ACUTE STROKE. Internal Medicine Lecture July 17, 2018
|
|
|
- Stewart Rogers
- 5 years ago
- Views:
Transcription
1 ACUTE STROKE Internal Medicine Lecture July 17, 2018 Lauren E. Fournier, MD Vascular Neurology Fellow at UTHealth Slides adapted courtesy of Dr. Anjail Sharrief
2 OBJECTIVES Residents will be able to discuss epidemiology and risk factors for ischemic and hemorrhagic stroke. Residents will be able to recognize acute stroke symptoms and have an understanding of the NIHSS. Residents will be able to identify the different stroke subtypes and comment on management differences.
3 Epidemiology of Stroke Stroke is the 2 nd leading cause of death in the world Stroke is the 4 th leading cause of death in the United States Stroke is a leading cause of adult disability Approximately 800,000 strokes occur each year Every 40 seconds, someone has a stroke in US Every 4 minutes, someone dies of a stroke in the US Roger VL et al. Circulation 2014
4 The Economic Impact Direct and indirect costs of 34.3 billion dollars Direct costs 18.8 billion dollars Average lifetime cost of ischemic stroke is $140,000 per person Per capita cost of stroke estimates highest in African Americans Largest component loss of earnings Roger VL et al. Circulation 2014
5 Types of Stroke Ischemic (87%) Extracranial Atherosclerosis Intracranial Atherosclerosis Cardioembolic Small Vessel Disease Other Hemorrhagic - Intracerebral (10%) Subarachnoid Hemorrhage (3%) Roger VL et al. Circulation 2014
6 Transient Ischemic Attack In the past, defined as focal cerebral ischemic event with symptoms lasting < 24 hours Newer proposed definition (2002) Brief episode of neurological dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than one hour, and without evidence of acute infarction 15% of strokes are preceded by TIA Between 2-10% of patients with TIA will have a stroke within 2 days, up to 17% will have a stroke at 3 months Use of terminology mini stroke may minimize the importance of rapid evaluation and management of TIA events Easton et al, Stroke. 2009;40:
7 Risk Factors for Ischemic Stroke MODIFIABLE Hypertension Tobacco Use Diabetes Dyslipidemia Coronary Artery Disease Atrial fibrillation Obstructive Sleep Apnea Substance abuse OCP/Hormone Use NON-MODIFIABLE Age Gender Race / Ethnicity Genetic predisposition Hypercoagulable states Malignancy
8 Risk Factors for Hemorrhagic Stroke Age, Race/ ethnicity, Gender HYPERTENSION Vascular abnormality Arteriovenous malformation, arteriovenous fistula, aneurysm, cavernous malformation Coagulopathy Iatrogenic: anticoagulation, chemotherapy Other: liver disease, renal disease, etc Drugs of abuse (cocaine, amphetamines, etc) Trauma Cerebral Venous Sinus Thrombosis
9 Signs and Symptoms Anterior Circulation Aphasia difficulty with language Neglect / inattention Visual field cut Monocular vision loss Hemiparesis Face, arm, leg on same side Hemisensory loss Face, arm, leg on same side Dysarthria difficulty with speech Posterior Circulation Vertigo Ataxia Double vision Dysarthria Visual field cut Hemiparesis and hemisensory loss Facial involvement may be contralateral to arm and leg weakness/ sensory loss
10 NIHSS 1a. Level of consciousness 1b. LOC Questions: - The current month? - Age? 1c. LOC Commands: - Open and close the eyes. - Grip and release nonparetic hand. Scoring 0 = Alert; keenly responsive. 1 = Not alert; but arousable by minor stimulation to obey, answer, or respond. 2 = Not alert; requires repeated stimulation to attend, or is obtunded and requires strong or painful stimulation to make movements (not stereotyped). 3 = Responds only with reflex motor or autonomic effects or totally unresponsive, flaccid, and areflexic. 0 = Answers both questions correctly. 1 = Answers one question correctly. 2 = Answers neither question correctly. 0 = Performs both tasks correctly. 1 = Performs one task correctly. 2 = Performs neither task correctly.
11 NIHSS Scoring 2. Best Gaze 0 = Normal. 1 = Partial gaze palsy; gaze is abnormal in one or both eyes, but forced deviation or total gaze paresis is not present. 2 = Forced deviation, or total gaze paresis not overcome by the oculocephalic maneuver. 3. Visual 0 = No visual loss. 1 = Partial hemianopia. 2 = Complete hemianopia. 3 = Bilateral hemianopia (blind including cortical blindness).
12 NIHSS Scoring 4. Facial Palsy 0 = Normal symmetrical movements. 1 = Minor paralysis (flattened nasolabial fold, asymmetry on smiling). 2 = Partial paralysis (total or near-total paralysis of lower face). 3 = Complete paralysis of one or both sides (absence of facial movement in the upper and lower face).
13 NIHSS 5a. Motor Left Arm 5b. Motor Right Arm 0 = No drift; limb holds 90 (or 45) degrees for full 10 seconds. 1 = Drift; limb holds 90 (or 45) degrees, but drifts down before full 10 seconds; does not hit bed or other support. 2 = Some effort against gravity; limb cannot get to or maintain (if cued) 90 (or 45) degrees, drifts down to bed, but has some effort against gravity. 3 = No effort against gravity; limb falls. 4 = No movement. UN = Amputation or joint fusion, explain:
14 NIHSS 6a. Motor Left Leg 6b. Motor Right Leg 7. Limb Ataxia - Finger-nose-finger - Heel-shin 0 = No drift; leg holds 30-degree position for full 5 seconds. 1 = Drift; leg falls by the end of the 5- second period but does not hit bed. 2 = Some effort against gravity; leg falls to bed by 5 seconds, but has some effort against gravity. 3 = No effort against gravity; leg falls to bed immediately. 4 = No movement. UN = Amputation or joint fusion, explain: 0 = Absent. 1 = Present in one limb. 2 = Present in two limbs. UN = Amputation or joint fusion, explain:
15 NIHSS 8. Sensory 0 = Normal; no sensory loss. 1 = Mild-to-moderate sensory loss; patient feels pinprick is less sharp or is dull on the affected side; or there is a loss of superficial pain with pinprick, but patient is aware of being touched. 2 = Severe to total sensory loss; patient is not aware of being touched in the face, arm, and leg.
16 NIHSS 9. Best Language 0 = No aphasia; normal. 1 = Mild-to-moderate aphasia; some obvious loss of fluency or facility of comprehension, without significant limitation on ideas expressed or form of expression. Reduction of speech and/or comprehension, however, makes conversation about provided materials difficult or impossible. For example, in conversation about provided materials, examiner can identify picture or naming card content from patient s response. 2 = Severe aphasia; all communication is through fragmentary expression; great need for inference, questioning, and guessing by the listener. Range of information that can be exchanged is limited; listener carries burden of communication. Examiner cannot identify materials provided from patient response. 3 = Mute, global aphasia; no usable speech or auditory comprehension.
17 NIHSS 10. Dysarthria 0 = Normal. 1 = Mild-to-moderate dysarthria; patient slurs at least some words and, at worst, can be understood with some difficulty. 2 = Severe dysarthria; patient's speech is so slurred as to be unintelligible in the absence of or out of proportion to any dysphasia, or is mute/anarthric. UN = Intubated or other physical barrier, explain: 11. Extinction and Inattention (formerly Neglect) 0 = No abnormality. 1 = Visual, tactile, auditory, spatial, or personal inattention or extinction to bilateral simultaneous stimulation in one of the sensory modalities. 2 = Profound hemi-inattention or extinction to more than one modality; does not recognize own hand or orients to only one side of space.
18 NIHSS
19 NIHSS
20 NIHSS Tools
21 ISCHEMIC STROKE SUBTYPES More than the Basics

22 Extracranial Atherosclerotic Disease Involves carotid or vertebral arteries Stroke Mechanism Artery to artery embolism Acute occlusion of artery from plaque rupture Reduced cerebral perfusion/ flow-related Variable clinical presentation MRI of a 72 yo man with hypertension, tobacco use, internal carotid artery stenosis, carotid bruit, presenting with right-sided weakness and aphasia Furie et al, Stroke. 2011;42:

23 Small Vessel Disease Cause of small subcortical or lacunar strokes Mechanism of stroke Occlusion of small deep penetrating end-arteries Related to lipohyalinosis and microatheroma formation May have classic presentation Pure motor / hemiparesis Pure sensory stroke Ataxic hemipareis Dysarthria/ clumsy hand Mixed sensory/ motor 55 year old woman with hypertension and diabetes presenting with right arm and leg weakness Furie et al, Stroke. 2011;42:

24 Intracranial Atherosclerosis Atherosclerosis in major intracranial vessels Includes internal carotid, middle cerebral, vertebral, basilar, etc Mechanism of Stroke Artery to artery embolism Decreased perfusion related to limitation of flow Acute plaque rupture and vessel occlusion Variable clinical presentation 57 year old man with hypertension and poorly controlled diabetes, p/w left facial weakness, dysarthria, unsteadiness, with vertebral and basilar artery atherosclerosis



25 Cardioembolic Stroke Source - Atrial fibrillation - MI related left ventricular thrombus - Cardiomyopathy - Right to left shunt - Thrombus formation on native or prosthetic valve - Endocarditis - Aortic arch disease - Infarct appearance - Multiple vascular territories - Single vascular territory Furie et al, Stroke. 2011;42:
26 Other Causes: Hypercoagulabe States May be associated with embolic appearing stroke or stroke in young Antiphosholipid antibodies Inherited Thrombophilias Factor V Leiden mutation, prothrombin gene mutation, others Malignancy Pregnancy Carotid or vertebral artery dissection Cerebral venous sinus thrombosis Sickle Cell Disease Infectious or Inflammatory vasculopathies Autoimmune conditions with our without vasculitis Sjogren s syndrome, Lupus Furie et al, Stroke, 2011
27 INPATIENT MANAGEMENT Ischemic Stroke
28 Code Stroke at Memorial Hermann Acute onset of stroke symptoms in your patient Dial or the operator to activate a Code Stroke At the bedside, establish time of last seen normal with the help of nursing staff Gather other pertinent information, like medication list, kidney function, coagulation studies Stroke team will arrive to assess the patient Stroke team consists of a fellow, senior resident and junior resident, sometimes medical students
29 Code Stroke at LBJ Acute onset of symptoms in your patient Activate a rapid response first AND Code Stroke by calling Give a call back number for the neurology resident to reach you The rapid response team will come to the bedside, including the attending or hospitalist (if after hours) and charge nurse The on-call neurology resident will return your page, but is not always in-house
30 Acute Treatment INTRAVENOUS TPA Proven effective treatment of ischemic stroke up to 4.5 hours after onset of symptoms There are additional contraindications for the 3 to 4.5 hour time window Patients receiving tpa have increased likelihood of having minimal or no disability at 3 months Despite efficacy, fewer than 5% of individuals with ischemic stroke receive tpa. Many patients present out of the time window. Jauch et al, Stroke 2013
31 Acute Treatment INTRAVENOUS TPA tpa Exclusion Criteria: SBP >185 mmhg or DBP >110 mmhg Stroke/head trauma in previous 3 months Symptoms suggest SAH Recent intracranial or intraspinal surgery Previous intracranial hemorrhage Intracranial neoplasm, AVM or aneurysm INR >1.7 aptt >40 sec Platelet count <100K Use of oral anticoagulant direct thrombin inhibitors or direct factor Xa inhibitors Serum glucose <50 Active bleeding or acute trauma Non-compressive arterial puncture in last 7 days Demaerschalk et al, 2015
32 Acute Treatment INTRAVENOUS TPA tpa Relative Exclusion Criteria: Only minor or rapidly improving stroke symptoms Pregnancy Seizure at onset with postictal residual neurological impairments Major surgery or serious trauma within previous 14 days Recent GI or urinary tract hemorrhage in previous 21 days Recent MI within previous 3 months Demaerschalk et al, 2015
33 Acute Treatment MECHANICAL THROMBECTOMY Several RCTs have demonstrated efficacy of mechanical thrombectomy with stent retrievers at improving 90 day outcomes Intra-arterial thrombectomy (IAT) should be considered for all patients presenting with acute ischemic stroke and large vessel occlusion within 6 hours of symptom onset After two recent studies (DAWN and DEFUSE-3), IAT should also be considered when last seen normal is 6 24 hours in carefully selected patients All patients who are eligible should also receive tpa within the 4.5 hours time window Powers et al, Stroke 2018
34 Initial Evaluation and Management CT head when patient arrives to ED or as soon as possible inpatient Rule out hemorrhage Changes from ischemic stroke may not be evident for several hours Blood vessel imaging CTA head and neck MRA head and neck (usually with MRI brain) Carotid doppler/ TCD if renal function precludes above Determine eligibility for tpa and IAT Call stroke and endovascular teams Blood pressure management Control BP < 185/110 with IV medication prior to tpa administration Permissive hypertension (220/100) if not administering tpa Jauch et al, Stroke 2013
35 Evaluation and Management MRI brain Determine extent and pattern of infarct Better evaluate prior ischemic / hemorrhagic insults Laboratory Studies Fasting lipid panel, HgbA1c TSH / Free T4 if atrial fibrillation Hypercoagulable / inflammatory studies in select patients Cardiac Studies Cardiac monitoring (at minimum 24 hours) for atrial fibrillation Transthoracic ECHO with bubble to assess for PFO Transesophageal ECHO if TTE negative for select patients Jauch et al, Stroke 2013
36 Medications Antiplatelets aspirin, clopidogrel, aspirin-dipyridamole Held for 24 hours post-tpa Anticoagulation Typically held for one to two weeks after stroke Initiated in the hospital for certain conditions High-intensity statin therapy Atorvastatin 40-80mg Rosuvastatin 20-40mg Long-acting anti-hypertensives Initiation at 24 hours BP reduction may be delayed in certain patients Jauch et al, Stroke 2013
37 Rehabilitation Physical therapy and Occupational Therapy Evaluation Evaluate inpatient and long-term therapy needs Speech/ Language evaluation Evaluation of swallowing function Evaluation of aphasia Evaluation of cognitive deficits Determine inpatient and long-term therapy needs Neurorehabilitation evaluation Physician specialist may be needed to help determine therapy needs
38 Recovery Curve Percent Recovery Months Very Good Pre- Morbid Fair/Poor Pre- Morbid
39 Discharge Disposition Inpatient rehabilitation Skilled nursing facility Home with Home Therapy Home with Outpatient Therapy Home without therapy needs Additional Workup May be sent with 30 day monitor to assess for paroxysmal atrial fibrillation if etiology not determined
40 INPATIENT MANAGEMENT Hemorrhagic Stroke
41 Initial Evaluation and Management Airway/Breathing/Circulation CT head Blood pressure management Control Blood Pressure: SBP < 140 mmhg Reverse Coagulopathy Platelets for thrombocytopenia Prothrombin complex concentrate/vitamin K for Warfarin related ICH Prothrombin complex concentrate/dabigatran antidote for NOAC related ICH Laboratory Studies CBC, CMP, Coags, Urine Toxicology Hemphill et al, Stroke 2015
42 Evaluation and Management Neurosurgery Consultation External Ventricular Drain Clot evacuation/ Decompression Aneurysm clipping or coiling AVM embolization or resection Blood vessel imaging CTA head / MRA head CTV head (sinus thrombosis) Other Studies MRI Brain for selected patients Cerebral Angiogram Jauch et al, Stroke 2013
43 CASES
44 Case 1 Patient is a 55 year old man with PMH of smoking and alcohol abuse and has not seen a physician in over 10 years who presented with right face, arm, and leg numbness. NIHSS is 2 (for sensory changes and mild dysarthria) on presentation. He was last seen normal 6 hours ago. Initial CT brain is negative. Blood pressure is 196/85, HR is 75. What do you do next?
45 Case 1 He did not receive tpa because he was out of window. His NIHSS is also very low. He is given an aspirin on admission. Blood pressure remains in 180 s-190 s systolic. He is found to have a small left thalamic ischemic infarct on MRI. CTA of the head and neck shows mild atherosclerotic disease. What other work up do you need?
46 Case 1 Transthoracic echocardiogram shows EF 60-65%, moderate LVH, no PFO. LDL is 110, HgbA1c is 5.0. He is evaluated by physical therapy and occupational therapy and cleared for discharge home independently. What medications would you start him on? You discharge him with aspirin, atorvastatin 80 mg daily, and Lisinopril for his hypertension. You counsel him on smoking cessation.
47 Case 1 Stroke etiology? Likely small vessel disease.
48 Case 2 Patient is a 65 year old man with history of HTN who presents with acute onset aphasia and right hemiparesis. He was last seen normal within 3 hours of symptom onset. NIHSS on initial evaluation is 12 (facial droop - 1, dysarthria -1, right sided paresis - 7, aphasia - 1, sensory - 1). Blood pressure is 175/85, HR is 80. The patient has no exclusions for tpa therapy. Head CT is negative for hemorrhage, and he receives IV tpa. CTA shows proximal left M1 (middle cerebral artery) occlusion so he goes for IA thrombectomy.

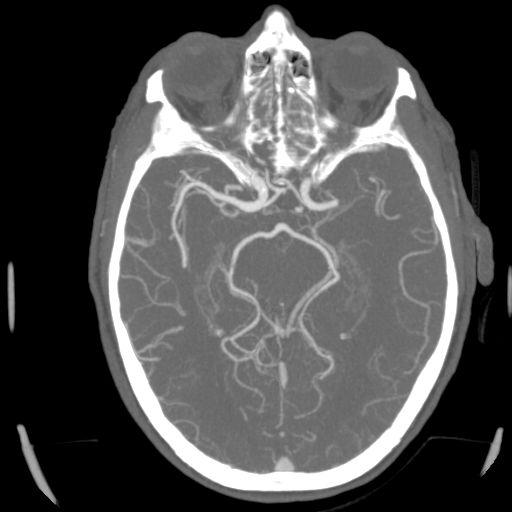
49 Case 2 CT CTA

50 Case 2 IAT is successful, and symptoms improve rapidly to NIHSS 2. MRI shows embolic appearing stroke in left MCA distribution as well as small stroke in right MCA distribution. What is the next important work up for this patient? What are you concerned about? He undergoes further hospital workup: - Cardiac Telemetry (48 hours) - TTE and TEE EF is 55%, no PFO, no thrombus, but LA is enlarged - Lipid panel shows LDL is HgbA1c is 5.9 He is discharged home on aspirin, atorvastatin 80 mg, lisinopril 20mg.
51 Case 2 He presents to clinic for follow-up 2 weeks after discharge. He inquires about further testing. What do you recommend?
52 Case 2 You order event monitor and the following week, you are notified that he has atrial fibrillation. His CHADS2Vasc Score is 4, suggesting > 4% risk of stroke per year. What is your next step in management? A. Continue aspirin since it is early to start anticoagulation B. Repeat CT and start anticoagulation if no hemorrhage C. Start anticoagulation now
