Lung diseases. Fatima Obeidat, MD Assistant Professor of Pathology/Neuropathology University of Jordan
|
|
|
- Jeffery Allen
- 5 years ago
- Views:
Transcription

1 Lung diseases Fatima Obeidat, MD Assistant Professor of Pathology/Neuropathology University of Jordan
2 Restrictive lung disease Granulomatous types
3 I. Sarcoidosis - Although sarcoidosis is an example of a restrictive lung disease, it is a multisystem disease characterized by noncaseating granulomas in many tissues and organs.
4 - Mycobacterial or fungal infections may also produce noncaseating granulomas; so the histologic diagnosis of sarcoidosis is one of exclusion
5 Epidemiology - Sarcoidosis occurs throughout the world, affecting both genders and all races and age groups. - There is a predilection for adults younger than 40 years of age - Sarcoidosis is one of the few pulmonary diseases with a higher prevalence among nonsmokers.
6 ETIOLOGY AND PATHOGENESIS - Although the etiology of sarcoidosis remains unknown, several lines of evidence suggest that it is a disease of disordered immune regulation in genetically predisposed persons exposed to certain environmental agents
7 - Immunologic abnormalities in sarcoidosis suggest the development of a cell mediated response to an unidentified antigen and the process is driven by CD4+ helper T cells. - These abnormalities include: 1. Intra alveolar and interstitial accumulation of CD4+ TH1 cells
8 2. Increases in T cell derived TH1 cytokines such as IL2 and IFN-γ, resulting in T cell expansion and macrophage activation. 3. The bronchoalveolar lavage contains abundant CD4+ T cells 4. Anergy to common skin test antigens such as purified protein derivative (PPD
9 - The role of genetic factors is suggested by familial clustering and association with HLA classes such as HLA-A1 and HLA-B8 - After lung transplantation, sarcoidosis recurs in the new lungs in 75% of cases
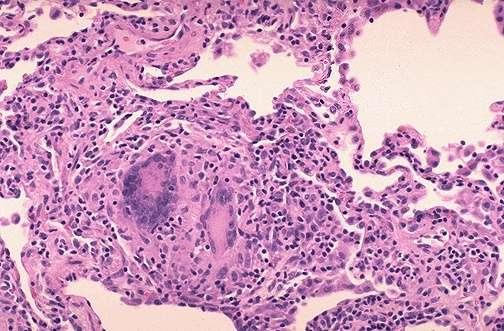
10 MORPHOLOGY - The diagnostic histopathologic feature is noncaseating epithelioid granuloma, irrespective of the organ involved
11 Note: The giant cells may show 1. Schaumann bodies: - Are laminated concretions composed of calcium and proteins 2. Asteroid bodies - Are Stellate inclusions enclosed within giant cells Note- Their presence (1&2) is not required for diagnosis of sarcoidosis they also may occur in granulomas of other origins

12 Schaumann bodies

13 Asteroid bodies
14 - Rarely, foci of central necrosis may be present in sarcoid granulomas. - Caseation necrosis typical of tuberculosis is absent.
15 Involved organs: 1. The lungs are involved at some stage of the disease in 90% of patients: - The granulomas predominantly involve the interstitium rather than air spaces, with some tendency to localize in the connective tissue around bronchioles and venules and in the pleura
16 - In 5% to 15% of patients, the granulomas eventually are replaced by diffuse interstitial fibrosis, resulting in a so called honeycomb lung 2. Intrathoracic hilar and paratracheal lymph nodes are enlarged in 75% to 90% of patients, while a third present with peripheral lymphadenopathy
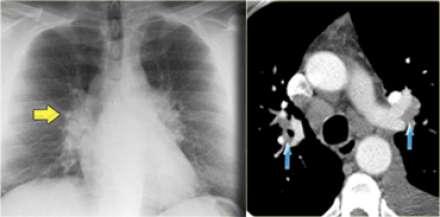
17 sarcoidosis
18 3. Skin lesions are encountered in approximately 25% of patients A. Erythema nodosum: - Is the hallmark of acute sarcoidosis consists of raised, red, tender nodules on the anterior aspects of the legs.

19 Erythema Nodosum
20 - Sarcoidal granulomas are uncommon in these lesions. b. Discrete painless subcutaneous nodules, and these usually reveal abundant noncaseating granulomas
21 3. Involvement of the eye occurs in about one half of patients and the ocular involvement takes the form of iridocyclitis. - These ocular lesions are frequently accompanied by inflammation in the lacrimal glands, with suppression of lacrimation
22 4. Unilateral or bilateral parotitis with painful enlargement of the parotid glands occurs in less than 10% of patients with sarcoidosis; some develop xerostomia (dry mouth).
23 5- Other findings include hypercalcemia and is not related to bone destruction but is caused by increased calcium absorption secondary to production of active vitamin D by the mononuclear phagocytes in the granulomas.
24 Clinical Features - In many affected persons the disease is asymptomatic, discovered on routine chest films as bilateral hilar adenopathy or as an incidental finding at autopsy.
25 - In about two thirds of symptomatic cases. a. gradual appearance of respiratory symptoms (shortness of breath, dry cough, or vague substernal discomfort) or b. constitutional signs and symptoms (fever, fatigue, weight loss, anorexia, night sweats)
26 - Because of the variable and nondiagnostic clinical features, diagnosis is made by lung or lymph node biopsy. - The presence of non caseating granulomas is suggestive of sarcoidosis, but other identifiable causes of granulomatous inflammation must be excluded
27 Clinical course - Sarcoidosis is characterized by either progressive chronicity or periods of activity interspersed with remissions - 70% of affected persons recover with minimal or no residual manifestations
28 - 20% develop permanent lung dysfunction or visual impairment - 10% develop pulmonary fibrosis and cor pulmonale
29 2. Hypersensitivity Pneumonitis - Is an immunologically mediated inflammatory lung disease that primarily affects the alveoli and is often called allergic alveolitis. - Most often it is an occupational disease that results from heightened sensitivity to inhaled antigens such as in moldy Hay.
30 - The damage occurs at the level of alveoli ;so manifests as a predominantly restrictive lung disease. - The occupational exposures are diverse, but the syndromes share common clinical and pathologic findings and probably have a very similar pathophysiologic basis
31 Examples Syndrome Exposure-Antigens a. Farmer's lung Moldy hay--micropolyspora b. Maple bark disease-moldy maple bark - Cryptostroma c-pigeon breeder's lung-pigeon droppings-pigeon serum proteins in droppings
32 - Is an immunologically mediated disease 1. Bronchoalveolar lavage specimens consistently demonstrate increased numbers of T lymphocytes of both CD4+ and CD8+ phenotype. 2. Most patients have specific antibodies in their serum
33 3. Cmplement and immunoglobulins have been demonstrated within vessel walls by immunofluorescence, indicating type III hypersensitivity. 4. The presence of noncaseating granulomas in two thirds of patients with this disorder suggests a role for type IV hypersensitivity as well.
34 Morphology - Patchy mononuclear cell infiltrates in the pulmonary interstitium mainly lymphocytes - Interstitial non-caseating granulomas are present in about 2 thirds of th cases - In advanced cases, diffuse interstitial fibrosis
35 Hypersensitivity Pneumonitis
36 Clinical Manifestations - May manifest either as: A. An acute reaction: - Characterized by fever, cough, dyspnea, and constitutional signs and symptoms arising 4 to 8 hours after exposure.
37 - With the acute form of this disease, the diagnosis is usually obvious because of the temporal relationship of symptom onset to exposure to the incriminating antigen.
38 b. or as a chronic disease - characterized by insidious onset of cough, dyspnea, malaise, and weight loss.
39 - If antigenic exposure is terminated after the acute attacks, complete resolution of pulmonary symptoms occurs within days - Failure to remove the inciting agent eventually results in an irreversible chronic interstitial pulmonary disease

40 Honeycomb lung
41 Diffuse alveolar hemorrhagic syndromes
42 1. Goodpasture Syndrome - Is an uncommon condition characterized by a proliferative, usually rapidly progressive, glomerulonephritis( and) hemorrhagic interstitial pneumonitis. - Both the renal and the pulmonary lesions are caused by antibodies targeted against the noncollagenous domain of the α3 chain of collagen IV.
43 - These antibodies can be detected in the serum of more than 90% of persons with Goodpasture syndrome
44 - The characteristic linear pattern of immunoglobulin deposition (usually IgG, sometimes IgA or IgM) that is the hallmark diagnostic finding in renal biopsy specimens may be seen along the alveolar septa by immunoflurescence studies.
45 - Plasmapheresis and immunosuppressive therapy have markedly improved the once-dismal prognosis for this disease. - Plasma exchange removes offending antibodies, and immunosuppressive drugs inhibit antibody production. - With severe renal disease, renal transplantation is eventually required
46 2.Idiopathic Pulmonary Hemosiderosis - Is a rare disease of uncertain etiology that has pulmonary manifestations and histologic features similar to those of Goodpasture syndrome but a. No associated renal disease b. No circulating anti-basement membrane antibody..
47 - Most cases occur in children, although the disease is reported in adults as well, who have a better prognosis - With steroid and immunosuppressive therapy, survival has markedly improved from the historical 2.5 years; - thus, an immune-mediated etiology is postulated

48 Diffuse alveolar hemorrhage syndrome perl sstain

49 Lung tumors
50 - Primary lung cancer is also a common disease accounting for 95% of primary lung tumors Carcinomas - Carcinoma of the lung is the single most important cause of cancer-related deaths in industrialized countries - It accounts for about one third of cancer deaths in men, and has become the leading cause of cancer deaths in women
51 - The peak incidence of lung cancer is in persons in their 50s and 60s. - The prognosis with lung cancer is dismal: 1.The 5- year survival rate for all stages of lung cancer combined is about 16%, 2. disease localized to the lung, the 5-year survival rate is 45%
52 - The four major histologic types of carcinomas of the lung a. Adenocarcinoma b. Squamouscell carcinoma, c. Small cell carcinoma, d. and large cell carcinoma
53 - Because of changes in smoking patterns in the U.S., adenocarcinoma has replaced squamous cell carcinoma as the most common primary lung tumor in recent years
54 - Carcinomas of the lung were classified into two groups: a. Small cell lung cancer (SCLC) and b. Non-small cell lung cancer (NSCLC), including adenocarcinomas and squamous cell carcinomas.
55 - The reason for this historical distinction was that virtually all SCLCs have metastasized by the time of diagnosis and are not curable by surgery and are treated by chemotherapy, with or without radiation therapy
56 - By contrast, NSCLCs were more likely to be resectable and usually responded poorly to chemotherapy; however, now therapies are available that target specific mutated gene products present in the various subtypes of NSCLC, mainly in adenocarcinomas. - NSCLC must be classified into histologic and molecular subtypes
57 ETIOLOGY - There is strong evidence that cigarette smoking and, to a much lesser extent, other environmental insults are responsible for the genetic changes in lung cancers. - About 90% of lung cancers occur in active smokers or those who stopped recently.
58 - The increased risk becomes 60 times greater among habitual heavy smokers (two packs a day for 20 years) than among nonsmokers. - Since only 11% of heavy smokers develop lung cancer, - however, other predisposing factors must be operative in the pathogenesis of this deadly disease.
59 - The mutagenic effect of carcinogens is conditioned by (genetic) factors. - Many chemicals (procarcinogens) require metabolic activation via the P- 450 monooxygenase enzyme system for conversion into ultimate carcinogens
60 - Persons with specific genetic polymorphisms involving the P-450 genes have an increased capacity to metabolize procarcinogens derived from cigarette smoke, and thus have the greatest risk for development of lung cancer
61 - For reasons not entirely clear, women have a higher susceptibility to carcinogens in tobacco than men. - Although cessation of smoking decreases the risk of developing lung cancer over time, it may never return to baseline levels
62 - Passive smoking increases the risk of developing lung cancer to approximately twice that of nonsmoker - The smoking of pipes and cigars also increases the risk, but only modestly
63 - There is increased incidence of lung carcinoma in asbestos workers; and workers exposed to dusts containing arsenic, chromium, uranium, nickel, and vinyl chloride
64 Note- Exposure to asbestos increases the risk of lung cancer fivefold in nonsmokers. - Heavy smokers exposed to asbestos have an approximately 55 times greater risk for development of lung cancer than that for nonsmokers not exposed to asbestos
65 PATHOGENESIS - Smoking-related carcinomas of the lung arise by a stepwise accumulation of a multitude of genetic abnormalities that result in transformation of benign progenitor cells in the lung into neoplastic cells.
66 - The sequence of molecular changes is not random but follows a predictable sequence that parallels the histologic progression toward cancer.
67 - Inactivation of tumor suppressor genes located on the short arm of chromosome 3 (3p) is a very early event, whereas TP53 mutations or activation of the KRAS
68 2. In. Adenocarcinomas a.activating mutations of the epidermal growth factor receptor (EGFR) and these tumors are sensitive to agents that inhibit EGFR signaling, but the response often is short-lived.
69 b. MET tyrosine kinase gene amplifications c. In 4% of adenocarcinomas are EML4- ALK tyrosine kinase fusion genes and
70 4. ALK tyrosine kinase fusion genes and c- - These abnormalities, while rare, are important because of their therapeutic implications, as they can be targeted with tyrosine kinase inhibitors.
71 - The identification of genetic alterations producing overactive EGFR, ALK, and MET has opened up a new era of "personalized" lung cancer therapy, in which the genetics of the tumor guides the selection of drugs
72 - Among the major histologic subtypes of lung cancer, squamous and small-cell carcinomas show the strongest association with tobacco exposure.
73 MORPHOLOGY 1. Squamous cell carcinomas : a. are more common in men than in women b. are closely correlated with a smoking history;
74 c. They tend to arise centrally in major bronchi and eventually spread to local hilar nodes, d. Disseminate outside the thorax later than do other histologic types
75 e. Large lesions may undergo central necrosis, giving rise to cavitation. f. Are preceded by the development, over years, of squamous metaplasia or dysplasia in the bronchial epithelium,
76 h. Eventually, the small neoplasm reaches a symptomatic stage, when mass begins to obstruct the lumen of a major bronchus, often producing distal atelectasis and infection.

77 Squamous cell carcinoma of lung
78 2. Adenocarcinomas: a. May occur as central lesions but usually are more peripherally located, many with a central scar. b. Are the most common type of lung cancer in women and nonsmokers
79 c.in general, adenocarcinomasgrow slowly and form smaller masses than do the other subtypes d. they tend to metastasize widely at an early stage - On histologic examination, they may assume a variety of forms, including :
80 a. acinar(gland-forming), b. and. papillary, b. Mucinous which often is multifocal and may manifest as pneumonia like consolidation) d. and solid types. :requires demonstration of intracellular mucin production by special stains to establish its adenocarcinomatous lineage
81 Note: Although foci of squamous dysplasia may be present in the epithelium proximal to resected adenocarcinomas, these are not the precursor lesions for this tumor.
82 - The putative precursor of peripheral - adenocarcinomas is atypical adenomatous hyperplasia which progresses to a. adenocarcinoma in situ (formerly bronchioloalveolar carcinoma), b. Minimally invasive adenocarcinoma (tumor less than 3 cm and invasive component measuring 5 mm or less), c. and invasive adenocarcinoma (tumor of any size that has invaded to depths greater than 5 mm).
83 Adenocarcinomain situ (AIS), formerly called bronchioloalveolarcarcinoma, often involves peripheral parts of the lung, as a single nodule. - The key features of AIS are: a. Diameter of 3 cm or less, b. Growth along preexisting structures, c. and preservation of alveolar architecture
84 d. The tumor cells, which may be nonmucinous, mucinous or mixed, grow in a monolayer along the alveolar septa, which serve as a scaffold (this has been termed a lepidic
85 growth pattern, e. By definition, AIS does not demonstrate destruction of alveolar architecture or stromal invasion with desmoplasia, features that would merit the diagnosis of frank adenocarcinoma
86 3. Small cell lung carcinomas (SCLCs) are: a. Centrally located with extension into the lung parenchyma b. Early involvement of the hilar and mediastinal nodes. c. Are composed of tumor cells: 1. with a round to fusiformshape, scant cytoplasm, and finely granular chromatin.
87 2. Mitotic figures frequently are seen 3.Necrosis is invariably present and may be extensive 5. Fragile cells that show fragmentation and "crush artifact". 6. Nuclear molding resulting from close apposition of tumor cells that have scant cytoplasm.

88 Small cell carcinoma of the lung
89 1. For all of these neoplasms, it is possible to trace involvement of successive chains of nodes in carina, in the mediastinum, and in the neck (scalene nodes) and clavicular regions and then distant metastases. - Involvement of the left supraclavicular node (Virchow node) is particularly characteristic and sometimes calls attention to an occult primary tumor
90 3. They may infiltrate the superior vena cava to cause either venous congestion or the vena caval syndrome
91 3.Apical neoplasms (Pancoast tumors) causes Pancoast syndrome characterized by: a. Invasion of the brachial or cervical sympathetic plexus to cause severe pain in the distribution of the ulnar nerve r to produce Horner syndrome (ipsilateral enophthalmos,ptosis, miosis, and anhidrosis).
92 b.is accompanied by destruction of the first and second ribs and sometimes thoracic vertebrae
93 Clinical Course - Are silent, cancers that in many cases have spread so as to be unresectable before they produce symptoms. - In some instances, chronic cough and expectoration call attention to still localized, resectable disease.
94 - By the time hoarseness, chest pain, superior vena cava syndrome, pleural effusion, or segmental atelectasis or pneumonitis makes its appearance, the prognosis is grim
95 - Too often, the tumor presents with symptoms resulting from metastatic spread to the brain (mental or neurologic changes), liver (hepatomegaly), or bones (pain). - Although the adrenals may be nearly obliterated by metastatic disease, adrenal insufficiency (Addison disease) is uncommon,
96 - It is estimated that 3% to 10% of all patients with lung cancer develop clinically overt paraneoplasticsyndromes. 1. Hypercalcemia: caused by secretion of a parathyroid hormone-related peptide by squamous cell carcinoma
97 - Osteolytic lesions may also cause hypercalcemia, but this would not be a paraneoplastic syndrome 2.Cushing syndrome (production of Adrenocorticotropic hormone);by small cell carcinoma
98 (3) syndrome of inappropriate secretion of antidiuretic hormone; by small cell carcinoma (4) neuromuscular syndromes, including a myasthenic syndrome, peripheral neuropathy, and polymyositis 5) clubbing of the fingers and hypertrophic pulmonary osteoarthropathy by any type of carcinoma (
99 6) coagulation abnormalities, including migratory.thrombophlebitis, nonbacterial endocarditis, adenocarcinoma
Reparatory system 18 lectures Heyam Awad
 Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system lectures Heyam Awad
 Reparatory system lectures 8-10 Heyam Awad note These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system lectures 8-10 Heyam Awad note These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors.
 Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
Cancer in the United States, 2004
 Cancer in the United States, 2004 Five-year Cancer Survival Rates (%) US 1974-1998 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast Source: CA Cancer J Clin 2000;50:7-33
Cancer in the United States, 2004 Five-year Cancer Survival Rates (%) US 1974-1998 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast Source: CA Cancer J Clin 2000;50:7-33
Lung Cancer Risks. Cancer in the United States, Cancer Death Rates, US The Scheme: From Nicotine Addiction to Lung Cancer
 Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer. Definition of lung cancer Malignancy arising from lung tissue
 Lung Cancer Definition of lung cancer Malignancy arising from lung tissue Epidemiology of lung cancer Commonest malignancy in western world Commonest cause of death in men and women in the UK Approximately
Lung Cancer Definition of lung cancer Malignancy arising from lung tissue Epidemiology of lung cancer Commonest malignancy in western world Commonest cause of death in men and women in the UK Approximately
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
8/22/2016. Major risk factors for the development of lung cancer are: Outline
 Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma
 July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
INDEX. surgpath.theclinics.com. Note: Page numbers of article titles are in boldface type. diffuse pleural fibrosis, pleural plaques,
 INDEX Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, minimally invasive. See Minimally invasive adenocarcinoma (MIA). Airway-centered interstitial fibrosis, 183 184 ALK (anaplastic
INDEX Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, minimally invasive. See Minimally invasive adenocarcinoma (MIA). Airway-centered interstitial fibrosis, 183 184 ALK (anaplastic
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
3/30/2009 Lung Cancer Deaths 2008 Lung Cancer Deaths Lung Cancer Deaths--Males Males 5
 LUNG CANCER 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Very common Very lethal Lung Cancer Median age of diagnosis approximately 70 years, but affects all ages(even pediatric!) Advances in
LUNG CANCER 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Very common Very lethal Lung Cancer Median age of diagnosis approximately 70 years, but affects all ages(even pediatric!) Advances in
Lung Cancer Incidence 2008 Lung Cancer Deaths-Males 2008 Incidence Total U.S.(all types): 1,437,180 Lung Cancer Deaths-Females Lung cancer 215,000(15%
: 1,437,180 Lung Cancer Deaths-Females Lung cancer 215,000(15%") Multidisciplinary approach 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Neurology Neurosurgery Orthopedic surgery General surgery Vascular surgery Gastroenterology Cardiology Lung Cancer Very
Multidisciplinary approach 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Neurology Neurosurgery Orthopedic surgery General surgery Vascular surgery Gastroenterology Cardiology Lung Cancer Very
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Definition. Epidemiology. Lung Cancer is a disease which cancer (malignant tumors) cells grow in the lungs. LUNG CANCER Debra Mercer BSN, RN, RRT
 cells grow in the lungs. LUNG CANCER Debra Mercer BSN, RN, RRT") LUNG CANCER Debra Mercer BSN, RN, RRT Definition Lung Cancer is a disease which cancer (malignant tumors) cells grow in the lungs. Epidemiology Leading cancer killer in both men and women in the US - 169,
LUNG CANCER Debra Mercer BSN, RN, RRT Definition Lung Cancer is a disease which cancer (malignant tumors) cells grow in the lungs. Epidemiology Leading cancer killer in both men and women in the US - 169,
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the highest incidence
 LUNG CANCER 2010 Mark B. Stoopler, M.D. Division of Medical Oncology Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the
LUNG CANCER 2010 Mark B. Stoopler, M.D. Division of Medical Oncology Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Lecture Goals. Lung (Bronchogenic) Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic
 Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic") Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Chronic Diffuse Interstitial (Restrictive) Diseases. By: Shefaa Qa qa
 Diseases. By: Shefaa Qa qa") Chronic Diffuse Interstitial (Restrictive) Diseases By: Shefaa Qa qa Restrictive lung diseases, are characterized by reduced expansion of lung parenchyma (lung compliance) and decreased total lung capacity.
Chronic Diffuse Interstitial (Restrictive) Diseases By: Shefaa Qa qa Restrictive lung diseases, are characterized by reduced expansion of lung parenchyma (lung compliance) and decreased total lung capacity.
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Histopathological and CT Imaging Correlation of Various Primary Lung Carcinoma
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 3 Ver. VII (Mar. 2016), PP 104-110 www.iosrjournals.org Histopathological and CT Imaging Correlation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 3 Ver. VII (Mar. 2016), PP 104-110 www.iosrjournals.org Histopathological and CT Imaging Correlation
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
DISEASES OF THE RESPIRATORY SYSTEM LECTURE 5 DR HEYAM AWAD FRCPATH
 DISEASES OF THE RESPIRATORY SYSTEM LECTURE 5 DR HEYAM AWAD FRCPATH RESTRICTIVE, INTERSTITIAL LUNG DISESAES. FIROSING DISESES. GRANULOMATOUS DISEASES. EOSINOPHILIC. SMOKING RELATED. FIBROSING DISEASES
DISEASES OF THE RESPIRATORY SYSTEM LECTURE 5 DR HEYAM AWAD FRCPATH RESTRICTIVE, INTERSTITIAL LUNG DISESAES. FIROSING DISESES. GRANULOMATOUS DISEASES. EOSINOPHILIC. SMOKING RELATED. FIBROSING DISEASES
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Lung Cancer Case Study
 Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
YOUR LUNG CANCER PATHOLOGY REPORT
 UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
Interstitial Lung Diseases(ILD) By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun
 By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun") Interstitial Lung Diseases(ILD) By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun. 26.11.11 Introduction Interstitial Lung Diseases (ILD) are group of diseases that affect the interstitium of the lungs,
Interstitial Lung Diseases(ILD) By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun. 26.11.11 Introduction Interstitial Lung Diseases (ILD) are group of diseases that affect the interstitium of the lungs,
What is lung cancer? Contents
 13 11 20 Information and support What is lung cancer? Contents About the lungs What is lung cancer? How common is it? Different types of lung cancer Causes Symptoms Information reviewed by About the lungs
13 11 20 Information and support What is lung cancer? Contents About the lungs What is lung cancer? How common is it? Different types of lung cancer Causes Symptoms Information reviewed by About the lungs
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
SCPA502-Respiratory Pathology
 Problem Mr. B is 57 years old, high 157 cm and weight 76 kg. He has worked as the dump truck driver in the coal mine since 1980, and also smoked cigarette 1 pack/day more than 30 years. What are the risk
Problem Mr. B is 57 years old, high 157 cm and weight 76 kg. He has worked as the dump truck driver in the coal mine since 1980, and also smoked cigarette 1 pack/day more than 30 years. What are the risk
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
CELL-MEDIATED IMMUNITY
 LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
LECTURE #4 1 LYMPHATIC SYSTEM 2 CELL-MEDIATED IMMUNITY T-lymphocytes (activated in the thymus) identify aggressors and try to destroy them through the production of lymphokines (synthesized proteins) Killer
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Cancer in the United States, 2007
 Cancer in the United States, 2007 Lung Cancer in the United States Annual Cancer Deaths Five-Year Survival 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast The
Cancer in the United States, 2007 Lung Cancer in the United States Annual Cancer Deaths Five-Year Survival 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast The
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Renal tumors of adults
 Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Renal tumors of adults Urinary Tract Tumors 2%-3% of all cancers in adults. The most common malignant tumor of the kidney is renal cell carcinoma. Tumors of the lower urinary tract are twice as common
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Pulmonary Diseases. We Move A Lot of Air. Basic Categories. Alveolar Level. Developmental
 Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
LUNG CANCER. Agnieszka Słowik, MD. Department of Oncology, University Hospital in Cracow Jagiellonian University
 LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Lec #2 histology. Bronchioles:
 Lec #2 histology. Last lecture we talked about the upper respiratory tract histology, this one is about the lower part histology. We will discuss the histology of: -bronchioles -respiratory bronchioles
Lec #2 histology. Last lecture we talked about the upper respiratory tract histology, this one is about the lower part histology. We will discuss the histology of: -bronchioles -respiratory bronchioles
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013
 Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013 Overview Radiography Computed Tomography Magnetic Resonance Imaging Nuclear Imaging Show All Multimedia Library References Overview For patients with
Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013 Overview Radiography Computed Tomography Magnetic Resonance Imaging Nuclear Imaging Show All Multimedia Library References Overview For patients with
Common things are common, but not always the answer
 Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
PDF created with pdffactory Pro trial version
 Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Sarcoidosis. Sarcoidosis Care at National Jewish Health. Causes
 Sarcoidosis Sarcoidosis is a chronic disease that can affect any organ in the body, but most commonly affects the lungs. Very small (microscopic) clusters of inflammation or white cells, called granulomas,
Sarcoidosis Sarcoidosis is a chronic disease that can affect any organ in the body, but most commonly affects the lungs. Very small (microscopic) clusters of inflammation or white cells, called granulomas,
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Molecular Pathobiology of Lung Cancer. William K. Funkhouser, MD PhD Department of Pathology and Lab Medicine University of North Carolina
 Molecular Pathobiology of Lung Cancer William K. Funkhouser, MD PhD Department of Pathology and Lab Medicine University of North Carolina Outline Lung Anatomy Lung Carcinoma Classification & Morphology
Molecular Pathobiology of Lung Cancer William K. Funkhouser, MD PhD Department of Pathology and Lab Medicine University of North Carolina Outline Lung Anatomy Lung Carcinoma Classification & Morphology
Master Class: Fundamentals of Lung Cancer
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this