Define Shock, mostly as it relates to bleeding Options and evidence for tools of resuscitation Understand a little about coagulation and coagulopathy
|
|
|
- Imogene Carroll
- 5 years ago
- Views:
Transcription

1


2 Define Shock, mostly as it relates to bleeding Options and evidence for tools of resuscitation Understand a little about coagulation and coagulopathy 1:1:1 New advances
3 Reduced perfusion of vital organs leading to inadequate oxygen and nutrients necessary for normal tissue and cellular function. (1,5) Cellular level: Reduction of mitochondrial oxygen Anaerobic glycolysis of ATP Accumulation of pyruvate Lactic Acidosis
4 MAP = 75 MAP = 55
5 MAP = 75 MAP = 55
6 Base Deficit % Mortality Normal 6 Mild 11 Moderate (+ 0-15) (+ 0-20) 53 <
7 Shock Le Dran, 1731: secousse (jarring) 2 Sparrow : shock 1920 Blalock showed that shock after trauma was due to blood loss 2 Bluntly traumatize dog s legs Increased weight in the legs showed enough blood volume loss to account for the shock.

8
9 Hardaway (Ann Surg 1963) Porcine Model Trauma alone to one thigh produced no mortality. Hemorrhage alone to 40mm hg systolic for 4hrs produced zero mortality. Combined trauma and hemorrhagic shock produced 91% mortality Vietnam Wound Analysis (J. Trauma 1978) Soldiers often died of shock despite being adequate treated with IV fluids and appropriate surgical procedures.
10 Hardaway (1990 Crit Care) Pig Study 60 blows to each thigh Produced 100% mortality within 48hrs Even though normal blood volume was maintained with IV fluids. Pigs died of DIC and ARDS


11 More complicated Trauma + Bleeding + Trauma = DIC & ARDS = DEATH



12 Chest Abdomen Retroperitoneal Muscle compartments Street
13 Class I Class II Class III Class IV Blood loss < 750 cc 0-15% % % >2000cc >40% HR Normal PP Normal BP Normal Normal UOP Normal Normal Decreased Negligible Mental Normal Anxious Confused Lethargic Fluid Crystalloid Crystalloid Crys+blood Crys+blood *ATLS; kg male
14 Wiggers 1950s: Animal models (7,8,9) Blood taken out through a catheter until set blood pressure was reached. Re-Administration of shed blood did not improved morbidity and mortality.
15 Shires 1970s (7,8,9) : Large extracellular fluid deficit was greater than could be attributed to vascular refill alone Only infusion of both shed blood and lactated ringers to replace the ECF deficit showed improved outcome.
16 Third space loss into interstium and tissues 3:1 rule of crystalloid for every 1 ml of blood loss ATLS: 2 liters of crystalloid through large bore IV for early treatment of hemorrhagic shock.
17 Vigorous fluid resuscitation bleeding Hemodilution increased Recurrent Hypotension
18 Injection of a fluid that will increase blood pressure has dangers in itself If the pressure is raised before the surgeon is ready to check any bleeding that might take place, blood that is sorely needed may be lost. Cannon, JAMA 70: , 1919
19 Injection of a fluid that will increase blood pressure has dangers in itself If the pressure is raised before the surgeon is ready to check any bleeding that might take place, blood that is sorely needed may be lost. Cannon, JAMA 70: , 1919
20 Dogma has come under question for uncontrolled hemorrhage. Shires and similar animal models: Controlled hemorrhage (8) Newer animal and human resuscitation studies Uncontrolled hemorrhage Permissive hypotension
21 Bickell (8) Porcine model Aggressive replacement of blood loss with three times the volume of crystalloid Increased hemorrhage and decreased survival. Stern and Kowalenko (19) Pigs bled through femoral catheter and aortotomy Resuscitated to systolic blood pressure of 40, 60, 80mmHg. Most bleeding and highest mortality occurred in the 80mmHg group.
22 Riddez (12) Dog aortotomy 4 resuscitation groups No fluid 1:1 replacement blood loss with LR 2:1 3:1 Aortic blood flow and blood loss increased with the amount of fluid used Highest mortality in no fluid and 3:1 fluid group
23 Riddez (12) Dog aortotomy 4 resuscitation groups No fluid 1:1 replacement blood loss with LR 2:1 3:1 Aortic blood flow and blood loss increased with the amount of fluid used Highest mortality in no fluid and 3:1 fluid group
24 Riddez (12) Dog aortotomy 4 resuscitation groups No fluid --->shock 1:1 replacement blood loss with LR 2:1 3:1 -->Rebleeding Aortic blood flow and blood loss increased with the amount of fluid used Highest mortality in no fluid and 3:1 fluid group
25 Bickell & Mattox (NEJM 1994) Randomized prospective trial of 598 patients with penetrating torso injuries Immediate v delayed resuscitation group Immediate group average of 900ml LR Delayed group 100ml Delayed group Better survival to discharge rate (70% vs. 62% p=0.04) Fewer overall complications.
26 Delaying massive fluid resuscitation until the time of surgery prevents: Exacerbating uncontrolled internal hemorrhage Clot dissolution / popping the clot Dilution of clotting factors Hypothermia
27 Caveats Brain injury CPP=MAP-ICP SBP>100 mmhg Fast evacuation to definitive surgical care Unclear results for non-penetrating trauma Elderly patients



