enter the lungs through the airways Perilymphatic Area Peripheral part of the secondary lobule Site of diseases that are located in the lymphatics of the interlobular septa
12 DPLD of Known Cause (collagen vascular disease, drugs, infection, occupation) Idiopathic Interstitial Pneumonias Idiopathic Pulmonary Fibrosis Desquamative Interstitial Pneumonia, Respiratory Bronchiolitis Interstitial Lung Disease, Acute Interstitial Pneumonia, Cryptogenic Organizing Pneumonia, Nonspecific Interstitial Pneumonia, Lymphocytic Interstitial Pneumonia Granulomatous DPLP (Sarcoidosis) Other forms of DPLD (Lymphangioleiomyomatosis and Pulmonary Langerhans Cell Histiocytosis)
13 Pattern of Disease Reticular Nodular High-attenuation (groundglass, consolidation) Low-attenuation (emphysema, cystic) Location in the secondary lobule Centrilobular, perlymphatic, or random Upper versus lower lung zone predominance Central versus peripheral predominance Additional findings Pleural fluid Lymphadenopathy Cardiomegaly Esophageal dilation Traction bronchiectasis
14 Morphologic findings have to be combined with history of the patient and clinical findings Clinical presentation Demographics (age/gender/race) Pulmonary and extrapulmonary manifestations Temporal course Environmental exposure and occupational history Drug history Smoking history Past history of illnesses Family history
15 Acute Onset (1-14 days) Limited diagnoses considered in the differential Acute interstitial pneumonia, acute hypersensitivity pneumonitis, acute eosinophilic pneumonia, acute decompensated heart failure, acute infectious process Sub-acute to Chronic (Months to Years) More common presentation Less useful to narrow the differential diagnosis
16 Organic Antigens (bacteria, fungi, mycobacteria) Moldy hay, silage, grain Aerosolized hot tub water Stagnant humidifier water Organic Antigens (animal protein) Bird feathers and droppings Laboratory animal dander Inorganic Antigens Di-isocyanates (used in production of polyurethanes) Aerosolized machine lubricants
17 Inorganic Dusts Asbestos Silica Iron (siderosis) Mixed (coal worker) Complex (9/11 lung disease) Radiation Exposure
18 Complete past medication review Medications taken for prolonged periods Some medications have a long latency period (amiodarone) Over-the-Counter Medications Oily nose drops Herbal medications Illegal/Recreational Drugs Temporal relationship with current manifestations
19 Reticular Pattern Too many lines Coalescence of lines creates nodular appearance at intersection The result of thickening of the interlobular septa or as a result of fibrosis (honeycombing) Septal Thickening Thickening of the lung interstitium by fluid, fibrous tissue, or infiltration by cells Smooth: Usually seen in interstitial pulmonary edema but also seen in alveolar proteinosis and lymphangitic spread of carcinoma Nodular or Irregular: Lymphangitic spread of carcinoma or lymphoma, sarcoidosis and silicosis
20 Smooth Septal Thickening Alveolar Proteinosis (accumulation of PAS positive phospholipoprotein from surfactant) Crazy Paving (PJP, ARDS, NSIP, BAC, COP, sarcoidosis, and alveolar hemorrhage) Irregular Septal Thickening Focal irregular septal thickening in the right upper lobe due to lymphangitic carcinomatosis In sarcoidosis the findings would be more diffuse

21 Random Randomly distributed relative to the structures of the lung and secondary lobule Centrilobular Nodules spare the pleural surfaces Most peripheral nodules are centered 5-10 mm from fissues or the pleural surface Perilymphatic Seen in relation to pleural surfaces, interlobular septa, and peribronchovascular interstitium Almost always visible in subpleural location
22

 Smoking related (upper lung")
23 Hematogenous metastases Miliary tuberculosis Miliary fungal infections Extensive sarcoidosis may mimic the pattern Pulmonary Langerhans Cell Histiocytosis (early nodular stage) Characterized by multiple cysts of varying size Early disease with nodules (later cavitate to form cysts) Smoking related (upper lung predominance)

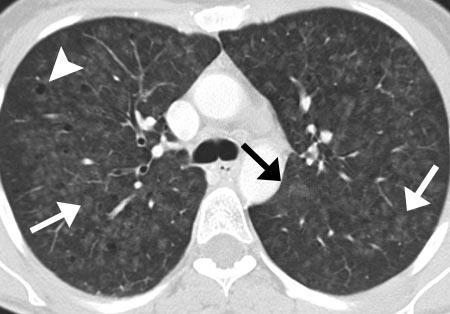
24 Without tree-inbud opacities Ill-defined nodular ground-glass opacities removed from pleural and fissural surfaces Subacute Hypersensitivity Pneumonitis RB-ILD LIP
 centrilobular bronchioles (bronchiolitis) Clustered: MTB/MAI, Fungal, Bacterial Infection Diffuse: Panbronchiolitis, viral infections, cystic")
25 Ground-glass nodules with prominent tree-in-bud opacities Appearance of an irregular and often nodular branching structure, most easily identified in the lung periphery Represents dilated and impacted (mucous or pus filled) centrilobular bronchioles (bronchiolitis) Clustered: MTB/MAI, Fungal, Bacterial Infection Diffuse: Panbronchiolitis, viral infections, cystic fibrosis



26 Nodules visible along the pleural surface, the central bronchovascular interstitium, and along interlobular septa Sarcoidosis Silicosis Coal-Workers Pneumoconiosis

27 Ground-Glass Opacity Hazy increase in lung opacity without obscuration of underlying vessels Increase in lung density is due filling of alveolar spaces with pus, edema, hemorrhage, inflammation, or tumor cells Also secondary to thickening of the interstitium or alveolar walls below the spatial resolution of HRCT (as seen in fibrosis 60-80% of patient s with GGO on HRCT have active and potentially treatable lung disease

28 Acute Pulmonary Edema Heart failure ARDS Pulmonary Hemorrhage Pneumonia Acute Eosinophilic Pneumonia Chronic Hypersensitivity Pneumonitis Organizing Pneumonia Chronic Eosinophilic Pnuemonia Fibrosis UIP NSIP Bronchoalveolar Cell Carcinoma

29 Consolidation Hazy increase in lung opacity with obscuration of underlying vessels Pneumonia PJP, viral, bacterial, Mycoplasma Eosinophilic pneumonia Organizing pneumonia Edema: Heart failure, ARDS, AIP Fibrosis: UIP, NSIP, radiation Tumor: BAC and lymphoma Idiopathic: Sarcoidosis and Alveolar Proteinosis

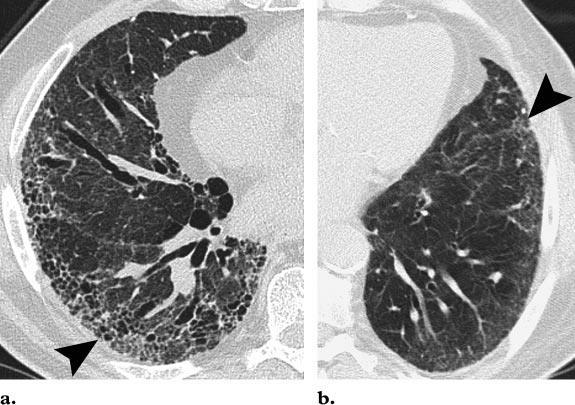
30 Emphysema Areas of low attenuation without visible walls as a result of parenchymal destruction Honeycombing Presence of small cystic spaces with irregularly thickened walls composed of fibrous tissue Predominate in peripheral and subpleural lung regions Several contiguous layers IPF, connective-tissue disease, asbestosis, endstage HP, end-stage sarcoidosis
 Cystic fibrosis Cilia abnormalities (primary ciliary dyskinesia) Autoimmune disease (RA, Sjogren s) ABPA Inflammatory bowel disease Immune deficiency (immunoglobulin")
31 Bronchiectasis Localized bronchial dilation Bronchial wall thickening, lack of normal tapering with visibility of airways in the peripheral lung, mucous retention in the bronchial lumen Prior infection (focal bronchiectasis) Cystic fibrosis Cilia abnormalities (primary ciliary dyskinesia) Autoimmune disease (RA, Sjogren s) ABPA Inflammatory bowel disease Immune deficiency (immunoglobulin deficiency and HIV) Alpha-1 antitrypsin

32 Cysts and Cavities Cysts are radiolucent areas with a wall thickness < 4 mm Lymphangioleiomyomatosis Pulmonary Langerhans Cell Histiocytosis Lymphocytic Interstitial Pneumonia Cavities are radiolucent areas with a wall thickness > 4mm Staph aureus, fungal infection, TB, septic emboli, squamous cell cancer, Wegner s
33 Upper Lung Zone Inhaled particles (silica, coal) Smoking related diseases Centrilobular emphysema RB-ILD Pulmonary Langerhans Cell Histiocytosis Hypersensitivity Pneumonitis Sarcoidosis Lower Lung Zone UIP (IPF, collagen vascular disease) Asbestosis Aspiration Pulmonary edema Panlobular emphysema Affects the whole secondary lobule Alpha-1 antitrypsin deficiency
34 Central Zone Sarcoidosis Cardiogenic pulmonary edema Pulmonary alveolar proteinosis Peripheral Zone UIP (IPF, collagen vascular disease) Chronic eosinophilic pneumonia Cryptogenic organizing pneumonia Asbestosis Hematogenous metastases
35
36 One of the most common histologic findings in patients with IIP s Need to distinguish from UIP given the improved survival and responsiveness to corticosteroids Typical age is years Gradually worsening dyspnea over several months, cough, fatigue, weight loss No gender predilection Need to rule out secondary causes Collagen vascular disease, hypersensitivity pneumonitis, druginduced pneumonitis, HIV infection
37 Histologic Features Temporally and spatially homogenous lung involvement Cellular NSIP: thickening of alveolar septa is caused by inflammatory cells Fibrosing NSIP: interstitial fibrosis is seen in addition to mild inflammation Imaging Features (HRCT) Subpleural and symmetric distribution of lung abnormalities Patchy ground-glass opacities combined with irregular linear or reticular opacities and scattered micronodules
38
39 Typical age is 55 years Women and men are equally affected Mild dyspnea, cough, and fever developing over a few weeks Need to exclude known causes of organizing pneumonia Infection, drug-induced, collagen vascular disease PFT s show restriction and diffusion impairment Minority with airways obstruction Typical complete recovery with oral corticosteroids High rate of relapse within 1-3 months of stopping treatment Prolonged treatment for at least 6 months initially to avoid relapse
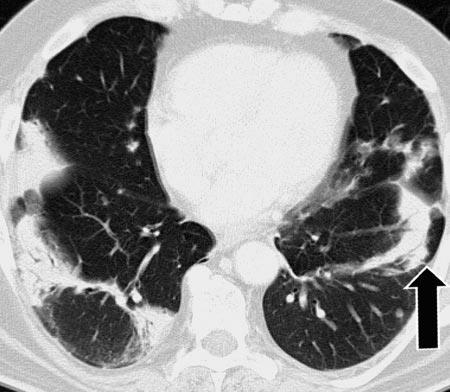
40 Histologic Features Patchy process characterized primarily by organizing pneumonia involving alveolar ducts and alveoli with our without bronchiolar intraluminal polyps Connective tissue of all the same age Changes centered on small airways Imaging Features (HRCT) Findings are more extensive than expected from review of plain radiograph Peripheral or peribronchial distribution with lower lung zone predominance Opacities vary from ground-glass to consolidation Opacities migrate (changing size and location)
41
42 Respiratory bronchiolitis Histopathologic lesion found in cigarette smokers Pigmented intraluminal macrophages in the 1 st and 2 nd order respiratory bronchioles Rarely symptomatic but can rarely present as an ILD Current smokers typically age years 30 pack year history Men affected twice as often as women Present with mild dyspnea and cough Symptoms are not disabling Mild to moderate reduction in DLCO Treatment is smoking cessation
 Plain chest radiograph insensitive for detection Centrilobular nodules in combination with ground-glass")
.")
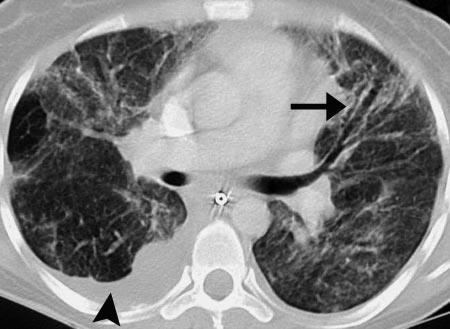
43 Histologic Features Intraluminal accumulation of pigmented macrophages centered around the respiratory bronchioles Mild peribronchiolar inflammation Imaging Features (HRCT) Plain chest radiograph insensitive for detection Centrilobular nodules in combination with ground-glass opacities and bronchial wall thickening Ground-glass opacities correlate with macrophage accumulation in alveolar ducts and alveolar spaces Pigmented alveolar macrophages in a terminal bronchiole and the adjacent alveoli (arrows). Moderate peribronchiolar inflammation and fibrosis are present (arrowhead).
44
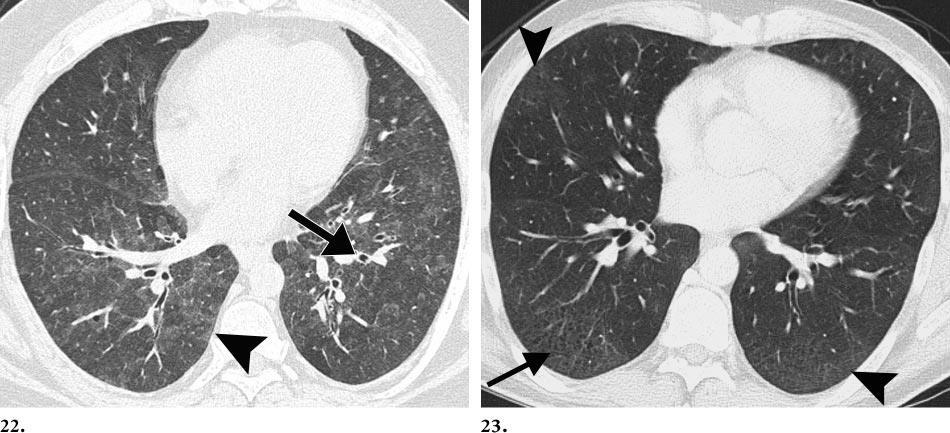
45 Considered by many to represent the end of a spectrum of RB-ILD Typical age is years Current or former smokers Rarely occurs in nonsmokers who have had environmental inhalation exposures Men affected twice as often as women Insidious onset of dyspnea and dry cough over weeks to months Progression to respiratory failure and death can occur Treatment is smoking cessation Oral corticosteroids can be trialed
 Diffuse ground-glass opacities Correlates histologically with the spatially homogenous intraalveolar accumulation of macrophages and thickening of alveolar septa Peripheral and lower")
46 Histologic Features Accumulation of pigmented macrophages and a few desquamated alveolar epithelial cells in the alveoli Lung involvement is more diffuse and uniform in DIP opposed to RB-ILD Imaging Features (HRCT) Diffuse ground-glass opacities Correlates histologically with the spatially homogenous intraalveolar accumulation of macrophages and thickening of alveolar septa Peripheral and lower lung zone predominance Irregular linear opacities and a reticular pattern are frequent
47
48 Typical age is fifth decade of life Present with slowly progressive dyspnea and cough (over a period of 3 or more years) Fever, night sweats, weight loss, chest pain, arthralgia Very rare Need to evaluate for secondary causes Sjogrens, RA, primary biliary cirrhosis, autoimmune hemolytic anemia, chronic active hepatitis, hypogammaglobulinemia, severe combined immunodeficiency, AIDS More common in women Corticosteroids are used for treatment Response is unpredictable
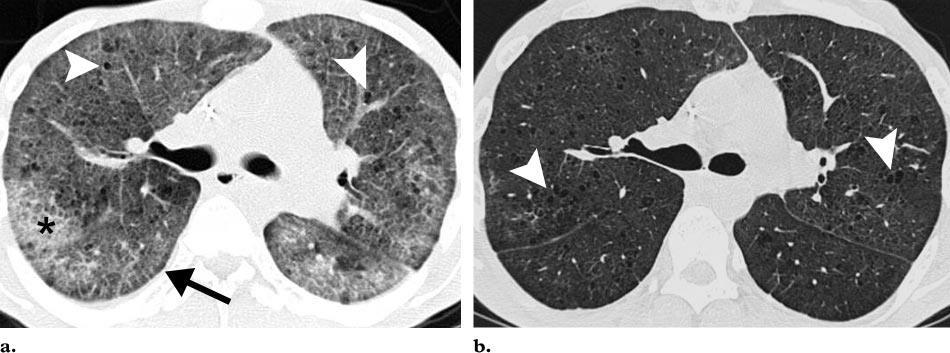
 Diffuse bilateral abnormalities with a lower lung predominance Ground-glass attenuation (diffuse interstitial inflammation) Thin-walled perivascular cysts (usually within the lung parenchyma")
49 Histologic Features Diffuse infiltration of the interstitium by lymphocytes, plasma cells, and histiocytes Reactive lymphoid follicles distributed along the peribronchiolar regions Imaging Features (HRCT) Diffuse bilateral abnormalities with a lower lung predominance Ground-glass attenuation (diffuse interstitial inflammation) Thin-walled perivascular cysts (usually within the lung parenchyma throughout the mid lung zones) Widening of alveolar septa by lymphoid infiltrates (arrow) (inset), which consist of mature lymphocytes, plasma cells, and histiocytes.
50
51 Mean age of 50 years Men and women are equally affected Prior illness suggestive of a viral upper respiratory infection Myalgias, arthralgias, fever, chills, malaise Median time from 1 st symptom to time of presentation is less than 3 weeks Hypoxemia develops early and progresses rapidly to respiratory failure Need to distinguish from: Diffuse alveolar damage (DAD) superimposed on UIP, DAD with collagen vascular disease, ARDS (DAD of known cause), infection (PJP, CMV), druginduced pneumonitis, acute hypersensitivity pneumonitis, and acute eosinophilic pneumonia No proven treatment Corticosteroids may be effective in early phase of disease Poor prognosis with nearly 50% mortality rate
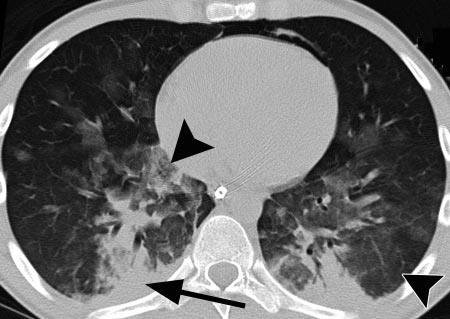
52 Histologic Features (Diffuse Alveolar Damage) Early exudative phase Interstitial and intraalveolar edema, formation of hyaline membranes, and diffuse alveolar infiltration by inflammatory cells Organizing phase (end of first week of lung injury) Formation of granulation tissue resulting in alveolar wall thickening Fibrotic changes in AIPD are uniform and characterized by numerous fibroblasts but relatively little collagen deposition Imaging Features (HRCT) Early exudative phase Ground-glass opacities (alveolar septal edema and hyaline membranes) Areas of consolidation (less extensive and limited to the dependent area of the lung) Intraalveolar edema and hemorrhage Organizing phase Consolidations present (intraalveolar fibrosis) Late phase Architecularal distortion, traction bronchiectasis, and honecombing
53
54
55 The most common entity of the IIPS 50 years old or older Progressively worsening dyspnea and nonproductive cough No obvious gender predilection Incidence in men age 55 or greater is greater than women of the same age Estimated mean survival of 2-5 years from the time of diagnosis Two new treatment options recently FDA approved Pirfenidone (Esbriet) Nintedanib (Ofev)

56 Histologic Features Hallmark of usual interstitial pneumonia (UIP) is presence of scattered fibroblastic foci Lung involvement is heterogenous and areas of normal lung alternate with interstitial inflammation and honeycombing Discordant histologic patterns may be present UIP pattern in one biopsy specimen is associated with a worse prognosis
57 UIP Pattern Requires All Four Features Subpleural, basal predominance Reticular abnormality Honeycombing with or without traction bronchiectasis Absence of features listed as inconsistent with UIP pattern Inconsistent with UIP Pattern Upper or mid-lung predominance Peribronchovascular predominance Extensive ground-glass abnormality Profuse micronodules Discrete cysts Diffuse mosaic attenuation/airtrapping Consolidation in bronchopulmonary segments
58
59
60 May provide a specific diagnosis in a limited number of cases of DPLD Lymphocentric Disorders Sarcoidosis, carcinoma, infection Specific Histopathology Eosinophilic pneumonia, alveolar proteinosis Insufficient to diagnose histopathologic patterns that require establishment of an architectural patent (most IIPs)
61 1. Granulomatous diseases 2. Malignant tumors/lymphangitic 3. DAD (any cause) 4. Certain infections 5. Alveolar proteinosis 6. Eosinophilic pneumonia 7. Vasculitis 8. Amyloidosis 9. EG/HX/PLCH 10. LAM 11. RB/RBILD/DIP 12. UIP/NSIP/LIP COP 13. Small airways disease 14. PHT and PVOD Transbronchial Biopsy Often Sometimes Never Surgical Biopsy
62 IIPs are rare but are considered prototypes of the much more common secondary interstitial pneumonias that can be encountered in frequent disorders (sarcoidosis, vasculitis, and collagen vascular disease) The classification of IIPs is based on histologic criteria, but those histologic patterns are closely associated with imaging patterns that correlate well with histologic findings Establishing the final diagnosis of IIPs requires close communication and interaction between clinicians, radiologists, and pathologists Diagnosis of IIPs is a dynamic process, and preliminary diagnostic assumptions may need to be revised during the diagnostic work-up. High-resolution CT is indicated in virtually all patients suspected to have IIPs
63 It is key to identify patients with UIP and differentiate them from patients with other IIPs, because UIP has a substantially poorer prognosis than other IIPs In all patients suspected to have IIPs who do not show the typical clinical and radiologic features of UIP, surgical lung biopsy should be performed Biopsy specimens should always be obtained from more than one lobe, and high-resolution CT should serve as a guiding tool for determining the appropriate anatomic location of the biopsy site
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Daria Manos RSNA 2016 RC 401. https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html
 Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Non-neoplastic Lung Disease II
 Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Bronkhorst colloquium Interstitiële longziekten. Katrien Grünberg, klinisch patholoog
 Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Radiologic Approach to Smoking Related Interstitial Lung Disease
 Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
How to identify interstitial pneumonias.
 How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
NONE OVERVIEW FINANCIAL DISCLOSURES UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF (UIP) FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP
 FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP") UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
The crazy-paving pattern: A radiological-pathological correlated and illustrated overview
 The crazy-paving pattern: A radiological-pathological correlated and illustrated overview Poster No.: C-0827 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: W. F. M. De Wever, J. Coolen,
The crazy-paving pattern: A radiological-pathological correlated and illustrated overview Poster No.: C-0827 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: W. F. M. De Wever, J. Coolen,
Mimics in chest disease: interstitial opacities
 Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
I don t need you. Disclosure Statement. Pathology Approach to ILD 11/5/2016. Kirk D. Jones, MD UCSF Dept of Pathology
 Pathology Approach to ILD Disclosure Statement Relevant financial relationships with a commercial interest: Boeringer Ingleheim, speaker Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu I don
Pathology Approach to ILD Disclosure Statement Relevant financial relationships with a commercial interest: Boeringer Ingleheim, speaker Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu I don
Epidemiology and classification of smoking related interstitial lung diseases
 Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
Case Presentations in ILD. Harold R. Collard, MD Department of Medicine University of California San Francisco
 Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases
 Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
CLEARING THE AIR ON DIFFUSE PARENCHYMAL (INTERSTITIAL) LUNG DISEASE (ILD)
 LUNG DISEASE (ILD)") CLEARING THE AIR ON DIFFUSE PARENCHYMAL (INTERSTITIAL) LUNG DISEASE (ILD) David Northrop MBA, RRT Assistant Director of Respiratory Therapy Services The University of Kansas Health System Clinical Assistant
CLEARING THE AIR ON DIFFUSE PARENCHYMAL (INTERSTITIAL) LUNG DISEASE (ILD) David Northrop MBA, RRT Assistant Director of Respiratory Therapy Services The University of Kansas Health System Clinical Assistant
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
A Review of Interstitial Lung Diseases
 Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Progress in Idiopathic Pulmonary Fibrosis
 Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Histopathologic Approach to Interstitial Lung Disease
 Histopathologic Approach to Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu Disclosures I have nothing to disclose 1 Why? Much of interstitial lung disease biopsies
Histopathologic Approach to Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu Disclosures I have nothing to disclose 1 Why? Much of interstitial lung disease biopsies
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Pathologic Assessment of Interstitial Lung Disease
 Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Spectrum of Cystic Lung Disease and its Mimics. Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology
 Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Diffuse Interstitial Lung Diseases: Is There Really Anything New?
 : Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
: Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
Lung CT: Part 2, The Interstitial Pneumonias Clinical, Histologic, and CT Manifestations
 Integrative Imaging Review Ferguson and Berkowitz CT of Interstitial Pneumonia Integrative Imaging Review CME SAM Lung CT FOCUS ON: Emma C. Ferguson 1 Eugene A. Berkowitz 2 Ferguson EC, Berkowitz EA Keywords:
Integrative Imaging Review Ferguson and Berkowitz CT of Interstitial Pneumonia Integrative Imaging Review CME SAM Lung CT FOCUS ON: Emma C. Ferguson 1 Eugene A. Berkowitz 2 Ferguson EC, Berkowitz EA Keywords:
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines
 Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Disclosures. Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting. Relevant financial relationships: None. Off-label usage: None
 Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Idiopathic interstitial pneumonias (IIPs) are a group of
 are a group of") SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy
 Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Interstitial syndrome
 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy
 Idiopathic Pulmonary Fibrosis Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy JMAJ 46(11): 469 474, 2003 Yukihiko SUGIYAMA Professor, Division of Pulmonary Medicine, Department of
Idiopathic Pulmonary Fibrosis Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy JMAJ 46(11): 469 474, 2003 Yukihiko SUGIYAMA Professor, Division of Pulmonary Medicine, Department of
Radiologic-pathologic correlation of pulmonary diseases
 The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
IPF: Epidemiologia e stato dell arte
 IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
Diagnostic challenges in IPF
 Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Cystic Lung Disease. Cristopher A. Meyer, MD
 Cystic Lung Disease Cristopher A. Meyer, MD Air filled structure with definable wall typically less than 1 mm thick Cris A. Meyer, M.D. Professor of Radiology University of Wisconsin School of Medicine
Cystic Lung Disease Cristopher A. Meyer, MD Air filled structure with definable wall typically less than 1 mm thick Cris A. Meyer, M.D. Professor of Radiology University of Wisconsin School of Medicine
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images
 Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings
 Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings Poster No.: C-2358 Congress: ECR 2013 Type: Educational Exhibit Authors: V. Cuartero Revilla, M. Nogueras Carrasco, P. Olmedilla
Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings Poster No.: C-2358 Congress: ECR 2013 Type: Educational Exhibit Authors: V. Cuartero Revilla, M. Nogueras Carrasco, P. Olmedilla
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Chest imaging II. Interstitial lung diseases
 Chest imaging II. Interstitial lung diseases Dávid L. Tárnoki MD, PhD Ádám D. TárnokiMD, PhD Department of Radiology Semmelweis University Topics 1. Interstitial lung diseases 2. Occupational lung diseases
Chest imaging II. Interstitial lung diseases Dávid L. Tárnoki MD, PhD Ádám D. TárnokiMD, PhD Department of Radiology Semmelweis University Topics 1. Interstitial lung diseases 2. Occupational lung diseases
Lines and crackles. Making sense of ILD
 Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates
 and Updates") Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Diagnostic Imaging of Diffuse Infiltrative Disease of the Lung
 Thematic Review Series Respiration 2004;71:4 19 DOI: 10.1159/000075642 Diagnostic Imaging of Diffuse Infiltrative Disease of the Lung Maurizio Zompatori a Claudio Bnà a Venerino Poletti c Enrica Spaggiari
Thematic Review Series Respiration 2004;71:4 19 DOI: 10.1159/000075642 Diagnostic Imaging of Diffuse Infiltrative Disease of the Lung Maurizio Zompatori a Claudio Bnà a Venerino Poletti c Enrica Spaggiari
Micronodular lung pattern - Differential diagnosis
 Micronodular lung pattern - Differential diagnosis Poster No.: P-0074 Congress: ESTI 2015 Type: Educational Poster Authors: P. Ninitas, F. Marinho, P. Campos, I. Távora ; Lisbon/PT, 1 2 2 3 1 1 3 Funchal/PT,
Micronodular lung pattern - Differential diagnosis Poster No.: P-0074 Congress: ESTI 2015 Type: Educational Poster Authors: P. Ninitas, F. Marinho, P. Campos, I. Távora ; Lisbon/PT, 1 2 2 3 1 1 3 Funchal/PT,
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus
 Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
Challenges in the Diagnosis of Interstitial Lung Disease
 Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Hypersensitivity Pneumonitis: Spectrum of High-Resolution CT and Pathologic Findings
 CT of Hypersensitivity Pneumonitis Chest Imaging Pictorial Essay C. Isabela S. Silva 1 ndrew Churg 2 Nestor L. Müller 1 Silva CIS, Churg, Müller NL Keywords: high-resolution CT, hypersensitivity pneumonitis,
CT of Hypersensitivity Pneumonitis Chest Imaging Pictorial Essay C. Isabela S. Silva 1 ndrew Churg 2 Nestor L. Müller 1 Silva CIS, Churg, Müller NL Keywords: high-resolution CT, hypersensitivity pneumonitis,
Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete Prague, June 2014
 Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Workshop Cyst & Lucency. How to Approach
 Workshop Cyst & Lucency How to Approach To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt
Workshop Cyst & Lucency How to Approach To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt
Challenges in the Diagnosis of Interstitial Lung Disease
 Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Radiological features of idiopathic interstitial pneumonia: a pictorial review
 Radiological features of idiopathic interstitial pneumonia: a pictorial review Poster No.: C-2012 Congress: ECR 2013 Type: Educational Exhibit Authors: M. Piccoli, F. Roccasalva, S. Palmucci, G. Cappello,
Radiological features of idiopathic interstitial pneumonia: a pictorial review Poster No.: C-2012 Congress: ECR 2013 Type: Educational Exhibit Authors: M. Piccoli, F. Roccasalva, S. Palmucci, G. Cappello,
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
American Thoracic Society European Respiratory Society Classification of the Idiopathic Interstitial Pneumonias: Advances in Knowledge since 20021
 This copy is for personal use only. To order printed copies, contact reprints@rsna.org American Thoracic Society European Respiratory Society Classification of the Idiopathic Interstitial Pneumonias: Advances
This copy is for personal use only. To order printed copies, contact reprints@rsna.org American Thoracic Society European Respiratory Society Classification of the Idiopathic Interstitial Pneumonias: Advances
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
T he diagnostic evaluation of a patient with
 546 REVIEW SERIES Challenges in pulmonary fibrosis? 1: Use of high resolution CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias Michael B Gotway, Michelle M
546 REVIEW SERIES Challenges in pulmonary fibrosis? 1: Use of high resolution CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias Michael B Gotway, Michelle M
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
ARTICLE IN PRESS. Ahuva Grubstein a, Daniele Bendayan b, Ithak Schactman c, Maya Cohen a, David Shitrit b, Mordechai R. Kramer b,
 Respiratory Medicine (2005) 99, 948 954 Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature
Respiratory Medicine (2005) 99, 948 954 Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature
International consensus statement on idiopathic pulmonary fibrosis
 Eur Respir J 2001; 17: 163 167 Printed in UK all rights reserved Copyright #ERS Journals Ltd 2001 European Respiratory Journal ISSN 0903-1936 PERSPECTIVE International consensus statement on idiopathic
Eur Respir J 2001; 17: 163 167 Printed in UK all rights reserved Copyright #ERS Journals Ltd 2001 European Respiratory Journal ISSN 0903-1936 PERSPECTIVE International consensus statement on idiopathic
Chronic Interstitial (Restrictive) Lung Disease
 Lung Disease") Chronic Interstitial (Restrictive) Lung Disease Fibrosing Usual interstitial pneumonia (idiopathic pulmonary fibrosis) IPF/UIP Nonspecific interstitial pneumonia(nsip) Cryptogenic organizing pneumonia(cop)
Chronic Interstitial (Restrictive) Lung Disease Fibrosing Usual interstitial pneumonia (idiopathic pulmonary fibrosis) IPF/UIP Nonspecific interstitial pneumonia(nsip) Cryptogenic organizing pneumonia(cop)
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT
 Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP)
") Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP) Assem El Essawy (1) & Amr A. Nassef (٢) Abstract Identification of interstitial pneumonia (IP) was mainly based on histological
Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP) Assem El Essawy (1) & Amr A. Nassef (٢) Abstract Identification of interstitial pneumonia (IP) was mainly based on histological
Hypersensitivity Pneumonitis: Epidemiology and Classification
 Hypersensitivity Pneumonitis: Epidemiology and Classification Ulrich Costabel, MD University of Duisburg-Essen, Ruhrlandklinik Department of Pneumology/Allergy Objectives Definitions, Etiology Epidemiology
Hypersensitivity Pneumonitis: Epidemiology and Classification Ulrich Costabel, MD University of Duisburg-Essen, Ruhrlandklinik Department of Pneumology/Allergy Objectives Definitions, Etiology Epidemiology
Dr.kassim.m.sultan F.R.C.P
 Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Micronodular Lung Disease an algorithm
 Micronodular Lung Disease an algorithm H. Page McAdams, MD Department of Radiology Duke University Medical Center Durham, NC USA page.mcadams@duke.edu Question Which of the following lung diseases is MOST
Micronodular Lung Disease an algorithm H. Page McAdams, MD Department of Radiology Duke University Medical Center Durham, NC USA page.mcadams@duke.edu Question Which of the following lung diseases is MOST
IPF - Inquadramento clinico
 IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
DISEASES OF THE RESPIRATORY SYSTEM LECTURE 5 DR HEYAM AWAD FRCPATH
 DISEASES OF THE RESPIRATORY SYSTEM LECTURE 5 DR HEYAM AWAD FRCPATH RESTRICTIVE, INTERSTITIAL LUNG DISESAES. FIROSING DISESES. GRANULOMATOUS DISEASES. EOSINOPHILIC. SMOKING RELATED. FIBROSING DISEASES
DISEASES OF THE RESPIRATORY SYSTEM LECTURE 5 DR HEYAM AWAD FRCPATH RESTRICTIVE, INTERSTITIAL LUNG DISESAES. FIROSING DISESES. GRANULOMATOUS DISEASES. EOSINOPHILIC. SMOKING RELATED. FIBROSING DISEASES
Unpaid scientific collaborator & advisor with Veracyte, Inc.
 Diagnosis and Classification of Idiopathic Interstitial Pneumonias: Role of Histopathology in the Golden Age of Consensus Jeffrey L. Myers, M.D. A. James French Professor of Diagnostic Pathology Vice Chair
Diagnosis and Classification of Idiopathic Interstitial Pneumonias: Role of Histopathology in the Golden Age of Consensus Jeffrey L. Myers, M.D. A. James French Professor of Diagnostic Pathology Vice Chair
* * APPROACH TO NON- NEOPLASTIC LUNG DISEASE IN TRANSBRONCHIAL AND SURGICAL BIOPSIES. Financial Disclosures: NONE. BIOPSY TECHNIQUES Bronchoscopic
 APPROACH TO NON- NEOPLASTIC LUNG DISEASE IN TRANSBRONCHIAL AND SURGICAL BIOPSIES Thomas V. Colby, M.D. Mayo Clinic Arizona Geraldine C. Zeiler Professor of Cytopathology Mayo Clinic Arizona Financial Disclosures:
APPROACH TO NON- NEOPLASTIC LUNG DISEASE IN TRANSBRONCHIAL AND SURGICAL BIOPSIES Thomas V. Colby, M.D. Mayo Clinic Arizona Geraldine C. Zeiler Professor of Cytopathology Mayo Clinic Arizona Financial Disclosures:
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Imaging: how to recognise idiopathic pulmonary fibrosis
 REVIEW IDIOPATHIC PULMONARY FIBROSIS Imaging: how to recognise idiopathic pulmonary fibrosis Anand Devaraj Affiliations: Dept of Radiology, St George s Hospital, London, UK. Correspondence: Anand Devaraj,
REVIEW IDIOPATHIC PULMONARY FIBROSIS Imaging: how to recognise idiopathic pulmonary fibrosis Anand Devaraj Affiliations: Dept of Radiology, St George s Hospital, London, UK. Correspondence: Anand Devaraj,
Difficulties Diagnosing Idiopathic Pulmonary Fibrosis
 1. er Encuentro Entre Neumólogos y Radiólogos, Madrid, Spain, 2016, October 14th Difficulties Diagnosing Idiopathic Pulmonary Fibrosis Simon Walsh King s College Hospital Foundation Trust London, United
1. er Encuentro Entre Neumólogos y Radiólogos, Madrid, Spain, 2016, October 14th Difficulties Diagnosing Idiopathic Pulmonary Fibrosis Simon Walsh King s College Hospital Foundation Trust London, United
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
The radiological differential diagnosis of the UIP pattern
 5th International Conference on Idiopathic Pulmonary Fibrosis, Modena, 2015, June 12th The radiological differential diagnosis of the UIP pattern Simon Walsh King s College Hospital Foundation Trust London,
5th International Conference on Idiopathic Pulmonary Fibrosis, Modena, 2015, June 12th The radiological differential diagnosis of the UIP pattern Simon Walsh King s College Hospital Foundation Trust London,
Idiopathic Pulmonary of Care
 Chapter 6.1 Living Medical etextbook A Digital Tool at the Point of Care From Projects In Knowledge Pulmonology Idiopathic Pulmonary Fibrosis @Point of Care IPF Case Study: Typical Presentation, Role of
Chapter 6.1 Living Medical etextbook A Digital Tool at the Point of Care From Projects In Knowledge Pulmonology Idiopathic Pulmonary Fibrosis @Point of Care IPF Case Study: Typical Presentation, Role of
Case 4 History. 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar
 Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than
 TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker. Michael B. Gotway, MD
 August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ USA Clinical History: A 55 year old woman presented
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ USA Clinical History: A 55 year old woman presented