COPD in Radiology, with a Focus on Bronchiectasis and Emphysema
|
|
|
- Tamsin Terry
- 6 years ago
- Views:
Transcription
1 November, 2002 COPD in Radiology, with a Focus on Bronchiectasis and Emphysema Evan Lyon, Harvard Medical School, Year IV Course Director
2 Why is COPD important? Its common: 30 million Americans living with chronic lung disease million American men and women have chronic bronchitis. Nearly 2 million have emphysema from a 1993 National Health Survey. It affects lives: 114 million days of restricted activity due to chronic bronchitis and emphysema in the same survey. This is 312,000 person / years lost. It can be fatal: In 1993, there were 95,900 deaths from COPD. This made it the 4 th leading cause of death in the United States. Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., 2000, pg and 2
3 Who is at risk for COPD? Smokers Tobacco smoke accounts for 80-90% of the risk for developing COPD. But only 10-15% of smokers develop clinically significant COPD. The reason for this remains unknown. Men > Women even when controlling for smoking. M + M is inversely proportional to socioeconomic status. COPD aggregates in families, even with alpha 1 -antitrypsin deficiency is excluded. Atopic Individuals are at increased risk for all forms of COPD, not just asthma. Occupational Hazards. Children of mother s who smoke, low birth weight, and frequent childhood pulmonary infections. Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., 2000, pg
4 Natural History of COPD FEV1 of < 0.8 L usually produces symptomatic dyspnea. Nonsmokers lose FEV 1 at an accelerating rate with age; the average loss is about 30 ml/year. 30 cigarettes/day average a slightly greater rate of decline. A susceptible smoker who stops smoking at age 50 loses function at the rate for nonsmokers. The ex-smoker on this graph delayed onset of dyspnea by 11 years after quitting at age 50. Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., 2000, pg. 2002, figure
5 Definitions Chronic bronchitis Epidemiologically = presence of chronic productive cough for 3 months in each of 2 successive years. No other underlying cause, e.g., M. tuberculosis, carcinoma of the lung, bronchiectasis, cystic fibrosis, and chronic congestive heart failure. Emphysema A condition of the lung characterized by abnormal, permanent enlargement of the air spaces distal to the terminal bronchiole, accompanied by destruction of their walls and without obvious fibrosis. RCoNA, 36:1, 1998 pg. 15. Asthma Asthma is a chronic inflammatory disorder of the airways. In susceptible individuals, this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing. These episodes are usually associated with widespread but variable airflow obstruction that is often reversible either spontaneously or with treatment. [Also with] bronchial hyperresponsiveness. M and N, pg Asthma must have limited air flow. Emphysema and chronic bronchitis may be diagnosed without air flow limitation. Bronchiectasis Morphologic definition = Permanent dilatation of bronchi. Cylindrical or tubular, vericose, and saccular or cystic. 5
6 Clinical History Cough is the most frequent symptom. Usually dyspnea causes patients to seek medical attention. Chronic bronchitis is the most common cause of hemoptysis in the United States. Usually in association with an infective episode. COPD is a functional / clinical diagnosis. Radiology can only suggest this diagnosis. Median survival in a Finnish population after the first hospital admission for COPD was 5.7 years. Respiration 64: , Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed.,

7 Complications 1 Bullae P.L. is a 45 year old woman, s/p thoroscopic right apex wedge resection for a small pulmonary nodule. Chest tube in place. Bullous changes in the left apex. BIDMC Exam Courtesy of Dr. Phil Boiselle. 7

8 Complications 1.1 Bullae Same patient as previous slide. CT shows extent of bullous changes in the left apex. Post-surgical changes are seen on the right. Patients with pulmonary bullae are at increased risk for pneumothorax and pulmonary infections. BIDMC Exam Courtesy of Dr. Phil Boiselle. 8
9 Complications - 2 Pneumothorax Patients with COPD have poor pulmonary reserve. Suspect pneumothroax in a patient with COPD who has sudden increase in symptoms. Spontaneous pneumothroax in a normal person is usually not dangerous; in COPD it can be life threatening. May be difficult to treat pneumothorax in COPD if there is a bronchopleural fistula. Remember expiration films can help clarify the diagnosis. Large bullae can mimic pneumothorax. Review old films! Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., 2000, pgs