28 Blood Crystalloid Colloid Hypertonic saline

29 Lowery 1971(Surg Gynecol Obstet) Vietnam war study LR v NS Healthy soldiers No difference in outcome

30 Waters 2001 (Aneth Analg) Patients undergoing aortic aneurysm repair NS More volume (~ ml) Hyperchloremic acidosis Dilutional coagulopathy Todd (J. Trauma 2007; 62:636-9) Swine bled via liver injury & resuscitated to MAP 90mmHg NS More volume Hyperchloremic acidosis Dilutional coagulopathy

31 Conclusion No mortality difference LR Lower overall volume More buffering capacity NS Metabolic acidosis Dilutional coagulopathy Preferred fluid outside of US Probably no difference for prehospital or early fluid resuscitation.
32 Advantages Cheap Easy to store and warm Established safety Predictable rise in cardiac output Disadvantages 14 Large volumes needed Dilutional coagulopathy Increase cytokine activation 7 No oxygen carrying capacity May Increase ICP
33 Proposed Benefits (15) Smaller volume Less pulmonary edema Stays in the intravascular space Quicker return to normal hemodynamics Smaller package Antioxidant and anti-inflammatory effects
")
34 Disadvantages (16) Transmission of diseases Increased bleeding Hypersensitivity reactions Renal failure Accumulation Taken up by RES Dose limit (20-50mL/kg) Cost
35 Schierhout and Robertson; BMJ total studies, 7 trauma studies Albumin, dextran, gelatin v Crystalloid Colloids associated with 4% increased risk of mortality Cochrane meta analysis; BMJ trials total; 4 trauma studies (1977, 1978, 1983) Albumin, 23 trials; Hydroxyethyl Starch (HES), 16 trials; Gelitin, 16 trials; Dextran, 9 trials 6% increased mortality Albumin kills our patients (1 out of 17)
36 Wilikes (2001 Ann Int Med) 27 studies: trauma and surgical pts Albumin v crystalloid No effect of albumin on mortality Choi et al.(1999 Crit Care Med) All kinds of colloids v crystalloids No difference in mortality
37 Cochrane Review 2006 As colloids are not associated with improvement in survival, and as they are more expensive than crystalloids, it is hard to see how their continued use can be justified outside the context of RCTs.
38 SAFE trial 2004 (N Engl J Med 2004) Double blind RCT, 7000 pts, 16 ICUs, 18 month period 4% albumin v 0.9% normal saline First 4 days volume albumin to saline (1:1.4) No difference in 2 groups in 28 all day cause mortality Sub group analysis: difference between trauma and sepsis patients RR of death pts with severe sepsis= 0.87 Overall trauma mortality higher for albumin v saline (13.5% v 10%) TBI separated, no difference in mortality SAFE brains study proposed
39 Conclusion Most studies do not show reduction of mortality Possible risk of increased mortality Increased cost Routine use of colloids not supported in Trauma May be beneficial in Septic patients, SBP, ARDS Promise with HES and newer colloids (16) Further RCT trials needed
40 Rapid plasma volume expansion (17) Pull of fluid to vascular space secondary to increased concentration gradient Decreases ICP Potential benefits in TBI patients Military use Weighs less 1 liter NS bag=2744 cm3 in volume and 1.1 kg Storage space for helicopters and ground ambulances
41 Adverse effects Hyperosmolar coma Hypernatremia Seizures arrhythmias Tissue necrosis Allergic reactions
42 Australian prehospital study (JAMA 2004) Double blind prospective RCT, 229 pts SBP<100 Blunt head trauma Excluded polytrauma pts HTS v LR Conclusion Both groups received same volume of fluids No difference in survival, length of stay, neurologic outcome
43 Wade et al; 1997 meta analysis 11 studies Hypertonic saline alone and with dextran v isotonic saline No difference for HS v isotonic saline HSD showed slight improvement in survival Especially with TBI pts and penetrating injuries
44 Cost Compatibility/error 18 Incorrect blood-1:40,000 (death 1:2million) Immune complications 18 1:40,000 Infection 19 Sepsis 1:500,000 (RBCs) 1:50,000 (platelets) Hep B 1:250,000 Hep C & HIV 1:2million Storage requirements Citrate toxicity Hypocalcemia Hyperkalemia
45 Clotting takes time (2-10 minutes in the best of circumstances) Clots are physically weak There is limited clotting material to work with (even in the whole body) 10 grams of fibrinogen total 15 ml of platelets total in normal individuals
.")

46 Ten times more people die from clotting than from bleeding (heart attacks, strokes, pulmonary emboli, etc). Moderate bleeding is an uncommon event, but clotting is a continuous threat. The body evolved to deal with bruising and minor to moderate bleeding.


47 Blood loss (volume) = area x rate x time Area is determined by the extent of initial injury or the need for surgical exposure. Rate of blood loss is a function of the tissues involved and the blood pressure Time of bleeding is a function of the rate of blood loss with subsequent fall in blood pressure, the rate of blood coagulation, and the effect of interventions
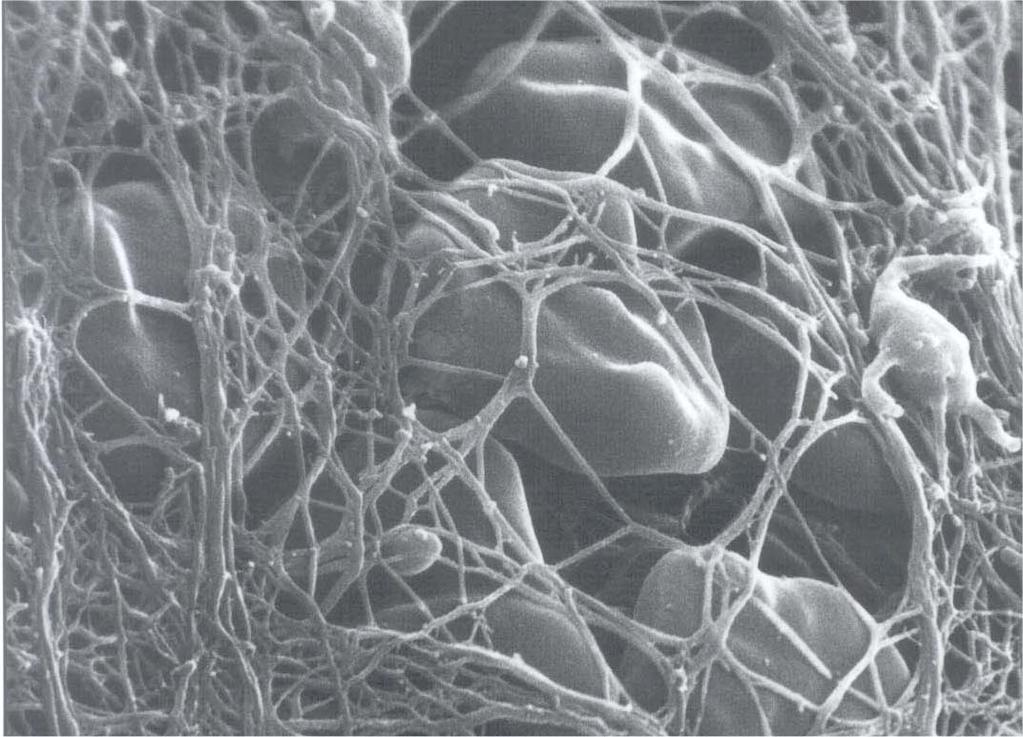
48 CLOT
49 The Classic Coagulation Cascade Intrinsic Pathway tested with the PTT XII XIIa MacFarlane, Nature 1964 Davie & Ratnoff, Science 1964 XI XIa IX IXa (VIIIa) X II Fibrinogen Extrinsic Pathway tested with the PT VIIa VII (TF) Xa (Va) II Fibrin a Common pathway

50 Loss Dilution Hypothermia Acidosis Consumption Fibrinolysis Coagulopathy of Trauma DIC
51 Tissue Injury Inflammation Hemorrhage Loss, Consumption, Dilution COAGULOPATHY Dysfunction Dysfunction Acidosis Genetics Hypothermia Anticoagulants Figure 1. Causes of coagulopathy in trauma patients.

52 J Trauma, Derangements in coagulation occur rapidly after trauma even after adjusting for ISS By the time of arrival at the ED, 1/3 of trauma patients had a coagulopathy associated with a poor outcome

53 J Trauma, 2003.
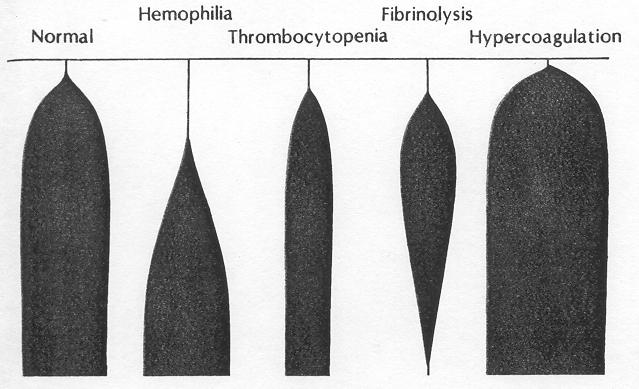
54 Method Wire turns 4.75 back and forth. Clot elasticity but not blood viscosity torque the wire. Normal values R = 6-8 min R + K = min α = >50 MA = mm A 60 = >85% MA
55 TEG can measure hemostasis and fibrinolysis Normal values R = 6-8 min R + K = min α = >50 MA = mm A 60 = >85% MA F = >300 min - F is a measure of the rate of clot lysis
56


57 17 y/o male shot in porta hepatis massive TX in course of damage control surgery TEGs before and after rviia show increased activity in plasma and platelet phases TEG before rviia R = 11 min, a = 12, MA = 12 mm TEG after rviia R = 3.3 min, a = 60, MA = 44 mm

58 A symposium held at the U.S. Army Institute of Surgical Research, May 2005

59 If clinically evident coagulopathy is prevented by the early use of FFP, subsequent blood product consumption is likely to be less. In massive transfusion, early 1:1:1 PRBC : Plasma : platelets are indicated

60 Reviewed massive transfusion protocols from well-developed trauma systems in Denver, Houston, Helsinki, Sydney, and Baltimore. This group then presented a massive transfusion protocol based on the best data from their review. 1:1:1
61 Effect of FFP : RBC Ratio on Overall Mortality in 252 Massively Transfused Trauma Patients (long term outcomes) % Chi Square RB: p=0.006 RG: p<0.001 BG: p=0.034 Mortality % % 20 n=31 n=56 20% 10 n= :22-1:4 1:3.9-1:2.1 1:2-1:0.59 FFP : RBC Ratio 8









62 PRBC Hct 55% 335 ml Plt 5.5x ml FFP 80% 275 ml So Component Therapy Gives You 1U PRBC + 1U PLT + 1U FFP Hct 29% Plt 87K Coag activity 65% 950 mg fibrinogen 500 ml Warm Hct: 38-44% Plt: K Coags: 100% 1000 mg Fibrinogen Armand & Hess, Transfusion Med. Rev., 2003


 1 Unit Plasma (275")


63 Whole blood 500 ml (Hct 38% 50%; Plts 150 K 400 K; Plasma coagulation activity100%) 150 ml anticoagulant added; centrifuged 1 Unit PRBC (335 ml, Hct 55%) 1 Unit Plasma (275 ml, coagulation activity 80%) 1 Unit Platelets (50 ml, 5.5 x plts Patient Receives 650 ml fluid: Hct 29%, Plts 88 K, 65% coagulation activity
64 Act prior to the onset of coagulopathy INR still normal Less than 1 blood volume transfusion Strive to maintain clotting Plasma (uncrossmatched?) Platelets Normothermia Adequate HCT
65 Any fluid which does not clot or carry oxygen should be suspect.


66
67 Is easy to store and use Stops inappropriate hemorrhage Does not clot working vessels Has no side effects Is free

68 $6,800
69 Recombinant human product Facilitates cell-based coagulation, triggering thrombin burst on platelet surface In large doses, requires only Factor I (Fibrinogen), II (Thrombin) and platelets to produce clotting Licensed only for use in hemophiliacs with inhibitors to Factor VIII or IX, or patients with FVIIa deficiency
70

71 Pre PT Post PT Prothrombin Time (sec)
72



73 Off-label use requested by attending physician Gatekeeper approval required Life threatening hemorrhage Coagulopathy Failure of conventional therapy Non-futile Periodic data analysis approved by the IRB Dutton RP et al. J Trauma 57: , 2004
74 100 mcg/kg Shock Rapid bleeding 1.2 mg (smallest possible dose) No shock Slow or no bleeding


75 20% no response (futile) 80% response rate (hemostasis) 50% die Traumatic brain injury (average 5.5 day LOS) Multiple organ system failure (average 32 day LOS) 50% survive to discharge Overall survival about 40% LOS, length of stay. Dutton RP et al. J Trauma. 2004;57:
76 FVIIa is a potent pro-coagulant Thrombotic complications will be highly patient dependant: Unstable atherosclerotic disease Blunt vascular injury (carotid, mesenteric arteries) Extracorporeal circulation Other pro-coagulants? Probably not dose dependant!
77 Looking into hemoglobin substitutes as oxygen carriers. Nothing FDA approved yet Hemostatic dressings, liquids, etc. Suspended animation


78 All bleeding stops Try to stop the bleeding before the heart stops beating Resuscitate before a coagulopathy develops 1:1:1 A little hypotension is a good thing Control the chaos
79 1. Kolecki, P. Hypovolemic Shock; emedicine Mar Hardaway, R. A brief review of traumatic shock leading to a new theory and new treatment. J Applied Research 2003; 3: Mattox, K. Permissive Hypotension. Trauma.org; Bozeman, W. Hemorrhagic Shock. emedicine Jan Colwell, C. Management of shock in adult trauma. Uptodate.com; Jan Udeani, J. Hemorrhagic shock; emedicine Mar Krausz, M. Initial resuscitation of hemorrhagic shock. World J Emerg Surg. 2006; 1:14 8. Revell, M. Fluid resuscitation in prehospital trauma care: a consensus view. Emerg Med J. 2002; 19: Gutierrez, G. Clinical review: Hemorrhagic shock. 10. Kreimeier, U. Permissive hypotension. Schweiz Med. 2000; 130:


80 11. Kowalenko, T. Improved outcome with hypotensive resuscitation of uncontrolled hemorrhagic shock in swine model. J Trauma Sep;3: Bickell, W. Immediate v delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. NEJM 331: Pascoe, S. Management of hypovolemic shock in the trauma patient NSW Inst of Trauma and Inj management Rob, S. Lactated ringers is superior to normal saline in the resuscitation of uncontrolled hemorrhagic shock. J Trauma Cochran review Boldt, J. Fluid Choice for resuscitation of the trauma patient. Can J Anesth :5 17. Svensen, C. Using small volume resuscitation in Sweden: observations from initial experiences. Trans Altern in Transfusion Med :3 18. Shot and Dark 1996, Blood Transfusions. Wekipedia.com
Emergency Blood and Massive Transfusion: The Surgeon s Perspective. Transfusion Medicine Update September 16 17, 2009
 Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
"Small Volume" Resuscitation for Trauma Cases : PRO Aspects
 "Small Volume" Resuscitation for Trauma Cases : PRO Aspects Jim Holliman, M.D., F.A.C.E.P. Program Manager, Afghanistan Health Care Sector Reconstruction Project Center for Disaster and Humanitarian Assistance
"Small Volume" Resuscitation for Trauma Cases : PRO Aspects Jim Holliman, M.D., F.A.C.E.P. Program Manager, Afghanistan Health Care Sector Reconstruction Project Center for Disaster and Humanitarian Assistance
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
The changing face of massive transfusion
 The changing face of massive transfusion HAABB, Kansas City, 18 April 2018 John R. Hess, MD, MPH, FACP, FAAAS Professor of Laboratory Medicine Medical Director, Transfusion Service, Harborview MC U of
The changing face of massive transfusion HAABB, Kansas City, 18 April 2018 John R. Hess, MD, MPH, FACP, FAAAS Professor of Laboratory Medicine Medical Director, Transfusion Service, Harborview MC U of
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Hydroxyethyl starch and bleeding
 Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury
 Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Hemorrhagic Shock in the Pediatric Patient: New Therapies and Practices
 Hemorrhagic Shock in the Pediatric Patient: New Therapies and Practices Richard P. Dutton, M.D., M.B.A. In trauma, as in other subspecialties, randomized controlled trials focused on pediatric patients
Hemorrhagic Shock in the Pediatric Patient: New Therapies and Practices Richard P. Dutton, M.D., M.B.A. In trauma, as in other subspecialties, randomized controlled trials focused on pediatric patients
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
FLUID RESUSCITATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY. Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center
 UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients?
 Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Does a Controlled Fluid Resuscitation Strategy Decrease Mortality in Trauma Patients? death Haemorrhage remains the biggest killer of major trauma patients Expected deaths will increase to 8 million/year
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Pathophysiologie und Therapie bei Massenblutung
 Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Neue Wirkungsmechanismen von Transfusionsplasma
 Neue Wirkungsmechanismen von Transfusionsplasma Lorenzo ALBERIO Médecin chef Hématologie générale et Hémostase Service et Laboratoire centrale d Hématologie CHUV, Lausanne Trauma patient Bleeding Thrombosis
Neue Wirkungsmechanismen von Transfusionsplasma Lorenzo ALBERIO Médecin chef Hématologie générale et Hémostase Service et Laboratoire centrale d Hématologie CHUV, Lausanne Trauma patient Bleeding Thrombosis
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant factor VIIa: Hype or hope? Jed Gorlin MD, MBA
 Recombinant factor VIIa: Hype or hope? Jed Gorlin MD, MBA Goals of presentation Challenge current use of rviia using data Review how rviia works Approved indications Review results of randomized trials
Recombinant factor VIIa: Hype or hope? Jed Gorlin MD, MBA Goals of presentation Challenge current use of rviia using data Review how rviia works Approved indications Review results of randomized trials
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Tactical Combat Casualty Care Guideline Change Fluid Resuscitation for Hemorrhagic Shock in TCCC
 Tactical Combat Casualty Care Guideline Change 14-01 Fluid Resuscitation for Hemorrhagic Shock in TCCC 2 June 2014 Why a change was needed: The last update to the fluid resuscitation recommendations in
Tactical Combat Casualty Care Guideline Change 14-01 Fluid Resuscitation for Hemorrhagic Shock in TCCC 2 June 2014 Why a change was needed: The last update to the fluid resuscitation recommendations in
Introduction to coagulation and laboratory tests
 Introduction to coagulation and laboratory tests Marc Jacquemin Special Haemostasis Laboratory Center for Molecular and Vascular Biology University of Leuven Coagulation in a blood vessel: fibrin stabilises
Introduction to coagulation and laboratory tests Marc Jacquemin Special Haemostasis Laboratory Center for Molecular and Vascular Biology University of Leuven Coagulation in a blood vessel: fibrin stabilises
Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes ~ 100 units Heparin neutralization in ~ 5 min
 Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
True/False: Idarucizumab can be utilized for the management of bleeding associated with dabigatran.
 Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
Resuscitation Update
 Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
INTRAVENOUS FLUIDS. Ahmad AL-zu bi
 INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
4/23/2009. September 15, 2008
 The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
ORIGINAL PAPERS. Fluid Resuscitation in Pre-Hospital Trauma Care: a consensus view
 J R Army Med Corps 2001; 147: 147-152 ORIGINAL PAPERS Consensus Working Group on Pre-hospital fluids representing: Faculty of Pre-Hospital Care Royal College of Surgeons of Edinburgh Faculty of Accident
J R Army Med Corps 2001; 147: 147-152 ORIGINAL PAPERS Consensus Working Group on Pre-hospital fluids representing: Faculty of Pre-Hospital Care Royal College of Surgeons of Edinburgh Faculty of Accident
PUZZLE. EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT?
 PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
Hypotensive Resuscitation in Patients with Ruptured Abdominal Aortic Aneurysm
 Eur J Vasc Endovasc Surg 31, 339 344 (2006) doi:10.1016/j.ejvs.2005.11.003, available online at http://www.sciencedirect.com on REVIEW Hypotensive Resuscitation in Patients with Ruptured Abdominal Aortic
Eur J Vasc Endovasc Surg 31, 339 344 (2006) doi:10.1016/j.ejvs.2005.11.003, available online at http://www.sciencedirect.com on REVIEW Hypotensive Resuscitation in Patients with Ruptured Abdominal Aortic
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Hypotensive Resuscitation
 Curr Anesthesiol Rep (2014) 4:209 215 DOI 10.1007/s40140-014-0064-7 ANESTHESIA FOR TRAUMA (J-F PITTET, SECTION EDITOR) Hypotensive Resuscitation Jeremy B. Smith Jean-Francois Pittet Albert Pierce Published
Curr Anesthesiol Rep (2014) 4:209 215 DOI 10.1007/s40140-014-0064-7 ANESTHESIA FOR TRAUMA (J-F PITTET, SECTION EDITOR) Hypotensive Resuscitation Jeremy B. Smith Jean-Francois Pittet Albert Pierce Published
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials