Pulmonary Pathology II. William Bligh-Glover M.D. Department of Anatomy, CWRU
|
|
|
- Dora Newton
- 5 years ago
- Views:
Transcription

1 Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU
2 Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish the types of lung infection, and comprehend their etiologies, epidemiology, pathogenesis and prognosis Comprehend the etiology, pathogenesis/pathophysiology and consequences of lung abscess
3 Pulmonary Hypertension Defined as at least 25% of systemic pressure; normal is 10% of systemic, due to low resistance of pulmonary vasculature Hypertension usually due to structural diseases causing increased pulmonary blood flow or pressure, increased pulmonary vascular resistance or left heart resistance Note: pulmonary atherosclerosis implies there is pulmonary hypertension
4 Pulmonary Hypertension Emphysema Hypoxia and alveolar destruction reduce the number of capillaries, causing increased arterial resistance, Congenital heart disease Elevated pressures due to valvular disease Recurrent PE Reduced area of vascular bed with consistent pressures VOD Fenfluramine/phenterimine Idiopathic Decreased production of nitric oxide and prostacyclin and increased levels of endothelin, leading to endothelial cell activation and thrombogenesis Women 20-40
5 Pulmonary Hypertension Treatment vasodilators, calcium channel blockers, nitric oxide, anti-thrombotic medications Consequences Right heart hypertrophy (Cor pulmonale) Dyspnea Pneumonia

6 Recurrent PE

7 Plexiform Lesions

8 Cor Pulmonale Cartoon

9 Cor Pulmonale Gross
10 Pulmonary Hypertension Consequences of pulmonary hypertension Pulmonary atherosclerosis Recurrent thromboemboli Intimal thickening Plexiform lesions Reversible/Irreversible Reversible if arterial lesions restricted to medial hypertrophy, intimal thickening of longitudinal smooth muscle or cellular intimal proliferation Irreversible if moderate/severe concentric laminar intimal fibrosis, fibrinoid necrosis, plexiform lesions
11 Non-Infectious Diseases Leading to Pulmonary Hypertension Acute Interstitial Pneumonia (AIP) Bronchiolitis Obliterans Organizing Pneumonia (BOOP) Desquamative Interstitial Pneumonia (DIP) Usual Interstitial Pneumonia (UIP)
12 Acute Interstitial Pneumonia Also called Hamman-Rich syndrome Rapidly progressive disease with no identifiable cause; death usually within 2 months Young adults with influenza-like illness followed by shortness of breath Micro: resembles diffuse alveolar damage with brisk interstitial fibroblastic proliferation
13 Bronchiolitis Obliterans-Organizing Pneumonia Common response to infectious or inflammatory injury to lungs Also associated with drugs, collagen vascular disease, graft versus host disease in bone marrow transplant patients Cause cannot be determined from biopsy - requires clinical history Acute onset with cough, shortness of breath, fever and malaise Excellent prognosis; steroid resistance may lead to death
14 Desquamative Interstitial Pneumonitis Usually adults with insidious onset of shortness of breath, progressing to respiratory insufficiency; also cough, cyanosis, clubbing Cause unknown Mean survival 12 years, mortality 28% 90% are current or past cigarette smokers Associated with collagen vascular disease, positive ANA (similar to UIP) Treatment: steroids (respond better than UIP)
15 Usual Interstitial Pneumonitis Most common pattern of idiopathic pulmonary fibrosis Usually ages % have unknown cause with insidious onset (exertional dyspnea) and chronic evolution; complications include secondary pulmonary hypertension, cor pulmonale, cardiac failure Reduced diffusing capacity is mainly due to ventilationperfusion mismatch from ventilation of lung tissue with capillary destruction and perfusion of under ventilated alveoli Treatment: steroids (20% improve) Mean survival 6 years, mortality 66%
16 Pulmonary Infections Bacterial Pneumococcus Mycobacterial CF Aspiration Viral Mycoplasma Fungal
17 Pneumonia Old Man s Friend Final common pathway Lung is #1 site for infections that cause lost workdays Impairment of defense mechanisms or host resistance Normal defense mechanisms: Nasal clearance (sneezing, blowing, swallowing) Mucociliary elevator (smoking) Alveolar clearance (alveolar macrophages) Host resistance Age Intoxication Other diseases Bronchopneumonia vs. Lobar pneumonia Bronchopneumonia Patchy consolidation of the lung centered on bronchi Neutrophils in bronchi, bronchioles and adjacent alveolar spaces Lobar pneumonia Consolidation of entire lung Rare because of antibiotics Vulnerable patients Old Young Drunks Congestion, red hepatization, grey hepatization, resolution
18 Pneumococcus (Streptococcus pneumoniae) Gram positive, capsulated, lancet-shaped diplococcus Respiratory flora Pneumonia, Otitis media, Meningitis

19 Bronchopneumonia Gross

20 Bronchopneumonia Low Micro

21 Bronchopneumonia High Micro

22 Lobar Pneumonia

23 Pneumococcus
24 Final Common Pathway Old Man s Friend Impairment Viral pneumonia Breaking hip
25 Tuberculosis A.K.A. Consumption, commonest infectious COD in Operas Mycobacteria tuberculosis Mycobacteria bovis Lung involvement is the major cause of morbidity/mortality Rarely involves skin, oropharynx, lymphoid tissue Pott s disease (TB of spine) Prosector s wart (TB of hand) Suppressed by cell mediated immunity, therefore Cases increasing due to AIDS There have been emergence of multiple-drug resistant strains Impaired patients not completing a course of antibiotics Treated with months of antibiotics (INH, Rifampin) Streptomycin in the early days
26 Mycobacterium tuberculosis Acid-fast, slow growing bacillus Aerobe Two organisms M. tuberculosis M. bovis
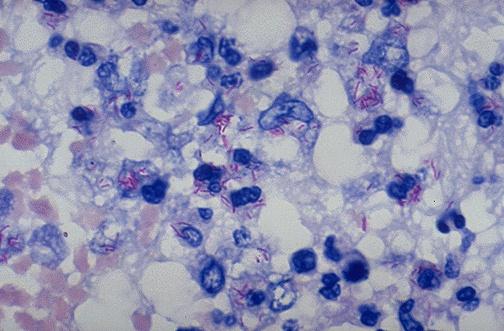
27 Mycobacterium tuberculosis
28 Gohn Complex Gohn complex Parenchymal coin lesion Subpleural Near upper/lower lobe interlobar fissure High oxygen tension) Caseous lymph nodes Resolution Fibrosis Calcification Asymptomatic

29 Gohn Complex
30 Reactivation (Secondary) TB 5-10% of cases of primary infection Produces more damage than primary TB Apical areas of consolidation with caseous necrosis in draining nodes Usually get progressive fibrous encapsulation, which causes focal pleural adhesions, may contain anthracotic pigment Tubercles coalesce over time, creating confluent area of consolidation

31 TB Granuloma

32 TB Granuloma High Power

33 Saranac Lake
34 La Boheme
35 Miliary TB Not Military TB Looks like lung is shot through with millet seeds Progressive spread in compromised individuals

36 Miliary TB
37 Viral Pneumonia Influenza Parainfluenza Adenovirus Respiratory syncytial virus Children Cytomegalovirus, Herpes Immunocompromised

38 Viral Pneumonia Micro

39 RSV Cytopathic Effect
40 Mycoplasma Atypical pneumonia Walking pneumonia Interstitial pneumonia, bronchopneumonia Often asymptomatic Cold agglutinins present in 50% of cases Anti-I IgM
41 Fungal Pneumonia Aspergillus niger Pneumocystis carinii Histoplasma capsulatum
42 Aspergillus niger Colonization of abscess cavity Colonization of tuberculoma Invasive aspergillosis Immunocompromised AIDS Transplants Associated with renal transplant recipients

43 Aspergilloma Gross

44 Aspergillus Fungus Ball
45 Aspergillus Micro Vessel tropic fungus Holy-water sprinkler

46 Aspergillus Micro
47 Pneumocystis carinii AIDS defining illness Opportunistic fungus bronchoalveolar lavage, biopsy Most common pneumonia in AIDS patients, CD4 < 200 protein-calorie malnutrition Causes diffuse or patchy pneumonia Little fungi on GMS

48 P. carinii
49 Pulmonary Abscess Causes Sino bronchial infections Dental sepsis Obstruction Bronchiectasis Aspiration Alcoholism Coma Drugs Debilitation 10% of cases are associated with underlying carcinoma Aspiration induced abscesses more common on right side Right middle, right lower lobes Right sided bronchus straight shot Cough, fever, copious foul-smelling sputum, chest pain,

50 Pulmonary Abscess Gross

51 Aspiration Pneumonia

52 Pulmonary Abscess Necrotizing infection with tissue destruction

53 Pleuritis
54 Consequences of Abscesses Empyema Hemothorax Sepsis Adhesions
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Sheet: Patho-Pulmonary infections Done by: Maen Faoury
 Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
Sheet: Patho-Pulmonary infections Done by: Maen Faoury Pneumonitis : might be an infection or not. Chemical Pneumonitis : not an infection. Parenchyma : an infection.( تندرج تحت ال pneumonitis) Lung Parenchyma
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Exam 2 Respiratory Disorders
 Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
2015/4/14. Pneumonia. Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) Lobar pneumonia.
 Lobar pneumonia.") Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Pulmonary Diseases. We Move A Lot of Air. Basic Categories. Alveolar Level. Developmental
 Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
Pulmonary Diseases We Move A Lot of Air Alveolar Level Functions Oxygenation CO 2 & ph Basic defenses Nose hairs Cilia Mucus Cough reflex Immune system Basic Categories Congenital Infectious Neoplastic
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES
 Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
Appendix E1. Epidemiology
 Appendix E1 Epidemiology Viruses are the most frequent cause of human infectious diseases and are responsible for a spectrum of illnesses ranging from trivial colds to fatal immunoimpairment caused by
Appendix E1 Epidemiology Viruses are the most frequent cause of human infectious diseases and are responsible for a spectrum of illnesses ranging from trivial colds to fatal immunoimpairment caused by
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections.
 In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
In the name of God Principles of post Tx infections 1: Potential etiologies of infection in these patients are diverse, including common and uncommon opportunistic infections. Infection processes can progress
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Respiratory Pathophysiology
 Respiratory Pathophysiology Objectives: Respiratory infections and lung cancer. Pleural effusion & edema, pleuritis, pneumothorax and atelectasis. Obstructive airway disease and chronic interstitial lung
Respiratory Pathophysiology Objectives: Respiratory infections and lung cancer. Pleural effusion & edema, pleuritis, pneumothorax and atelectasis. Obstructive airway disease and chronic interstitial lung
Patient information: Pneumonia in adults (Beyond the Basics)
") Page 1 of 8 Official reprint from UpToDate www.uptodate.com 2014 UpToDate Patient information: Pneumonia in adults (Beyond the Basics) Authors Thomas J Marrie, MD Thomas M File, Jr, MD Section Editor John
Page 1 of 8 Official reprint from UpToDate www.uptodate.com 2014 UpToDate Patient information: Pneumonia in adults (Beyond the Basics) Authors Thomas J Marrie, MD Thomas M File, Jr, MD Section Editor John
May. Pathology #2. part. Rahaf Al-yousef. Mohammad Al-Qudah
 8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
8 th May Pathology #2 nd Pneumonias 2 part Mohammad Al-Qudah Rahaf Al-yousef In the first part of our lectures today, we will define pneumonia clinically and pathologically(which is an infection of the
PATHOLOGY & PATHOPHYSIOLOGY
 PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF THE RESPIRATORY SYSTEM DISORDERS OF THE RESPIRATORY SYSTEM Disorders of the Respiratory System Infections Degenerative Tumours Immune Trauma Congenital Upper respiratory
PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF THE RESPIRATORY SYSTEM DISORDERS OF THE RESPIRATORY SYSTEM Disorders of the Respiratory System Infections Degenerative Tumours Immune Trauma Congenital Upper respiratory
Histopathology: pulmonary pathology
 Histopathology: pulmonary pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about these
Histopathology: pulmonary pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about these
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Anatomy of the Respiratory System Respiratory Infections Respiratory tract can be divided into: Upper Respiratory Tract (URT): Sinuses Nasopharynx,.
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Anatomy of the Respiratory System Respiratory Infections Respiratory tract can be divided into: Upper Respiratory Tract (URT): Sinuses Nasopharynx,.
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines
 Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pathology of pulmonary vascular disease. Dr.Ashraf Abdelfatah Deyab. Assistant Professor of Pathology Faculty of Medicine Almajma ah University
 Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Pathology lab 4 DONE BY : MORAD ABU QAMAR
 Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Firm Texture. (chronic) Cut surface: purulent exudate in bronchi Sequels: Abscesses,
 Cut surface: purulent exudate in bronchi Sequels: Abscesses,") 2008 Classification of Pneumonias in Domestic Animals There is no universal classification! Based on texture, distribution of lesions and type of exudate, pneumonias in domestic animals are currently classified
2008 Classification of Pneumonias in Domestic Animals There is no universal classification! Based on texture, distribution of lesions and type of exudate, pneumonias in domestic animals are currently classified
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
The Respiratory System. Dr. Ali Ebneshahidi
 The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Respiratory Diseases
 8-year system Curriculum 6nd Week Theme Respiratory Diseases ZHANG WEI ( 张伟 ) Associate Professor, Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhejiang University
8-year system Curriculum 6nd Week Theme Respiratory Diseases ZHANG WEI ( 张伟 ) Associate Professor, Ph.D. Institute of Pathology & Forensic Medicine Department of Pathology & Patho-physiology Zhejiang University
SCPA502-Respiratory Pathology
 Problem Mr. B is 57 years old, high 157 cm and weight 76 kg. He has worked as the dump truck driver in the coal mine since 1980, and also smoked cigarette 1 pack/day more than 30 years. What are the risk
Problem Mr. B is 57 years old, high 157 cm and weight 76 kg. He has worked as the dump truck driver in the coal mine since 1980, and also smoked cigarette 1 pack/day more than 30 years. What are the risk
CHRONIC INFLAMMATION
 CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
Index. B Biological factors, 2 Brain stem encephalitis, Burkitt s lymphoma, 83, 105
 Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
RESPIRATORY TRACT INFECTIONS. CLS 212: Medical Microbiology Zeina Alkudmani
 RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
RESPIRATORY TRACT INFECTIONS CLS 212: Medical Microbiology Zeina Alkudmani Lower Respiratory Tract Upper Respiratory Tract Anatomy of the Respiratory System Nasopharynx Oropharynx Respiratory Tract Infections
NFECTIONS THROUGH THE RESPIRATORY TRACT
 NFECTIONS THROUGH THE RESPIRATORY TRACT **Infective agent s **Transmission **Host * viral infections * Bacterial infections *Fungal infections **Control of air-borne infections **INFECTIVE AGENTS The infective
NFECTIONS THROUGH THE RESPIRATORY TRACT **Infective agent s **Transmission **Host * viral infections * Bacterial infections *Fungal infections **Control of air-borne infections **INFECTIVE AGENTS The infective
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Unit 9. Respiratory System 16-1
 Unit 9 Respiratory System 16-1 Works together with the circulatory system Exchange of gases between atmosphere, blood, and cells If respiratory system and/or circulatory system fails, death will occur
Unit 9 Respiratory System 16-1 Works together with the circulatory system Exchange of gases between atmosphere, blood, and cells If respiratory system and/or circulatory system fails, death will occur
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Pneumocystis. Pneumocystis BIOL Summer Introduction. Mycology. Introduction (cont.) Introduction (cont.)
 Introduction (cont.)") Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
How to identify interstitial pneumonias.
 How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
Respiratory System Disorders 3
 Respiratory System Disorders 3 Lecture 25 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Porth s Pathophysiology: Concepts of Altered Health States Sheila C. Grossman
Respiratory System Disorders 3 Lecture 25 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Porth s Pathophysiology: Concepts of Altered Health States Sheila C. Grossman
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Destructive pulmonary disease due to mixed anaerobic infection
 Thorax (1970), 25, 41. Destructive pulmonary disease due to mixed anaerobic infection 0. SERIKI, A. ADEYOKUNNU, T. 0. DE LA CRUZ Departments of Paediatrics and Surgery, University College Hospital, Ibadan,
Thorax (1970), 25, 41. Destructive pulmonary disease due to mixed anaerobic infection 0. SERIKI, A. ADEYOKUNNU, T. 0. DE LA CRUZ Departments of Paediatrics and Surgery, University College Hospital, Ibadan,
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
09-Mar-15 PNEUMONIA RESPIRATORY SYSTEM L-3
 RESPIRATORY SYSTEM L-3 Professor Department of Pathology, University of Agriculture, Faisalabad. Email: mtjaved@uaf.edu.pk Web: https://sites.geocities.ws/mtjaved PNEUMONIA The pulmonary inflammatory response
RESPIRATORY SYSTEM L-3 Professor Department of Pathology, University of Agriculture, Faisalabad. Email: mtjaved@uaf.edu.pk Web: https://sites.geocities.ws/mtjaved PNEUMONIA The pulmonary inflammatory response
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than
 TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
Alveolar condensation syndrome
 Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
66YM Chronic obstructive pulmonary disease annual review. H Chronic obstructive pulmonary disease
 Supplementary materials Table S1. Read codes to define COPD Read code Medical code Clinical event Read term 66YM.00 11287 382901 Chronic obstructive pulmonary disease annual review H3...00 1001 338812
Supplementary materials Table S1. Read codes to define COPD Read code Medical code Clinical event Read term 66YM.00 11287 382901 Chronic obstructive pulmonary disease annual review H3...00 1001 338812