53 Case 2 Stroke etiology? Cardioembolic.
54 Questions? Thank you for your attention!
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health
 what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
ED Stroke Panel Page 1 of 2
 ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Patient Care Orders for CODE STROKE: alteplase Administration order set for Acute Ischemic Stroke less than 4.5 hours
 Allergy Alert: NO YES (Refer to Care-Area Administrative Data Screen in MEDITECH) Orders: The prescriber must check the tick box or complete the blank to activate the order. Any changes to be initialled
Allergy Alert: NO YES (Refer to Care-Area Administrative Data Screen in MEDITECH) Orders: The prescriber must check the tick box or complete the blank to activate the order. Any changes to be initialled
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
SARASOTA MEMORIAL HOSPITAL. NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH STROKE SCALE (neu04) Nursing
 Nursing") SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH Nursing DATE: REVIEWED: PAGES: PS1094 7/01 3/18 1 of 5 RESPONSIBILITY: RN, LPN PURPOSE: OBJECTIVE: DEFINITION:
SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE NATIONAL INSTITUTE OF HEALTH Nursing DATE: REVIEWED: PAGES: PS1094 7/01 3/18 1 of 5 RESPONSIBILITY: RN, LPN PURPOSE: OBJECTIVE: DEFINITION:
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Case. Learning objectives. NIHSS values. Presenter Disclosure Information
 1:30 2:30 pm Primary Care of the Stroke Patient SPEAKER Thomas P. Bleck MD, MCCM, FNCS Presenter Disclosure Information The following relationships exist related to this presentation: Thomas P. Bleck,
1:30 2:30 pm Primary Care of the Stroke Patient SPEAKER Thomas P. Bleck MD, MCCM, FNCS Presenter Disclosure Information The following relationships exist related to this presentation: Thomas P. Bleck,
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Stroke Oxygen Study Randomisation Form
 Identification sticker or Name Sex DOB male / female Unit No /Hiss No DD MM YYYY Stroke Oxygen Study Randomisation Form Trial Centre name Investigator name STEP ELIGIBILITY FOR TRIAL INCLUSION Time since
Identification sticker or Name Sex DOB male / female Unit No /Hiss No DD MM YYYY Stroke Oxygen Study Randomisation Form Trial Centre name Investigator name STEP ELIGIBILITY FOR TRIAL INCLUSION Time since
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
GERIATRICS CASE PRESENTATION
 GERIATRICS CASE PRESENTATION CASE 79 year old Patient X was admitted to hospital with SOB. He had a hx of sarcoidosis and asbestosis. Home oxygen requirement is 3-3.5litre. He was admitted, given ceftriaxone
GERIATRICS CASE PRESENTATION CASE 79 year old Patient X was admitted to hospital with SOB. He had a hx of sarcoidosis and asbestosis. Home oxygen requirement is 3-3.5litre. He was admitted, given ceftriaxone
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
PATIENT S NOTES History and Physical Brain Attack Stroke
 UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL The following is a list of variables and how to complete each one:
 MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
MD SUBTYPE ADJUDICATION VARIABLE DEFINITIONS MANUAL 2014-15 The following is a list of variables and how to complete each one: (PHY-1) Case, per physician review: The most important task for the physicians
Acute Ischemic Stroke Mechanism, Diagnosis, Treatment
 Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine Objectives Better understanding of stroke mechanisms
Acute Ischemic Stroke Mechanism, Diagnosis, Treatment IM Resident Lecture December 2016 Mohammad Shafie, MD PhD MEng Department of Neurology UC Irvine Objectives Better understanding of stroke mechanisms
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care
 Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
As seen in Cath Lab Digest In the Unlikely Event: Optimal Care Strategies for Stroke in the Cath Lab
 By Mona Steinbeiser As seen in Cath Lab Digest In the Unlikely Event: Optimal Care Strategies for Stroke in the Cath Lab As a result of advanced technology and science, stroke is now the fifth-leading
By Mona Steinbeiser As seen in Cath Lab Digest In the Unlikely Event: Optimal Care Strategies for Stroke in the Cath Lab As a result of advanced technology and science, stroke is now the fifth-leading
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
Call the Transfer Line at (216)
") Stroke & Cerebrovascular Center To access the Stroke Team at Case Medical Center 24/7 for patient transfers or urgent advice, Call the Transfer Line at (216) 844-1111 Atherosclerotic Plaque: Ischemic Stroke:
Stroke & Cerebrovascular Center To access the Stroke Team at Case Medical Center 24/7 for patient transfers or urgent advice, Call the Transfer Line at (216) 844-1111 Atherosclerotic Plaque: Ischemic Stroke:
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic