Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
|
|
|
- Mervin Piers Rodgers
- 6 years ago
- Views:
Transcription

1 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD


2 Water or salt?
3 Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied to total body sodium content Sodium concentration (ie hypo or hypernatremia) determined by proportion of total body sodium to water The kidneys regulate sodium and water balance independently

4 Physiology of water regulation You are in the desert w/ no access to water What happens physiologically
5 Physiology of water regulation Insensible losses Skin 500cc (possibly more in hospitalized patients) Urine losses 500cc (electrolyte free water loss) Respiratory 400cc (more in hospitalized patients) Stool 200cc
6
7
8 Physiology of water regulation Change in plasma osmolality (increase) ADH Thirst Vasopressin receptor V1 V2 Aquaporins Water moves down concentration gradient
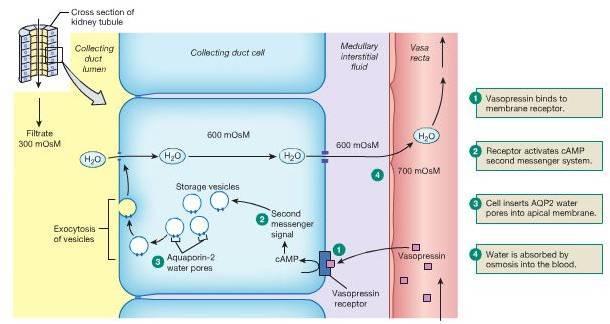
9 ADH physiology
10 Case 1 35 yr old man s/p motorcycle vs. auto seen in SICU. Has been in ICU for 3 weeks Multiple trips to OR for orthopedic surgeries Prolonged vent requirements s/p VAP with sepsis Consulted for hypernatremia management
11 Case 1 Receiving multiple drips and antibiotics mixed in saline. Receiving tube feeds. Surgical team added water flushes due to the hypernatremia at 300cc every 6 hours Exam sig for : On vent, normotensive and HDS, decreased breath sounds, anasarca. External fixators present on LLE Labs: Na 165 Cr 1.2 BUN 105
12 Case 1 What is your approach?
13 Case 1 Problems: Hypernatremia Hypervolemic vs. euvolemic vs. hypovolemic Azotemia Hypervolemia Too much salt or too little water?
14 Case 1 Water deficit calculation: H2O def= TBW x (current Na/140-1) TBW= 45-60% of lean body wt in kg Data: current wt 110kg IBW 85kg Recommendations?
15 Case 1 Goal decrease in sodium 10meq/L in 1 st 24h max 16-18meq/L in 1 st 48h How much free water needed? How would you administer it? What monitoring is needed?
16 Case 1 You decide about 3 L is needed Water flushes increased to 125cc/hr Call parameters given to RN Next AM you open chart Serum sodium is 170 What happened?
17 Case 1 You study I/O and med list a bit further Cardiology has started pt on lasix (polydoctoring) Intake was 4L, output was 6.5L (drains, urine output, diarrhea from TF) Ongoing adjustment is needed to account for ongoing water losses. Impossible to quantify in most cases In general replacement rate will underestimate amount of water needed (ie will see undercorrection)
18 Hyponatremia Simply put, hyponatremia develops in 2 situations- Water intake which overwhelms excretory capacity (rare, such as severe psychogenic polydypsia) Intake of a water load which cannot be excreted due to low GFR or persistent effects of ADH
19 Hyponatremia Usually divided according to volume status Hypovolemic hyponatremia Total body water decreased Volume (total body sodium) decreased more Euvolemic hyponatremia Total body water increased Volume (total body sodium) no change Hypervolemic hyponatremia Total body water increased more Volume (total body sodium) increased Best to think of volume status (sodium balance) and water balance (sodium concentration) completely separately
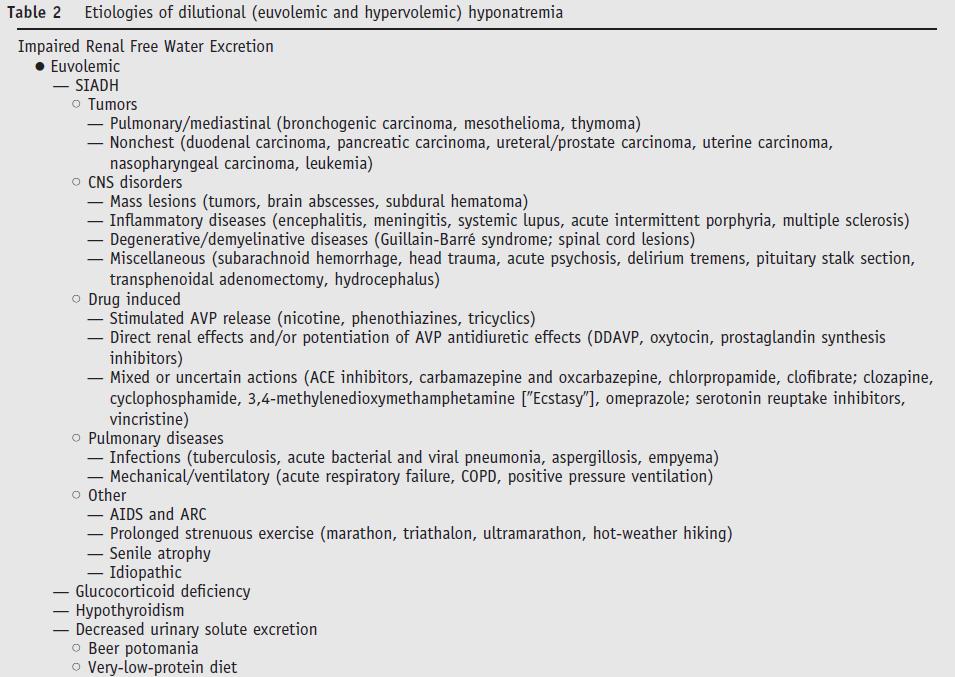
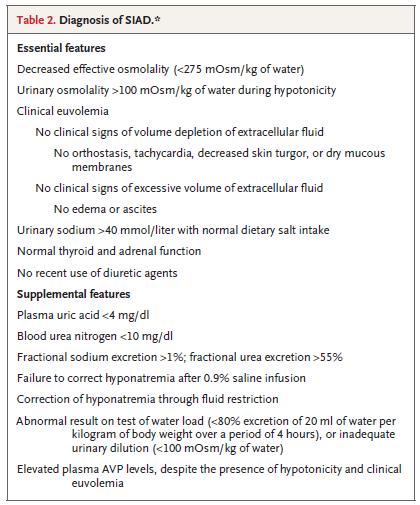
20 Hyponatremia My steps in evaluating hyponatremic disorders How much time do I have-- ie is pt symptomatic? Hypo-osmolar? Rule out---- pseudohyponatremia (rare) hypertonic hyponatremia Volume status? Signs of volume depletion? Signs of volume excess? If euvolemic, reason for SIADH? Rule out thiazide diuretics, severe hypothyroidism, adrenal insufficiency Rule out poor solute intake ( beer potomania or tea and toast diet ) Working diagnosis Treatment plan and monitoring frequency
21 Case 2 57 yo woman with PMH of hypothyroidism presents w/ a 1 week history of upper resp symptoms along w/ n/v. Very little intake other than trying to hydrate. Brought to ER by family for progressive confusion. The time is noon. Exam: BP 100/54 HR 101, confused, no edema. Labs: Na 118 K 3.4 BUN 5 Scr 0.4 Osm 250 BG 130 TSH wnl Urine data Osm 141 Na 36 SG <1.005 (after NS?)
22 Case 2 Hyponatremia Type? Symptomatic? Pt is bolused 2L NS in ED
23 Case 2 You are consulted at 9pm by admitting hospitalist however RN kindly holds call till the next morning. Unit secretary calls in consult after case mgmt rounds Time is 10am Na is 140 Pt feels better, back to normal RN states pt has put out liters of urine and asks if pt can be discharged today Are you concerned? What are the risks?
24 Osmotic demyelination syndrome Acute hyponatremia causes brain edema Adaptation begins immediately and is complete around 48hrs Loss of water, sodium, intracellular potassium, organic solutes Rapid correction can result in ODS Usually in pts w/ serum sodium <120 on presentation At risk pts: cirrhosis, alcoholism, malnourished, OLTx Current rate of correction recommendations: Less than meq/l in 1 st 24h and 18mEq/L in 1 st 48h
25 Case 2 What are your recommendations???
26 Case 2 Increase in Na --- Goal increase --- Therapy ---

27 Case 2
28 Case 3 48 yo man with smoking history presents with confusion and drowsiness. Meds include combivent. BP 130/84 HR 70, JVP 4cm, clear lungs, no edema. CXR shows COPD changes. Family is concerned that he drinks beer all day and eats very little. Labs- Na 117 K 3.6 SOsm 258 Una 90 Uosm 662
29 Case 3 Symptoms? Volume status? Differential diagnosis? What other labs or imaging would you order? Treatment options?
30
31 Case 3
32 Case 3 How would you treat? A. 3% saline B. Fluid restriction C. Salt tabs and lasix D. Tolvaptan

33 Case 3 3% saline Rate To raise serum Na by 10 meq/l over 24h assuming pt is 70kg, TBW=42L Na needed is 420meq. Volume needed is around 800cc of 3% or a STARTING rate of 33cc/hr. I would stop when pts symptoms ceased or when sodium >124 Close monitoring is essential
34 Case 4 58 yo woman with a history of ischemic cardiomyopathy admitted with pulmonary edema. Meds include metoprolol, spironolactone, furosemide, lisinopril. Exam- BP 97/54 HR 85, alert and oriented, JVP 9cm, lungs w/ diffuse crackles, 1+ LE edema Labs- Na 121 K 3.5 BUN 45 Scr 1.1 Urine data- UNa 15 UCl <5 Uosm 210 (6hrs after last diuretic dose)
35 Case 4 Symptoms? Volume? Workup? Treatment options?

36 Vasopressin receptor antagonists Advantages Addresses underlying issue Efficacy Allows less strict fluid restriction Disadvantages Hospitalization Cost Rapid correction Thirst Black Box Warnings

37 Questions?
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
IX: Electrolytes. Sodium disorders. Specific Learning Objectives: Dan Henry, MD Clerkship Director University of Connecticut School of Medicine
 IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:
![[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:](/thumbs/73/69178995.jpg "[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:") COI Disclosure Busting Myths and de-mist-ifying its Assessment & Management Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP Faculty of Pharmaceutical Sciences The University of British Columbia Lower
COI Disclosure Busting Myths and de-mist-ifying its Assessment & Management Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP Faculty of Pharmaceutical Sciences The University of British Columbia Lower
BEFORE the session. Sodium & Water Assessment & Therapeutics. LMPS Residents
 BEFORE the session 1. Get Loewen s Sodium & Water Assessment & Therapeutics 1-pager at www.peterloewen.com/made 2. Read McGee S, Abernethy WB, Simel DL. Is this patient hypovolemic? JAMA 1999;281:1022-9
BEFORE the session 1. Get Loewen s Sodium & Water Assessment & Therapeutics 1-pager at www.peterloewen.com/made 2. Read McGee S, Abernethy WB, Simel DL. Is this patient hypovolemic? JAMA 1999;281:1022-9
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hyponatremia Clinical Significance. Ágnes Haris MD PhD, St. Margit Hospital, Budapest
 Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Samsca. Samsca (tolvaptan) Description
 Description") Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
75 year old woman with Hyponatremia. Sharon H. Chou, MD Endorama September 13, 2012
 75 year old woman with Hyponatremia Sharon H. Chou, MD Endorama September 13, 2012 History of Present Illness 75 yo woman who was previously healthy until the past month when she had recurrent admissions
75 year old woman with Hyponatremia Sharon H. Chou, MD Endorama September 13, 2012 History of Present Illness 75 yo woman who was previously healthy until the past month when she had recurrent admissions
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Each tablet contains:
 Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Pediatric Sodium Disorders
 Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Workshop CME 22 mars Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 Workshop CME 22 mars 2013 Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles Overcorrection of chronic hyponatremia CASE REPORT I (1) Female 71 year Altered
Workshop CME 22 mars 2013 Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles Overcorrection of chronic hyponatremia CASE REPORT I (1) Female 71 year Altered
hyponatremia/hypo-osmolality/hypotonic dehydration
 E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
Eggplant: The Story of Sodium in Neurocritical Care
 Eggplant: The Story of Sodium in Neurocritical Care Larry Burris, DO Medical Director NCC - Sanford Health Medical Director Renal Transplant - Sanford Health Assistant Professor of Medicine SSOM NaCl Facts
Eggplant: The Story of Sodium in Neurocritical Care Larry Burris, DO Medical Director NCC - Sanford Health Medical Director Renal Transplant - Sanford Health Assistant Professor of Medicine SSOM NaCl Facts
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
 Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
SAMSCA (tolvaptan) oral tablet
 oral tablet") SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Hyponatremia: A Review
 Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Pediatric Dehydration and Oral Rehydration. May 16/17
 Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Neurohypophysis. AVP Receptors. Hyponatremia in Pituitary Disorders 9/29/2016. Lewis S. Blevins, Jr., M.D.
 in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives. Objectives
 Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
Objectives. Objectives
 Objectives Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation mediate
Objectives Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation mediate
SATURDAY PRESENTATIONS
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS Annual Meeting
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluids, Electrolytes, and Nutrition
 Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Case Studies of Electrolyte Disorders ACOI Board Review Mark D. Baldwin D.O. FACOI
 Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Empowering Pharmacists to Improve Management of Hyponatremia. Learning Objectives. Diagnostic Algorithm for Hyponatremia
 Empowering Pharmacists to Improve Management of Hyponatremia A Patient-Centric, Process of Care Guide Learning Objectives Discuss the clinical consequences of undertreatment of hyponatremia, including
Empowering Pharmacists to Improve Management of Hyponatremia A Patient-Centric, Process of Care Guide Learning Objectives Discuss the clinical consequences of undertreatment of hyponatremia, including
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Disorders of Water Metabolism
 Disorders of Water Metabolism Joshua M. Thurman and Tomas Berl 2 Introduction Disorders of water balance and serum Na ( S Na ) are very common in hospitalized patients [ 1 ]. In health, water balance and
Disorders of Water Metabolism Joshua M. Thurman and Tomas Berl 2 Introduction Disorders of water balance and serum Na ( S Na ) are very common in hospitalized patients [ 1 ]. In health, water balance and
Physiology of the body fluids, Homeostasis
 Physiology of the body fluids, Homeostasis Tamas Banyasz The Body as an open system 1. Open system: The body exchanges material and energy with its environment 2. Homeostasis: The process through which
Physiology of the body fluids, Homeostasis Tamas Banyasz The Body as an open system 1. Open system: The body exchanges material and energy with its environment 2. Homeostasis: The process through which
A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
PROTRACTED ACUTE HYPERVOLEMIC HYPERNATREMIA UNMASKED AFTER VASOPRESSIN THERAPY, A CASE REPORT, REVIEW OF LITERATURE, AND PROPOSED ALGORITHMIC APPROACH
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Fluid and electrolyte abnormalities. Melanie P. Hoenig (Derman) Associate Professor BIDMC
 Associate Professor BIDMC") Fluid and electrolyte abnormalities Melanie P. Hoenig (Derman) Associate Professor BIDMC Disclosures: Editor, Kidney Self Assessment Program American Society of Nephrology Hyponatremia* Hypernatremia Hyperkalemia
Fluid and electrolyte abnormalities Melanie P. Hoenig (Derman) Associate Professor BIDMC Disclosures: Editor, Kidney Self Assessment Program American Society of Nephrology Hyponatremia* Hypernatremia Hyperkalemia
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Not all Hyponatremia is a Saline Deficiency SIADH in the Real World
 Not all Hyponatremia is a Saline Deficiency SIADH in the Real World Mark D. Baldwin D.O., FACOI Professor and chair of the Department of Internal Medicine Pacific Northwest University of Health Sciences
Not all Hyponatremia is a Saline Deficiency SIADH in the Real World Mark D. Baldwin D.O., FACOI Professor and chair of the Department of Internal Medicine Pacific Northwest University of Health Sciences
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Correction of hypervolaemic hypernatraemia by inducing negative Na + and K + balance in excess of negative water balance: a new quantitative approach
 Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?
![Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?](/thumbs/95/124873940.jpg "Serum [ Serum Na] = 128 meq/l Question~ why Question~ wh edema?") Objectives Case Summary Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation
Objectives Case Summary Volume regulation entails the physiology of salt content regulation The edematous states reflect the pathophysiology of salt content regulation The mechanisms of normal volume regulation
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
ORIGINAL ARTICLE HYPONATREMIA IN ELDERLY *Dr. T. Prabhu. Annamalai University, Annamalainagar , Tamilnadu, India
 Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 2, Issue 10, pp 325-332, October, 2014 ORIGINAL ARTICLE
Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 2, Issue 10, pp 325-332, October, 2014 ORIGINAL ARTICLE
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
11/4/2010. Learning Objectives. Question 1. Question 2 PLEASE ANSWER THE HYPONATREMIA PRE-ACTIVITY TEST QUESTIONS. A. True B.
 Faculty Disclosures James S. Kalus, PharmD, BCPS (AQ CV) Senior Manager, Patient Care Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE Saturday, October 23, 2010 Hemant Dhingra, MD
Faculty Disclosures James S. Kalus, PharmD, BCPS (AQ CV) Senior Manager, Patient Care Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE Saturday, October 23, 2010 Hemant Dhingra, MD
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Disorders o f of water water Detlef Bockenhauer
 Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
For more information about how to cite these materials visit
 Author(s): Roger Grekin, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Roger Grekin, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA
 Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Metabolic Abnormalities in Critically Ill Patients
 CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต
 Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต Content : Electrolyte Emergency!! Serum sodium Normal serum sodium: 135-145 meq/l Normal serum osmolality: 285-295 mosm/l Normal urine sodium: 10-20
Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต Content : Electrolyte Emergency!! Serum sodium Normal serum sodium: 135-145 meq/l Normal serum osmolality: 285-295 mosm/l Normal urine sodium: 10-20
A Clinical Approach to the Treatment of Chronic Hypernatremia
 Acid-Base and Electrolyte Teaching Case A Clinical Approach to the Treatment of Chronic Hypernatremia Ahmed Al-Absi, MD, 1 * Elvira O. Gosmanova, MD, 1 and Barry M. Wall, MD 1,2 Hypernatremia is a commonly
Acid-Base and Electrolyte Teaching Case A Clinical Approach to the Treatment of Chronic Hypernatremia Ahmed Al-Absi, MD, 1 * Elvira O. Gosmanova, MD, 1 and Barry M. Wall, MD 1,2 Hypernatremia is a commonly
Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC.
 Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC. Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to
Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC. Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia *
 An In-Depth Look: NORMAL AND ABNORMAL WATER BALANCE CE Article #1 Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia * Katherine M. James, DVM, PhD, DACVIM Veterinary Information Network
An In-Depth Look: NORMAL AND ABNORMAL WATER BALANCE CE Article #1 Normal and Abnormal Water Balance: Hyponatremia and Hypernatremia * Katherine M. James, DVM, PhD, DACVIM Veterinary Information Network
Intravenous Fluids: In the ER and on the floor. MEValletta,, MD August 4, 2005 Resident Core Conference Lecture Series
 Intravenous Fluids: In the ER and on the floor MEValletta,, MD August 4, 2005 Resident Core Conference Lecture Series Objectives Understand appropriate fluid resuscitation Understand appropriate fluid
Intravenous Fluids: In the ER and on the floor MEValletta,, MD August 4, 2005 Resident Core Conference Lecture Series Objectives Understand appropriate fluid resuscitation Understand appropriate fluid
Metabolism of water and electrolytes. 2. Special pathophysiology disturbances of intravascular volume and
 Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Hyponatremia 11/4/2010. Learning Objectives
 JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
Body water content. Fluid compartments. Regulation of water output. Water balance and ECF osmolallty. Regulation of water intake
 Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Sym pt om s of "hyponat rem ia" Serum [Na + ] m Eq/ L: - Asymptomatic
![Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic](/thumbs/94/122329913.jpg "Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic") Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Anemia and Pallor. These podcasts are designed to give medical students an overview of key
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Anemia and Pallor. These podcasts are designed to give medical students an overview of key
Workshop on Hyponatremia. Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 Workshop on Hyponatremia Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles CASE REPORT I A 70-year-old female patient is hospitalized because she fall on the
Workshop on Hyponatremia Pr Guy DECAUX Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles CASE REPORT I A 70-year-old female patient is hospitalized because she fall on the
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries