Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
|
|
|
- Wilfrid Gibson
- 5 years ago
- Views:
Transcription
1 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals





2
3 Disclosures of Interest Associate Clinical Director NIHR Leeds In-Vitro Diagnostic Co-operative NICE AKI and CKD Guideline Update Committee Member 2018 NICE Diagnostic Assessment Programme Committee for Point of Care Creatinine Testing before Contrast BMJ Best Practice Editor
4 Outline Physiology Causes Complications Clinical assessment Treatment Case presentation
5 Physiology Sodium Extracellular ion Normal > 135 meq/l Responsible for osmolality Osmolality Total no. of moles of solute/ kg of slovent mosmol/kg Determines transcellular distribution of water
6 Physiology Sodium concentration/osmolality maintained by Urinary excretion of sodium and water ADH secretion Water load ingestion Suppression of ADH Excretion of dilute urine
7 Physiology Max daily urine output 10 L Min urine osmolality mosmol/kg Max urine osmolality 1000 mosmol/kg (age based)
8 Clinical Features Symptoms depend on severity and rate of sodium reduction gradual decreases in sodium usually result in minimal symptoms rapid decreases can result in severe symptoms (cerebral oedema) Polydipsia muscle cramps Headaches Confusion altered mental status Coma status epilepticus
9 Causes Pseudohyponatraemia Hyperlipideamia Hyperglyceamia Myeloma - hyperproteinaemia Hypovolaemic hyponatraemia Diuretics Thiazides GI losses Adrenal insufficiency Osmotic diuresis Mannitol Salt wasting nephropathies
10 Causes Hypervolaemic hyponatraemia Heart failure reduced cardiac output Unsuppressed ADH Liver cirrhosis arterial vasodilatation Unsuppressed ADH CKD egfr<15 Min urine osmolality mosmol/kg
11 Causes Euvolaemic hyponatraemia Malnourishment Exercise excessive water ingestion Reset osmostat Pregnancy Primary polydipsia Prostate surgery Sorbitol irrigation - absorption SIADH
12 Causes of SIADH CNS disease Malignancy Drugs Carbamazepine Fluoxetine Serotonin inhibitors Hypothyroidism Adrenal insufficiency Pulmonary disease Recent surgery
13 Clinical Assessment Comprehensive clinical evaluation Mental status Identify potential cause Recent surgery, medication etc Volume status Hypovolaemic Renal or GI fluid losses Euvolaemia SIADH Hypervolaemia (oedema) Heart failure Liver cirrhosis
14 Investigations U&Es Bicarbonate Glucose Serum osmolality Urine Na Urine osmolality

15 Assessment of Hyponatreamia
16 Assessment of Hypo-osmolar hyponatraemia Na < 135 meq/l Urine Osm < 100 Urine Osm > 100 Psychogenic Polydipsia Assess kidney function Normal Kidney disease Volume status? Primary kidney disease Euvolaemic Hypervolaemic Hypovolaemic SIADH e.g. Drugs UNa > 20 UNa < 20 UNa > 20 UNa < 20 Kidney Dx Cirrhosis Heart failure Kidney losses e.g. duiretics Extra-renal losses e.g. Vomiting Diarrhoea, Burns
17 Treatment Key considerations Duration of hyponataemia? Acute < 48hrs Chronic > 48hrs Severity?
18 Treatment Rate of correction of sodium Severe hyponatraemia ( Na < 120 meq/l) with neurological symptoms Rapid initial correction 4-6 meq/l in first 4-6 hrs Identify cause (Avoid correcting by > 8 meq/l in 24 hr period if > 48hrs duration)
19 Treatment
20 Treatment Risk of overly rapid correction Osmotic demyelination Occurs a few days afterwards Results from rapid movement of water out of cells pontine and extra-pontine regions seizures disturbed consciousness gait changes MRI changes
: 231")
21 Indian J Crit Care Med Jul-Aug; 17(4):
22 Treatment Mild to moderate hyponatraemia ( meq/l) Less severe symptoms Identify reversible cause Fluid restrict < 800 mls/day Oral salts 9g ~ 154mEq sodium
23 Treatment Role of ADH antagonist? Tolvaptan oral Used in patients with hyponatraemia secondary to SIADH Risks of Overly rapid correction Hepato-toxicity limit use < 30 days
24 Treatment Renal Replacement Therapy Acute onset < 48hrs In setting of AKI Volume overload Oliguric Rapid correction recommended Intermittent HD CRRT
25 Treatment Renal Replacement Therapy Chronic onset > 48hrs In setting of AKI Volume overload Oliguric Gradual correction recommended CRRT Monitor Na + on ABG Adjust dose of CRRT
26 Case Presentation
27 Case Presentation 65 year old male End stage kidney failure Membranous GN Kidney transplant 2006 Biventricular heart failure Bronchiectasis
28 Case Presentation Admitted 20/11/17 Felt generally unwell for a month Lethargy Reduced appetite Wt 52Kg Fevers Increasingly breathless for last 3 months reduced exercise tolerance
29 Case Presentations Mycophenolate Mofetil Tacrolimus Paracetamol Fluoxetine Lansoprazole Atorvastatin Ramipril Furosemide
30 Case Presentation On examination Alert, not confused Normovolaemic on examination BP 80/50 Crackles at lung bases O 2 Saturations 95%
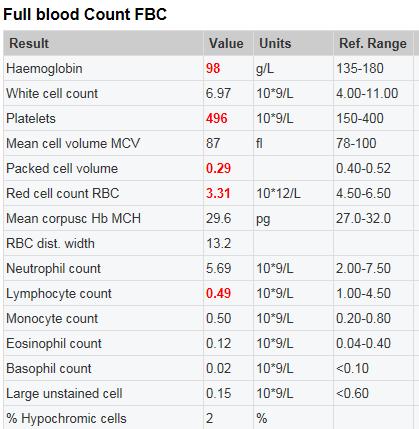
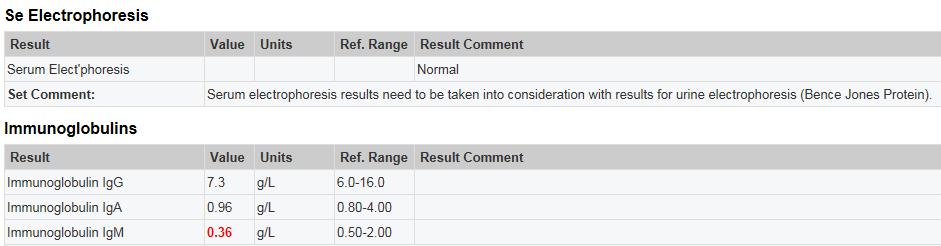
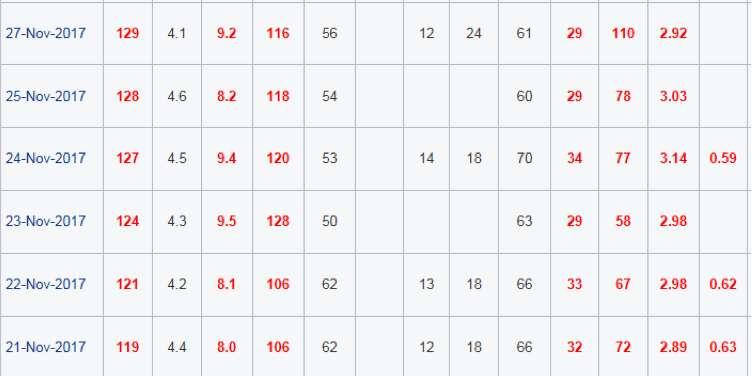
31 Case Presentation Investigations Hyponatraemia Hypercalcaemia Elevated CRP
32 Case Presentation
33 20/11/17
34 20/11/17

35 Heart size is at the upper limits of normal. There is perihilar interstitial oedema
36 Case Presentation Initial treatment IV 0.9% sodium chloride fluid resucitation caution Oral fluid restriction Fluoxetine stopped Pamidronate Dietician input
37 20/11/17

38 20/11/17 Hypo-osmolar hyponatraemia
39 20/11/17

40 23/11/19
41 CT 23/11/19 CT Thorax Abdomen Pelvis with contrast : Comparison is made with previous CTs up to including 14/11/2008. There are progressive lung changes with quite extensive groundglass type inflammatory change predominantly in the upper lobes. Bronchiectasis at the bases and plugging of the left lower lobe bronchus with low density material. Comment: Progressive lung changes with new groundglass change
42 Case Presentation Respiratory referral Bronchoscopy abnormal left lower lobe with extensive secretions
43 25/11/17
44 27/11/17
45 BAL Result Patient allergic to Trimethoprim Commenced on Primaquine (G6pd normal) and clindamycin for 21days
46
47 Patient discharged Case Presentation
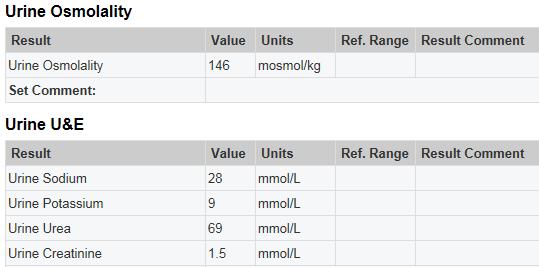
48 Summary Chronic hypo-osmolar hyponatraemia Euvoleamic Multiple causes Malnourished Fluoxetine PCP Urine osmolality 146 mosmol/kg SIADH
49 Conclusions Comprehensive clinical evaluation Duration Severity Investigations Cause Treatment Acute rapid correction possible Chronic gradual correction
50 Thank You

51 Thank You! Website: Follow us on Tel:
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Disorders o f of water water Detlef Bockenhauer
 Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Disorders of water Detlef Bockenhauer How do we measure water? How do we measure water? Not directly! Reflected best in Na concentration Water overload => Hyponatraemia Water deficiency => Hypernatraemia
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypomagnesemia
 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist Hyponatremia Salt and water imbalance Management Acute vs chronic Approach! How to make the correct diagnosis?! How to treat safely? Etiology!
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPONATRAEMIA Summary. Start. End. Key: Na + below normal range ( mmol/L) Symptomatic?
 Symptomatic?") CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPONATRAEMIA Summary Key: General tes ED/MAU/SRU/Acute GP/Amb-Care GP/SWASFT In-patient wards Start Na + below normal range (135 145mmol/L) Refer to endocrinology
CLINICAL GUIDELINE FOR THE MANAGEMENT OF HYPONATRAEMIA Summary Key: General tes ED/MAU/SRU/Acute GP/Amb-Care GP/SWASFT In-patient wards Start Na + below normal range (135 145mmol/L) Refer to endocrinology
Public Assessment Report. Scientific discussion. Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR
 SE/H/1443/01/MR") Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Eggplant: The Story of Sodium in Neurocritical Care
 Eggplant: The Story of Sodium in Neurocritical Care Larry Burris, DO Medical Director NCC - Sanford Health Medical Director Renal Transplant - Sanford Health Assistant Professor of Medicine SSOM NaCl Facts
Eggplant: The Story of Sodium in Neurocritical Care Larry Burris, DO Medical Director NCC - Sanford Health Medical Director Renal Transplant - Sanford Health Assistant Professor of Medicine SSOM NaCl Facts
SAMSCA (tolvaptan) oral tablet
 oral tablet") SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
IX: Electrolytes. Sodium disorders. Specific Learning Objectives: Dan Henry, MD Clerkship Director University of Connecticut School of Medicine
 IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Metabolism of water and electrolytes. 2. Special pathophysiology disturbances of intravascular volume and
 Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Update in. Acute Kidney Injury. Mark Devonald Consultant Nephrologist. Nottingham AKI Research Group
 Update in Acute Kidney Injury Mark Devonald Consultant Nephrologist If you stay awake you might hear about Why AKI is important Some cases to illustrate some specific points A couple of updates on AKI
Update in Acute Kidney Injury Mark Devonald Consultant Nephrologist If you stay awake you might hear about Why AKI is important Some cases to illustrate some specific points A couple of updates on AKI
Neurohypophysis. AVP Receptors. Hyponatremia in Pituitary Disorders 9/29/2016. Lewis S. Blevins, Jr., M.D.
 in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
A large proportion of the body consists of water. Sodium is the major electrolyte that influences the water content and its distribution.
 WATER AND SODIUM DISTURBANCES A large proportion of the body consists of water. Sodium is the major electrolyte that influences the water content and its distribution. JOCELYN NAIcKER BSc, MB ChB, MFGP
WATER AND SODIUM DISTURBANCES A large proportion of the body consists of water. Sodium is the major electrolyte that influences the water content and its distribution. JOCELYN NAIcKER BSc, MB ChB, MFGP
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
The adult patient with hyponatraemia
 C Hirst MBChB FRCA A Allahabadia MBChB MD FRCP J Cosgrove MBBS FRCA FFICM Matrix reference 1A01, 2C01, 3C00 Key points Sodium is the most abundant and osmotically important extracellular cation. Disorders
C Hirst MBChB FRCA A Allahabadia MBChB MD FRCP J Cosgrove MBBS FRCA FFICM Matrix reference 1A01, 2C01, 3C00 Key points Sodium is the most abundant and osmotically important extracellular cation. Disorders
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
After i.v injection 45% of the amount of desmopressin is found in the urine within 24 hours.
 MINIRIN Tablets 0.1 and 0.2 mg Declaration Tablets 0.1 mg. Each tablet contains desmopressin acetate 0.1 mg and excipients q.s Tablets 0.2 mg. Each tablet contains desmopressin acetate 0.2 mg and excipients
MINIRIN Tablets 0.1 and 0.2 mg Declaration Tablets 0.1 mg. Each tablet contains desmopressin acetate 0.1 mg and excipients q.s Tablets 0.2 mg. Each tablet contains desmopressin acetate 0.2 mg and excipients
Acute Kidney Injury 2
 South West Cardiovascular Strategic Clinical Network Acute Kidney Injury 2 Audit review meeting 18/07/2014 Redwood Education Centre Author: Summary of results: Dr Preetham Boddana Consultant Nephrologist
South West Cardiovascular Strategic Clinical Network Acute Kidney Injury 2 Audit review meeting 18/07/2014 Redwood Education Centre Author: Summary of results: Dr Preetham Boddana Consultant Nephrologist
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Acute Kidney Injury in The Acute Oncology Patient
 Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Preventing Acute Kidney Injury
 Preventing Acute Kidney Injury Dr Andy Lewington MSc Clin Ed FRCP Consultant Nephrologist/Honorary Clinical Associate Professor Director of Undergraduate Medical Education Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk
Preventing Acute Kidney Injury Dr Andy Lewington MSc Clin Ed FRCP Consultant Nephrologist/Honorary Clinical Associate Professor Director of Undergraduate Medical Education Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk
MANAGEMENT OF HYPONATRAEMIA
 ABC of Intravenous Fluids, Electrolyte Disorders and AKI Management in Adults WASD 3 MANAGEMENT OF HYPONATRAEMIA Hyponatraemia (HoN) is a serum sodium concentration (s[na]),135mmol/l. It is due to an excess
ABC of Intravenous Fluids, Electrolyte Disorders and AKI Management in Adults WASD 3 MANAGEMENT OF HYPONATRAEMIA Hyponatraemia (HoN) is a serum sodium concentration (s[na]),135mmol/l. It is due to an excess
Disorders of sodium balance after brain injury Kate Bradshaw MBBS FRCA Martin Smith MBBS FRCA
 Disorders of sodium balance after brain injury Kate Bradshaw MBBS FRCA Martin Smith MBBS FRCA Sodium disturbances are common in patients with brain injury because of the major role that the central nervous
Disorders of sodium balance after brain injury Kate Bradshaw MBBS FRCA Martin Smith MBBS FRCA Sodium disturbances are common in patients with brain injury because of the major role that the central nervous
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Acute Kidney Injury. Patient Information Leaflet
 Acute Kidney Injury Patient Information Leaflet What is Acute Kidney Injury (AKI)? Acute Kidney injury is a rapid fall in kidney function in a person who has become unwell. It can happen over hours or
Acute Kidney Injury Patient Information Leaflet What is Acute Kidney Injury (AKI)? Acute Kidney injury is a rapid fall in kidney function in a person who has become unwell. It can happen over hours or
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Acid Base Balance by: Susan Mberenga RN, BSN, MSN
 Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Correction of hypervolaemic hypernatraemia by inducing negative Na + and K + balance in excess of negative water balance: a new quantitative approach
 Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Objectives Body Fluids Electrolytes The Kidney and formation of urine
 Objectives Body Fluids Outline the functions of water in the body. State how water content varies with age and sex. Differentiate between intracellular and extra-cellular fluid. Explain how water moves
Objectives Body Fluids Outline the functions of water in the body. State how water content varies with age and sex. Differentiate between intracellular and extra-cellular fluid. Explain how water moves
Use the following diagram to answer the next question. 1. In the diagram above, pressure filtration occurs in a. W b. X c. Y d. Z
 Part A: Multiple Choice Questions Value: 32 Marks Suggested time: 40 minutes Instructions: For each question select the best answer and record your choice on the Scantron card provided. Using an HB pencil,
Part A: Multiple Choice Questions Value: 32 Marks Suggested time: 40 minutes Instructions: For each question select the best answer and record your choice on the Scantron card provided. Using an HB pencil,
Mannitol-induced Metabolic Alkalosis
 Electrolyte & Blood Pressure :, 00 ) Mannitolinduced Metabolic Alkalosis Kyung Pyo Kang, M.D., Sik Lee, M.D., Kyung Hoon Lee, M.D., and Sung Kyew Kang, M.D. Department of Internal Medicine, Research Institute
Electrolyte & Blood Pressure :, 00 ) Mannitolinduced Metabolic Alkalosis Kyung Pyo Kang, M.D., Sik Lee, M.D., Kyung Hoon Lee, M.D., and Sung Kyew Kang, M.D. Department of Internal Medicine, Research Institute
Package leaflet: Information for the user. Nocdurna 25 microgram oral lyophilisate Nocdurna 50 microgram oral lyophilisate.
 Package leaflet: Information for the user Nocdurna 25 microgram oral lyophilisate Nocdurna 50 microgram oral lyophilisate desmopressin Read all of this leaflet carefully before you start taking this medicine
Package leaflet: Information for the user Nocdurna 25 microgram oral lyophilisate Nocdurna 50 microgram oral lyophilisate desmopressin Read all of this leaflet carefully before you start taking this medicine
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
LESSON ASSIGNMENT. After completing this lesson, you will be able to: 4-1. Identify the general characteristics of diuretics.
 LESSON ASSIGNMENT LESSON 4 Diuretics. LESSON ASSIGNMENT Paragraphs 4-1 through 4-6. LESSON OBJECTIVES After completing this lesson, you will be able to: 4-1. Identify the general characteristics of diuretics.
LESSON ASSIGNMENT LESSON 4 Diuretics. LESSON ASSIGNMENT Paragraphs 4-1 through 4-6. LESSON OBJECTIVES After completing this lesson, you will be able to: 4-1. Identify the general characteristics of diuretics.
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
hyponatremia/hypo-osmolality/hypotonic dehydration
 E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
E87.1 Hypo-osmolality and hyponatremia CC Diagnosis: hyponatremia/hypo-osmolality/hypotonic dehydration Discussion is decreased sodium level in the blood. Serum osmolarity is low in true hyposmolar hyponatremia.
Acute Kidney Injury. Eleanor Haskey BSc(hons) RVN VTS(ECC) VPAC A1
 RVN VTS(ECC) VPAC A1") Acute Kidney Injury Eleanor Haskey BSc(hons) RVN VTS(ECC) VPAC A1 Anatomy and Physiology The role of the kidneys is to filter the blood through the glomerulus to form filtrate. The filtrate is then reabsorbed
Acute Kidney Injury Eleanor Haskey BSc(hons) RVN VTS(ECC) VPAC A1 Anatomy and Physiology The role of the kidneys is to filter the blood through the glomerulus to form filtrate. The filtrate is then reabsorbed
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Hyponatremia Clinical Significance. Ágnes Haris MD PhD, St. Margit Hospital, Budapest
 Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Suboptimal hydration harms patients.
 Suboptimal hydration harms patients. NHS Fife is committed to improving hydration management. To achieve this we need your help! In 2014 new fluid balance charts were implemented in the Victoria Hospital,
Suboptimal hydration harms patients. NHS Fife is committed to improving hydration management. To achieve this we need your help! In 2014 new fluid balance charts were implemented in the Victoria Hospital,
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Treating the syndrome of inappropriate ADH secretion with isotonic saline
 Q J Med 1998; 91:749 753 Treating the syndrome of inappropriate ADH secretion with isotonic saline W. MUSCH and G. DECAUX1 From the Department of Internal Medicine, Bracops Hospital, Brussels, and 1Department
Q J Med 1998; 91:749 753 Treating the syndrome of inappropriate ADH secretion with isotonic saline W. MUSCH and G. DECAUX1 From the Department of Internal Medicine, Bracops Hospital, Brussels, and 1Department
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year One Developed Summer 2017 Overview Basic A & P of: Urinary system Kidneys Followed by: Introduction to Acute Kidney Injury Urinary System The
Acute Kidney Injury (AKI) Undergraduate nurse education Year One Developed Summer 2017 Overview Basic A & P of: Urinary system Kidneys Followed by: Introduction to Acute Kidney Injury Urinary System The
Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are
 Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017
 ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
Extracellular fluid (ECF) compartment volume control
 compartment volume control") Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Water Balance Made Easier Joon K. Choi, DO. Extracellular fluid (ECF) compartment volume control Humans regulate ECF volume mainly by regulating body sodium content. Several major systems work together
Management of the patient with established AKI. Kelly Wright Lead Nurse for AKI King s College Hospital
 Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
0.45% Sodium Chloride Injection, USP
 PRESCRIBING INFORMATION 0.45% Sodium Chloride Injection, USP IV Fluid and Electrolyte Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision: November 22, 2013 Submission Control
PRESCRIBING INFORMATION 0.45% Sodium Chloride Injection, USP IV Fluid and Electrolyte Replenisher Baxter Corporation Mississauga, Ontario L5N 0C2 Canada Date of Revision: November 22, 2013 Submission Control
Disclaimer. Chapter 3 Disorder of Water, Electrolyte and Acid-base Professor A. S. Alhomida. Disorder of Water and Electrolyte
 Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Ricky Bell Renal/ICM Registrar
 Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
Samsca. Samsca (tolvaptan) Description
 Description") Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
Each tablet contains:
 Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Brunel Health Core Ten Results for Sam Witter. Thank you for submitting a sample of your blood to be tested by Brunel Health.
 Brunel Health Core Ten Results for Sam Witter Dear Sam, Thank you for submitting a sample of your blood to be tested by Brunel Health. We are pleased to say that there was enough viable sample to test
Brunel Health Core Ten Results for Sam Witter Dear Sam, Thank you for submitting a sample of your blood to be tested by Brunel Health. We are pleased to say that there was enough viable sample to test
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Hyponatremia in Children with Acute Central Nervous System Diseases
 Bahrain Medical Bulletin, Volume 30, No 1, March 2008 Hyponatremia in Children with Acute Central Nervous System Diseases Lamia M Al Naama, PhD* Meaad Kadhum Hassan, CABP** Entisar A. Al Shawi, MSc***
Bahrain Medical Bulletin, Volume 30, No 1, March 2008 Hyponatremia in Children with Acute Central Nervous System Diseases Lamia M Al Naama, PhD* Meaad Kadhum Hassan, CABP** Entisar A. Al Shawi, MSc***
SODIUM BALANCE Overview
 SODIUM BALANCE Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS III Seminar VJ Temple 1 How are solute and solvent related to solution?
SODIUM BALANCE Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS III Seminar VJ Temple 1 How are solute and solvent related to solution?
Essential Shared Care Agreement: Lithium
 Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/