10 Complications 2.1 Where is the abnormality? Pneumothroax in the LLL in a patient with moderate/severe COPD. Courtesy of Dr. Chad Brecher, Chief Resident BIDMC Radiology. 10
11 Complications - 3 Cor Pulmonale Alveolar hypoxia increased pulmonary vascular resistance. Emphysema also leads to loss of vascular bed. Acidemia locally in the lung can also contribute to increased pulmonary vascular pressures. Hypoxia erythrocytosis increased blood viscosity. Increased intrathoracic pressure secondary to air trapping may also increase right heart strain. Usually a minor effect. Diagnosis of Cor Pulmonale Can diagnose on CXR, EKG, palpation of the heart, prominent and split S2, etc. Rx = 0 2 acutely and at home. Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., 2000, pg
 and right pulmonary artery")
 and left (long black arrows) pulmonary")
12 Complications 3.1 PA shows enlargement of the main pulmonary artery (black arrow) and right pulmonary artery (black arrow). Peripheral pulmonary arteries are reduced in caliber. Lateral shows enlargement of both the right (short) and left (long black arrows) pulmonary arteries. White arrow shows right ventricular enlargement. 12
13 Complications - 4 Pneumonia Data are sparse, but generally agreed that pneumonia is more common in patients with COPD. All types of pneumonia seem to be increased. Evidence that treating with empiric antibiotics helps COPD flares??? Sleep Disorders Common and a major source of morbidity. Nighttime hypoxia may contribute to pulmonary hypertension. Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., 2000, pgs


14 Lung Anatomy Lung buds at 4 weeks Grey s Anatomy, plate 948 Lung buds a few divisions later Grey s Anatomy, plate 949 Trachea main stem bronchi segmental bronchi bronchioles respiratory bronchioles alveoli. There are 500,000 respiratory bronchioles. Each respiratory bronchiole has a diameter of 0.04cm. The area of respiratory bronchioles is 1000 cm 2. RCoNA 36:1, 1998 pg
15 Brochiectasis Bronchiectasis is irreversible dilatation of the bronchial tree. The disease may cause chronic sputum production and hempotysis or be may be asymptomatic. DDx is extensive. Morphological findings of bronchiectasis represent a final common pathway for many disease processes. Prevalence worldwide is unknown. Three morphologic types. 1. Cylindrical or tubular 2. Vericose 3. Saccular or cystic NEJM, 346: 18, pgs May 2,
16 Brochiectasis on Film - 1 ON CXR Loss of definition and increased number and size of bronchovascular markings. Thought secondary to peribronchial fibrosis and secretions. Loss of lung volume. Honeycombing. Cystic spaces up to 2cm. Bronchography introduced in 1922 was the gold standard for diagnosis until HRCT. NEJM, 346: 18, pgs May 2,

17 Brochiectasis on Film 1.1 BIDMC Patient A. H. is a 40 year old woman with mild bronchiectasis. Exam at BIDMC Moderate increase in lung markings, especially in the lingula which obscures the left heart border. No hilar or mediastinal lymphadenopathy. BIDMC 17

18 Brochiectasis on Film 1.2 Cylindrical and cystic bronchiectasis on PA and bronchography. Without bronchograpy, the increased markings on the PA film would have been difficult to interpret. Paul and Juhl's Essentials of Radiologic Imaging, 7th ed., Figure 26-8, Page


19 Brochiectasis on Film 1.3 BIDMC D.R. is 64 year old man with bronchiectasis. BIDMC exams BIDMC Courtesy of Dr. Phil Boiselle. 19

20 Brochiectasis on Film 1.4 S.M. is a 76 year old woman with bibasilar bronchiectasis in the setting of a hiatal hernia. Possibly the result of chronic aspiration. BIDMC Exam BIDMC 20
21 Brochiectasis on Film Diagnosis HRCT is the best modality for assessing bronchiectasis. Rule of Thumb Most reliable radiologic finding for cylindrical bronchiectasis is visualization of bronchi within 1 cm of pleura or visualization of bronchi abutting the mediastinal pleura. Lack of bronchial tapering and increased bronchoarterial ratios can help, but they occur in 10% to 20% of healthy subjects. 21

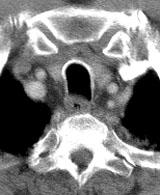
22 Bronchus < 1cm from pleura Patient A.H. is a 40 year old woman with bronchiectasis of unclear etiology. Note also that abnormal bronchi do not taper proximal to distal. BIDMC Exam at BIDMC 22


23 Bronchus / Pulmonary Artery Ratio Patient A. H. age 40 Bronchus at this level = 4.9mm Pulmonary Artery Branch = 3.1mm Ratio = 1.5 BIDMC Exam at BIDMC Pt. T. C. age 39 with a normal chest CT Bronchus at this level = 2.9 mm Pulmonary Artery Branch = 4.2 mm Ratio = 0.69 Exam at BIDMC BIDMC 23
24 Bronchiectasis on HRCT: Resolution matters. Conventional CT with 8-10mm collimation showed sensitivity of 60% to 80% and a specificity of 86% to 100%. HRCT with 1.5-mm collimation at 10-mm intervals improved sensitivity to a range of 96% to 98% with a specificity of 93% to 99%. With the use of 4-mm collimation at 5-mm intervals, CT scanning was 100% sensitive for the cystic and varicose types and 94% sensitive for the cylindrical variety. Fake Outs Artifacts from respiratory and cardiac motion. Inappropriate collimation and electronic windowing. Diffuse lung diseases such as pulmonary histiocytosis X, lymphangioleiomyomatosis, cystic changes in patients with AIDS and P. carinii pneumonia, and cystic metastases. Look for cyst next to an artery. This favors bronchiectasis over a cystic metastasis. Paul and Juhl's Essentials of Radiologic Imaging, 7th ed., Page
25 DDx of Bronchiectasis Aspergillus as part of allergic bronchopulmonary aspergillosis can contribute to broncheal destruction. Kartagener s Syndrome look for triad of situs abnormalities, nasal sinusitis, and bronchiectasis. CF is a common cause. In RA clinics, 1-3% of patients have clinical bronchiectasis. HRCT reveals 30% of RA patients with lung involvement. NEJM, 346: 18, pgs May 2, Table 1 from page


26 Segmental Anatomy Respiratory bronchiole Lymphatics and pulmonary veins Grey s Anatomy, Figs 975 and 976, from 26
27 Emphysema Up to 30% of the lung can be involved before symptoms occur. 66 of adults have emphysema at autopsy. Diagnosis on CR from 65-80%. CT is more sensitive for diagnosis that CR or PFTs, but consistently underestimates when compared to pathology. CR can see emphysema before it becomes symptomatic. 3 types, in reference to the secondary lobule. Centrilobular or Centriacinar. Panlobular or Panacinar. Paraseptal or Distal Lobular or Subpleural. Paracicatricial empysema also exists in the setting of pulmonary fibrosis, but this is a different diagnosis. Dilation of acinii from scarring. Emphysema can be either focal or diffuse within the lung. Paul and Juhl's Essentials of Radiologic Imaging, 7th ed., Page
28 Radiologic Criteria for Emphysema Criteria for chest radiographic diagnosis of emphysema include two or more of the following: 1. Depression and flattening of the diaphragm on the posteroanterior roentgenogram with blunting of costophrenic angles. The actual level of the diaphragm is not as significant as the contour. (This can be determined from a straight line connecting the costophrenic junction to the vertebrophrenic junction on each side; if the highest level of the contour is less than 1.5 cm above this line, the diaphragm can be recorded as flat.) 2. Irregular radiolucency of the lung, caused by irregularity in distribution of the emphysematous tissue destruction 3. Abnormal retrosternal radiolucency, as seen on lateral view, measuring 2.5 cm or more from the sternum to the most anterior margin of the ascending aorta 4. Flattening or even concavity of the diaphragm contour on the lateral chest radiograph, as determined by the presence of a sternodiaphragmatic angle of 90 or larger. Paul and Juhl's Essentials of Radiologic Imaging, 7th ed., Page
29 Emphysema in Radiology Decreased vascular markings suggests emphysema. When combined with hyperinflation, specificity of diagnosis increases. Saber-sheath Trachea. Sagital diameter or trachea is larger than coronal diameter. Sagital / coronal ratio of 2:1 to diagnose the finding. Measured 1cm above the the aortic arch. 95 percent of patients with saber-sheath trachea have clinical or physiologic COPD. Contrast this with 18 percent of controls (normal trachea) in the study population. Automated density mask programs assessing HRCT images for emphysema and comparing inspiration / expiration films are currently being researched as a method to quantify emphysematous changes. This is not in clinical practice, but may replace PFTs for quantification of all forms of COPD. RCoNA 36:1,

30 Examples Patient P. J. is a 65 year old man with emphysema, DM, neuropathy, and HTN. Exam at BIDMC BIDMC Rule of thumb: sternodiaphragmatic angle < 90% suggests COPD. 30

31 Example What s Abnormal? Patient D.V., a 61 year old woman with emphysema. Exam Ignore this for the moment. BIDMC 31

32 Examples What abnormalities do you see? Increased Retrosternal Radiolucency. 3.6cm. Flattened Diaphragm BIDMC Patient D.V., a 61 year old woman with emphysema. Exam 32





33 Saber-sheath Trachea Normal Saber-sheath trachea 33
34 Centrilobular Emphysema Paradigm = SMOKING. Smoking raises alpha1-antitrypsin levels by 20 percent. Other toxic exposures may produce this pattern. Tends to effect the upper and posterior portions of the lung, sparing the lower portions. Normal bronchial anatomy. Diagrams from RCoNA 36:1, 1998 pg. 16. Centrilobular Emphysema 34


35 J.C., a 71 year-old Smoker with Emphysema BIDMC exam BIDMC BIDMC Patient has bilateral pleural effusions and bibasilar consolidation, suspicious for pneumonia. For emphysema in a smoker, our attention is to the apices. Compliments of Dr. Chad Brecher, Chief Resident BIDMC Radiology. 35

36 CT with Centrilobular Emphysema J.C., age 71. BIDMC exam BIDMC Courtesy of Dr. Chad Brecher, Chief Resident BIDMC Radiology. 36

37 CT with Centrilobular Emphysema J.C., age 71. Worse at the apices. BIDMC exam BIDMC Courtesy of Dr. Chad Brecher, Chief Resident BIDMC Radiology. 37

38 Bullous Emphysema on HRCT Peripheral Bullae from centrilobular emphysema. Arrows represent preserved lung tissue and vessels Image from RCoNA 36:1, 1998 pg. 45, figure

39 Panacinar Emphysema Paradigm = alpha 1 -antitrypsin deficiency. Tends to effect lower lung > upper lung. Can be focal behind an obstruction or congenital bronchial abnromality or diffuse. Photograph: cut surface of inflation-fixed lung. Diagram from RCoNA 36:1, 1998 pg. 16. Murray & Nadel: Textbook of Respiratory Medicine, 3rd ed., Figure 38-13, Page


40 Panacinar Emphysema due to alpha 1 -antitrypsin deficiency J.C. is a 51 year old man with alpha 1 -antitrypsin deficiency and severe emphysema. BIDMC Exam BIDMC BIDMC Courtesy of Dr. Phil Boiselle. 40

41 Panacinar Emphysema on CT Pt. J.C. at age 51. Extensive emphysema at the apices. BIDMC exam BIDMC Courtesy of Dr. Phil Boiselle. 41

42 Panacinar Emphysema on CT Pt. J.C. at age 51. Even more extensive emphysema at the bases. BIDMC exam BIDMC Courtesy of Dr. Phil Boiselle. 42
43 Paraseptal Emphysema Emphysema along fibrous intralobar septa. Remainder of the lung is spared. Usually no airflow compromise. Apical bullae can give rise to spontaneous pneumothroax. 43
44 Conclusions Rules of Thumb General Look for hyperinflation. Explain all bullae. Greater than expected lucency on PA chest radiograph, especially if focal or patchy should make one suspicious for COPD. Bronchiectasis Bronchi visible less than 1cm from the periphery or abutting the mediastinum. Increased bronchi / vascular ratio. Emphysema Retrosternal radiolucency of greater than 2.5 cm. Flattening or concavity of the diaphragm on the lateral chest radiograph: sternodiaphragmatic angle of 90 or larger. 44
45 References Radiologic Clinics of North America. Volume 36, Number 1. January Imaging of Obstructive Pulmonary Disease. W. Richard Webb, Guest Editor. Paul and Juhl's Essentials of Radiologic Imaging, Seventh Edition John Juhl, Andrew Crummy, and Janet Kuhlman, eds. Lippincott Williams and Wiklins, Philadelphia and New York. Textbook of Respiratory Medicine, Third Edition John Murray and Jay Nadel, eds. W.B. Saunders Company, Philadelphia. Barker, A.F. Bronchiectasis. New England Journal of Medicine - 2-May-2002; 346(18): Pulmonary Arterial Hypertension. Valerie L Ward, MD and Robert D Pugatch, MD, June 10, 1997 at Diagnosis for Case of the Week - September 20, Virginia Commonwealth University Medical School. 45
46 Thanks Phil Boiselle, MD for images. Chad Brecher, MD for images. for guidance and for organizing this radiology clerkship Larry Barbaras and Cara Lyn D amour for putting these presentations on the web. Pamela Lepkowski for EVERYTHING else 46
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA INTRODUCTION In this lecture we will discuss atelectasis which is a complication of several medical and surgical
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA INTRODUCTION In this lecture we will discuss atelectasis which is a complication of several medical and surgical
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Radiologic-pathologic correlation of pulmonary diseases
 The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
Undergraduate Teaching
 Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Atopic Pulmonary Disease: Findings on Thoracic Imaging
 July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
July 2003 Atopic Pulmonary Disease: Findings on Thoracic Imaging Rebecca G. Breslow Harvard Medical School Year IV Churg-Strauss Syndrome Hypersensitivity Pneumonitis Asthma Atopic Pulmonary Disease Allergic
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC
 Interpretation Brent Burbridge, MD, FRCPC") Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
8/14/2017. Objective: correlate radiographic findings of common lung diseases to actual lung pathologic features
 What is that lung disease? Pulmonary Patterns & Correlated Pathology Dr. Russell Tucker, DACVR Objective: correlate radiographic findings of common lung diseases to actual lung pathologic features Improved
What is that lung disease? Pulmonary Patterns & Correlated Pathology Dr. Russell Tucker, DACVR Objective: correlate radiographic findings of common lung diseases to actual lung pathologic features Improved
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Chest and cardiovascular
 Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
A Case of Pediatric Plasma Cell Granuloma
 August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Radiology of the respiratory disease
 Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
SURGERY FOR GIANT BULLOUS EMPHYSEMA
 SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease
 Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Exam 2 Respiratory Disorders
 Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Workshop Cyst & Lucency. How to Approach
 Workshop Cyst & Lucency How to Approach To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt
Workshop Cyst & Lucency How to Approach To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt
Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis?
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 12 Number 1 Swyer-James Syndrome: An Infrequent Cause Of Bronchiectasis? A Huaringa, S Malek, M Haro, L Tapia Citation A Huaringa, S Malek, M
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
Group B: Directed self-study Group C: Anatomy lab. Lecture: Structure and function of larynx. Lecture: Dead space & compliance of lungs
 Timetable Week 1 (1 st January 2018) Theme: Structure and functions of the lungs Group A: Anatomy lab Group C: Histology lab Upper Group B: Anatomy lab Group C: Anatomy lab Group A: Histology lab Upper
Timetable Week 1 (1 st January 2018) Theme: Structure and functions of the lungs Group A: Anatomy lab Group C: Histology lab Upper Group B: Anatomy lab Group C: Anatomy lab Group A: Histology lab Upper
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Disease spectrum. IPA Invasive pulmonary aspergillosis
 Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Aspergillus & ABPA Disease spectrum IPA Invasive pulmonary aspergillosis ABPA ABPA pathophysiology conidia of Aspergillus trapped in mucous and narrowed airways of asthmatics/cf germinate to form hyphae
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities
 Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
The Respiratory System. Dr. Ali Ebneshahidi
 The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
How does COPD really work?
 How does COPD really work? by Alex Goodell View online Where does COPD fit in the mix of respiratory diseases? I ve made a map of the major pathologies outlined in Robbins and First Aid (obviously these
How does COPD really work? by Alex Goodell View online Where does COPD fit in the mix of respiratory diseases? I ve made a map of the major pathologies outlined in Robbins and First Aid (obviously these
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
HRCT Versus Volume Rendering (Three Colors, Three Densities Lung Images) in Diagnosis of Small Airway Disease: A Comparative Study
 in Diagnosis of Small Airway Disease: A Comparative Study") Med. J. Cairo Univ., Vol. 84, No. 1, March: 359-364, 2016 www.medicaljournalofcairouniversity.net HRCT Versus Volume Rendering (Three Colors, Three Densities Lung Images) in Diagnosis of Small Airway Disease:
Med. J. Cairo Univ., Vol. 84, No. 1, March: 359-364, 2016 www.medicaljournalofcairouniversity.net HRCT Versus Volume Rendering (Three Colors, Three Densities Lung Images) in Diagnosis of Small Airway Disease:
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Interactive Lecture. Lecture 7 - Interactive. Radiology of cardiorespiratory disease. Editing File. Done By. Color Coding Important Notes Extra
 Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Introduction to Chest Radiography
 Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Pediatric High-Resolution Chest CT
 Pediatric High-Resolution Chest CT Alan S. Brody, MD Professor of Radiology and Pediatrics Chief, Thoracic Imaging Cincinnati Children s s Hospital Cincinnati, Ohio, USA Pediatric High-Resolution CT Short
Pediatric High-Resolution Chest CT Alan S. Brody, MD Professor of Radiology and Pediatrics Chief, Thoracic Imaging Cincinnati Children s s Hospital Cincinnati, Ohio, USA Pediatric High-Resolution CT Short
ARTICLE IN PRESS. Ahuva Grubstein a, Daniele Bendayan b, Ithak Schactman c, Maya Cohen a, David Shitrit b, Mordechai R. Kramer b,
 Respiratory Medicine (2005) 99, 948 954 Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature
Respiratory Medicine (2005) 99, 948 954 Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
CASE REPORTS. Idiopathic Unilateral Hyperlucent Lung
 CASE REPORTS Idiopathic Unilateral Hyperlucent Lung The Swyer-James Syndrome J. Judson McNamara, M.D., Harold C. Urschel, M.D., J. H. Arndt, M.D., Herman Ulevitch, M.D., and W. B. Kingsley, M.D. I diopathic
CASE REPORTS Idiopathic Unilateral Hyperlucent Lung The Swyer-James Syndrome J. Judson McNamara, M.D., Harold C. Urschel, M.D., J. H. Arndt, M.D., Herman Ulevitch, M.D., and W. B. Kingsley, M.D. I diopathic
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Obstructive Lung Diseases. By: Shefaa Qa qa
 Obstructive Lung Diseases By: Shefaa Qa qa Obstructive lung diseases (or airway diseases) are characterized by an increase in resistance to airflow due to partial or complete obstruction at any level from
Obstructive Lung Diseases By: Shefaa Qa qa Obstructive lung diseases (or airway diseases) are characterized by an increase in resistance to airflow due to partial or complete obstruction at any level from
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
HASPI Medical Anatomy & Physiology 14b Lab Activity
 HASPI Medical Anatomy & Physiology 14b Lab Activity Name(s): Period: Date: Respiratory Distress Respiratory distress is a broad medical term that applies to any type of breathing difficulty and the associated
HASPI Medical Anatomy & Physiology 14b Lab Activity Name(s): Period: Date: Respiratory Distress Respiratory distress is a broad medical term that applies to any type of breathing difficulty and the associated
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Evaluation of the chest Part II.
 Evaluation of the chest Part II. Nagy Endre SZEGEDI TUDOMÁNYEGYETEM ÁOK, RADIOLÓGIAI KLINIKA, SZEGED ANATOMY parenchyma: alveoloacinar system, pulmonary arteries and veins interstitium: connective tissues
Evaluation of the chest Part II. Nagy Endre SZEGEDI TUDOMÁNYEGYETEM ÁOK, RADIOLÓGIAI KLINIKA, SZEGED ANATOMY parenchyma: alveoloacinar system, pulmonary arteries and veins interstitium: connective tissues
Web Chapter 3. Image Gallery: Lesion detection on low dose chest CT
 Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Pulmonary Sequestration
 July 26, 2004 Pulmonary Sequestration Jonathan Shaw, Harvard Medical School Year IV What do these two patients have in common? Patient 1: 50 y.o. non-smoking female with several months cough and hemoptysis;
July 26, 2004 Pulmonary Sequestration Jonathan Shaw, Harvard Medical School Year IV What do these two patients have in common? Patient 1: 50 y.o. non-smoking female with several months cough and hemoptysis;
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Disclosure. Clinical Chest Radiography Interpretation Part I
 Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
The Respiratory System
 The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
The Respiratory System Respiratory Anatomy Upper respiratory tract Nose Nasal passages Pharynx Larynx Respiratory Anatomy Functions of the upper respiratory tract: Provide entry for inhaled air Respiratory
Cystic Lung Disease: a Comparison of Cystic Size, as Seen on Expiratory and Inspiratory HRCT Scans
 Cystic Lung Disease: a Comparison of Cystic Size, as Seen on Expiratory and Inspiratory HRCT Scans Ki-Nam Lee, MD 1 Seong-Kuk Yoon, MD 1 Seok Jin Choi, MD 2 Jin Mo Goo, MD 3 Kyung-Jin Nam, MD 1 Index words:
Cystic Lung Disease: a Comparison of Cystic Size, as Seen on Expiratory and Inspiratory HRCT Scans Ki-Nam Lee, MD 1 Seong-Kuk Yoon, MD 1 Seok Jin Choi, MD 2 Jin Mo Goo, MD 3 Kyung-Jin Nam, MD 1 Index words:
High resolution computed tomography (HRCT) assessment of β 2 -agonist induced bronchodilation in chronic obstructive pulmonary disease patients
 assessment of β 2 -agonist induced bronchodilation in chronic obstructive pulmonary disease patients") European Review for Medical and Pharmacological Sciences High resolution computed tomography (HRCT) assessment of β 2 -agonist induced bronchodilation in chronic obstructive pulmonary disease patients
European Review for Medical and Pharmacological Sciences High resolution computed tomography (HRCT) assessment of β 2 -agonist induced bronchodilation in chronic obstructive pulmonary disease patients
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Assignable revenue codes: Explanation of services:
 computed tomography Chest/Cardiac Assignable revenue codes: Explanation of services: 0350 CT Scan General Classification 0351 CT Scan Head Scan 0352 CT Scan Body Scan 0359 CT Scan Other CT Scans Known
computed tomography Chest/Cardiac Assignable revenue codes: Explanation of services: 0350 CT Scan General Classification 0351 CT Scan Head Scan 0352 CT Scan Body Scan 0359 CT Scan Other CT Scans Known
Elderly Man with Dyspnoea
 Asia Pacific Family Medicine, 2004; 3 (1-2): 46-50 RADIOLOGY SERIES Elderly Man with Dyspnoea Wei-Yang LIM Faculty of Medicine National University of Singapore, Singapore Wilfred CG PEH Singapore Health
Asia Pacific Family Medicine, 2004; 3 (1-2): 46-50 RADIOLOGY SERIES Elderly Man with Dyspnoea Wei-Yang LIM Faculty of Medicine National University of Singapore, Singapore Wilfred CG PEH Singapore Health
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
The Upper Airway. Trachea. The Human Airway. Nasopharynx Oropharynx Larynx
 The Human Airway (with thanks to David N. Hager, MD, PhD Johns Hopkins University) The Upper Airway Nasopharynx Oropharynx Larynx voice airflow Gray, Anatomy of the Human Body Trachea Length: 9-15 cm Internal
The Human Airway (with thanks to David N. Hager, MD, PhD Johns Hopkins University) The Upper Airway Nasopharynx Oropharynx Larynx voice airflow Gray, Anatomy of the Human Body Trachea Length: 9-15 cm Internal
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH