Case presentation. Dr REESAUL R
|
|
|
- Deirdre Norton
- 5 years ago
- Views:
Transcription
1 Case presentation Dr REESAUL R
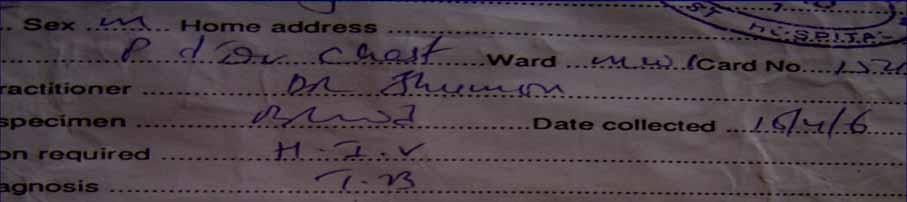
2 Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea
3 Case 1(6/April/2006) Mr S Single 25 years old young man Work helper in `Pizza Hut since 5 years Smokes 5 cigarettes daily since 10 years IVDA since 3 years Occasional Alcohol Elder Brother had TB 6 years back
4 Case 1 Since early childhood several visits AHC and private doctors for cough : ATB, cough mixture and discharge : Diagnosis of acute bronchitis/asthma Since last 4 months(december 2005) complaining cough and night fever Several attendance (4) AHC and twice casualty VH, each visits : ATB, Prednisone,Cough mixture, Paracetamol No investigations done discharge with : Diagnosis of acute bronchitis Refer on 6/4/06 by private GP to chest clinic
5 Case 1 Examination : 1m74,52 kg complaining of weight loss 10kg/4 months Temperature 38.5 Productive cough, dyspnoea with orthopnea, mild haemoptysis and Left chest pain Crackles 2 lungs and reduced air entry left base
6 Case 1 CXR (7/4/06): R + L opacities + infiltrates Left pleural effusion Spo2 : 87 % at rest ABG at rest : Po2: 59 mmhg, Pco2 : 32mmHg, Ph 7.45 Tapping Left effusion : 100 ml blood stain fluid Biochemistry: protein: 3.5g/l, glucose: 6.5mmol Cytology : lymphocytes +++ No malignant cells AFB : direct negative


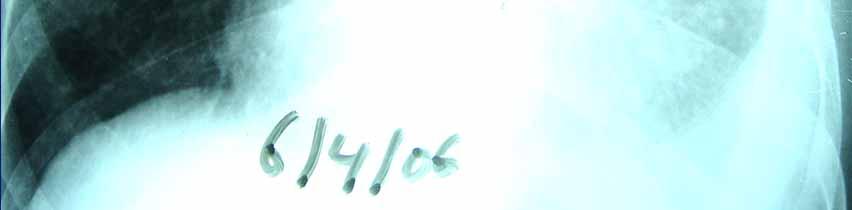
7 CXR on admission 6/4/06



8 Cytology report effusion Viral infection, Tb malignancy,lupus,pancreatitis
9 Case 1 Possible Diagnosis? Young male IVDA with bilateral opacities and infiltrates U>L with Exsudative lymphocytic effusion and hypoxia-hypocapnia + Fever Atypical pneumonia? viral pneumonia? Pleuro-pneumonia in IVDA? Pulmonary tuberculosis with pleural TB? Cystic fibrosis with chest infection involvement? Pneumocystose Jirovecy immuno-suppression? Pulmonary oedema with endocarditis in IVDA? Systemic disease with lung involvement? Malignancy with lung involvement? PE?
10 Case 1 FBC: N with ESR 40, SGOT/SGPT raise Mantoux test : 4mm Blood culture : negative Serology HIV : negative Sputum : pseudomonas aeruginosa +++ Sputum AFB direct : +++ Sweat test normal at VH central lab Serology chlamydia and mycoplasma negative ANF negative ECG normal, Cardiac Echo doppler normal D-dimer negative

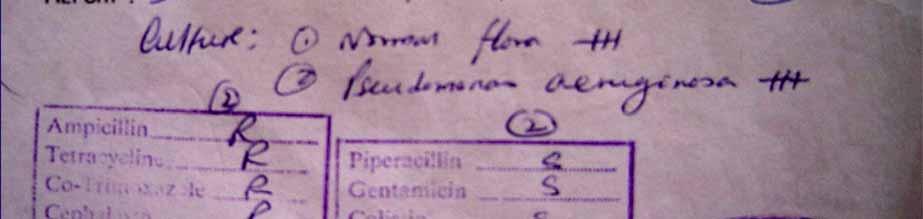
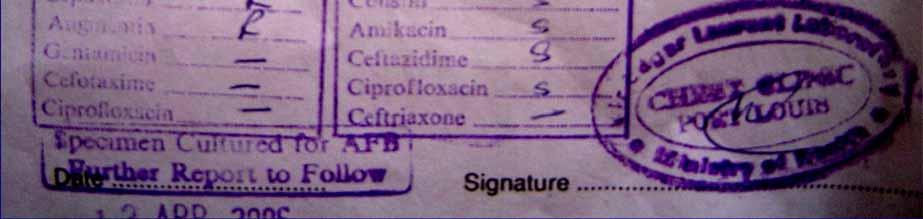
11 Sputum result 12/4/06


12 Blood test HIV



13 Blood test FBC ESR

14 Blood test LFT
15 Positive findings case1 other findings AFB direct +++ Pseudomonas A +++ Exsudative lymphocytic effusion HIV negative Blood culture negative Serology mycoplasma chlamydia negative Sweat test normal ANF negative Cytology effusion no malignancy Echo Doppler cardiac normal D-dimer negative
16 Case 1 Diagnosis : Pulmonary TB and with pseudomonas colonisation Initiated on anti TB drugs : IRP and Ethambutol IV Ceftazidime 1g tds + IV Amikacin 750mg od O2 : 3-4 l/m IV fluids
17 Case 1 Clinical improvement on antibiotics and anti TB drugs Day 6 th sputum pathogen negative for pseudomonas A and sputum AFB direct still ++ Final Diagnosis pulmonary TB IV Antibiotics stop 15 days continuation of Anti TB drugs
18 Case 1 Day 10 th severe skin rash ATT stop and initiated on anti-h1 and prednisone 40mg Reintroduction Pyrazinamide then Ethambutol then Rifampicin then Isoniazid On 150mg Isoniazid pruritis and rash Desensitization to Isoniazid (25/50/75/100/ mg) good response
19 Case 1 Day 30 th : sudden onset dyspnoea and Right chest pain in ward Temp 36 BP 130/60 pulse 130 Spo2 : 87% No Air entry right lung Possible diagnosis?


20 CXR Sudden dyspnea
21 Case 1 CXR : complete Right Pneumothorax Chest drain inserted R side at SSRN 5 th day complete re-expansion R lung and drain removed transfer back to Poudre d`or hospital


22 CXR insertion R chest drain



23 CXR chest drain remove day 5
24 Case 1 Sputum month 1 AFB + Sputum month 2 AFB + Sputum month 3 AFB negative CXR : improving Discharge on IR and B6 follow up OPD chest Clinic Culture sputum M tuberculosis sensitive to 1 st line anti Tb drugs

25 Sputum result month 1



26 Sputum result month 2


27 Sputum result month 3
28 CXR after 6 month treatment


29 Culture sputum
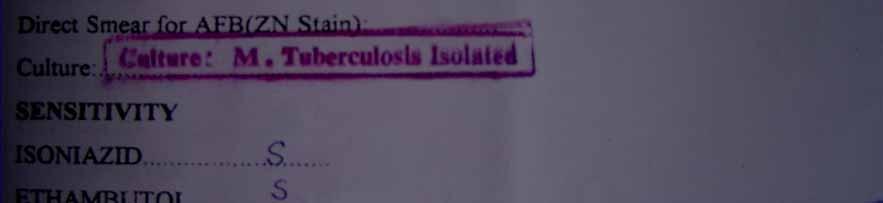

30 Culture/Sensitivity results
31 Case 1 Regular follow up at chest clinic out patient Off all respiratory symptoms CXR improving Sputum AFB negative Completed 6 months regiment anti Tb Regular follow up at chest clinic

32 CRX after 1 year
33 After 6 years 2012 Mr. S admitted 26/03/2012 with : Fever Chronic Cough with dyspnea at rest and effort Headache without stiffness of neck SPO2 85% at rest ABG at rest (Po2 55,Pco2 34, ph 7.39)
34 Examination Fever 38 with Myalgia and night sweats 5kg weight loss since 4 weeks. Bilateral Lung crepitations Jaundice Moderate Hepato-splenomegaly Moderate Ascitis No peripheral lymph nodes

35 26/03/2012
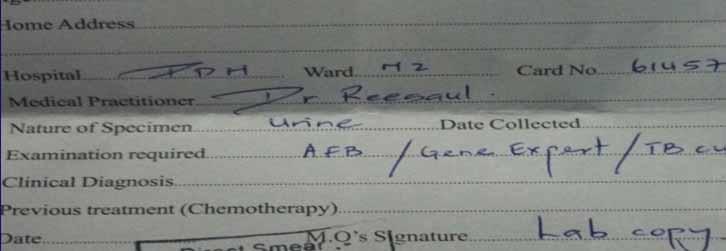
36 Investigations Blood culture, FBC,ESR,CRP H1N1 throat swab Malarial Parasarites Serology HIV Serology Hepatitis B&C Urine ( M/C/S and AFB) Serology Mycoplasma Urine Legionella Serology Leptospirosis Positive findings Pancytopenia ESR: 95 CRP : 65 Raised SGOT SGPT HypoNatraemia :128
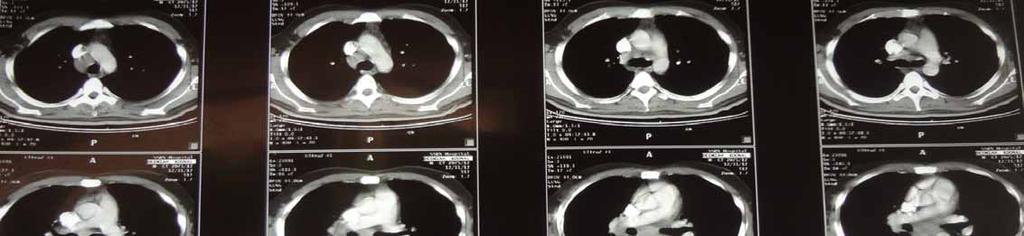
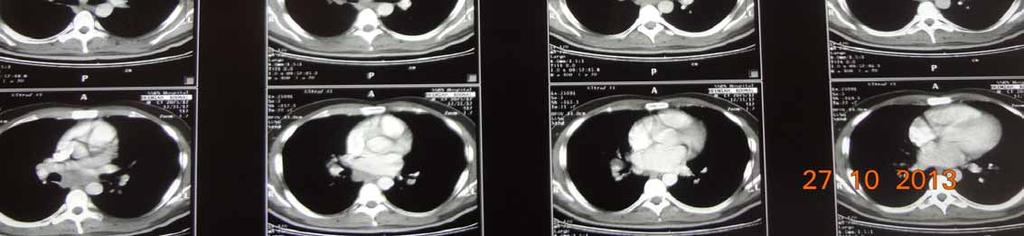
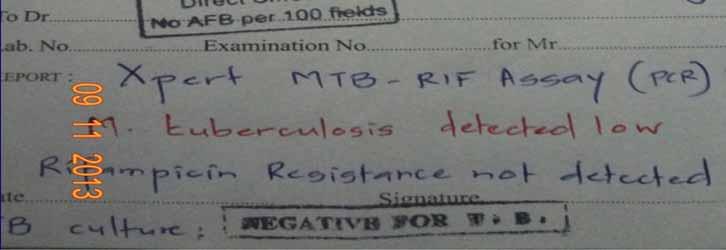
37 Investigations Serology HIV : Positive with CD4 count at 233 Bronchoscopy + lavage : AFB direct Negative and Pneumocystose Negative HR CT scan thorax : miliary opacities + few mediastinal nodes Lumbar Puncture and CT Brain : Normal findings Echo abdomen : ascitis + hepato-splenomegaly Urine Legionella : Negative Serology Leptospirosis : Negative Serology Mycoplasma : Negative Urine for AFB: Direct & culture and PCR GeneXpert MTB/RIF

38 HR CT Thorax
39
40 CD4 count HIV/AIDS CD4 counts and Respiratory infections > <50 Viral infection Bacterial infection M Tuberculosis +_ + + +_ + _ Kaposi disease +_ Pneumocytose juroveci Toxoplasmose Pulmonary cryptococcosis +_ + + CMV/ Atypical Tb(MAC +_ +


41
42 Miliary tuberculosis ( Extra Tb) Initiated on anti Tb drugs Isoniazid + Rifabutin +Ethambutol + Pyrazinamide and IM streptomycin Prednisolone 40mg /daily Oxygen ARV drugs after 3 weeks Clinical and Radiological improvement Regular follow up at chest clinic and AIDS unit




43 27/04/12 22/05/12 26/03/12 13/09/12 21/06/12
44 Mr. S age of 31, died on March 30 th 2013 in the flash flood at Port Louis
45 Miliary Tuberculosis in Mauritius Of all patients with TB in Mauritius, 1.5% are estimated to have miliary tuberculosis Only 2 pediatric cases : 7 and 9 year old boys with miliary TB ( ) Age group in adults: years Sex Ratio Male/female : 4/1
46 GeneXpert MTB/RIF Performed on Patients with Miliary Tb Patient Sputum CSF Gastric aspirate Urine 100% yield stool Culture 1/ Neg + Neg + Neg + 2/(HIV) + Neg Neg + Neg + 3/ Neg Neg Neg + Neg + 4/Pregnant Neg Neg Neg + Neg + 5/child + Neg + + Neg +
47 CD4 count HIV/AIDS CD4 counts and Respiratory infections > <50 Viral infection Bacterial infection Tuberculosis +_ + + +_ + _ Kaposi disease +_ Pneumocytose juroveci Toxoplasmose Pulmonary cryptococcosis +_ + + CMV/ Atypical Tb(MAC +_ +
48 Conclusion Prevention and Reduction of Tb in areas of low incidence Mauritius Tb prevention measures are no longer designed to cover the entire population Rather to enable early detection of index cases in high risk groups(dm,alcohol,hiv.. Reduce prevalence of latent TB infection in persons with risk of progression to active disease(contacts,hiv ) Targeted testing(cxr, Mantoux, IGRA`s) Treatment of Latent TB infection(isoniazid )
49 Thank you Merci
50 ERJ Sensitivity Gene Xpert MTB/RIF for the diagnosis of extra-pulmonary tuberculosis ERJ 2011 vol 40 no

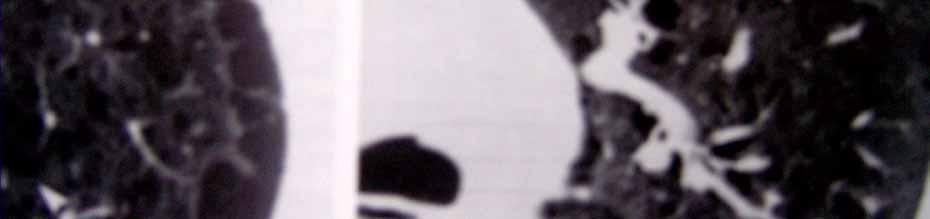

51 HR CT scan thorax


52 we have several thousands years of TB behind us..still 24 th march 1905



53


54 HR CT scan thorax
Index No. All five (05) questions should be answered. All questions carry equal marks.
 questions should be answered. All questions carry equal marks.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
A Vietnamese woman with a 2-week history of cough
 Delphine Natali 1, Hai Tran Pham 1, Hung Nguyen The 2 delphinenatali@gmail.com Case report A Vietnamese woman with a 2-week history of cough A 52-year-old nonsmoker Vietnamese woman without any past medical
Delphine Natali 1, Hai Tran Pham 1, Hung Nguyen The 2 delphinenatali@gmail.com Case report A Vietnamese woman with a 2-week history of cough A 52-year-old nonsmoker Vietnamese woman without any past medical
TB in Children. The diagnostic challenge. Ralph Diedericks Red Cross Hospital
 TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
Enlarging TB Lymph Node Improving or Deteriorating? History. History. Physical examination. Distribution of lymph nodes
 Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Dr Marie Bruyneel and Deborah Konopnicki. BVIKM/SBMIC November 8th, 2012
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Radiological syndroms. Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome
 Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive abdominal distension 3 months Failure
 Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Pneumonia 2017 OMAR PIRZADA
 Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Tuberculosis. Anne Dunleavy. Excellence in specialist and community healthcare
 Tuberculosis Anne Dunleavy Excellence in specialist and community healthcare Overview Epidemiology Illustrative cases Treatment Priorities Conclusion Presentation title / St George s University Hospitals
Tuberculosis Anne Dunleavy Excellence in specialist and community healthcare Overview Epidemiology Illustrative cases Treatment Priorities Conclusion Presentation title / St George s University Hospitals
A 50-year-old male with fever, cough, dyspnoea, chest pain, weight loss and night sweats
 Petru Emil Muntean muntean.petruemil@yahoo.com Pulmonology, Spitalul Clinic Judetean Mures, Targu Mures, Romania. A 50-year-old male with fever, cough, dyspnoea, chest pain, weight loss and night sweats
Petru Emil Muntean muntean.petruemil@yahoo.com Pulmonology, Spitalul Clinic Judetean Mures, Targu Mures, Romania. A 50-year-old male with fever, cough, dyspnoea, chest pain, weight loss and night sweats
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Pleural Effusion. Exudative pleural effusion - Involve an increase in capillary permeability and impaired pleural fluid resorption
 Pleural Effusion Definition of pleural effusion Accumulation of fluid between the pleural layers Epidemiology of pleural effusion Estimated prevalence of pleural effusion is 320 cases per 100,000 people
Pleural Effusion Definition of pleural effusion Accumulation of fluid between the pleural layers Epidemiology of pleural effusion Estimated prevalence of pleural effusion is 320 cases per 100,000 people
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Diagnosis of tuberculosis in children H Simon Schaaf
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis
 All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
* MILIARY MOTTLING --
 * MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
* MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Interstitial syndrome
 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB, or NOT TB? A Tough Question in Kids!
 TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service
 Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Opportunistic Infections BHIVA Guidelines
 Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Latent TB Infection and Screening Programme. Johan van Wijgerden London TB Programme Manager
 Latent TB Infection and Screening Programme Johan van Wijgerden London TB Programme Manager TB case rates by upper tier local authority of residence, London, 2016 TB case rates by Middle Super Output
Latent TB Infection and Screening Programme Johan van Wijgerden London TB Programme Manager TB case rates by upper tier local authority of residence, London, 2016 TB case rates by Middle Super Output
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Clinical Manifestations of HIV
 HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Common things are common, but not always the answer
 Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Drug-sensitive and drugresistant
 CHAPTER 7 87 Drug-sensitive and drugresistant tuberculosis Tuberculosis Types of active TB disease Five I s to reduce the burden of TB in PLHIV Clinical presentation of extrapulmonary TB Evaluating for
CHAPTER 7 87 Drug-sensitive and drugresistant tuberculosis Tuberculosis Types of active TB disease Five I s to reduce the burden of TB in PLHIV Clinical presentation of extrapulmonary TB Evaluating for
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
UK Meningitis Study CRF
 History Date of onset of symptoms Route of admission A and E GP Other Date of admission to hospital* / / Time of admission (24 hour clock) : *record time and date of admission to A and E if admitted ia
History Date of onset of symptoms Route of admission A and E GP Other Date of admission to hospital* / / Time of admission (24 hour clock) : *record time and date of admission to A and E if admitted ia
Guideline for management of children & adolescents with pleural empyema
 CHILD AND ADOLESCENT HEALTH SERVICE PRINCESS MARGARET HOSPITAL FOR CHILDREN Guideline for management of children & adolescents with pleural empyema This guideline provides an evidence-based framework for
CHILD AND ADOLESCENT HEALTH SERVICE PRINCESS MARGARET HOSPITAL FOR CHILDREN Guideline for management of children & adolescents with pleural empyema This guideline provides an evidence-based framework for
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
10/12/2018. Infectious Disease cases in migrants IRN CCHF. AFG 3 +ve env WPV1 Total WPV1: 8 PAK 2 +ve env WPV1 Total WPV1: 3.
 Infectious Disease cases in migrants Sultan Quaboo has been in power since 1970. At that time, there was 50 km tarred road in the country Eskild Petersen, MD, DMSc, DTM&H Adjunct Professor of Tropical
Infectious Disease cases in migrants Sultan Quaboo has been in power since 1970. At that time, there was 50 km tarred road in the country Eskild Petersen, MD, DMSc, DTM&H Adjunct Professor of Tropical
Fever of unknown origin
 Fever of unknown origin Case B History of the present illness 75 years old women presented at our hospital with since months daily fevers between 38 to 39.5 Celsius (100.4-103.1 F) with night sweats. Her
Fever of unknown origin Case B History of the present illness 75 years old women presented at our hospital with since months daily fevers between 38 to 39.5 Celsius (100.4-103.1 F) with night sweats. Her
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
Natural History of Untreated HIV-1 Infection
 Opportunistic infections Dr. Guido van den Berk December 2009 HIV [e] EDUCATION Natural History of Untreated HIV-1 Infection 1000 + CD4 Cells 800 600 400 Constitutional Symptoms Early Opportunistic Infections
Opportunistic infections Dr. Guido van den Berk December 2009 HIV [e] EDUCATION Natural History of Untreated HIV-1 Infection 1000 + CD4 Cells 800 600 400 Constitutional Symptoms Early Opportunistic Infections
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Professor Rob Miller
 BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Professor Rob Miller University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Prof Rob Miller
BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Professor Rob Miller University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Prof Rob Miller
A 43year old man presented with cough and breathlessness. Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital
 A 43year old man presented with cough and breathlessness Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital PARTICULARS OF THE PATIENT: Patients name : Mr. Md. Ismail,43 years. Address : Chittagong.
A 43year old man presented with cough and breathlessness Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital PARTICULARS OF THE PATIENT: Patients name : Mr. Md. Ismail,43 years. Address : Chittagong.
Top Tips for Pleural Disease in 2012
 Top Tips for Pleural Disease in 2012 The unilateral pleural effusion on the Post Take Ward Round Pleural Effusion on CXR Bedside ultrasound + Pleural aspirate Empyema Nil evidence infection Admit IV antibiotics
Top Tips for Pleural Disease in 2012 The unilateral pleural effusion on the Post Take Ward Round Pleural Effusion on CXR Bedside ultrasound + Pleural aspirate Empyema Nil evidence infection Admit IV antibiotics
Diagnostic Approach to Pleural Effusion
 Original Article GCSMC J Med Sci Vol (IV) No (I) January-June 2015 Diagnostic Approach to Pleural Effusion Rushi Patel*, Viral Shah*, Deepali Kamdar** Abstract : Aim : Normally the pleural cavities contain
Original Article GCSMC J Med Sci Vol (IV) No (I) January-June 2015 Diagnostic Approach to Pleural Effusion Rushi Patel*, Viral Shah*, Deepali Kamdar** Abstract : Aim : Normally the pleural cavities contain
Treatment of MDR-TB in high HIV- prevalence settings. Hind Satti, M.D. PIH-Lesotho October 20, 2008
 Treatment of MDR-TB in high HIV- prevalence settings Hind Satti, M.D. PIH-Lesotho October 20, 2008 Early outcomes of MDR-TB treatment Retrospective cohort analysis Registered between July 21, 2007 and
Treatment of MDR-TB in high HIV- prevalence settings Hind Satti, M.D. PIH-Lesotho October 20, 2008 Early outcomes of MDR-TB treatment Retrospective cohort analysis Registered between July 21, 2007 and
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP /15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain,
 Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Appendix to Gibson et al. Application of a decision rule and a D-dimer assay in the
 Appendix to Gibson et al. Application of a decision rule and a D-dimer assay in the diagnosis of pulmonary embolism (Thromb Haemost 2010; 103.4) Case 1 You are paged by an emergency room physician, who
Appendix to Gibson et al. Application of a decision rule and a D-dimer assay in the diagnosis of pulmonary embolism (Thromb Haemost 2010; 103.4) Case 1 You are paged by an emergency room physician, who
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
HIV-associated Pulmonary Disease. Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond QUESTION: HIV-associated Pulmonary Diseases
 Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Let s Talk TB. A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Lancelot M. Pinto, MD, MSc Author Madhukar Pai, MD, PhD co-author and Series Editor Abstract Nearly 50% of patients with
Breathlessness in advanced disease. February 2017
 Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Breathlessness in advanced disease February 2017 Breathlessness Managing breathlessness in primary care Chronic breathlessness Acute exacerbation of breathlessness Breathlessness at end of life Breathlessness
Tuberculosis. New TB diagnostics. New drugs.new vaccines. Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012
 Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Tuberculosis New TB diagnostics. New drugs.new vaccines Dr: Hussein M. Jumaah CABM Mosul College of Medicine 23/12/2012 Tuberculosis (TB )is a bacterial disease caused by Mycobacterium tuberculosis (occasionally
Non-cardiogenic pulmonary edema: when to think and how to treat?
 Non-cardiogenic pulmonary edema: when to think and how to treat? Muhammad Abdur Rahim MBBS, FCPS (Medicine) Assistant Professor BIRDEM Academy and Ibrahim Medical College Case 1 Male, 38 years Fever 4
Non-cardiogenic pulmonary edema: when to think and how to treat? Muhammad Abdur Rahim MBBS, FCPS (Medicine) Assistant Professor BIRDEM Academy and Ibrahim Medical College Case 1 Male, 38 years Fever 4
Skin Pathway Group Alemtuzumab in Cutaneous Lymphoma
 Skin Pathway Group Alemtuzumab in Cutaneous Lymphoma Indication: Treatment of patients with Cutaneous Lymphoma (Unlicensed use) Disease control prior to Reduced Intensity Conditioning Stem Cell Transplant
Skin Pathway Group Alemtuzumab in Cutaneous Lymphoma Indication: Treatment of patients with Cutaneous Lymphoma (Unlicensed use) Disease control prior to Reduced Intensity Conditioning Stem Cell Transplant