PEDIATRIC EKG WORKSHOP
|
|
|
- Cornelia Houston
- 5 years ago
- Views:
Transcription
1 WHAT s NEW IN MEDICINE 2018 PEDIATRIC EKG WORKSHOP Salaam Sallaam, MD Asst. Prof, Division of Cardiology Department of Pediatrics Seattle Children s Hospital
2 OVERVIEW Pediatric EKG interpretation Normal variants Pediatric Tachyarrhythmias Pediatric Bradycardias Miscellaneous
3 OVERVIEW Pediatric EKG interpretation Normal variants Pediatric Tachyarrhythmias Pediatric Bradycardias Miscellaneous

4 Cardiac Conduction System
5 Pediatric EKG Interpretation - Get familiar with the EKG machine - Be organized and methodical - Look at EVERY EKG the same way, no matter how abnormal it appears - Describe findings - Think of differential diagnosis of each abnormal finding - Integrate EKG with history, PE, and other patient data to formulate diagnosis
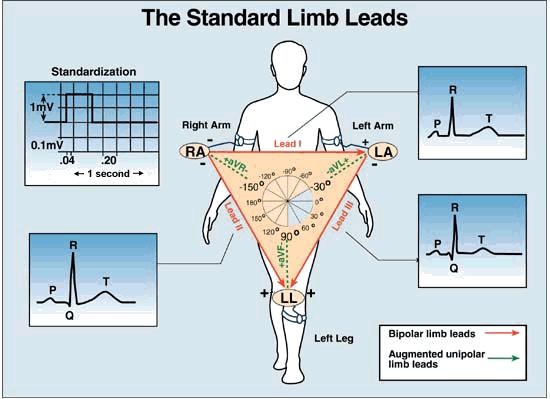
6 Technique The 12 lead EKG includes recordings from: Standard bipolar leads I, II and III Augmented leads avf, avl and avr Standard unipolar precordial leads V1 to V6 In a 15 lead EKG: The right-sided leads V3R, V4R and V7 are recorded additionally In addition, a longer recording of a single lead (usually lead II) is obtained to analyze the rhythm more precisely Lead II is chosen for most EKG interval measurements, as it is parallel to the long axis of the heart
7

8 V1: Fourth intercostal space to the right of the sternum. V2: Fourth intercostal space to the Left of the sternum. V3: Directly between leads V2 and V4. V4: Fifth intercostal space at midclavicular line. V5: Level with V4 at left anterior axillary line. V6: Level with V5 at left midaxillary line. (Directly under the midpoint of the armpit)
9 IMPORTANT POINTS TO CONSIDER o Was EKG properly obtained? Correct lead placement Normal paper speed (25 mm per second) Appropriate sensitivity full standard 1mV = 10 mm deflection limb and chest leads may NOT be the same standard o How old is the patient? Normals are age dependent

10 QRS Standardization 1 millivolt PR QT interval Full Half 0.2 secs
11 Basic EKG
12 EKG ANALYSIS Rhythm Rate Axis Morphology Intervals Hypertrophy
13 EKG ANALYSIS Rhythm Rate Axis Morphology Intervals Hypertrophy
14 Rhythm Sinus rhythm = sinus node - AV node Atrial rhythm Left atrium - AV node Low right atrium - AV node P wave axis (leads I and avf) = sinus rhythm = left atrial rhythm = low right atrial rhythm
15 Rhythm assessment contd. SA node RA LA -90 (+) I (-) avf (I) LV (-) I (+) avf RV (+) I (+) avf (avf) +90
16 Rhythm assessment (contd) No P waves junctional or idioventricular rhythm atrial fibrillation Multiple P waves (for each QRS) atrial flutter 2 nd or 3 rd degree AV block P waves of different shapes wandering atrial pacemaker PAC s
17 EKG ANALYSIS Rhythm Rate Axis Morphology Intervals Hypertrophy

18 Heart Rate Using a normal paper speed of 25 mm/second, Each small box on the EKG = 1 mm or 0.04 seconds. Each large box, or 5 mm, = 0.20 seconds.

19 Calculating Heart Rate Method 1: Count the number of small squares between the R-R intervals and divide 1500 by the number of small squares Method 2: Count the number of large squares between the R-R intervals and divide 300 by the number of large squares
.")
20 Calculating Heart Rate Method 3: Count and multiply the number of QRS complexes on the 12 lead ECG paper by 6 to obtain the heart rate (it takes 10 secs to record an EKG). Method 4: Memorize heart rate for selected RR intervals ( ) Start

21 Sinus Arrhythmia
22 EKG ANALYSIS Rhythm Rate Axis Morphology Intervals Hypertrophy
23 Axis determination Leads I and avf are normally used to determine the QRS axis. Normal axis: Positive QRS in leads I and avf. Left axis deviation: Positive QRS in lead I and negative QRS in lead avf. Right axis deviation: Negative QRS in lead I and a positive QRS in lead avf. Indeterminate axis: Negative QRS in lead I and avf, also referred to as extreme RAD.
24 I avf 270 I avf I avf 90 I avf
25 EKG ANALYSIS Rhythm Rate Axis Morphology Intervals Hypertrophy
26 Morphology P - axis - amplitude - duration
27 Axis Amplitude lead II (if NSR) normal < 3 mm Morphology > 3 mm lead II = right atrial enlargement uration lead V 1 normal < 0.1 sec (2.5 small boxes) > 0.1 sec or broad/notched P waves in lead V 1 = left atrial enlargement


28 RA enlargement LA enlargement
29 Morphology R - axis - amplitude - duration Q S
30 QRS axis (contd) I avf (-)90 0 (+) (+)90 (-)90 0 (-) (+)90 (+) (-)90 0 (+)90 (-) (-) (+)90
31 QRS axis -90 Age specific normals RA LA (I) LV RV 3 yr Newborn (avf) mo
32 QRS axis Right axis deviation RVH Right bundle branch block Left axis deviation Endocardial cushion defect Tricuspid atresia LVH (volume overload) Left bundle branch block

33 Right axis deviation
34 Left axis deviation
35 QRS Amplitude o Normals by age and lead (R & S waves) o > ULN indicates ventricular hypertrophy cannot use if bundle branch block present o Low voltage (limb leads < 5 mm) Myocarditis Pericarditis/pericardial effusion Hypothyroidism Thick chest wall

36 Left ventricular hypertrophy

37 Right Ventricular hypertrophy
38 QRS Duration o Time required for ventricular depolarization o General, <0.08 sec (2 small boxes) o Prolonged = abnormal delay or spread of impulse through ventricles Bundle branch blocks (R & L) Interventricular conduction delay Ventricular rhythm/ arrhythmias Ventricular pacemaker
39 Q waves o Ventricular septal depolarization o Present in leads II, III, avf, V 5, and V 6 o Normal amplitude < 5 mm o Normal duration < 0.02 sec o Deep and wide Infarction Fibrosis
40 Morphology T - axis - amplitude - duration
41 T waves o Ventricular repolarization o Usually mirrors QRS o Lead V 1 very important variable from birth to 5 days (+ is OK) negative until adolescence strong indicator of RVH and ventricular strain pattern if abnormal
42 T waves o Tall, peaked T waves Hyperkalemia LVH/volume overload o Flat T waves Non-specific Hypokalemia Hypothyroidism Pericarditis, myocarditis, ischemia LVH/pressure overload
43 EKG ANALYSIS Rhythm Rate Axis Morphology Intervals Hypertrophy
44 Intervals PR interval R P Q PQ S PR
45 PR interval o Impulse delay in AV node o Age specific normals o Prolonged PR (1 st degree AV block) abnormal AV node conduction myocarditis, toxins, metabolic derangement, congenital heart disease, medications, normal variant o Short PR WPW (delta wave) enhanced AVN conduction
46 ST segment R T J-point Q S ST
47 ST segment o Horizontal, isoelectric o 1-2 mm elevation/depression is not necessarily abnormal o J-point Depression Elevation or early repolarization o Abnormal ST shifts abnormal T waves downward sloping ST segment horizontal ST segment for >0.08 sec
48 ST segment J-point T T T J-point depression ST depression Early repolarization
49 ST segment o Pathologic ST changes Pericardial disease Myocarditis Myocardial ischemia/infarction Electrolyte abnormalities hypocalcemia prolongs ST segment (and QTc) hypercalcemia shortens ST segment
50 QT interval o Time required for ventricular depolarization and repolarization o Varies with heart rate o QTc = QT/ RR Normal < 0.45, up to 0.49 in infants o Prolonged QTc Hypocalcemia Myocarditis, myocardial disease Long QT syndrome
51 Summary o Keep in mind the reason for EKG o Look at every tracing the same way o Patient age o Calibration ( standard ) o Rhythm o Rate o Systematic, left-to-right inspection of EKG
52 OVERVIEW Pediatric EKG interpretation Normal variants Pediatric Tachyarrhythmias Pediatric Bradycardias Miscellaneous
53 Introduction o Rhythm disturbances in children Primary Secondary Associated with cardiac disease o The major risk of any arrhythmia is decreased cardiac output or degeneration into more critical arrhythmia, leading to syncope or death o Therefore it is important to determine the potential for any arrhythmia to degenerate into critical arrhythmia
54 General Principles o Symptoms may vary depending on the age o Recording of a suspected arrhythmia is necessary before diagnosing or treating a suspected arrhythmia o The urgency of work up and treatment depends on Symptom severity Cardiac structure & function Activity profile of a patient o P/E most often may be entirely normal
55 General Principles In evaluating a patient with arrhythmia associated with hemodynamic compromise, THINK SIMPLE. Fast/ disorganized: cardioversion/ defibrillation Slow: CPR
56 OVERVIEW Pediatric EKG interpretation Normal variants Pediatric Tachyarrhythmias Pediatric Bradycardias Miscellaneous

57 Normal Variants Recognition of normal variants is important to allay anxiety and to avoid unnecessary investigations Sinus arrhythmia: Phasic variations in heart rate with inspiratory acceleration and expiratory deceleration


58 Wandering atrial pacemaker: Characterized by different P wave morphologies on the same EKG Related to alterations in vagal tone Wenckebach phenomena: Progressive lengthening of PR interval followed by a dropped beat. Related to alterations in vagal tone
59 Variations in heart rate: Sinus tachycardia: Has been documented at rates at bpm Always look for a secondary cause Differentiated from SVT: variations with activity/ crying, and presence of secondary cause Sinus bradycardia: Sinus rate below expected for patient s age A highly conditioned athlete may have resting heart rate less than 40 bpm Be careful to rule out other causes like increased intracranial pressure, eating disorders, gastric distension, pharyngeal stimulation, toxins and drugs

60 Early Repolarization: - J-point elevation (of no more than 3 mm) with an upwardly concave ST segment - ST-segment elevation is more frequent in chest leads but can occur in leads I and II - Prevalent in young, African American males - Can be affected by exercise and hyperventilation
61 OVERVIEW Pediatric EKG interpretation Normal variants Pediatric Tachyarrhythmias Pediatric Bradycardias Miscellaneous
62 Evaluation of a child with an arrhythmia History: Accurate description may vary with age Important questions to ask: - How frequently and for how long do these episodes occur? - How does it begin and terminate? - What, if anything, initiates the episodes? - What, if anything, terminates the episodes? - History of caffeine intake, or any other meds? - In infants, enquire for symptoms of heart failure
63 Evaluation of a child with an arrhythmia Physical Examination: In setting of acute arrhythmia: - Check for signs of hemodynamic instability (suggested by evidence of poor cardiac output, hypotension, shock, altered mental status, and respiratory distress) In the setting of paroxysmal episodes: - Evaluate for any exacerbating factors e.g. fever, anemia, hyperthyroidism - Evaluate for any congenital heart defects that frequently are associated with arrhythmias - Evaluate for any infectious conditions
64 Diagnostic Testing EKG in sinus rhythm - Baseline rhythm - Conduction and repolarization intervals - Axes - Evidence of hypertrophy - Other abnormalities like pre-excitation, abnormal T wave morphology, etc EKG in arrhythmia accurate diagnosis Others: - Holter if daily symptoms - Event monitors (external or implantable) if more sporadic
65 Diagnostic Approach Three questions will define majority of the arrhythmias 1. Is the arrhythmia regular or irregular? 2. Are the QRS complexes narrow or wide? 3. What is the relationship between the P waves and the QRS complexes?
66 1. Is the arrhythmia regular or irregular? Regular Sinus tachycardia SVT Escape rhythms VT Irregular Sinus tachycardia Sinus arrhythmia Ectopic beats Advanced degree heart blocks AF/VF VT
67 2. Are the QRS complexes narrow or wide? Narrow QRS complexes: - Supraventricular - Junctional Wide QRS complexes: - Ventricular in origin - Paced complexes - Supraventricular if ass. with baseline BBB if ass. with rate dependent aberrancy if ass. with pre-excitation
68 3. What is the relationship between P waves and QRS complexes? 1:1 AV relationship: SVT Occ. VT > 1:1 AV relationship: Ectopic atrial tachycardia Multifocal atrial tachycardia Atrial flutter < 1:1 AV relationship: VT Junctional ectopic tachycardia
69


70 Narrow Complex Tachycardia - SVT

71 Wide Complex Tachycardia - VT


72 WPW syndrome

73 Atrial Flutter

74 Atrial fibrillation

75 Ectopic Atrial Tachycardia (with Variable Ventricular Response)
76 In pts with hemodynamic stable narrow complex tachycardia, adenosine can be diagnostic if not therapeutic.


77

78 Multifocal Atrial Tachycardia
79

80 Junctional Ectopic Tachycardia

81 Long QT syndrome
82 Torsade's de Pointes
83 OVERVIEW Pediatric EKG interpretation Normal variants Pediatric Tachyarrhythmias Pediatric Bradycardias Miscellaneous
 - Commonly with underlying atrial fibrillation (AF) or")
84 The diagnostic possibilities of bradycardia are limited Sinus node dysfunction Clinical syndrome characterized by - Chronic SA nodal dysfunction - AV nodal conduction disturbances - Alternating bradycardia and tachycardia (the bradycardiatachycardia syndrome) - Commonly with underlying atrial fibrillation (AF) or atrial flutter

85 Heart blocks/ AV node dysfunction: Atrioventricular (AV) block is defined as a delay or interruption in the transmission of an atrial impulse to the ventricles due to an anatomical or functional impairment in the conduction system First-degree AV block occurs when the PR-interval is greater than the upper limits of normal for age. In general, the normal PR-intervals are: 70 to 170 msec in newborns, and 80 to 220 msec in young children and adults It reportedly occurs in up to 6 percent of normal neonates
 - It usually does not progress to complete block")
86 Second-degree AV block, the organized atrial impulse fails to be conducted to the ventricle in a 1:1 ratio Mobitz type 1 block (Wenckebach phenomena): - There is progressive prolongation of the PR-interval until a P wave fails to be conducted. - Mobitz type 1 block is seen in normal children and young adults especially at times of high parasympathetic tone (e.g., sleep or in well-trained athletes) - It usually does not progress to complete block

87 Mobitz type 2 block: - The PR interval remains unchanged prior to the P wave that suddenly fails to conduct to the ventricles - It is associated with various forms of congenital heart disease and is seen after cardiac surgery. - Type 2 block occurs at or below the level of the AV node, indicating disease within the His bundle and bundle branches. - It has a less predictable course and frequently progresses to complete heart block

88 Third-degree AV block (Complete heart block): - There is complete failure of the atrial impulse to be conducted to the ventricles. - The atrial and ventricular activity are independent of one another. - The escape rhythm (usually slower than the lower limits of normal for age) is dictated by the location of the block - It can be either congenital or acquired
89 Miscellaneous

90 Acute Pericarditis

91 Acute Pericarditis

92 Acute Pericarditis
93 ALCAPA

94 HCMP with WPW

95 Pompe s disease

96 Dextrocardia
97 PAC s
98 PAC s Normally conducted PAC
99 PAC s Normally conducted PAC Blocked PAC

100 PAC s Normally conducted PAC Blocked PAC Aberrantly conducted PAC

101 PJC s

102 PVC s

103 Hyperkalemia
104 Hyperkalemia The earliest changes of hyperkalemia are - Appearance of peaked, narrow T waves - Shortened QT interval, which reflect abnormally rapid repolarization At a plasma K concentration 7 to 8 meq/l (changes due to delayed depolarization) - Widening of the QRS complex - Decreased amplitude with widening and eventual loss of the P wave, PR prolongation can also occur - Followed sometimes by second-degree or third-degree AV block Final changes - Sine-wave pattern, in which the widened QRS complex merges with the T wave - Followed by ventricular fibrillation or asystole



105 Hyperkalemia The earliest changes of hyperkalemia are - Appearance of peaked, narrow T waves - Shortened QT interval, which reflect abnormally rapid repolarization At a plasma K concentration 7 to 8 meq/l (changes due to delayed depolarization) - Widening of the QRS complex - Decreased amplitude with widening and eventual loss of the P wave, PR prolongation can also occur - Followed sometimes by second-degree or third-degree AV block Final changes - Sine-wave pattern, in which the widened QRS complex merges with the T wave - Followed by ventricular fibrillation or asystole
106 EKG changes with CNS Disease ECG abnormalities occur most often in patients with SAH, ischemic stroke, ICH, head trauma, neurosurgical procedures, acute meningitis, intracranial space-occupying tumors, and epilepsy The prevalence of EKG abnormalities in this group of patients varies from 50 to 90% Most common findings are depressed ST segments, flat or inverted T waves, prominent U waves, and prolongation of the QTc
107 Hypothermia EKG features of hypothermia - The Osborn wave, also known as the J wave, is a hump-like deflection between the QRS complex and the early part of the ST segment - Shivering artifacts due to muscular tremor - Sinus bradycardia - QRS prolongation, prolongation of the PR interval & QTc - Atrial fibrillation is common below 32 C - Risk of ventricular fibrillation is high below 28 C
108 THANK YOU
109 QUESTIONS

110 Pediatric Cardiology Board Review Book second edition QUESTION 1 A newborn presents with a narrow complex tachycardia. Adenosine is given, and the following rhythm strip was recorded. What is the most effective method for terminating the tachycardia? A. Cardioversion B. Oral propranolol C. Oral digoxin D. Intravenous amiodarone E. Oral amiodarone

111 QUESTION 2 A 16-year-old football player comes to you for evaluation of palpitations and dizziness. The following EKG was obtained. What would you do? A. Perform a 24-hour Holter monitor. If there are no arrhythmias, let him play B. Permanently disqualify him from all competitive sports based on the ECG C. Let him play as the ECG findings are a normal variant D. Not let him play until evaluation including an echocardiogram is performed E. Let him play and repeat the ECG in 6 months Pediatric Cardiology Board Review Book second edition
112 QUESTION 3 A 5-year-old child with diabetes ketoacidosis with a heart rate of 140 bpm. Serum potassium concentration is 8.5 mg/l. The ECG rhythm strip would be expected to demonstrate which of the following? A. Low amplitude T wave B. Prominent Q wave C. Prolonged QRS duration D. Short PR interval E. High amplitude P wave Pediatric Cardiology Board Review Book second edition
113 QUESTION 4 You would advise caution when using which of the following drugs in a patient with long QT syndrome (LQTS)? A. Lidocaine B. Amoxicillin with clavulanate C. Verapamil D. Erythromycin E. Metoprolol Pediatric Cardiology Board Review Book second edition

114 QUESTION 5 A 14-year-old previously healthy girl collapses while playing soccer. Following successful cardiopulmonary resuscitation, the following ECG was obtained. Which of the following is the most likely test to define her diagnosis? Pediatric Cardiology Board Review Book second edition
115 QUESTION 5 A 14-year-old previously healthy girl collapses while playing soccer. Following successful cardiopulmonary resuscitation, the following ECG was obtained. Which of the following is the most likely test to define her diagnosis? A. Cardiac MRI B. EP study C. Echocardiogram D. Genetic testing for KCNQ1 mutation Pediatric Cardiology Board Review Book second edition

116 QUESTION 6 An asymptomatic 14-year-old patient with a normal examination and resting ECG has a 24hour Holter monitor showing the finding in below. while sleeping. The rest of the Holter is normal. Which of the following is the next most appropriate step? Pediatric Cardiology Board Review Book second edition
117 QUESTION 6 An asymptomatic 14-year-old patient with a normal examination and resting ECG has a 24hour Holter monitor showing the finding below. while sleeping. The rest of the Holter is normal. Which of the following is the next most appropriate step? EP study B. Exercise treadmill test C. Reassurance D. Initiation of a β -blocker E. Pacemaker implantation Pediatric Cardiology Board Review Book second edition
118 QUESTION 7 A newborn baby presents with complete AV block. Which of the following is the most likely finding in the mother? A. Serum potassium of 8 B. Ventricular septal defect C. Low platelet count D. Positive rheumatoid factor E. Ro (SSA) and La (SSB) antibodies Pediatric Cardiology Board Review Book second edition
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation. Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction
 * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction") ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
The ABC of Pediatric ECG
 The ABC of Pediatric ECG Mohamed Hamdan, MD, FAAP, FACC Assistant Professor of Pediatrics Columbia University College of Physicians and Surgeons, NY, USA Consultant Pediatric Cardiologist & Co-Director
The ABC of Pediatric ECG Mohamed Hamdan, MD, FAAP, FACC Assistant Professor of Pediatrics Columbia University College of Physicians and Surgeons, NY, USA Consultant Pediatric Cardiologist & Co-Director
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
5- The normal electrocardiogram (ECG)
") 5- The (ECG) Introduction Electrocardiography is a process of recording electrical activities of heart muscle at skin surface. The electrical current spreads into the tissues surrounding the heart, a small
5- The (ECG) Introduction Electrocardiography is a process of recording electrical activities of heart muscle at skin surface. The electrical current spreads into the tissues surrounding the heart, a small
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
ECG. Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13
 ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
2017 EKG Workshop Basic. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
EKG. Danil Hammoudi.MD
 EKG Danil Hammoudi.MD What is an EKG? The electrocardiogram (EKG) is a representation of the electrical events of the cardiac cycle. Each event has a distinctive waveform, the study of which can lead to
EKG Danil Hammoudi.MD What is an EKG? The electrocardiogram (EKG) is a representation of the electrical events of the cardiac cycle. Each event has a distinctive waveform, the study of which can lead to
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
PATIENT S NAME, DATE/TIME,
 ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida
 S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
CORONARY ARTERIES HEART
 CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
2017 BDKA Review. Regularity Rate P waves PRI QRS Interpretation. Regularity Rate P waves PRI QRS Interpretation 1/1/2017
 1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
ECG INTERPRETATION MANUAL
 Lancashire & South Cumbria Cardiac Network ECG INTERPRETATION MANUAL THE NORMAL ECG Lancashire And South Cumbria Cardiac Physiologist Training Manual THE NORMAL ECG E.C.G CHECKLIST 1) Name, Paper Speed,
Lancashire & South Cumbria Cardiac Network ECG INTERPRETATION MANUAL THE NORMAL ECG Lancashire And South Cumbria Cardiac Physiologist Training Manual THE NORMAL ECG E.C.G CHECKLIST 1) Name, Paper Speed,
, David Stultz, MD.
 http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C. For more presentations
 ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
PAEDIATRIC ACUTE CARE GUIDELINE. ECG Interpretation
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE ECG Interpretation Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE ECG Interpretation Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019
 THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM
 THE ANALYSIS OF THE ELECTROCARDIOGRAM") ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM Scridon Alina, Șerban Răzvan Constantin Recording and analysis of the 12-lead ECG is part of the basic medical assessment performed for every
ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM Scridon Alina, Șerban Răzvan Constantin Recording and analysis of the 12-lead ECG is part of the basic medical assessment performed for every
Lecture outline. Electrical properties of the heart. Automaticity. Excitability. Refractoriness. The ABCs of ECGs Back to Basics Part I
 Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Module 1: Introduction to ECG & Normal ECG
 Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing