BEFORE the session. Sodium & Water Assessment & Therapeutics. LMPS Residents
|
|
|
- Stephanie Morton
- 5 years ago
- Views:
Transcription
1 BEFORE the session 1. Get Loewen s Sodium & Water Assessment & Therapeutics 1-pager at 2. Read McGee S, Abernethy WB, Simel DL. Is this patient hypovolemic? JAMA 1999;281: Install MedCalX, QxCalculate, Medal, Mediquations, or equivalent on your phone and find these calculators in there: Water deficit or Free water deficit Change in serum sodium Fractional excretion of Na LMPS Residents Sodium & Water Assessment & Therapeutics Dr. Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP, RPh Associate Professor, University of British Columbia peter.loewen@ubc.ca
2 Why does it matter? Your patient is on multiple antihypertensives and today complains of dizziness on rising. BP reasonably well controlled. Should you decrease the dose of an antihypertensive? Your patient with Parkinson's disease seems to be developing postural hypotension. Does he need midodrine? You're consulted about a patient with severe hyponatremia and recent SSRI initiation. Is the hyponatremia drug-induced? Your CHF patient needs to be started on ACE-I. Her SCr is 155. How worried about a rise in SCr upon starting ACE-I are you? Your CHF patient is stable on ramipril 10mg, B-blocker, and furosemide 40mg. Lately his SCr has been creeping up. Physicians intends to decrease the ramipril dose because everybody knows ACE-I can cause renal failure. Is this a good idea? Your patient with HTN is admitted to hospital with CAP and has a serum Na of 129. Admitting physicians documents that the patient's HCTZ is being held due to "HCTZinduced hyponatremia" and that it should not be restarted. Is this sensible? Your patient has recurrent angina despite amlodipine+ntg patch. You believe metoprolol will be indicated, but are worried about his standing BP of 110/70 and postural drop. Can his anti-ischemic therapy be augmented? Ever been asked to "please procure some demeclocycline"? Know what tolvaptan is? Your vancomycin-treated patient is starting to show signs of GFR decline. Is it due to vancomycin? BY THE END OF THE SESSION, AND UPON REFLECTION & PRACTICE, STUDENTS SHOULD BE ABLE TO 1.Describe the difference between water and volume, dehydration, and volume depletion 2.Using physical assessment and laboratory parameters, diagnose the type of water-related defect a patient exhibits (e.g. hypovolemia, hyponatremia, hypernatremia, SIADH) 3.Demonstrate an APPROACH to evaluating water-related problems in a patient and their potential causes 4.Design a detailed therapeutic plan for treating the water-related disorder, including: Selecting and writing orders for an appropriate crystalloid solution (if required) or other drug therapy. Quantitative determination of quantities of crystalloid required and infusion rates Writing orders for (or conducting themselves) an appropriate monitoring plan.
3 The Plan Concepts Approach to assessing our patients Therapeutic options for our patients Treatment plans hypovolemia hypernatremia hyponatremia hypervolemia
4 To deepen and reinforce your knowledge & skill:
5 Where s your water? Total body water (TBW) = 0.6* x total body weight *More precisely: 0.45 for elderly female, 0.5 for non-elderly female or elderly male, 0.6 for non-elderly male. Intracellular fluid (ICF) Intracellular osmolality must be maintained for cells to function. Plasma osmolality will be sacrificed in either direction to achieve this. H2O freely crosses cell membranes. Na+ doesn t. Intracellular osmoles are mostly large proteins that don t move. H 2 O cell membrane Extracellular fluid (ECF) interstitial water 2/3 1/3 H 2 O Na+ intravascular water 3/4 1/4 Biological Imperatives maintain BP maintain intracellular environment (ph, temperature, osmolality)
.")
 INEFFECTIVE OSMOLES urea ethanol methanol Spasovski G, et al. Eur J Endocrinol. 2014 Feb 4;170(3):G1 G47.")
6 tonicity= the effective osmolality and is equal to the sum of the concentrations of the solutes which have the capacity to exert an osmotic force across the membrane ( effective osmoles ). Intracellular fluid (ICF) proteins Extracellular fluid (ECF) Na+ albumin EFFECTIVE OSMOLES Na K glucose mannitol (proteins - not solutes, but very effective) INEFFECTIVE OSMOLES urea ethanol methanol Spasovski G, et al. Eur J Endocrinol Feb 4;170(3):G1 G47. Words matter hypervolemia excess excess ICF hyponatremia euvolemia ECF ICF hypovolemia depletion dehydration
7 CASE 1: RK CASE 1: RK RK is an 83 y/o F admitted to your medical unit from assisted living with a 5-day history of coughing, difficulty breathing and increasing confusion. HPI: RK was in her usual state of health until one week ago when she developed what appeared to be an URTI. Her cough gradually got worse, being occasionally productive of yellowish sputum. She became increasingly confused over the following days. PMH: Stroke 6 months ago with some residual R sided weakness, Mild HTN, GERD, OA (knees) O/E: Wt. 50 kg (usually 54 kg), Temp 40C. Chest dull to auscultation and percussion. RR 27. Oriented x 1. CXR shows some RLL consolidation.
8 CASE 2: KP CASE 2: KP KP is a 77 y/o M brought to your urgent care center from home because of increasing lethargy and confusion over the past 48 hours. HPI: He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for isolated systolic hypertension. PMH: HTN. CAP. O/E: Oriented x 3. ~80kg. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. JVP <2cm ASA.
9 CASE 3: BW CASE 3: BW BW is a 67 y/o white M who presents to your primary care clinic complaining of general malaise and increasing confusion for one week. PMH: - Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago - Mild HTN x 5 y (metoprolol 100 mg po bid) - Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d) O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA.
10 Assessing your patient
11



12 Postural changes wait 1 minute! 2 minutes severe dizziness or HR 30 bpm or SBP 20 mmhg McGee S et al. JAMA. 1999;281: JVP
13
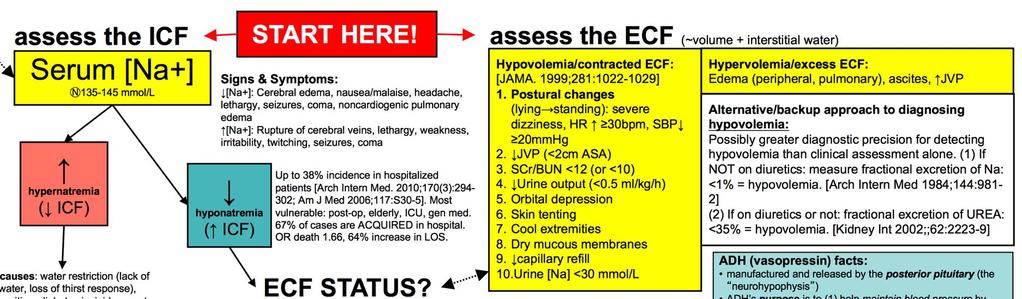
14 Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF) Why does serum [Na+] reflect ICF and what does it mean? H2O goes in Serum [Na+] is the best reflection of ICF status. Expanded ICF [Na+], or [Na+] reflects ICF Intracellular tonicity decreases ICF Need to maintain normal intracellular tonicity H2O moves ECF [Na+] Contracted ICF [Na+], or [Na+] reflects ICF H2O leaves [loop diuretics, fever] ICF Intracellular tonicity increases Need to maintain normal intracellular tonicity ECF H2O moves [Na+]
15 How does excess ICF cause hyponatremia? ICF ECF H2O goes in Intracellular tonicity decreases Need to maintain normal intracellular tonicity H2O moves [Na+] IV How does loss of ICF cause hypernatremia? H2O leaves [loop diuretics, fever] ICF Need to Intracellular maintain tonicity normal increases intracellular tonicity ECF H2O moves [Na+] IV
16 CASE 1: RK CASE 1: RK RK is an 83 y/o F admitted to your medical unit from assisted living with a 5-day history of coughing, difficulty breathing and increasing confusion. HPI: RK was in her usual state of health until one week ago when she developed what appeared to be an URTI. Her cough gradually got worse, being occasionally productive of yellowish sputum. She became increasingly confused over the following days. PMH: Stroke 6 months ago with some residual R sided weakness, Mild HTN, GERD, OA (knees) O/E: Wt. 50 kg (usually 54 kg), Temp 40C. Chest dull to auscultation and percussion. RR 27. Oriented x 1. CXR shows some RLL consolidation.
17 CASE 1: RK Questions about what you see here? What prompts you to be concerned about a Na/H2O problem? What is your APPROACH to assessing RK from a Na/H2O viewpoint? CASE 1: RK Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF)
18 CASE 1: RK CASE 1: RK What s your ASSESSMENT?
19 CASE 2: KP CASE 2: KP KP is a 77 y/o M brought to your urgent care center from home because of increasing lethargy and confusion over the past 48 hours. HPI: He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for isolated systolic hypertension. PMH: HTN. CAP. O/E: Oriented x 3. ~80kg. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. JVP <2cm ASA.
20 CASE 2: KP Questions about what you see here? What prompts you to be concerned about a Na/H2O problem? What is your APPROACH to assessing KP from a Na/H2O viewpoint? CASE 2: KP Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF)
21 CASE 2: KP CASE 2: KP What s your ASSESSMENT?
22 CASE 3: BW CASE 3: BW BW is a 67 y/o white M who presents to your primary care clinic complaining of general malaise and increasing confusion for one week. PMH: - Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago - Mild HTN x 5 y (metoprolol 100 mg po bid) - Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d) O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA.
23 CASE 3: BW Questions about what you see here? What prompts you to be concerned about a Na/H2O problem? What is your APPROACH to assessing BW from a Na/H2O viewpoint? CASE 3: BW Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF)
24 CASE 3: BW CASE 3: BW What s your ASSESSMENT? Why is this happening to BW? What other tests do we look at?
25 TRAP Treating deficiencies of ECF and ICF
26 CRYSTALLOIDS COLLOIDS
27 Osmolality of IV fluids matters. Why?
![Another perspective on crystalloids Normal plasma osmolality: 275-295 mosm/kg (~mmol/kg, ~mmol/l) Normal serum [Na+]: 135-145 meq/l Osmolality (mosm/l) [Na] ( & Cl) (meq/l) Dextrose](/docs-images/86/93658861/images/28-0.jpg "(g/l) NS (0.")
28 Another perspective on crystalloids Normal plasma osmolality: mosm/kg (~mmol/kg, ~mmol/l) Normal serum [Na+]: meq/l Osmolality (mosm/l) [Na] ( & Cl) (meq/l) Dextrose (g/l) NS (0.9% NaCl) Cal/L D5W /2NS D5-1/2NS /3D5-1/3NS % NaCl Seawater ~1000 ~475 Gatorade 365 ~20 ~220
29 Oral rehydration 413 mg of Na = 18 meq
30 CASE 1: RK CASE 1: RK RK is an 83 y/o F admitted to your medical unit from assisted living with a 5-day history of coughing, difficulty breathing and increasing confusion. HPI: RK was in her usual state of health until one week ago when she developed what appeared to be an URTI. Her cough gradually got worse, being occasionally productive of yellowish sputum. She became increasingly confused over the following days. PMH: Stroke 6 months ago with some residual R sided weakness, Mild HTN, GERD, OA (knees) O/E: Wt. 50 kg (usually 54 kg), Temp 40C. Chest dull to auscultation and percussion. RR 27. Oriented x 1. CXR shows some RLL consolidation.

31 CASE 1: RK Managing RK s Na & H2O issues: 1. Treat the HYPOVOLEMIA 2. Treat the HYPERNATREMIA CASE 1: RK Managing RK s Na & H2O issues: 1. Treat the HYPOVOLEMIA

32 CASE 1: RK Managing RK s Na & H2O issues: 2. Treat the HYPERNATREMIA CASE 1: RK Managing RK s Na & H2O issues: 2. Treat the HYPERNATREMIA
33 CASE 1: RK Orders for RK: Monitoring Plan: CASE 1: RK Orders for RK: 1. NS 500mL IV over 60mins 2. reassess 60mins 3. when euvolemic, start D5W ml/h Monitoring Plan: - serum electrolytes 8h after starting D5W infusion (target Na+?), frequency TBA thereafter - adjust infusion to achieve 0.5 mmol/l/h drop in serum [Na+] - continue until serum [Na+] ~145 and normal PO water intake
34 CASE 2: KP CASE 2: KP KP is a 77 y/o M brought to your urgent care center from home because of increasing lethargy and confusion over the past 48 hours. HPI: He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for isolated systolic hypertension. PMH: HTN. CAP. O/E: Oriented x 3. ~80kg. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. JVP <2cm ASA.

35 CASE 2: KP Managing KP s Na & H2O issues: 1. Treat the HYPOVOLEMIA CASE 2: KP Managing KP s Na & H2O issues: 1. Treat the HYPOVOLEMIA
36 CASE 2: KP Orders for KP: Monitoring Plan: CASE 2: KP Orders for KP: 1. NS 500mL IV over 30mins 2. reassess 30mins Monitoring Plan: - serum electrolytes in 4h - decide whether to admit - manage the diarrhea - decide re: antibiotic, CAP status
37 CASE 3: BW CASE 3: BW BW is a 67 y/o white M who presents to your primary care clinic complaining of general malaise and increasing confusion for one week. PMH: - Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago - Mild HTN x 5 y (metoprolol 100 mg po bid) - Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d) O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA.


38 CASE 3: BW Managing BW s Na & H2O issues CASE 3: BW Orders for BW: Monitoring Plan:

39 CASE 3: BW Orders for BW: 1. D/C fluoxetine 2. water restriction <500mL/d 3. liberalize salt in diet >10g/d Monitoring Plan: - decide whether to refer him for possible admission, home environment, supportive care - choose an alternate antidepressant, depending on response to fluoxetine so far - daily serum electrolytes until Na steadily rising - daily assessment of confusion CASE 3: BW ADVANCED TOPIC: what if BW had severe symptoms of hyponatremia and we wanted to give 3%NaCl IV to raise his serum [Na+] quickly?
40 CASE 3: BW ADVANCED TOPIC: what if BW had severe symptoms of hyponatremia and we wanted to give 3%NaCl IV to raise his serum [Na+] quickly?
41 To deepen and reinforce your knowledge & skill:

42 Why does it matter? Your patient is on multiple antihypertensives and today complains of dizziness on rising. BP reasonably well controlled. Should you decrease the dose of an antihypertensive? Your patient with parkinson's disease seems to be developing postural hypotension. Does he need midodrine? You're consulted about a patient with severe hyponatremia and recent SSRI initiation. Is the hyponatremia druginduced? Your CHF patient needs to be started on ACE-I. Her SCr is 155. How worried about a rise in SCr upon starting ACE-I are you? Your CHF patient is stable on ramipril 10mg, B-blocker, and furosemide 40mg. Lately his SCr has been creeping up. Physicians intends to decrease the ramipril dose because everybody knows ACE-I can cause renal failure. Is this a good idea? Your patient with HTN is admitted to hospital with CAP and has a serum Na of 129. Admitting physicians documents that the patient's HCTZ is being held due to "HCTZ-induced hyponatremia" and that it should not be restarted. Is this sensible? Your patient has recurrent angina despite amlodipine+ntg patch. You believe metoprolol will be indicated, but are worried about his standing BP of 110/70 and postural drop. Can his anti-ischemic therapy be augmented? Ever been asked to "please procure some demeclocycline"? Know what tolvaptan is? Your vancomycin-treated patient is starting to show signs of GFR decline. Is it due to vancomycin? Learning Objectives/Outcomes
43 The Plan Concepts Approach to assessing our patients Therapeutic options for our patients Treatment plans hypovolemia hypernatremia hyponatremia hypervolemia
44 Where s your water? Total body water (TBW) = 0.6* x total body weight *More precisely: 0.45 for elderly female, 0.5 for non-elderly female or elderly male, 0.6 for non-elderly male. Intracellular fluid (ICF) Extracellular fluid (ECF) Intracellular osmolality must be maintained for cells to function. Plasma osmolality will be sacrificed in either direction to achieve this. H2O freely crosses cell membranes. Na+ doesn t. Intracellular osmoles are mostly large proteins that don t move. H 2 O cell membrane interstitial water H 2 O Na+ intravascular water 2/3 1/3 3/4 1/4
45 Biological Imperatives maintain BP maintain intracellular environment (ph, temperature, osmolality) tonicity= the effective osmolality and is equal to the sum of the concentrations of the solutes which have the capacity to exert an osmotic force across the membrane ( effective osmoles ). Intracellular fluid (ICF) proteins Extracellular fluid (ECF) Na+ albumin EFFECTIVE OSMOLES Na K glucose mannitol (proteins - not solutes, but very effective) INEFFECTIVE OSMOLES urea ethanol methanol Spasovski G, et al. Eur J Endocrinol Feb 4;170(3):G1 G47.

46 Words matter hypervolemia excess excess ICF hyponatremia euvolemia ECF ICF hypovolemia depletion dehydration CASE 1: RK
47 CASE 1: RK RK is an 83 y/o F admitted to your medical unit from assisted living with a 5-day history of coughing, difficulty breathing and increasing confusion. HPI: RK was in her usual state of health until one week ago when she developed what appeared to be an URTI. Her cough gradually got worse, being occasionally productive of yellowish sputum. She became increasingly confused over the following days. PMH: Stroke 6 months ago with some residual R sided weakness, Mild HTN, GERD, OA (knees) O/E: Wt. 50 kg (usually 54 kg), Temp 40C. Chest dull to auscultation and percussion. RR 27. Oriented x 1. CXR shows some RLL consolidation. CASE 2: KP
48 CASE 2: KP KP is a 77 y/o M brought to your urgent care center from home because of increasing lethargy and confusion over the past 48 hours. HPI: He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for isolated systolic hypertension. PMH: HTN. CAP. O/E: Oriented x 3. ~80kg. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. JVP <2cm ASA. CASE 3: BW
49 CASE 3: BW BW is a 67 y/o white M who presents to your primary care clinic complaining of general malaise and increasing confusion for one week. PMH: - Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago - Mild HTN x 5 y (metoprolol 100 mg po bid) - Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d) O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA. Assessing your patient

50
51
52 Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF)
53 Why does serum [Na+] reflect ICF and what does it mean? H2O goes in Serum [Na+] is the best reflection of ICF status. Expanded ICF [Na+], or [Na+] reflects ICF Intracellular tonicity decreases ICF Need to maintain normal intracellular tonicity H2O moves ECF [Na+] Contracted ICF [Na+], or [Na+] reflects ICF H2O leaves [loop diuretics, fever] ICF Intracellular tonicity increases Need to maintain normal intracellular tonicity H2O moves ECF [Na+] How does excess ICF cause hyponatremia? ICF ECF H2O goes in Intracellular tonicity decreases Need to maintain normal intracellular tonicity H2O moves [Na+] IV
54 How does loss of ICF cause hypernatremia? H2O leaves [loop diuretics, fever] ICF Need to Intracellular maintain tonicity normal increases intracellular tonicity ECF H2O moves [Na+] IV CASE 1: RK
55 CASE 1: RK RK is an 83 y/o F admitted to your medical unit from assisted living with a 5-day history of coughing, difficulty breathing and increasing confusion. HPI: RK was in her usual state of health until one week ago when she developed what appeared to be an URTI. Her cough gradually got worse, being occasionally productive of yellowish sputum. She became increasingly confused over the following days. PMH: Stroke 6 months ago with some residual R sided weakness, Mild HTN, GERD, OA (knees) O/E: Wt. 50 kg (usually 54 kg), Temp 40C. Chest dull to auscultation and percussion. RR 27. Oriented x 1. CXR shows some RLL consolidation. CASE 1: RK Questions about what you see here? What prompts you to be concerned about a Na/H2O problem? What is your APPROACH to assessing RK from a Na/H2O viewpoint?
56 CASE 1: RK Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF) CASE 1: RK
57 CASE 1: RK What s your ASSESSMENT? CASE 2: KP
58 CASE 2: KP KP is a 77 y/o M brought to your urgent care center from home because of increasing lethargy and confusion over the past 48 hours. HPI: He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for isolated systolic hypertension. PMH: HTN. CAP. O/E: Oriented x 3. ~80kg. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. JVP <2cm ASA. CASE 2: KP Questions about what you see here? What prompts you to be concerned about a Na/H2O problem? What is your APPROACH to assessing KP from a Na/H2O viewpoint?
59 CASE 2: KP Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF) CASE 2: KP
60 CASE 2: KP What s your ASSESSMENT? CASE 3: BW
61 CASE 3: BW BW is a 67 y/o white M who presents to your primary care clinic complaining of general malaise and increasing confusion for one week. PMH: - Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago - Mild HTN x 5 y (metoprolol 100 mg po bid) - Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d) O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA. CASE 3: BW Questions about what you see here? What prompts you to be concerned about a Na/H2O problem? What is your APPROACH to assessing BW from a Na/H2O viewpoint?
62 CASE 3: BW Assess the ICF Serum [Na+] mmol/l hypernatremia ( ICF) hyponatremia ( ICF) CASE 3: BW
63 CASE 3: BW What s your ASSESSMENT? Why is this happening to BW? What other tests do we look at? TRAP
64 Treating deficiencies of ECF and ICF CRYSTALLOIDS COLLOIDS
65 Osmolality of IV fluids matters. Why?
66
67 Another perspective on crystalloids Osmolality (mosm/l) [Na] ( & Cl) (meq/l) Dextrose (g/l) NS (0.9% NaCl) Cal/L D5W /2NS D5-1/2NS /3D5-1/3NS % NaCl Seawater ~1000 ~475 Gatorade 365 ~20 ~220 Oral rehydration
68 CASE 1: RK CASE 1: RK RK is an 83 y/o F admitted to your medical unit from assisted living with a 5-day history of coughing, difficulty breathing and increasing confusion. HPI: RK was in her usual state of health until one week ago when she developed what appeared to be an URTI. Her cough gradually got worse, being occasionally productive of yellowish sputum. She became increasingly confused over the following days. PMH: Stroke 6 months ago with some residual R sided weakness, Mild HTN, GERD, OA (knees) O/E: Wt. 50 kg (usually 54 kg), Temp 40C. Chest dull to auscultation and percussion. RR 27. Oriented x 1. CXR shows some RLL consolidation.
69 CASE 1: RK Managing RK s Na & H2O issues: 1. Treat the HYPOVOLEMIA 2. Treat the HYPERNATREMIA CASE 1: RK Managing RK s Na & H2O issues: 1. Treat the HYPOVOLEMIA


70 CASE 1: RK Managing RK s Na & H2O issues: 2. Treat the HYPERNATREMIA CASE 1: RK Managing RK s Na & H2O issues: 2. Treat the HYPERNATREMIA
71 CASE 1: RK Orders for RK: Monitoring Plan: CASE 2: KP

72 CASE 2: KP KP is a 77 y/o M brought to your urgent care center from home because of increasing lethargy and confusion over the past 48 hours. HPI: He has had diarrhea for the past 4 days subsequent to a course of cefuroxime for mild CAP, and has been receiving HCTZ 25 mg/d for one year for isolated systolic hypertension. PMH: HTN. CAP. O/E: Oriented x 3. ~80kg. 100/60 supine, 75/45 standing. HR 65 supine, 80 standing. JVP <2cm ASA. CASE 2: KP Managing KP s Na & H2O issues: 1. Treat the HYPOVOLEMIA

73 CASE 2: KP Managing KP s Na & H2O issues: 1. Treat the HYPOVOLEMIA CASE 2: KP Orders for KP: Monitoring Plan:
74 CASE 3: BW CASE 3: BW BW is a 67 y/o white M who presents to your primary care clinic complaining of general malaise and increasing confusion for one week. PMH: - Carcinoma of the bronchus (surgical resection and radiation therapy) 4 months ago - Mild HTN x 5 y (metoprolol 100 mg po bid) - Depression (diagnosed 4 months ago and treated with fluoxetine 50 mg/d) O/E: Moderately obese, disoriented white male. BP 150/85 supine, 145/85 standing. HR 70 supine, 75 standing. Temp 36.8C, Wt. 100 kg, JVP 3 cm ASA.
75 CASE 3: BW Managing BW s Na & H2O issues CASE 3: BW ASIDE: what if we wanted to give 3%NaCl IV to raise BW s Na quickly?
76
77 CASE 3: BW ASIDE: what if we wanted to give 3%NaCl IV to raise BW s Na quickly? CASE 3: BW Orders for BW: Monitoring Plan:
78 Carroll AE. NY Times. Aug 24, 2015

:205 7.")
79 Tsindos S. Aust N Z J Public Health Jun 1;36(3): Guppy MPB. BMJ 2004;328:
[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:
![[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:](/thumbs/73/69178995.jpg "[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:") COI Disclosure Busting Myths and de-mist-ifying its Assessment & Management Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP Faculty of Pharmaceutical Sciences The University of British Columbia Lower
COI Disclosure Busting Myths and de-mist-ifying its Assessment & Management Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP Faculty of Pharmaceutical Sciences The University of British Columbia Lower
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Objectives. Objectives
 Objectives Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation mediate
Objectives Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation mediate
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders o f of water water Detlef Bockenhauer
 Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/21/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Pediatric Dehydration and Oral Rehydration. May 16/17
 Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Case Summary. Workshop Overview. Mr. M
 9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
9:00 10:30 Workshop Overview Mr. M Who is this document primarily intended to reach? What is the format? How soon should I see a newly referred heart failure patient? How often should my heart failure
Physiology of the body fluids, Homeostasis
 Physiology of the body fluids, Homeostasis Tamas Banyasz The Body as an open system 1. Open system: The body exchanges material and energy with its environment 2. Homeostasis: The process through which
Physiology of the body fluids, Homeostasis Tamas Banyasz The Body as an open system 1. Open system: The body exchanges material and energy with its environment 2. Homeostasis: The process through which
Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?
![Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?](/thumbs/95/124873940.jpg "Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?") Objectives Case Summary Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation
Objectives Case Summary Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Updates in Therapeutics 2015:
 Updates in Therapeutics 2015: The Pharmacotherapy Preparatory Review & Recertification Course Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, PharmD, BCPS University of Tennessee, Knoxville, TN
Updates in Therapeutics 2015: The Pharmacotherapy Preparatory Review & Recertification Course Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, PharmD, BCPS University of Tennessee, Knoxville, TN
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Renal physiology D.HAMMOUDI.MD
 Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
Renal physiology D.HAMMOUDI.MD Functions Regulating blood ionic composition Regulating blood ph Regulating blood volume Regulating blood pressure Produce calcitrol and erythropoietin Regulating blood glucose
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Body fluids. Lecture 13:
 Lecture 13: Body fluids Body fluids are distributed in compartments: A. Intracellular compartment: inside the cells of the body (two thirds) B. Extracellular compartment: (one third) it is divided into
Lecture 13: Body fluids Body fluids are distributed in compartments: A. Intracellular compartment: inside the cells of the body (two thirds) B. Extracellular compartment: (one third) it is divided into
All but Vaptans. Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 All but Vaptans Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles [ Na ] = Na + e + K + e TBW 60 y BW 66 kg, TBW ± 33 L, SNa 140 meq/l TBW 1 L SNa: 3% (or 4.2
All but Vaptans Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles [ Na ] = Na + e + K + e TBW 60 y BW 66 kg, TBW ± 33 L, SNa 140 meq/l TBW 1 L SNa: 3% (or 4.2
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Fluid & Electrolyte Therapy. Prof. Soliman Ali Hassan Prof. of Surgery Taibah university
 Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
SIMPLY. Fluids. Dr William Dooley
 SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
Taking Tolvaptan with a grain of salt. Jia (Shermaine) Ngo LMPS Pharmacy Resident October 7, 2016
 Ngo LMPS Pharmacy Resident October 7, 2016") Taking Tolvaptan with a grain of salt Jia (Shermaine) Ngo LMPS Pharmacy Resident 2016-2017 October 7, 2016 1 Learning Objectives Define Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Taking Tolvaptan with a grain of salt Jia (Shermaine) Ngo LMPS Pharmacy Resident 2016-2017 October 7, 2016 1 Learning Objectives Define Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
THe Story of salty Sam
 THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
SAMPLE SAQ QUESTIONS RCPSC General Internal Medicine Examination (2015)
") SAMPLE SAQ QUESTIONS RCPSC General Internal Medicine Examination (2015) Question 1 You are called by a relatively inexperienced physician practicing in a rural emergency department 3 hours from your center.
SAMPLE SAQ QUESTIONS RCPSC General Internal Medicine Examination (2015) Question 1 You are called by a relatively inexperienced physician practicing in a rural emergency department 3 hours from your center.
SIMPLY. Fluids. Dr Will Dooley
 SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Fluids, Electrolytes and Hydration. Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University
 Fluids, Electrolytes and Hydration Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Discuss optimum hydration and effects of dehydration
Fluids, Electrolytes and Hydration Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Discuss optimum hydration and effects of dehydration
Fluid and Electrolytes: Parenteral
 Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
Algorithm Focus. Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Perspective regarding the EMT- Intermediate algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Name that disease. C.J. Wolf, MD, CPC, CPC-H. University of Texas System Case #1
 Name that Disease C.J. Wolf, MD, CPC, CPC-H Asst. Systemwide Compliance Officer University of Texas System cwolf@utsystem.edu Case #1 17 year old girl who has lost 20 lbs in the last six months Thin and
Name that Disease C.J. Wolf, MD, CPC, CPC-H Asst. Systemwide Compliance Officer University of Texas System cwolf@utsystem.edu Case #1 17 year old girl who has lost 20 lbs in the last six months Thin and
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Resuscitation of the Critically ill Foal
 Resuscitation of the Critically ill Foal Sick Cell Syndrome Foal: Wishful Warm Blood filly DOB: March 25 1 AM Admission Date: March 25 11:25 AM 10 hours old Wishful History Born at 1 AM on March 25 Foal
Resuscitation of the Critically ill Foal Sick Cell Syndrome Foal: Wishful Warm Blood filly DOB: March 25 1 AM Admission Date: March 25 11:25 AM 10 hours old Wishful History Born at 1 AM on March 25 Foal
Pediatric Sodium Disorders
 Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing Pediatrics Case Studies: Child Dehydration
 Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Objectives. Objectives
 Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
2018/6/7 APSN/JSN CME Course Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6
 2018/6/7 APSN/JSN CME Course 2018 Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6 Case1 77F Left leg pain Na 112 Case2 39M Seizure Na 117 Case3 73M General malaise Na 120 Case1
2018/6/7 APSN/JSN CME Course 2018 Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6 Case1 77F Left leg pain Na 112 Case2 39M Seizure Na 117 Case3 73M General malaise Na 120 Case1
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Each tablet contains:
 Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Terminology. Terminology. Terminology. Molarity number of moles of solute / Liter of solution. a) Terminology b) Body Fluid Compartments
 Terminology b) Body Fluid Compartments") Integrative Sciences: Biological Systems A Fall 2011 Body Fluids Compartments, Renal Clearance and Renal Excretion of Drugs Monday, November 21, 2011 Lisa M. Harrison-Bernard, Ph.D. Department of Physiology;
Integrative Sciences: Biological Systems A Fall 2011 Body Fluids Compartments, Renal Clearance and Renal Excretion of Drugs Monday, November 21, 2011 Lisa M. Harrison-Bernard, Ph.D. Department of Physiology;
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
POST-OP CARDIAC SURGERY PHYSICIAN S ORDER SHEET USE BALLPOINT PEN ONLY. CARDIAC INTENSIVE CARE UNIT
 PHYSICIAN S SHEET Automatically Activate, if not in agreement, cross out and initial Activated by Checking Box ALLERGIES: None known YES Patient s Height: Patient s Weight: ALL MEDICATION and INTRAVENOUS
PHYSICIAN S SHEET Automatically Activate, if not in agreement, cross out and initial Activated by Checking Box ALLERGIES: None known YES Patient s Height: Patient s Weight: ALL MEDICATION and INTRAVENOUS
Fluids, Electrolytes, and Nutrition
 Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Workshop on Hyponatremia. Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 Workshop on Hyponatremia Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles CASE REPORT I A 70-year-old female patient is hospitalized because she fall on the
Workshop on Hyponatremia Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles CASE REPORT I A 70-year-old female patient is hospitalized because she fall on the
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround