Pancreatic Cancer: The ABCs of the AJCC and WHO
|
|
|
- Maximilian McCarthy
- 6 years ago
- Views:
Transcription
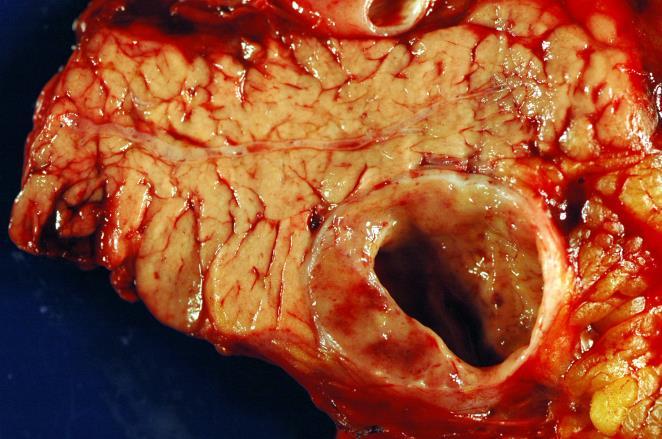
1 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology Case presentation Objectives Discuss pancreatic cancer and clinical relevant subtypes Review AJCC 8 th edition staging of exocrine and endocrine pancreatic neoplasms 2017 WHO classification of pancreatic neuroendocrine neoplasms Case Presentation 78-year-old female presenting with a 1 day history of jaundice and cola-colored urine. The patient had elevated serum liver transaminases and elevated serum pancreatic enzymes. These findings prompted an abdominal computed tomography (CT) scan. 1
2 Liver Head of the Pancreas Kidneys Liver Area of Necrosis Head of the Pancreas Kidneys Liver Bile Duct Pancreatic Mass (5.6 cm) Head of the Pancreas Kidneys 2
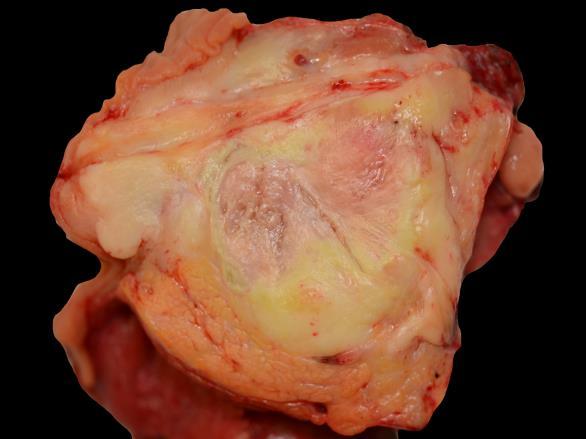
3 Pancreatic Mass (5.6 cm) 3
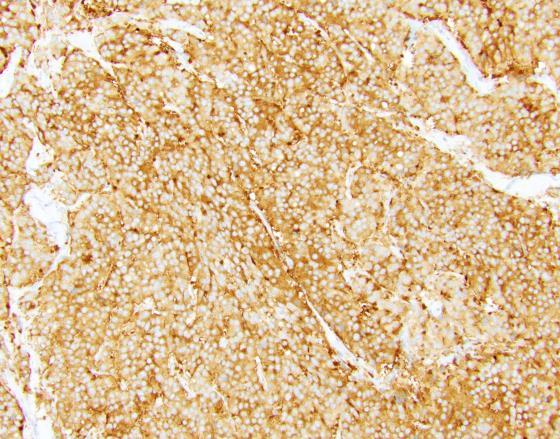
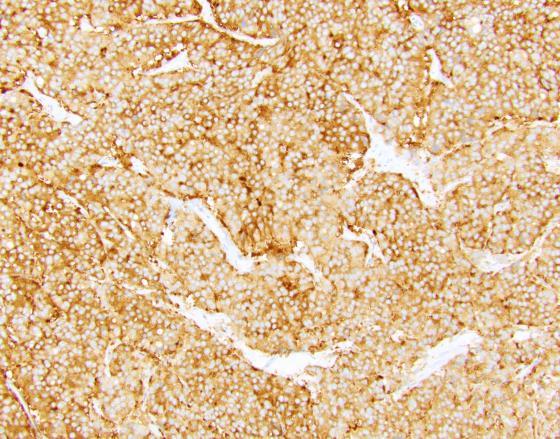
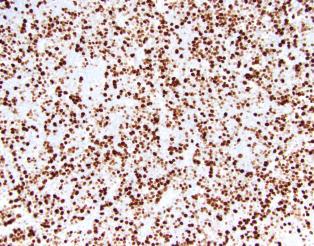
4 Synaptophysin Chromogranin A 4
, intraductal papillary mucinous neoplasm (IPMN) and mucinous cystic neoplasm (MCN) Evolution s role- in both familial and sporadic Surgery- only hope for cure (~15% are resectable) Outcome-")
5 Adenocarcinoma Definition- invasive gland-forming epithelial neoplasm Clinical presentation- diagnosis late in the course Pathology- varies Precursor lesions- pancreatic intraepithelial neoplasia (PanIN), intraductal papillary mucinous neoplasm (IPMN) and mucinous cystic neoplasm (MCN) Evolution s role- in both familial and sporadic Surgery- only hope for cure (~15% are resectable) Outcome- universally poor Common Bile Duct Duodenum Pancreatic Duct Common Bile Duct Duodenum Pancreatic Duct 5
: Most pancreatic cancers evolve through")


6 Pancreatic Duct Pancreatic Duct Pancreatic intraepithelial neoplasia (PanINs): Most pancreatic cancers evolve through PanINs: Low-grade PanIN High-grade PanIN (From Wilentz RE, lacobuzio-donahue CA, et al: Loss of expression of DPC4 in pancreatic intraepithelial neoplasia: evidence that DPC4 inactivation occurs late in neoplastic progression. Cancer Res 2000; 60:2002) 6

: Most")




7 Pancreatic intraepithelial neoplasia (PanINs): Most pancreatic cancers evolve through PanINs: Low-Grade Low-Grade Low-Grade High-Grade Haphazard growth Histologic Grades of Adenocarcinoma Well-differentiated Moderately-differentiated Poorly-differentiated 7

8 Variants of Pancreatic Ductal Adenocarcinoma Adenosquamous Carcinoma A malignant epithelial neoplasm of the pancreas with significant components of both glandular and squamous differentiation The squamous component should comprise at least 30% of the neoplasm Account for 3-4% of the malignancies of the exocrine pancreas Partial response to cisplatinum based chemotherapeutic regimens Squamous Differentiation Glandular Differentiation 8
 in large pools of extracellular mucin The colloid")

9 Colloid Carcinoma An infiltrating adenocarcinoma characterized by mucin producing neoplastic epithelial cells suspended ( floating ) in large pools of extracellular mucin The colloid component should comprise at least 80% of the neoplasm 1-3% of the malignancies of the exocrine pancreas Grossly soft gelatinous Almost always associated with an IPMN 5-year survival rates as high as 57% 9
 in large pools of extracellular mucin The colloid")

10 Perineural Invasion Colloid Carcinoma An infiltrating adenocarcinoma characterized by mucin producing neoplastic epithelial cells suspended ( floating ) in large pools of extracellular mucin The colloid component should comprise at least 80% of the neoplasm 1-3% of the malignancies of the exocrine pancreas Grossly soft gelatinous Almost always associated with an IPMN 5-year survival rates as high as 57% 10


11 Hepatoid Carcinoma A malignant epithelial neoplasm in which a significant component shows hepatocellular differentiation Only a handful have been reported Large polygonal cells with abundant eosinophilic cytoplasm The cells form trabecula and may have a sinusoidal vascularity Immunolabeling is similar if not the same as hepatocellular neoplasms 11
12 T3: Tumor extends beyond the pancreas Adapted from T3: Tumor extends beyond the pancreas Adapted from Medullary Carcinoma A malignant epithelial neoplasm characterized by poor differentiation, pushing borders, a syncytial growth pattern and necrosis May have prominent intratumoral lymphocytes Many, but not all, carcinomas with medullary histology have microsatellite instability Family history of cancer (Lynch syndrome) Trend towards longer survival and response to immune checkpoint inhibitors 12

 Trend towards longer survival and response to immune checkpoint inhibitors")
13 Medullary Carcinoma A malignant epithelial neoplasm characterized by poor differentiation, pushing borders, a syncytial growth pattern and necrosis May have prominent intratumoral lymphocytes Many, but not all, carcinomas with medullary histology have microsatellite instability Family history of cancer (Lynch syndrome) Trend towards longer survival and response to immune checkpoint inhibitors 13


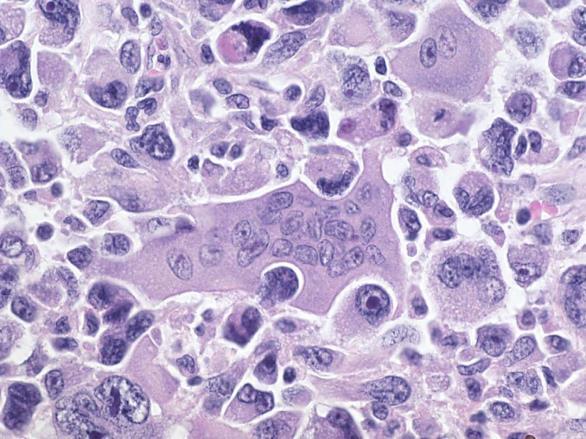
14 Undifferentiated Carcinoma A malignant epithelial neoplasm with a significant component showing no glandular structures or other features to indicate a definite direction of differentiation Range from pleomorphic epithelioid mononuclear cells containing abundant eosinophilic cytoplasm admixed with bizarre frequently multinucleated tumor giant cells, to relatively monomorphic spindle cells Mean survival of 5 months after diagnosis Anaplastic giant cell carcinoma 14

15 Sarcomatoid carcinoma Undifferentiated Carcinoma A malignant epithelial neoplasm with a significant component showing no glandular structures or other features to indicate a definite direction of differentiation Range from pleomorphic epithelioid mononuclear cells containing abundant eosinophilic cytoplasm admixed with bizarre frequently multinucleated tumor giant cells, to relatively monomorphic spindle cells Mean survival of 5 months after diagnosis Undifferentiated Carcinoma with Osteoclast-like Giant Cells Malignant epithelial neoplasm composed of large benign appearing multinucleated giant cells admixed with atypical neoplastic mononuclear cells The atypical mononuclear cells variably express markers of epithelial differentiation The osteoclast-like giant cells express markers of histiocytic/macrophage differentiation (benign) Highly aggressive neoplasms with a mean survival of only 12 months 15
16 16

17 Macrophage marker (CD68) Undifferentiated Carcinoma with Osteoclast-like Giant Cells Malignant epithelial neoplasm composed of large benign appearing multinucleated giant cells admixed with atypical neoplastic mononuclear cells The atypical mononuclear cells variably express markers of epithelial differentiation The osteoclast-like giant cells express markers of histiocytic/macrophage differentiation (benign) Highly aggressive neoplasms with a mean survival of only 12 months How is Pancreatic Cancer Staged? AJCC (7 th Edition): T-staging is prognostically significant Problematic areas for pathology include identifying extension beyond the pancreas >70% of resected pancreatic cancers are T3 Allen PJ et al. Annals of Surgery

18 AJCC 8 th Edition Staging Size rather than tumor extension Primary tumor (pt) ptx Primary tumor cannot be assessed pt0 No evidence of a primary tumor ptis High-grade dysplasia (carcinoma in situ) pt1 Tumor size 2 cm pt2 Tumor size > 2 cm and 4 cm pt3 Tumor size > 4 cm pt4 Tumor involves the celiac axis, superior mesenteric artery and/or common hepatic artery Tis: High-grade dysplasia (carcinoma in situ) pt1: Tumor 2 cm in size Adapted from 18
19 AJCC 8 th Edition Staging Size rather than tumor extension Primary tumor (pt) pt1 Tumor size 2 cm pt1a Tumor size 0.5 cm pt1b Tumor size > 0.5 cm and < 1.0 cm pt1c Tumor size 1.0 to 2.0 cm pt1a through pt1c is primarily for pancreatic adenocarcinomas arising from IPMNs pt2: Tumor > 2 cm but < 4 cm in size Adapted from pt3: Tumor 4 cm in size Adapted from 19
 is staged based on size pt4: Tumor involves the celiac axis, superior mesenteric artery &/or common")
20 Tumor extends beyond the pancreas (doesn t matter still based on tumor size) Adapted from Tumor extends beyond the pancreas (into the spleen) is staged based on size pt4: Tumor involves the celiac axis, superior mesenteric artery &/or common hepatic artery Adapted from 20
 Superior to the pancreatic head/uncinate and body/tail Inferior to the pancreatic head/uncinate")

21 AJCC 8 th Edition Staging Regional lymph nodes (pn) pnx Unable to assess regional lymph nodes pn0 No regional lymph node involvement pn1 Metastasis in 1 to 3 regional lymph nodes pn2 Metastasis in 4 or more regional lymph nodes Regional lymph nodes AJCC 8 th Edition Staging Regional lymph nodes (N) Superior to the pancreatic head/uncinate and body/tail Inferior to the pancreatic head/uncinate and body/tail Anterior pancreaticoduodenal and proximal mesenteric Posterior pancreaticoduodenal and proximal mesenteric Pancreatic head/uncinate: stomach pylorus (infrapyloric and subpyloric), hepatic artery, common bile duct and celiac Pancreatic body/tail: tail of pancreas, splenic hilum and pancreaticolienal N1 and N2: Regional lymph node involvement Adapted from 21


22 AJCC 8 th Edition Staging Distant Metastases (pm) pm0 No distant metastasis pm1 Distant metastasis **Note: M1 disease is typically a contraindication for surgical resection, so frequently a pathologic M0. Adapted from AJCC 8 th Edition Staging T- and N-staging are prognostically significant Allen PJ et al. Annals of Surgery

 Head of the Pancreas Kidneys Pancreatic Head Mass: Sarcoma?")
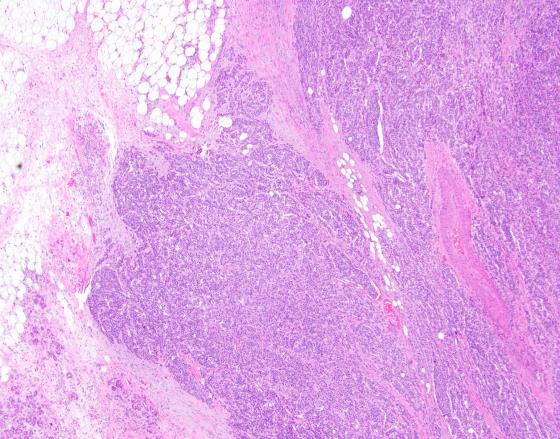
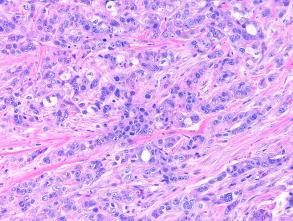
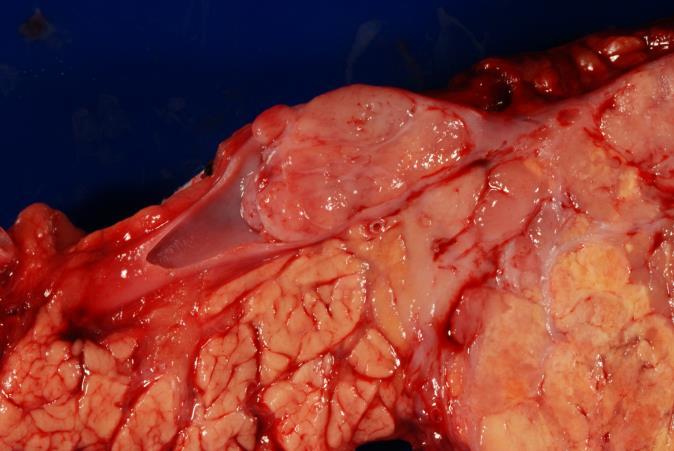
23 Variants Adenosquamous carcinoma Colloid carcinoma Hepatoid carcinoma Medullary carcinoma Undifferentiated carcinoma Undifferentiated carcinoma with osteoclast-like giant cells Liver Bile Duct Pancreatic Mass (5.6 cm) Head of the Pancreas Kidneys Pancreatic Head Mass: Sarcoma??? No Glandular Differentiation Identified 23
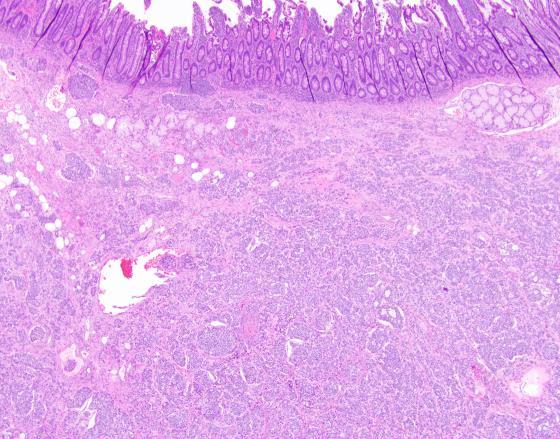
24 Common Bile Duct Ampulla Pancreatic Duct 24


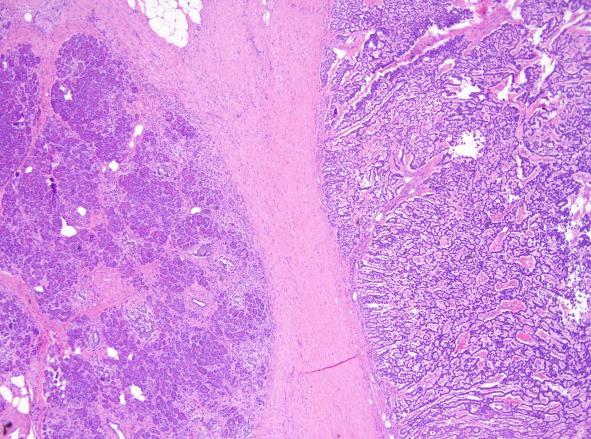
25 Incidence per 100,000 (NET/NEC) Incidence per 100,000 04/09/2018 Residual Pancreatic Parenchyma Spindled Neoplastic Cells Neuroendocrine Neoplasms All malignant neoplasms Neuroendocrine tumors/carcinomas Yao, JC et al. J Clin Oncol. 2008; 26: Desari, A et al. JAMA Oncol. 2017; 3:
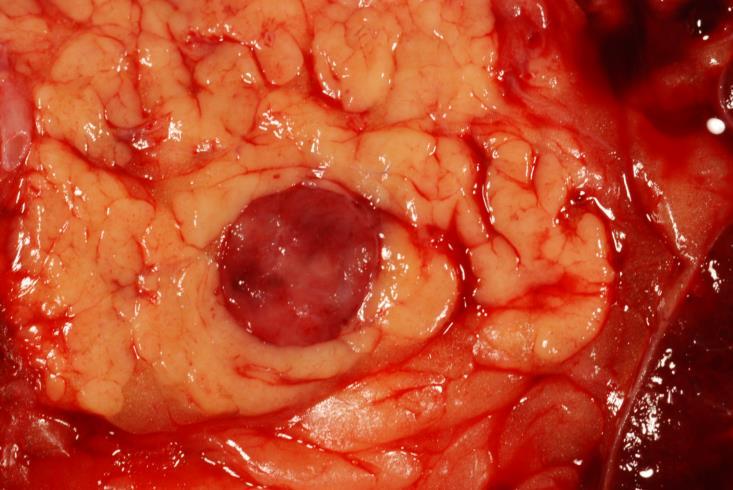
26 Neuroendocrine Neoplasms Lung Rectum Jejunum/Ileum Other Stomach Colon Pancreas Appendix Cecum Duodenum Gross 26


27 27

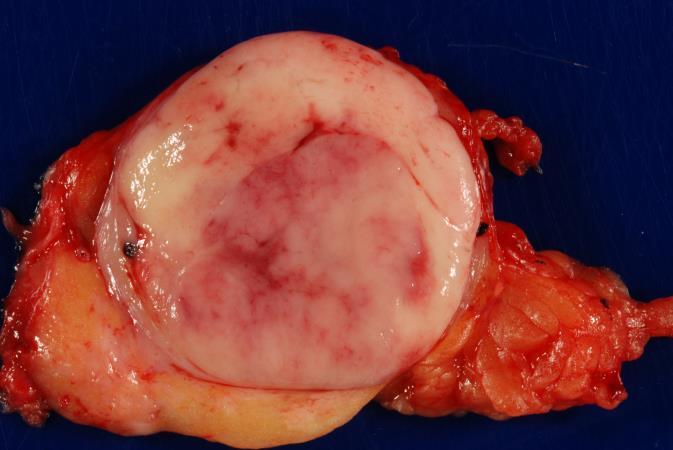
28 Spleen Gross 28

29 29

 Poorly-differentiated neuroendocrine carcinoma (NEC) Small cell")
30 Differentiation Lung (Differentiation): Carcinoid and Atypical carcinoid Neuroendocrine carcinoma Small cell carcinoma Large cell carcinoma Gastroenteropancreatic (Differentiation): Well-differentiated neuroendocrine tumor (NET) Poorly-differentiated neuroendocrine carcinoma (NEC) Small cell carcinoma Large cell carcinoma 30
 Resemblance to islets of")
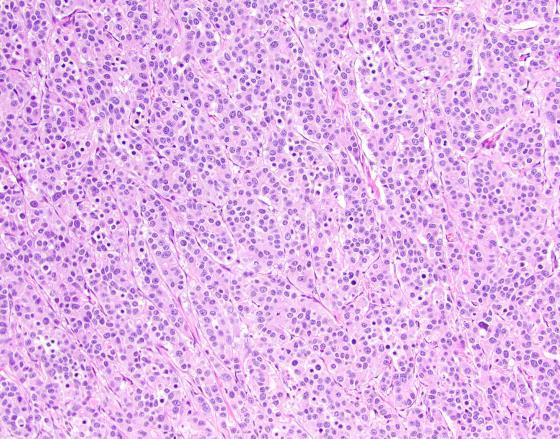
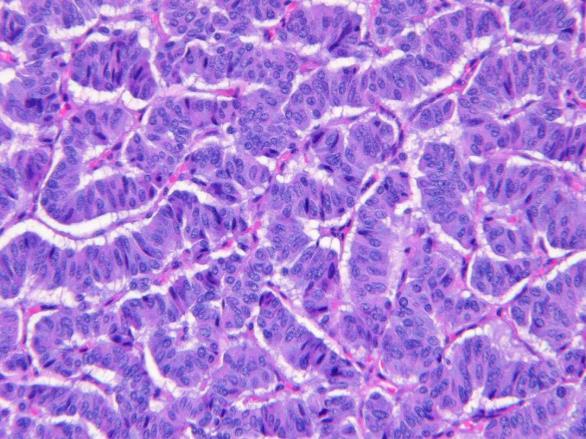
31 Carcinoid / Well-Differentiated Neuroendocrine Tumors Microscopic criteria: Various organoid histologic patterns: nesting, trabecular, glandular, gyriform, tubuloacinar or pseudorosette arrangements Uniform, finely granular, amphophilicto-eosinophilic cytoplasm Coarsely clumped nuclear chromatin ( salt and pepper ) Resemblance to islets of Langerhans 31


32 Poorly-Differentiated Neuroendocrine Carcinomas Microscopic subtypes: Small cell carcinoma Small cells with scant cytoplasm Fine chromatin Nuclear molding Diffuse growth pattern Large cell carcinoma Prominent nesting pattern Moderate amphophilic cytoplasm Large nuclei with clumped chromatin May have prominent nucleoli Small Cell Carcinoma Small Cell Carcinoma Small Cell Carcinoma Large Cell Carcinoma 32
: Low-grade (G1) Intermediate-grade (G2) High-grade (G3) Ki-67 Proliferation Index Ki-67 and Mitotic Index Differentiation Grade Ki-67 Index Mitotic Count")
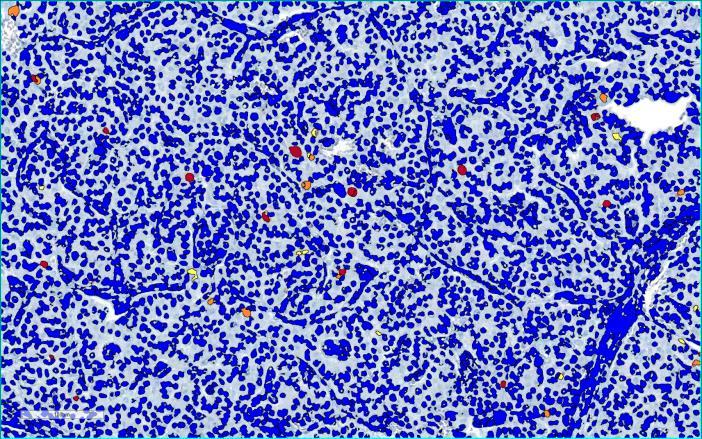
33 Carcinoid / Well-Differentiated Neuroendocrine Tumors Histologic Grade: Lung (< 11 mitoses per hpf): Carcinoid: < 2 mitoses per 10 hpf Atypical carcinoid 2-10 mitoses per 10 hpf Tumor necrosis Gastroenteropancreatic (mitoses & Ki-67): Low-grade (G1) Intermediate-grade (G2) High-grade (G3) Ki-67 Proliferation Index Ki-67 and Mitotic Index Differentiation Grade Ki-67 Index Mitotic Count Well-differentiated Low-grade (G1) < 3% < 2 / 10 HPF Well-differentiated Intermediate-grade (G2) 3 20% 2 20 / 10 HPF Well-differentiated or Poorly-differentiated High-grade (G3) > 20% > 20 / 10 HPF 33

 < 3% < 2 / 10 HPF H&E")


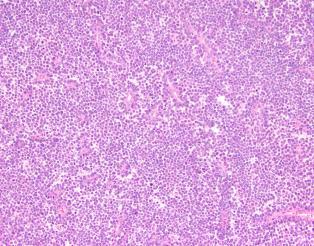
34 Ki-67 and Mitotic Index Differentiation Grade Ki-67 Index Mitotic Count Well-differentiated Low-grade (G1) < 3% < 2 / 10 HPF H&E Ki-67 Ki-67 and Mitotic Index Differentiation Grade Ki-67 Index Mitotic Count Well-differentiated Intermediate-grade (G2) 3 20% 2 20 / 10 HPF H&E Ki-67 Ki-67 and Mitotic Index Differentiation Grade Ki-67 Index Mitotic Count Well-differentiated or Poorly-differentiated High-grade (G3) > 20% > 20 / 10 HPF H&E Ki-67 34
35 Cumulative Survival 04/09/2018 Ki-67 and Mitotic Index G1 G G1 vs G2 G1 vs G3 G2 vs G3 P=0.040 P<0.001 P< G3 N= Survival Time (mo) 1. Rindi G, Klöppel G, Alhman H, et al. Virchows Arch. 2006;449: Rindi G, Klöppel G, Couvelard A, et al. Virchows Arch. 2007;451: Pape UF, Jann H, Müller-Nordhorn J, et al. Cancer. 2008;113: Ki-67 and Mitotic Index If Ki-67 and mitotic counts are discordant, it is recommended to assign a higher grade Differentiation Grade Ki-67 Index Mitotic Count Well-differentiated Low-grade (G1) < 3% < 2 / 10 HPF Well-differentiated Intermediate-grade (G2) 3 20% 2 20 / 10 HPF Well-differentiated or Poorly-differentiated High-grade (G3) > 20% > 20 / 10 HPF 35


36 Tang, LH et al. AJSP :

 > 20% > 20 / 10 HPF G3: NETs vs. NECs 1.0 0.8 0.")

37 Cumulative Survival 04/09/2018 Ki-67 and Mitotic Index If Ki-67 and mitotic counts are discordant, it is recommended to assign a higher grade Differentiation Grade Ki-67 Index Mitotic Count Well-differentiated Low-grade (G1) < 3% < 2 / 10 HPF Well-differentiated Intermediate-grade (G2) 3 20% 2 20 / 10 HPF Well-differentiated or Poorly-differentiated High-grade (G3) > 20% > 20 / 10 HPF G3: NETs vs. NECs G1 G G3 G1 vs G2 G1 vs G3 G2 vs G3 N=193 P=0.040 P<0.001 P< Basturk O, Yang Z, Tang LH, et al. AJSP. 2015; 39: Tang LH, Untch BR, Reidy DL, et al. Clin Cancer Res. 2016; 22:
38 G3: NETs vs. NECs Well-differentiated Neuroendocrine Tumors Surgical resection with curative is the most effective treatment Medical therapy: Somatostatin analogues (imaging) mtor inhibitors Alkylating agents Peptide receptor radionucleotide therapy Poorly-differentiated Neuroendocrine Carcinomas Platinum-based chemotherapy G3: NETs vs. NECs G3: NETs vs. NECs Well-differentiated Neuroendocrine Tumor (G3) or Poorly-differentiated Neuroendocrine Carcinoma (G3) 38
39 Pancreatic: NETs vs. NECs Well-differentiated Neuroendocrine Tumor (G3) or Poorly-differentiated Neuroendocrine Carcinoma (G3) Pancreatic: NETs vs. NECs Genes PanNETs Mutation Frequency MEN1 44% DAXX/ATRX 43% PIK3CA, PTEN, TSC1, & TSC2 15% TP53 3% RB1 0% CDKN2A 0% KRAS 0% TGFBR1, TGFBR2, SMAD4 0% Pancreatic: NETs vs. NECs Genes PanNETs Mutation Frequency MEN1 44% DAXX/ATRX 43% PIK3CA, PTEN, TSC1, & TSC2 15% TP53 3% RB1 0% CDKN2A 0% KRAS 0% TGFBR1, TGFBR2, SMAD4 0% Genes PanNECs Mutation Frequency MEN1 0% DAXX/ATRX 0% PIK3CA, PTEN, TSC1, & TSC2 0% TP53 95% RB1 74% CDKN2A 32% KRAS 29% TGFBR1, TGFBR2, SMAD4 10% 39
40 Pancreatic: NETs vs. NECs Pancreatic: NETs vs. NECs ATRX Pancreatic: NETs vs. NECs Pancreatic NET ATRX 40

41 Pancreatic: NETs vs. NECs Pancreatic NET ATRX RB Pancreatic: NETs vs. NECs Pancreatic NET Pancreatic NEC ATRX RB 41
42 Other Sites: NETs vs. NECs Well-differentiated Neuroendocrine Tumor (G3) or Poorly-differentiated Neuroendocrine Carcinoma (G3) How is a Gastroenteropancreatic Neuroendocrine Carcinoma (NEC) Staged? Primary tumor (pt) Regional lymph nodes (pn) Distant metastases (pm) How is a Gastroenteropancreatic Neuroendocrine Carcinoma (NEC) Staged? Primary tumor (pt) Regional lymph nodes (pn) Distant metastases (pm) Staged as other malignancies arising from that site (e.g. pancreatic adenocarcinoma) 42
43 How is a Gastroenteropancreatic Neuroendocrine Tumor (NET) Staged? Primary tumor (pt) Regional lymph nodes (pn) Distant metastases (pm) Different from other malignant neoplasms at the same organ site How is a Pancreatic NET T-Staged? Primary tumor (pt) ptx Tumor cannot be assessed pt1 Tumor limited to the pancreas, < 2 cm pt2 Tumor limited to the pancreas, 2 to 4 cm pt3 Tumor limited to the pancreas, > 4 cm, or invading the duodenum or common bile duct pt4 Tumor invades adjacent organs (stomach, spleen, spleen, adrenal gland) or wall of large vessels (the celiac axis or superior mesenteric artery) pt1: Tumor limited to the pancreas, < 2 cm pt1 Adapted from 43

44 pt2: Tumor limited to the pancreas, 2 to 4 cm pt2 Adapted from pt3: Tumor > 4 cm or extending into the duodenum or common bile duct pt3 Adapted from pt4: Tumor invades adjacent organs (e.g. spleen), celiac axis or SMA pt4 Adapted from 44
45 pt4: Tumor invades adjacent organs (e.g. spleen), celiac axis or SMA pt4 How is a Pancreatic NET N- and M-Staged? Regional lymph nodes (pn) pnx Unable to assess regional lymph nodes pn0 No regional lymph node involvement pn1 Regional lymph node involvement Distant metastases (pm) pm1 Distant metastases pm1a Metastasis confined to liver pm1b Metastasis to at least extrahepatic site (e.g. lung, ovary, bone, etc.) pm1c Both hepatic and extrahepatic metastases 45
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms
: Neuroendocrine Neoplasms") When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 David S. Klimstra, MD Chairman, Department of Pathology James
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
3/23/2017. Differentiation: Differentiation: Immunohistochemistry. Well Differentiated vs. Poorly Differentiated Neuroendocrine Neoplasms
 Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments
Disclosure Statement When Immunostains Can Get You Into Trouble (and how they can help you out): Neuroendocrine Neoplasms Arthur Purdy Stout Society March 5, 2017 Dr. Klimstra receives royalty payments
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Collecting Cancer Data: Pancreas
 Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Small cell neuroendocrine carcinoma icd 10
 Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Adenocarcinoma of the pancreas
 Adenocarcinoma of the pancreas SEMINARS IN DIAGNOSTIC PATHOLOGY 31 (2014) 443 451 Ralph H.Hruban, MD, David S. Klimstra, MD Paola Parente Anatomia Patologica Casa Sollievo della Sofferenza San Giovanni
Adenocarcinoma of the pancreas SEMINARS IN DIAGNOSTIC PATHOLOGY 31 (2014) 443 451 Ralph H.Hruban, MD, David S. Klimstra, MD Paola Parente Anatomia Patologica Casa Sollievo della Sofferenza San Giovanni
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
NAACCR Webinar Series 4/5/2018 COLLECTING CANCER DATA: PANCREAS
 COLLECTING CANCER DATA: PANCREAS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: PANCREAS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Kyle L. Ziegler, CTR. California Cancer Registry U.C. Davis Health System
 Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
2010 Update. NAACCR Webinar Series 1 4/1/2010. Agenda. Access to 2010 Information. CSv2. Collecting Cancer Data: Soft Tissue Sarcoma
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
5/21/2018. An Update on Pancreas Neoplasms. Arief Suriawinata, M.D. Lines of Differentiation in Pancreatic Neoplasms
 An Update on Pancreas Neoplasms Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and Laboratory Medicine Dartmouth-Hitchcock
An Update on Pancreas Neoplasms Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and Laboratory Medicine Dartmouth-Hitchcock
ORIGINAL ARTICLE. Am J Surg Pathol Volume 00, Number 00,
 ORIGINAL ARTICLE The High-grade (WHO G3) Pancreatic Neuroendocrine Tumor Category Is Morphologically and Biologically Heterogenous and Includes Both Well Differentiated and Poorly Differentiated Neoplasms
ORIGINAL ARTICLE The High-grade (WHO G3) Pancreatic Neuroendocrine Tumor Category Is Morphologically and Biologically Heterogenous and Includes Both Well Differentiated and Poorly Differentiated Neoplasms
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
University Journal of Pre and Para Clinical Sciences
 ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors
 AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
NEOPLASIA. 3. Which of the following tumour is benign a. Chondrosarcoma b. Osteochondroma c. Chondroblastoma d. Ewing s tumour e.
 NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
Undifferentiated carcinoma of the gall bladder: a rare entity
 Case Report Undifferentiated carcinoma of the gall bladder: a rare entity Medhi Pranita 1,*, Dowerah Swagata 2, Dutta Utpal 3, Dutta Aparna 4 1 Associate Professor, 2 Demonstrator, 3 PGT, 4 Assistant Professor,
Case Report Undifferentiated carcinoma of the gall bladder: a rare entity Medhi Pranita 1,*, Dowerah Swagata 2, Dutta Utpal 3, Dutta Aparna 4 1 Associate Professor, 2 Demonstrator, 3 PGT, 4 Assistant Professor,
Oncocytic carcinoma: A rare malignancy of the parotid gland
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Pancreatic intraepithelial
 Pancreatic intraepithelial neoplasia (PanIN) Markéta Hermanová St. Anne s University Hospital Brno Faculty of Medicine, Masaryk University Precursor lesions of invasive pancreatic cancer Pancreatic intraepithelial
Pancreatic intraepithelial neoplasia (PanIN) Markéta Hermanová St. Anne s University Hospital Brno Faculty of Medicine, Masaryk University Precursor lesions of invasive pancreatic cancer Pancreatic intraepithelial
A neoplasm is defined as "an abnormal tissue proliferation, which exceeds that of adjacent normal tissue. This proliferation continues even after
 NEOPLASIA Neoplasia is a very important topic in pathology because neoplasms are both common and serious diseases. A neoplasm literally means a new growth, and this term is used interchangeably with a
NEOPLASIA Neoplasia is a very important topic in pathology because neoplasms are both common and serious diseases. A neoplasm literally means a new growth, and this term is used interchangeably with a
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
Neoplasia part I. Dr. Mohsen Dashti. Clinical Medicine & Pathology nd Lecture
 Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseud
 GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
Protocol for the Examination of Specimens From Patients With Tumors of the Endocrine Pancreas
 Protocol for the Examination of Specimens From Patients With Tumors of the Endocrine Pancreas Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Tumors of the Endocrine Pancreas Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays
 2018 Current Issues in Surgical Pathology Summary (not actual lecture) Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays Sanjay Kakar, MD University of California,
2018 Current Issues in Surgical Pathology Summary (not actual lecture) Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays Sanjay Kakar, MD University of California,
Pathology of pancreatic tumors
 Review Article Pathology of pancreatic tumors Daniel Sanchez, Wang L. Cheung Department of Pathology, Orlando Health, Orlando, USA Contributions: (I) Conception and design: All authors; (II) Administrative
Review Article Pathology of pancreatic tumors Daniel Sanchez, Wang L. Cheung Department of Pathology, Orlando Health, Orlando, USA Contributions: (I) Conception and design: All authors; (II) Administrative
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Solid pseudopapillary tumour of the pancreas: Report of five cases
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..