Can We Prevent Delirium in the ICU?
|
|
|
- Frederica Spencer
- 5 years ago
- Views:
Transcription
1 Can We Prevent Delirium in the ICU? Dr Mervyn Maze MB ChB, FRCP, FRCA, FMedSci Department of Anesthesia and Perioperative Care, University California San Francisco 1
2 Questions regarding ICU Delirium What are the clinical manifestations? What are the etiogenic factors? Is sleep important? Is the choice of sedative agent important? What Level 1 evidence can guide pre-emptive therapy? 2
3 Clinical Manifestations and Diagnosis Newly-diagnosed fluctuating disturbance in Level of consciousness including attentiveness Cognitive function especially memory DSM IV - attributable to a medical condition Hyper- vs hypo-active delirium Long-lasting consequences Diagnosis CAM ICU 3
4 Risk Factors for Delirium in the ICU Patient-related Age Existing psychopathology (incl Alcoholism and TBI) Environmental Sleep deprivation Noise Light interventions CNS-altering Drugs Sedative/Analgesics Anticholinergics 4
5 Benefits of Natural Sleep Avoid Sleep Deprivation Cognitive Dysfunction Hypoactive delirium-like state Immune Dysfunction Susceptibility for infection High Mortality Rate from Sepsis Restoration and Repair 5
6 Sleep in the ICU Longer periods of wakefulness 1 Shorter periods of Deep Sleep Less time in stages III/IV NREM 2 Less periods of REM sleep 3 Loss of circadian rhythm 4 References: 1 Aurell and Elhmqvist, BMJ Cooper et al Chest Gabor et al Am J Resp Crit Care Freedman et al Am J Resp Crit Care
7 Conflict of Interest Dexmedetomidine patented for sedativehypnotic properties in 1986 with Mika Scheinin Reassigned rights to Farmos in 1987 $250K to support preclinical research at Stanford Farmos acquired by Orion Dexmedetomidine licensed to Abbott/Hospira Accrue no financial benefit from sales 7
8 Cl Clonidine H N N α 2 Agonists Dexmedetomidine H CH 3 N Cl N CH 3 CH 3 N Clonidine Dexmedetomidine Selectivity: α 2 :α 1 200:1 1 t 1/2 β 8 hrs 1 PO, patch, epidural 2 Antihypertensive 1 Analgesic adjunct 1 IV formulation not available in US Selectivity: α 2 :α :1 3 t 1/2 β 2 hrs 3 Intravenous 3 Sedative-analgesic 3 Only IV α 2 available for use in the US 1. Maze. White paper; Khan et al. Anaesthesia. 1999;54: Kamibayashi, Maze. Anesthesiology. 2000;93:

9 Ca ++ Ca ++ Ca ++ Decrease in action potential due to hyperpolarization α 2 A α 2 AR G o G k K + K + + Decrease in influx of Ca ++ K + 9
10 Molecular and Neuronal Action of α 2 agonists Initiated in the locus coeruleus (LC) Transduced by mechanisms which hyperpolarize the membrane Decrease firing rate of the LC neurons 10
11 Hypnotic Mechanism of Benzodiazepine Decreases wakefulness by positive allosteric modulation of α subunit of the GABA A receptor Similar to alcohol and barbiturates Decreases deeper phases of NREM sleep Increase dopamine release in VTA 1 similar reward mechanism as present in addictive drugs Withdrawal results in Anxiety Delirium Seizures 1. Tan et al Nature
12 Lorazepam and ICU Delirium Pandharipande et al, Anesthesiology 104:21-26,

13 13

14 Saper et al,

15 15

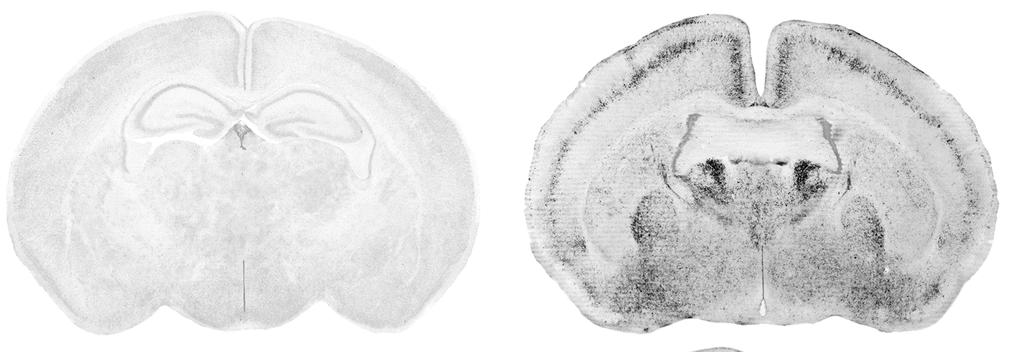
16 Dexmedetomidine Induces similar changes as NREM sleep in Brain Nuclei Nelson et al, Anesthesiology


17 Sedation by Dexmedetomidine Nelson et al Anesthesiology 2003 TMN DRN VLPO PPTg LC TMN: Tuberomammilary nulcleus VLPO: Ventrolateral preoptic nucleus LC: Locus Coeruleus PPTg: Pedunculopontine tegemental nucleus DRN: Dorsal raphe nucleus 2 17
18 fmri placebo - dexmedetomidine 18


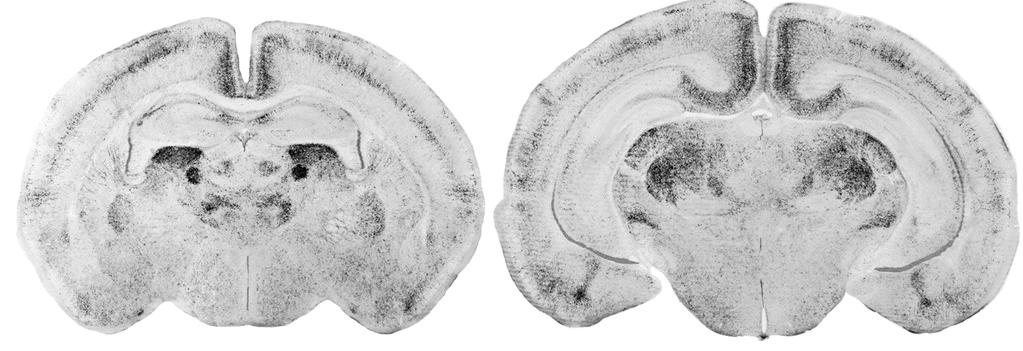
19 GABAergics don t Produce NREM sleep changes in Locus Ceruleus (LC) Nelson et al, Nat Neurosci

20 fmri placebo - midazolam 20
21 INTERPRETATION Hypnotics do not converge on the sleep pathway at the same point α 2 agonists within the brainstem GABAmimetics within the hypothalamus Results in different hypnotic responses 21
22 Ability to be aroused by noise to perform a task during sedation by dexmedetomidine vs midazolam Task & Noise Task alone PLA DEX MDZ Drug Coull et al,


23 Immunostaining for co-localization of orexin and cfos in Peri-Fornical Area during Anesthesia 23
24 Activity in Orexinergic Neurons during equi-hypnotic doses of General Anesthetics * * * * 10 0 SAL DEX ISO PTB PRO MUS 24


25 Neural substrates required for BDZ- vs a 2 -sedation Nelson et al, Nature Neuroscience 2002; Anesthesiology
26 INTERPRETATION Hypnotic action of dexmedetomidine is similar to natural sleep with an active arousal system 26
27 Potential Problems with ICU Sedative Regimens Produce Poor Sleep Hygiene Prolonged sedation provokes difficulty in weaning from mechanical ventilation increased length of stay in intensive care unit Precludes neurological examination Predisposes to delirium Predisposes to infection 27
28 Potential Benefits of ICU Sedation with Dexmedetomidine Active Arousal System Co-operative Sedation Responsive to Healthcare Team Assessment of System Function Less Isolation Permits wake-up while maintaining sedation Less Sleep Deprivation Less Delirium Less Infection Less MR from Sepsis 28







29 29
30 Maximize Efficacy of targeted sedation and reduce Neurological Dysfunction MENDS Trial To determine if changing sedation paradigms by targeting α 2 receptors instead of GABA receptors will reduce duration and prevalence of acute brain dysfunction (delirium and coma) achieve equivalent efficacy of sedation Other outcomes ventilator free days ICU and hospital lengths of stay neuropsychological function at discharge mortality at 28-days mortality rate from sepsis 30

31 MENDS Study Double blind randomized controlled trial Pandharipande et al, JAMA
32 Assessment of End Points Efficacy of sedation-ability to achieve sedation established by ICU team Duration of delirium - defined as delirium and coma free days, i.e the days alive and free of delirium or coma Mortality Rate at 28 days 32
33 Baseline Characteristics Demographic Lorazepam (n=51) Dexmed (n=52) P value Age 59 (45, 67) 60 (49,65) 0.96 Males 45% 58% 0.20 APACHE II 27 (24,32) 29 (24, 32) 0.75 SOFA score 9 (7,11) 10 (8,12) 0.23 Admitting Diagnosis Sepsis/ARDS 39% 37% 0.78 COPD 4% 4% 0.99 Pulmonary other 22% 23%
34 Baseline Characteristics Demographic Lorazepam (n=51) Dexmed (n=52) P value ICU type MICU 69% 71% 0.78 SICU 31% 29% 0.78 MV and enrollment Pre-enrollment lorazepam (mg) 17h (8,27) 22h (14,35) (0,3) 0.25 (0,4.25)
35 Efficacy of Sedation Outcome Loraz n=51 Dexmed n=52 P value % Days at Nurse Target 67 (48,83) 80 (58,100) 0.04 % Days at Physician Target 55 (8,67) 67 (50,85)
36 p=.01 Brain Dysfunction p=.09 p=.001 Dexmedetomidine Lorazepam Delirium/Coma-Free Days Delirium-Free Days Coma-Free Days Pandharipande et al, JAMA
37 Other Clinical Outcomes Outcome Loraz n=50 Dexmed n=51 P value MV free days 18 (0,23) 22 (0,24) 0.22 ICU stay 9 (6,13.5) 7.5 (5,18) 0.31 Mortality (28 days) 27% 17%
38 INTERPRETATION A strategy targeting the α 2 receptors and sparing the GABA receptors can Achieve target sedation goals Increase days free of delirium/ coma Increase days alive 38
39 Dex Long-Term Study MICU Ventilated on Sedatives 2(Dex):1 (Mdz) randomization Control Midazolam (GABA) +/- Fentanyl Intervention Dexmedetomidine (α2) +/- Fentanyl Riker R. et al JAMA

40 Prevalence of Delirium With Dexmedetomidine vs Midazolam Riker, R. R. et al. JAMA 2009;301: Copyright restrictions may apply. 40
41 41
42 Septic subgroup analysis Mechanical Ventilation Mortality Rate Length of Stay Pandharipande et al Critical Care
43 Demographics of septic subgroup Variable Lorazepam (n=20) Dexmedetomidine (n=19) P value Age 55 (44,65) 57 (49,66) 0.66 Males 35% 53% 0.17 Medical ICU 85% 84% 0.95 APACHE II 28 (25,32) 30 (24,32) 0.86 IQCODE 3 (3,3) 3 (3,3) 0.34 RASS 1 st evaluation -4 (-4,-3) -3 (-4,-2) 0.24 Study drug dose (units) 3 (2,4) 0.9 (4.5,1.1) NA 43


44 Acute Brain Dysfunction in Sedated Septic ICU Patients 44
45 Pandharipande et al Critical Care
46 Effect of Sedatives on ICU Delirium Benzodiazepines enhance likelihood of developing acute brain failure Dexmedetomidine may be beneficial Induces better sleep that enables Synaptic Downscaling provides space for processing new information Tononi & Cirelli Maintains immune system function 46
47 Safety of Midazolam in the NICU Ng et al, Cochrane Meta-analysis, 2010 Adverse neurological outcomes more prevalent after midazolam No definitive data to support the safety and effectiveness of benzodiazepines for neonatal sedation 47
48 Neuroapoptosis following GABAergics in Neonatal Mice 48
49 α 2 Adrenoceptor Agonist Properties during Neurodevelopment Trophic Effects in CNS through ERK Winzer-Serhan & Leslie 1999; Wang et al 2006 Hypnotic and Analgesic properties Sanders et al 2005 Anti-apoptotic properties Ma et al 2003 Sanders et al

50 50

51 Dexmedetomidine attenuates Isoflurane-induced Apoptotic Neurodegeneration Sanders et al 2009 Anesthesiology 51
52 Dex attenuates isoflurane-induced memory deficit 52

53 Dexmedetomidine prevents downregulation of perk by isoflurane Bcl-2 perk2 perk1 α-tubulin C Iso Iso + Dex 53
54 Poor sleep hygiene Conclusions Common in ICU patients Capable of producing delirium Sedatives can contribute to delirium Benzodiazepines preclude normal sleep α 2 agonists produce near-normal sleep Neonatal neuroapoptosis Provoked by benzodiazepines Prevented by α 2 agonists 54
55 Acknowledgements Nick Franks (Bill Lieb) Guo Tianzhi Daqing Ma Bing-Xue Chen Pratik Pandharipande, Wes Ely Laura Nelson, Anna Zacharia, Rob Sanders Clif Saper, Lee Limbird NIH MRC Wellcome Trust 55
Sleep and Clinical Outcomes in Critical Care and Perioperative Settings
 Sleep and Clinical Outcomes in Critical Care and Perioperative Settings Dr Mervyn Maze MB ChB, FRCP, FRCA, FMedSci Department of Anesthesia and Perioperative Care, Questions to be Addressed Why is sleep
Sleep and Clinical Outcomes in Critical Care and Perioperative Settings Dr Mervyn Maze MB ChB, FRCP, FRCA, FMedSci Department of Anesthesia and Perioperative Care, Questions to be Addressed Why is sleep
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
COGNITIVE DYSFUNCTION IN THE ELDERLY PATIENT QUIZ #34
 COGNITIVE DYSFUNCTION IN THE ELDERLY PATIENT QUIZ #34 M. ANGELE THEARD, MD STAFF ANESTHESIOLOGIST LEGACY EMANUEL MEDICAL CENTER PORTLAND, OR QUIZ TEAM: SHOBANA RAJAN, MD SUNEETA GOLLAPUDY, MD VERGHESE
COGNITIVE DYSFUNCTION IN THE ELDERLY PATIENT QUIZ #34 M. ANGELE THEARD, MD STAFF ANESTHESIOLOGIST LEGACY EMANUEL MEDICAL CENTER PORTLAND, OR QUIZ TEAM: SHOBANA RAJAN, MD SUNEETA GOLLAPUDY, MD VERGHESE
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Sedative-Hypnotics & the Treatment of Hypersomnia October 22, 2018 Pharm 9002 Mark Beenhakker, Pharmacology
 Sedative-Hypnotics & the Treatment of Hypersomnia October 22, 2018 Pharm 9002 Mark Beenhakker, Pharmacology markbeen@virginia.edu Glossary Anxiolytic: decreases anxiety Sedative: (1) decreases activity,
Sedative-Hypnotics & the Treatment of Hypersomnia October 22, 2018 Pharm 9002 Mark Beenhakker, Pharmacology markbeen@virginia.edu Glossary Anxiolytic: decreases anxiety Sedative: (1) decreases activity,
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Relevance of sleep neurobiology for cognitive neuroscience and anesthesiology
 1 Relevance of sleep neurobiology for cognitive neuroscience and anesthesiology Giancarlo Vanini, MD, Helen A. Baghdoyan, PhD, and Ralph Lydic, PhD Introduction Although general anesthetics are used for
1 Relevance of sleep neurobiology for cognitive neuroscience and anesthesiology Giancarlo Vanini, MD, Helen A. Baghdoyan, PhD, and Ralph Lydic, PhD Introduction Although general anesthetics are used for
Polysomnography SLEEP IN THE ICU AN OVERVIEW. Stages of Sleep. Morning Conference
 Polysomnography SLEEP IN THE ICU AN OVERVIEW Morning Conference Polysomnography measures: Patient s airflow though the nose and mouth Movements of respiratory muscles and limbs Eye movements Arterial blood
Polysomnography SLEEP IN THE ICU AN OVERVIEW Morning Conference Polysomnography measures: Patient s airflow though the nose and mouth Movements of respiratory muscles and limbs Eye movements Arterial blood
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Antidepressants and Sedatives. David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School
 Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Sedatives and Hypnotics. Ahmad Al-Tarifi. Zahra Khalil. Pharmacology. 1 P a g e
 Sedatives and Hypnotics Ahmad Al-Tarifi Zahra Khalil 1 P a g e Pharmacology 7 OCD can lead to an anxious behavior and anxiety can be treated with drugs called Sedatives and Hypnotics. What are sedatives?
Sedatives and Hypnotics Ahmad Al-Tarifi Zahra Khalil 1 P a g e Pharmacology 7 OCD can lead to an anxious behavior and anxiety can be treated with drugs called Sedatives and Hypnotics. What are sedatives?
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University
 Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
New approaches of sedation in critically ill patients.
 New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
MR04A3 An isoindoline derivative, New Sedative/Anesthetic Agent
 MR04A3 An isoindoline derivative, ew Sedative/Anesthetic Agent ovember 2009 1 Introduction Sedatives are widely used in: Settings providing stressful and painful procedures Gastroenterology (colonoscopy
MR04A3 An isoindoline derivative, ew Sedative/Anesthetic Agent ovember 2009 1 Introduction Sedatives are widely used in: Settings providing stressful and painful procedures Gastroenterology (colonoscopy
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Delirium: Prevention with Melatonin
 Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
European Society of Anaesthesiologists NITROUS OXIDE (N2O)-INDUCED ANALGESIA
-INDUCED ANALGESIA") European Society of Anaesthesiologists NITROUS OXIDE (N2O)-INDUCED ANALGESIA 14RC2 MERVYN MAZE Sir Ivan Magill Department of Anaesthetics and Intensive Care, Imperial College, London, UK Saturday June
European Society of Anaesthesiologists NITROUS OXIDE (N2O)-INDUCED ANALGESIA 14RC2 MERVYN MAZE Sir Ivan Magill Department of Anaesthetics and Intensive Care, Imperial College, London, UK Saturday June
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
ICU Delirium A Real Epidemic (or are we delirious)?
?") ICU Delirium A Real Epidemic (or are we delirious)? CCCF: Toronto October 2014 Jesse Hall MD University of Chicago Section of Pulmonary and Critical Care Medicine Faculty Disclosures Dr. Hall receives
ICU Delirium A Real Epidemic (or are we delirious)? CCCF: Toronto October 2014 Jesse Hall MD University of Chicago Section of Pulmonary and Critical Care Medicine Faculty Disclosures Dr. Hall receives
IJBCP International Journal of Basic & Clinical Pharmacology
 Print ISSN 2319-2003 Online ISSN 2279-0780 IJBCP International Journal of Basic & Clinical Pharmacology doi: 10.5455/2319-2003.ijbcp20141220 Research Article Comparison of two different doses of dexmedetomidine
Print ISSN 2319-2003 Online ISSN 2279-0780 IJBCP International Journal of Basic & Clinical Pharmacology doi: 10.5455/2319-2003.ijbcp20141220 Research Article Comparison of two different doses of dexmedetomidine
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
NEURAL MECHANISMS OF SLEEP (p.1) (Rev. 3/21/07)
 (Rev. 3/21/07)") NEURAL MECHANISMS OF SLEEP (p.1) (Rev. 3/21/07) 1. Revisitation of Bremer s 1936 Isolated Brain Studies Transected the brain: a. Cut between the medulla and the spinal cord ( encephale isole ) Note: recall
NEURAL MECHANISMS OF SLEEP (p.1) (Rev. 3/21/07) 1. Revisitation of Bremer s 1936 Isolated Brain Studies Transected the brain: a. Cut between the medulla and the spinal cord ( encephale isole ) Note: recall
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
SLEEP DISORDERS IN HUNTINGTON S DISEASE. Gary L. Dunbar, Ph.D.
 SLEEP DISORDERS IN HUNTINGTON S DISEASE Gary L. Dunbar, Ph.D. Executive Director, Field Neurosciences Institute Co-Director, Program in Neuroscience Central Michigan University Pre-Talk Test 1. Which type
SLEEP DISORDERS IN HUNTINGTON S DISEASE Gary L. Dunbar, Ph.D. Executive Director, Field Neurosciences Institute Co-Director, Program in Neuroscience Central Michigan University Pre-Talk Test 1. Which type
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Introduction to Physiological Psychology
 Introduction to Physiological Psychology Psych 260 Kim Sweeney ksweeney@cogsci.ucsd.edu cogsci.ucsd.edu/~ksweeney/psy260.html What could possibly go wrong? n Causes of Narcolepsy Uncertain, but appears
Introduction to Physiological Psychology Psych 260 Kim Sweeney ksweeney@cogsci.ucsd.edu cogsci.ucsd.edu/~ksweeney/psy260.html What could possibly go wrong? n Causes of Narcolepsy Uncertain, but appears
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Pain Management in the NICU. Tamorah Lewis MD, PhD
 Pain Management in the NICU & Iatrogenic Opiate Withdrawal Tamorah Lewis MD, PhD Assistant Professor Divisions of Neonatology & Clinical Pharmacology, Toxicology and Therapeutic Innovation The Children's
Pain Management in the NICU & Iatrogenic Opiate Withdrawal Tamorah Lewis MD, PhD Assistant Professor Divisions of Neonatology & Clinical Pharmacology, Toxicology and Therapeutic Innovation The Children's
Mechanisms of general anaesthesia. Nick Franks FRCA, FMedSci, FRS Imperial College London
 Mechanisms of general anaesthesia Nick Franks FRCA, FMedSci, FRS Imperial College London Etomidate Thiopental Propofol Halothane Isoflurane Sevoflurane Xenon Nitrous oxide Franks and Lieb Nature 367 607
Mechanisms of general anaesthesia Nick Franks FRCA, FMedSci, FRS Imperial College London Etomidate Thiopental Propofol Halothane Isoflurane Sevoflurane Xenon Nitrous oxide Franks and Lieb Nature 367 607
Brain dysfunction in the ICU
 High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
May 2013 Anesthetics SLOs Page 1 of 5
 May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
Effect of Noise Reduction Methods in the ICU on Sleep Quality. Veronica Tseng University of California, Irvine June 2016
 Effect of Noise Reduction Methods in the ICU on Sleep Quality Veronica Tseng University of California, Irvine June 2016 Introduction Sleep deprivation is a common problem in the critical care unit- in
Effect of Noise Reduction Methods in the ICU on Sleep Quality Veronica Tseng University of California, Irvine June 2016 Introduction Sleep deprivation is a common problem in the critical care unit- in
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Anxiolytic and Hypnotic drugs
 Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
General anesthetics. Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine
 General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
What you need to know about Delirium in ICU. Dr Valerie Page Watford General Hospital
 What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
EEG Sleep Circadian rhythms Learning Objectives: 121, 122
 EEG Sleep Circadian rhythms Learning Objectives: 121, 122 Zoltán Lelkes Electroencenphalography Hans Berger pen time amplifier electrodes 1 The waves of the EEG gamma > 30 Hz beta: 13-30 Hz Mental activity:
EEG Sleep Circadian rhythms Learning Objectives: 121, 122 Zoltán Lelkes Electroencenphalography Hans Berger pen time amplifier electrodes 1 The waves of the EEG gamma > 30 Hz beta: 13-30 Hz Mental activity:
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Unit 5. States of Consciousness
 Unit 5. States of Consciousness College Board - Acorn Book Course Description 2-4% And then suddenly, I saw this bright light at the end of the tunnel. Summary Outline A. Sleep and Dreaming B. Hypnosis
Unit 5. States of Consciousness College Board - Acorn Book Course Description 2-4% And then suddenly, I saw this bright light at the end of the tunnel. Summary Outline A. Sleep and Dreaming B. Hypnosis
States of Consciousness
 States of Consciousness On the Nature of Consciousness Awareness of and Stimuli Variations on levels of stream of consciousness unconscious Sleep/dreaming research A family of practices that train to heighten
States of Consciousness On the Nature of Consciousness Awareness of and Stimuli Variations on levels of stream of consciousness unconscious Sleep/dreaming research A family of practices that train to heighten
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Special Lecture 6 Effects of Sleep on Seizures ; A Path to sleep neurology (Somno-neurology)
") Special Lecture 6 Effects of Sleep on Seizures ; A Path to sleep neurology (Somno-neurology) Jun Kohyama, MD Tokyo Bay Urayasi/Ichikawa Medical Center Taiwan Pediatric Epilepsy Congress 2010 Dec. 26, 2010,
Special Lecture 6 Effects of Sleep on Seizures ; A Path to sleep neurology (Somno-neurology) Jun Kohyama, MD Tokyo Bay Urayasi/Ichikawa Medical Center Taiwan Pediatric Epilepsy Congress 2010 Dec. 26, 2010,
Sleep in ICU. Yuliya Boyko, Poul Jennum, Helle Oerding, Palle Toft
 Sleep in ICU Yuliya Boyko, Poul Jennum, Helle Oerding, Palle Toft Background: Why is sleep is important? Modulation of the immune system Regenerative processes Neurophysiological organisation Memory consolidation
Sleep in ICU Yuliya Boyko, Poul Jennum, Helle Oerding, Palle Toft Background: Why is sleep is important? Modulation of the immune system Regenerative processes Neurophysiological organisation Memory consolidation
From the Department of Pharmacy (JM, CAF) and Department of Pulmonary and Critical
 and Department of Pulmonary and Critical") PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD
 SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México
 Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients
Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Modules 7. Consciousness and Attention. sleep/hypnosis 1
 Modules 7 Consciousness and Attention sleep/hypnosis 1 Consciousness Our awareness of ourselves and our environments. sleep/hypnosis 2 Dual Processing Our perceptual neural pathways have two routes. The
Modules 7 Consciousness and Attention sleep/hypnosis 1 Consciousness Our awareness of ourselves and our environments. sleep/hypnosis 2 Dual Processing Our perceptual neural pathways have two routes. The
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Effect of Sedation With Dexmedetomidine vs Lorazepam on Acute Brain Dysfunction in Mechanically Ventilated Patients
 CARING FOR THE CRITICALLY ILL PATIENT Effect of Sedation With vs on Acute Brain Dysfunction in Mechanically Ventilated Patients The MENDS Randomized Controlled Trial Pratik P. Pandharipande, MD, MSCI Brenda
CARING FOR THE CRITICALLY ILL PATIENT Effect of Sedation With vs on Acute Brain Dysfunction in Mechanically Ventilated Patients The MENDS Randomized Controlled Trial Pratik P. Pandharipande, MD, MSCI Brenda
Status Epilepticus: Implications Outside the Neuro-ICU
 Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
ALCOHOL Other name(s): ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl
: ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl") Other name(s): ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl (OH) bound to carbon atoms. In EtOH, the carbon is in an ethyl
Other name(s): ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl (OH) bound to carbon atoms. In EtOH, the carbon is in an ethyl
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Chapter 5. Variations in Consciousness 8 th Edition
 Chapter 5 Variations in Consciousness 8 th Edition Consciousness: Personal Awareness Awareness of Internal and External Stimuli Levels of awareness James stream of consciousness Freud unconscious Sleep/dreaming
Chapter 5 Variations in Consciousness 8 th Edition Consciousness: Personal Awareness Awareness of Internal and External Stimuli Levels of awareness James stream of consciousness Freud unconscious Sleep/dreaming