Hyponatremia and Hypomagnesemia
|
|
|
- Wilfred Hampton
- 5 years ago
- Views:
Transcription
1 Hyponatremia and Hypomagnesemia Dre Kathy Ferguson,nephrologist


2 Hyponatremia Salt and water imbalance Management Acute vs chronic
3 Approach! How to make the correct diagnosis?! How to treat safely?
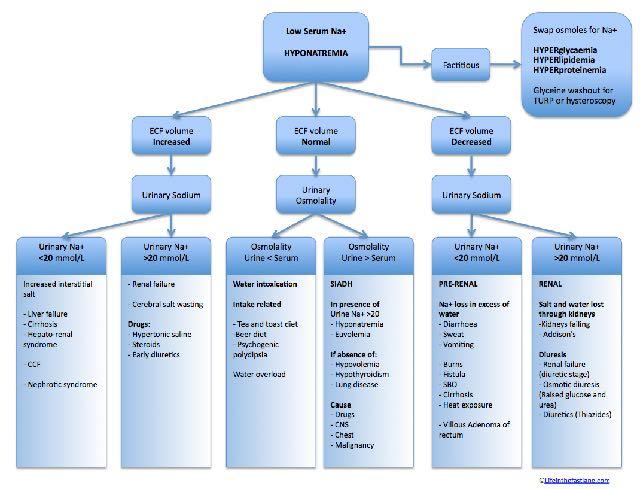
4 Etiology! Classification: volume status! Classification: serum osmolality! History and physical exam! List of medications! Serum: Bun, creat, lytes, glucose, osmolality! Urinary: Na, osmolality
5
6 High ADH! Hypovolemic hyponatremia! Extrarenal: Una <20 and Uosm >300! Renal: ex: diuretics Una>20! Euvolemic hyponatremia! SIADH, Hypothyroidism, Adrenal insufficiency! Una > 20, Uosm >200! Hypervolemic hyponatremia! CHF, Cirrhosis, Nephrotic syndrome! Una <20 and Uosm >300! Careful when more then one etiology!! Misleading!
7 Not related to ADH! CRF! Primary Polydipsie ( Una<20, Uosm )! Beer Potomanie( low solute load-roh)! Tea and toast ( low solute load)
8 Acute vs chronic! Acute HypoNa:! Cerebral edema! Nausea, malaise, headache, lethargy, seizures, coma! Chronic HypoNa:! Impaired cognition! Attention deficit! Gait instability and falls in elderly! Osteoporosis


9 Acute Hyponatremia
10
11 Treatment Chronic (>48hrs)! Fear Osmotic Demyelination Syndrome(ODS)! Confusion, diorientation, coma and seizures! Behavioral changes! Dysarthria,Dysphagia! Paraparesis, quadrapareris! Locked in! Prevention! Correction 8 meq/24 hrs and 18 meq/48 hrs! Risk greater if Na < 120! Follow Na q 2-4 hrs! D5% or Desmopressin if overcorrection
12 Prevention ODS and treatment If overcorrection! D5%( 6ml/kg x 2 hrs)! DDAVP 2microg iv or sc q 6hrs prn! Aim for your 24 and 48 hrs goal( 8 and 18 meq)! High risk group aim 6 meq/24 hrs:! Alcoholism, liver disease, malnutrition, hypok, Na <105
13 86 yo lady! RA: Compression fracture of T6! Symptoms of dizziness, nausea and disorientation! Past history: HTN, DM 2, depression! Medications: Hydrodiuril 25 mg qd( 10 years)! Glyburide 5 mg bid( 10 years)! Oxybutynin 4 mg/day ( 5 years)! Bethahistine 8 mg tid ( 1 week)! Domperidone 10 mg tid (1 week)! lorazepam 0.5 mg/day ( 10 years)! duloxetine 20 mg/day ( 2 weeks! LABS: Na 116 meq/l ( )
14 ! Visit to family physician 2 weeks ago:! Duloxetine prescribed for depression! Visit to the clinic 1 week ago! Betahistine and motilium for nausea, vertigo! Admited following a fall, complaining of nausea, disorientation! Labs: Na 116 K 3.2 Bun 8 Creat 70 Osmolality 239! Urine Osm: 385 Una 32! Dx?! How to treat?
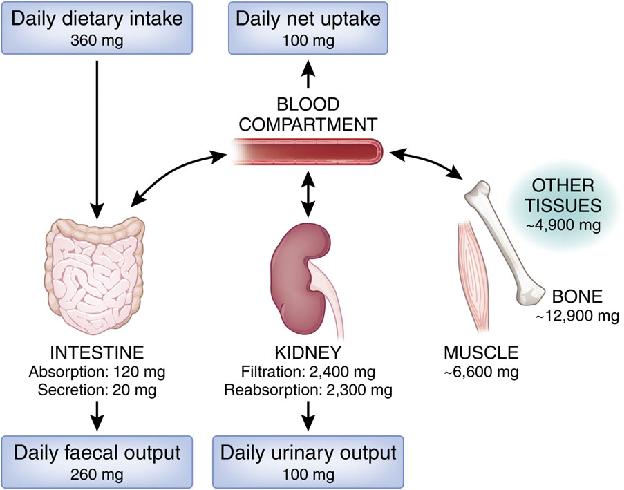
15
16 SIADH! Stop HCTZ! Fluid restriction 800 ml to 1000 ml! NaCL in diet and NaCl tablets! +- Loop Diuretics ( Osm >500)! NaCl 3% if symptomatic! V2receptor antagonist: Tolvaptan! $$, rapid correction, no clear role

17 Tolvaptan( V2 receptor Antagonist CHF Cirrhosis SIADH ADPKD $$$ Overly rapid correction!! Inadequate if neuro sx Do not use with NaCl 3% Monitoring of liver enzymes

18 Hypomagnesemia When to measure!? Importance of correction!?
19 Hypomagnesemia! What is the etiology?! What else should I look for?! How can I prevent?! How do I treat?
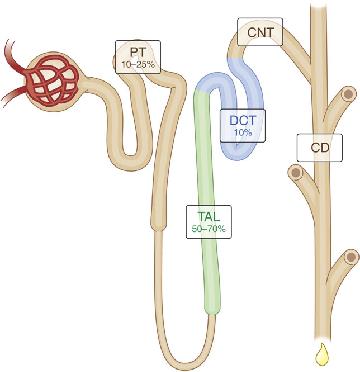
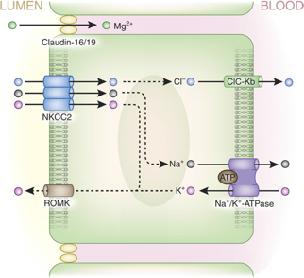
20 Kidney Mg Reabsorption
21
22 Physiology! Mg balance related to Ca,K+! Nature s physiologic CCB! Cofactor for the intracellular Na-K pump
23 Etiology! Gastrointestinal! Diarrhea, malabsorption, steatorrhea, small bowel surgery! Acute pancreatitis! PPI! Genetic! Poor intake! ROH ( Thiamine increase Mg deficiency!)! Parenteral nutrition
24 Etiology! Renal loss! Medications! Diuretics( loop,thiazide), Aminoglycoside, AmphoB, pentamidine, Calcineurin inh, Cisplatin, Chemotxcetuximab! Volume expansion! DM uncontrolled! ROH! HyperCa! Tubular dysfonction! Post ATN, Post obstruction, post tranplant! Bartter/Gitelman syndrome! Isolated hypomg, Familial HypoMg, HyperCa

25 Signs and symptoms! Asymptomatic! Cognitive impairment! Seizures-coma! Muscular! Cardiac:! arrythmia,! hypertension, IHD! Insuline resistance
26 When to measure in asymptomatic patient! DM! PPI! Chronic Diarrhea! Diuretics, aminoglycoside, chemotx, calcineurin inhibitor! Hypokalemia! Hypo or hypercalcemia! Malnourished! ICU! Acute MI
27 Evaluation! FeMg = Umg x PCr x 100%! Lytes, HCO3! Ca,PO4,alb! Bun, Creat! Gluc (0.7x PMg) x Ucr Above 2%: Mg renal loss
28 Treatment! GI loss:! Treat the diarrhea! Consider stopping PPI! Supplements po or iv( symptoms, tolerance)! MgCl better tolerated and more effective! Renal! Treat the cause if possible! Supplements: po or iv ( symptoms, tolerance)! Consider amiloride
29 Treatment! Severe symptoms: torsade de pointes! 1-2 g MgSO4: 4-8 mmol in 15 min then infusion( 4-8 g iv over hrs)! Severe neuromuscular symptoms: tetany! 1-2 g iv over min then infusion! Start po as soon as possible! IV Mg inhibits reabsorption Mg in loop of Henley
30 Treatment! Mg < 0.4 mmo/ll: give 4-8 g ( mmol)! Mg 0,4 0,6 mmol/l: 2-4 g ( 8-16 mmol)! Mg 0,6-0,8 mmol/l: 1-2 g ( 4-8 mmol)
31 57 yo patient! RC: Muscle spasm and weakness! Past hx: DM 2, GERD, IHD, HTN, alcoholism! Medications:! Metformin 1g bid! Gliclazide 80 mg bid! Pantoprazole 40 mg qd! Ramipril 10 mg qd! Bisoprolol 5 mg qd! Furosemide 20 mg qd! ASA 81 mg qd! Labs: Mg 0,33 mmol/l (0,71-0,94)

32 BP 190/ yo K 3.4 mmol/l Ca 1.97 mmol/l Creatinine 80 mmol/l FeMg 1% HbA1c: 7,1% HypoMg corrected after metformin stopped!
33 Conclusion! Severe HypoNa can be fatal! Chronic HypoNa as consequences! Treat cautiously! HypoMg is not always asymptomatic! Look for HypoMg in patient at risk! Correct if symptoms, below 0,6 mmol/l or if other risk factors of complications!

34 Thanks-Merci!
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Electrolyte Emergencies
 Electrolyte Emergencies Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia Hyponatremia Symptomatic: headaches,
Electrolyte Emergencies Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia Hyponatremia Symptomatic: headaches,
Hyponatraemia. Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals
 Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatraemia Dr Andy Lewington Consultant Nephrologist/Honorary Clinical Associate Professor Leeds Teaching Hospitals A.J.P.Lewington@leeds.ac.uk Disclosures of Interest Associate Clinical Director NIHR
Hyponatremia FOSPED 2018
 Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Hyponatremia FOSPED 2018 Prof. Dr. Mirjam Christ-Crain Department of Endocrinology, Diabetology and Metabolism University Hospital Basel Schweizerische Gesellschaft für Endokrinologie und Diabetologie
Workshop on Hyponatremia
 Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Workshop on Hyponatremia Debbie Rosenbaum MDCM FRCPc University of British Columbia Rocky Mountain / ACP Internal Medicine Meeting November 13 2009 Objectives Approach to diagnosis of hyponatremia Acute
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
SAMSCA (tolvaptan) oral tablet
 oral tablet") SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAMSCA (tolvaptan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
IX: Electrolytes. Sodium disorders. Specific Learning Objectives: Dan Henry, MD Clerkship Director University of Connecticut School of Medicine
 IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:
![[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:](/thumbs/73/69178995.jpg "[ Na+] COI Disclosure OBJECTIVES. By the end of the session, and upon further learning and reflection participants should be able to:") COI Disclosure Busting Myths and de-mist-ifying its Assessment & Management Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP Faculty of Pharmaceutical Sciences The University of British Columbia Lower
COI Disclosure Busting Myths and de-mist-ifying its Assessment & Management Peter Loewen B.Sc.(Pharm), ACPR, Pharm.D., FCSHP Faculty of Pharmaceutical Sciences The University of British Columbia Lower
Hyponatremia Clinical Significance. Ágnes Haris MD PhD, St. Margit Hospital, Budapest
 Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA
 Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Consultant emergency medicine Security Forces Hospital Ministry of Interior KSA Why Electrolytes are Important? IMMEDIATE LIFE THREAT. You can Save or KILL the patient fixing it. USEFUL CLUE to the UNDERLYING
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
BEFORE the session. Sodium & Water Assessment & Therapeutics. LMPS Residents
 BEFORE the session 1. Get Loewen s Sodium & Water Assessment & Therapeutics 1-pager at www.peterloewen.com/made 2. Read McGee S, Abernethy WB, Simel DL. Is this patient hypovolemic? JAMA 1999;281:1022-9
BEFORE the session 1. Get Loewen s Sodium & Water Assessment & Therapeutics 1-pager at www.peterloewen.com/made 2. Read McGee S, Abernethy WB, Simel DL. Is this patient hypovolemic? JAMA 1999;281:1022-9
Neurohypophysis. AVP Receptors. Hyponatremia in Pituitary Disorders 9/29/2016. Lewis S. Blevins, Jr., M.D.
 in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
in Pituitary Disorders Lewis S. Blevins, Jr., M.D. Neurohypophysis AVP secreting neurons in SON and PVN Osmo- and thirst receptors/centers in anterior hypothalamus Ascending pathways from ANS and brainstem
Workshop CME 22 mars Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles
 Workshop CME 22 mars 2013 Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles Overcorrection of chronic hyponatremia CASE REPORT I (1) Female 71 year Altered
Workshop CME 22 mars 2013 Pr Alain SOUPART Service de Médecine Interne Général Cliniques Universitaires Erasme, Bruxelles Overcorrection of chronic hyponatremia CASE REPORT I (1) Female 71 year Altered
NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
SATURDAY PRESENTATIONS
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY PRESENTATIONS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS Annual Meeting
 Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
Carolinas Chapter - American Association of Clinical Endocrinologists SATURDAY HANDOUTS 2018 Annual Meeting September 7-9, 2018 Kiawah Island Golf Resort Kiawah Island, SC This continuing medical education
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
Hyponatremia 11/4/2010. Learning Objectives
 JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
JAMES S. KALUS, PHARM.D, BCPS (AQ-CARDIOLOGY) Senior Manager, Patient Care Services, Department of Pharmacy Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE ANGELA STEWART, PHARM.D,
For more information about how to cite these materials visit
 Author(s): Roger Grekin, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Roger Grekin, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Case Studies of Electrolyte Disorders ACOI Board Review Mark D. Baldwin D.O. FACOI
 Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Case Studies of Electrolyte Disorders ACOI Board Review 2018 Mark D. Baldwin D.O. FACOI Disclosures None, just working for The Man Question 1 The first thing in evaluating a patient who has a disorder
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Samsca. Samsca (tolvaptan) Description
 Description") Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
Subject: Samsca Page: 1 of 5 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Last Review Date: September 20, 2018 Samsca Description Samsca (tolvaptan)
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Taking Tolvaptan with a grain of salt. Jia (Shermaine) Ngo LMPS Pharmacy Resident October 7, 2016
 Ngo LMPS Pharmacy Resident October 7, 2016") Taking Tolvaptan with a grain of salt Jia (Shermaine) Ngo LMPS Pharmacy Resident 2016-2017 October 7, 2016 1 Learning Objectives Define Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Taking Tolvaptan with a grain of salt Jia (Shermaine) Ngo LMPS Pharmacy Resident 2016-2017 October 7, 2016 1 Learning Objectives Define Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
Disorders of Water Metabolism
 Disorders of Water Metabolism Joshua M. Thurman and Tomas Berl 2 Introduction Disorders of water balance and serum Na ( S Na ) are very common in hospitalized patients [ 1 ]. In health, water balance and
Disorders of Water Metabolism Joshua M. Thurman and Tomas Berl 2 Introduction Disorders of water balance and serum Na ( S Na ) are very common in hospitalized patients [ 1 ]. In health, water balance and
11/4/2010. Learning Objectives. Question 1. Question 2 PLEASE ANSWER THE HYPONATREMIA PRE-ACTIVITY TEST QUESTIONS. A. True B.
 Faculty Disclosures James S. Kalus, PharmD, BCPS (AQ CV) Senior Manager, Patient Care Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE Saturday, October 23, 2010 Hemant Dhingra, MD
Faculty Disclosures James S. Kalus, PharmD, BCPS (AQ CV) Senior Manager, Patient Care Services Henry Ford Hospital, Detroit, MI NO RELATIONSHIPS TO DISCLOSE Saturday, October 23, 2010 Hemant Dhingra, MD
Objectives. Objectives
 Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Diagnosis & Management of Electrolyte & Acid Base Disturbances In the Acute Care Sophia Chu Rodgers, FNP, ACNP, FAANP, FCCM University of New Mexico Sandoval Regional Medical Center Albuquerque, New Mexico
Sym pt om s of "hyponat rem ia" Serum [Na + ] m Eq/ L: - Asymptomatic
![Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic](/thumbs/94/122329913.jpg "Sym pt om s of hyponat rem ia Serum [Na + ] m Eq/ L: - Asymptomatic") Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
Sym pt om s of "" Serum [Na + ] >130 m Eq/ L: - Asymptomatic Serum [Na + ] 120-130 m Eq/ L: - Nausea, vomiting - Fatigue, muscle cramps - Abdominal symptoms - Mild cognitive - Gait disturbances Serum [Na
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital
 JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
JUAN MIGUEL GIL R. ORTIZ, MD, FPCP, FPSN University of Santo Tomas Hospital HYPONATREMIA Hb 88 Creatinine 7 Na 130 K 5.8 Nonhypotonic Hyponatremia 1. Pseudohyponatremia 2. Presence of non-na effective
Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
 Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Case Reports in Nephrology Volume 2013, Article ID 801575, 4 pages http://dx.doi.org/10.1155/2013/801575 Case Report Tolvaptan in the Treatment of Acute Hyponatremia Associated with Acute Kidney Injury
Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC.
 Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC. Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to
Common Metabolic Abnormalities DR. SANJAY PANDEYA MD. FRCPC. Objectives 1. Review approach to hyponatremia Physiology & pathophysiology review Case-based common clinical questions Three-step process to
Supplemental Information
 FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
CCRN/PCCN Review Course May 30, 2013
 A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Public Assessment Report. Scientific discussion. Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR
 SE/H/1443/01/MR") Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
Public Assessment Report Scientific discussion Natriumklorid Abcur (sodium chloride) SE/H/1443/01/MR This module reflects the scientific discussion for the approval of Natriumklorid Abcur. The procedure
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Severe electrolyte- and acid-base disorders. GIC oktober 2013
 Severe electrolyte- and acid-base disorders GIC oktober 2013 Case (1) 19-year-old male, 60 kg Fever persisting for 1 month Cough and chest congestion for 10 days Lethargy for 1 week Admitted with diagnosis
Severe electrolyte- and acid-base disorders GIC oktober 2013 Case (1) 19-year-old male, 60 kg Fever persisting for 1 month Cough and chest congestion for 10 days Lethargy for 1 week Admitted with diagnosis
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic
Volume and Electrolytes. Fluid and Electrolyte Management. Why 125ml? Question. Normal fluid requirement. Normal losses
 Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Fluid and electrolyte abnormalities. Melanie P. Hoenig (Derman) Associate Professor BIDMC
 Associate Professor BIDMC") Fluid and electrolyte abnormalities Melanie P. Hoenig (Derman) Associate Professor BIDMC Disclosures: Editor, Kidney Self Assessment Program American Society of Nephrology Hyponatremia* Hypernatremia Hyperkalemia
Fluid and electrolyte abnormalities Melanie P. Hoenig (Derman) Associate Professor BIDMC Disclosures: Editor, Kidney Self Assessment Program American Society of Nephrology Hyponatremia* Hypernatremia Hyperkalemia
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Hyponatremia: A Review
 Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Analytic Review Hyponatremia: A Review Mary Ansley Buffington, MD, JD 1 and Kenneth Abreo, MD 1 Journal of Intensive Care Medicine 2016, Vol. 31(4) 223-236 ª The Author(s) 2015 Reprints and permission:
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Empowering Pharmacists to Improve Management of Hyponatremia. Learning Objectives. Diagnostic Algorithm for Hyponatremia
 Empowering Pharmacists to Improve Management of Hyponatremia A Patient-Centric, Process of Care Guide Learning Objectives Discuss the clinical consequences of undertreatment of hyponatremia, including
Empowering Pharmacists to Improve Management of Hyponatremia A Patient-Centric, Process of Care Guide Learning Objectives Discuss the clinical consequences of undertreatment of hyponatremia, including
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต
 Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต Content : Electrolyte Emergency!! Serum sodium Normal serum sodium: 135-145 meq/l Normal serum osmolality: 285-295 mosm/l Normal urine sodium: 10-20
Electrolyte imbalance พญ.วราภรณ เล ยวนรเศรษฐ หน วยโรคไต Content : Electrolyte Emergency!! Serum sodium Normal serum sodium: 135-145 meq/l Normal serum osmolality: 285-295 mosm/l Normal urine sodium: 10-20
NHS Grampian Staff Guidance For The Management Of Hypomagnesaemia In Adults. Consultation Group: See Page 4. Review Date: June 2021
 NHS...... Grampian NHS Grampian Staff Guidance For The Management Of Hypomagnesaemia In Adults Co-ordinators: Consultation Group: Approver:. Senior Medicines Information Pharmacist See Page 4 Medicine
NHS...... Grampian NHS Grampian Staff Guidance For The Management Of Hypomagnesaemia In Adults Co-ordinators: Consultation Group: Approver:. Senior Medicines Information Pharmacist See Page 4 Medicine
2018/6/7 APSN/JSN CME Course Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6
 2018/6/7 APSN/JSN CME Course 2018 Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6 Case1 77F Left leg pain Na 112 Case2 39M Seizure Na 117 Case3 73M General malaise Na 120 Case1
2018/6/7 APSN/JSN CME Course 2018 Division of Nephrology St. Luke s International Hospital Raku Son M.D., PGY6 Case1 77F Left leg pain Na 112 Case2 39M Seizure Na 117 Case3 73M General malaise Na 120 Case1
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Fluids, Electrolytes, and Nutrition
 Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
CLINICAL GUIDELINES ID TAG
 CLINICAL GUIDELINES ID TAG Title: Treatment of Hypomagnesaemia in adults Author: Speciality / Division: Directorate: Dr Peter Sharpe, Dr Neal Morgan, Jillian Redpath Chemical Pathology/Nephrology/Pharmacy
CLINICAL GUIDELINES ID TAG Title: Treatment of Hypomagnesaemia in adults Author: Speciality / Division: Directorate: Dr Peter Sharpe, Dr Neal Morgan, Jillian Redpath Chemical Pathology/Nephrology/Pharmacy
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
ORIGINAL ARTICLE HYPONATREMIA IN ELDERLY *Dr. T. Prabhu. Annamalai University, Annamalainagar , Tamilnadu, India
 Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 2, Issue 10, pp 325-332, October, 2014 ORIGINAL ARTICLE
Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 2, Issue 10, pp 325-332, October, 2014 ORIGINAL ARTICLE
Hyponatremia as a Cardiovascular Biomarker
 Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Hyponatremia as a Cardiovascular Biomarker Uri Elkayam, MD Professor of Medicine University of Southern California Keck School of Medicine elkayam@usc.edu Disclosure Research grant from Otsuka for the
Remember Taking Care of Patients & Managing Electrolytes is a Team Sport! EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities
 EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities 11 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Clinical Professor of Medicine Nephrology
EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities 11 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Clinical Professor of Medicine Nephrology
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Kidneys in regulation of homeostasis
 Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Updates in Therapeutics 2015:
 Updates in Therapeutics 2015: The Pharmacotherapy Preparatory Review & Recertification Course Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, PharmD, BCPS University of Tennessee, Knoxville, TN
Updates in Therapeutics 2015: The Pharmacotherapy Preparatory Review & Recertification Course Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, PharmD, BCPS University of Tennessee, Knoxville, TN
VanderbiltEM.com. ACEP 2013 Electrolyte Emergencies. Mastering Emergency Medicine. Electrolyte Emergency Questions. Electrolyte Emergency Questions
 ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Acids, Bases, and Salts
 Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.