Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
|
|
|
- Buck Kennedy
- 5 years ago
- Views:
Transcription
1 Dr. Rezzan Khan Consultant Nutritionist Shifa International Hospital
2
3 Concept of Fluid & Electrolyte Balance Body fluid and electrolyte homeostasis Differentiate between hypovolemic, euvolemic, and hypervolemic hyponatremia Recommend appropriate changes in nutrition support formulations for treatment of electrolyte abnormalities
4 Fluid balance ensures that the body stays hydrated; important for normal functioning of the body and optimal health. Maintaining fluid balance is vital for physical and mental performance. Water is one of the most essential nutrients that the body requires.
5 Why Fluid balance is important Loss of 10% body fluid = 8% weight loss SERIOUS Loss of 20% body fluid = 15% weight loss FATAL Fluid gained each day should = fluid lost each day (2-3L/day average) What is the minimum output per hour necessary to maintain renal function? 30 ml/hr
6 Age Infants Older adults Prior medical history Acute illness Chronic illness Environmental factors Diet Lifestyle Medications
7 Fetus: 90% water Premie: 80% water Term: 70-75% water Young children: 65-70% Adolescents: 60% water Lean individuals: greater percentage of body weight is water Fat individuals: smaller percentage of body weight is water
8 Method Body Surface Area (BSA) Method Recommended Dietary Allowance/Adolph Method Fluid Balance Method Weight Method Equation 1,500 ml/m2 x BSA = ml/day 1 ml/kcal of intake = ml/day Urine output ml/day ml/kg/day Age-adjusted Weight Method Average healthy adult: ml/kg/day Adult years old: 30 ml/kg/day Adult > 65 years old: 25 ml/kg/day Obese Adult Patient Method [(kg body weight 20) x 15] + 1,500 ml/day
9 Afebrile 70-kg Adult: 35 ml/kg/24 h If not a 70-kg Adult: Calculate the water requirement according to Kg Method? For the first 10 kg of body weight: 100 ml/kg/d plus For the second 10 kg of body weight: 50 ml/kg/d plus For the weight above 20 kg: 20 ml/kg/d
10 State of equilibrium in body Naturally maintained by adaptive responses Body fluids and electrolytes are maintained within narrow limits
11 *Effective circulating volume

12 *Effective circulating volume
13 *Effective circulating volume
14
15
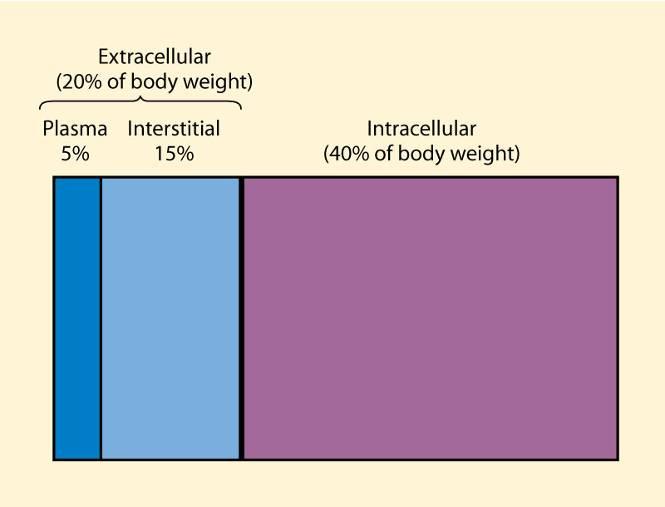
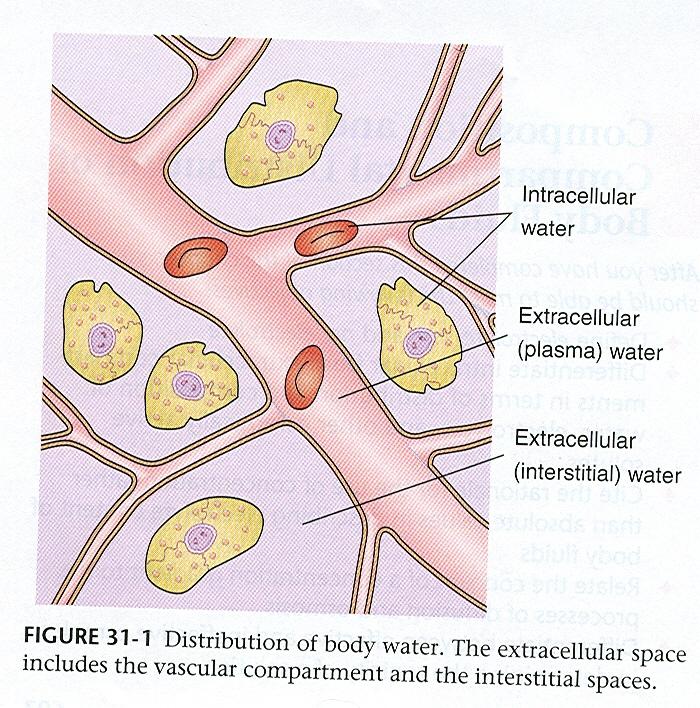
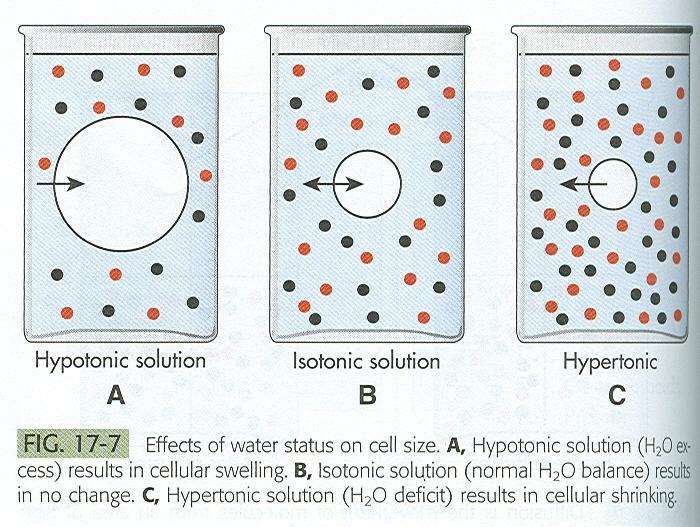
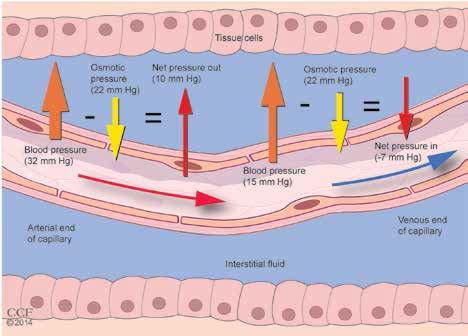
16 The intravascular volume of an average 70 kg man is approximately 5 L of which 2 L is red cell volume and 3 L plasma volume. The intravascular, extracellular fluid compartment equilibrates with the extracellular, extravascular fluid compartment (ECF 11 L), with a reduction in one compartment leading to a reduction of the other. Plasma to interstitial fluid shift results in edema Water deficit (increased ECF) Associated with symptoms that result from cell shrinkage as water is pulled into vascular system Water excess (decreased ECF) Develops from gain or retention of excess water
17 Plasma to interstitial fluid shift results in edema Water deficit (increased ECF) Associated with symptoms that result from cell shrinkage as water is pulled into vascular system Water excess (decreased ECF) Develops from gain or retention of excess water

18 First spacing Normal distribution of fluid in ICF and ECF Second spacing Abnormal accumulation of interstitial fluid (edema) Third spacing Fluid accumulation in part of body where it is not easily exchanged with ECF; fluid trapped and unavailable for functional use (ascites)


19 .
20
21 Treating an ECF requires aggressive management of sepsis, fluid, and renal function; nutritional, electrolyte, and metabolic support; management of fistula output; assessment of fistula anatomy; and when appropriate, corrective surgery.
22 Hypovolemia Hypervolemia Hypoproteinemia Definition Extracellular fluid deficit Extracellular fluid excess Loss of oncotic pressure leads to hypovolemia Causes Congestive heart failure Decreased protein intake Hemorrhage Increased protein loss Overdiuresis Renal failure Liver/kidney disease Vomiting/diarrhea Liver disease Burns Third-spacing Overzealous IV fluids Infection (ascites, burns) Sodium overload Hemorrhage Clinical Dry mucous membranes findings Sudden weight loss Oliguria Tachycardia Orthostatic hypotension
23 Type Isotonic Hypertonic Hypotonic Description and Causes Equal loss of sodium and water Gastrointestinal illness Most common cause Water loss exceeds sodium loss Fever Limited fluid intake Sodium loss exceeds water loss Diuretic use
24 Common Causes Hemorrhage Vomiting Diarrhea Burns Diuretic therapy Fever Impaired thirst
25 Signs/Symptoms Weight loss Thirst Orthostatic changes in pulse rate and bp Weak, rapid pulse Decreased urine output Dry mucous membranes Poor skin turgor
26 Encourage patient fluid intake of 1,000 3,000 ml daily (e.g., filling a pitcher each day and making sure it is empty at the end of the day) Monitor patient lab values for changes. Increased BUN/creatinine Increased serum sodium Increased serum osmolarity Increased hematocrit. Monitor patient urine output. Monitor patient for constipation or diarrhea. Weigh patient daily. Teach patient to drink despite not feeling thirsty, particularly if taking diuretics. Advise patient to avoid alcoholic, carbonated, and caffeinated beverages, which can increase diuresis.
27 Fluid Management Diet therapy Mild to moderate dehydration. Correct with oral fluid replacement. Oral rehydration therapy Solutions containing glucose and electrolytes. E.g., Pedialyte, Rehydralyte. IV therapy Type of fluid ordered depends on the type of dehydration and the clients cardiovascular status.
28
29 Common Causes: Congestive Heart Failure Early renal failure IV therapy Excessive sodium ingestion SIADH Corticosteroid
30 Signs/Symptoms Increased BP Bounding pulse Venous distention Pulmonary edema Dyspnea Orthopnea (diff. breathing when supine) crackles
31 Drug therapy Diuretics may be ordered if renal failure is not the cause. Restriction of sodium and saline intake I/O Weight
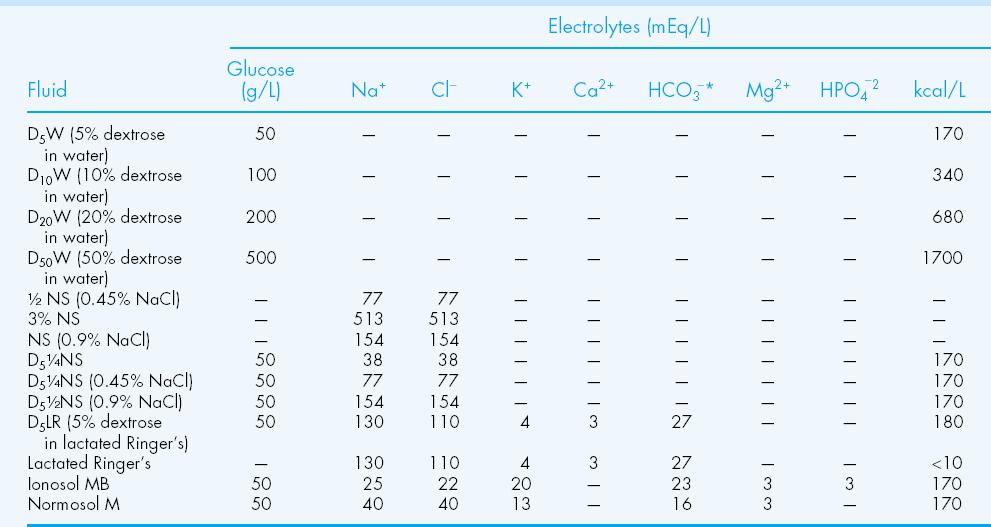
32 Gastric Loss (Nasogastric Tube, Emesis): D5 1/2 NS with 20 meq/l (mmol/l)potassium chloride (KCl) Diarrhea: D5LR with 15 meq/l (mmol/l) KCl. Use body weight as a replacement guide (about 1 L for each 1 kg, or 2.2 lb, lost)
33 Normal Saline (0.9%) (Na 154 meq/l, Cl 154 meq/l) Lactate Ringer's (Hartman's solution) (Na 130 meq/l, Cl 109 meq/l, K 4 meq/l, Lactate 28 meq/l, Ca 3 meq/l) Normosol-R (Na 140 meq/l, Cl 90 meq/l, K 5 meq/l, Mg 3 meq/l) Plasmalyte (Na 140 meq/l, Cl 98 meq/l, K 5 meq/l, Mg 3 meq/l)
34
35
36

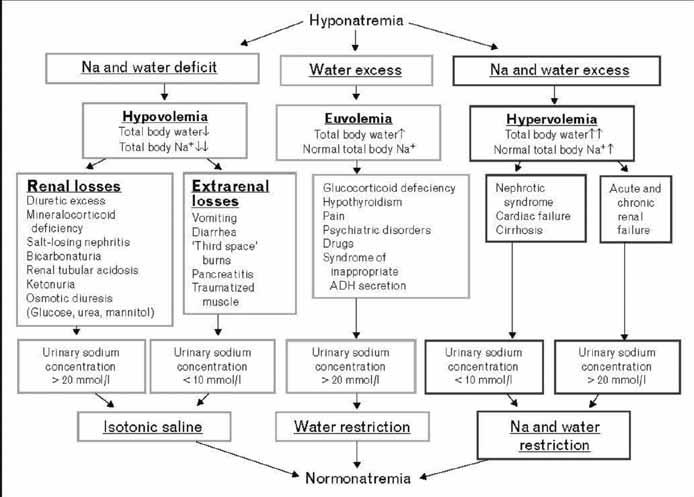
37 The goal is to find and correct the underlying cause. 1. Determine presence and severity of signs and symptoms. 2. Determine speed of onset: acute onset necessitates rapid correction of sodium; chronic onset necessitates slow correction of sodium. 3. Determine osmolality (tonicity): rule out isotonic and hypertonic osmolality. 4. Establish extracellular fluid volume status.
38 Serum Sodium Concentrations Symptoms 125 to 130 meq/l No symptoms, nausea, malaise, vomiting,disorientation 115 to 125 meq/l Headache, lethargy,obtunded, agitation, confusion, altered mental status <115 meq/l Seizures, coma, respiratory distress, death Symptoms vary widely and are patient-specific. Sodium and Fluids Disorders, Clinical Nutrition Week 2012,
39 Initial Data: 49-year-old female Weight: 50 kg Plasma sodium day 1: 123 meq/l Plasma sodium day 2: 126 meq/l Day 1 IV fluids: 1 L normal saline (sodium content is 154 meq/l) (3) Day 2 IV fluids: 1.5 L normal saline Step 1: Calculate total body water Total Body Water (TBW) for men: 0.6 L/kg x weight in kg Total Body Water (TBW) for women: 0.5 L/kg x weight in kg (3) Calculation for DD: 0.5 x 50 = 25 L Step 2: Calculate sodium deficit Sodium deficit : TBW x ([desired plasma sodium current plasma sodium])*(3) Calculation for DD: 25 x ( ) = 25 x 10 = 250 meq Step 3: Calculate how much 1 L normal saline** initially increases plasma sodium (7): Increase in plasma sodium = (sodium in NS plasma sodium) (TBW + 1) Calculation for DD: ( ) (25 +1) = = 1.19mEq/L

40 Hypervolemia, or fluid overload, is the medical condition where there is too much fluid in the blood. The opposite condition is hypovolemia, which is too little fluid volume in the blood. occurs when the body retains more water than it needs.
41 disruption in the salt/water balance in the body - short term illness, injury or surgery - Intravenous Fluids - Injury/Illness/Surgery - can also be due to long-term health conditions. - Kidney Disease - Liver Disease - Heart Disease

42 The symptoms of hypervolemia are consistent with excess water in the body Moist Cough Frothy Sputum Increased or Slowed Heart Rate Changes in Blood Pressure Swollen abdomen Shortness of Breath
43 symptoms of hypervolemia
44
45
46 Considerations When Assessing Electrolyte Imbalances Electrolyte content of nutrition products (i.e., parenteral nutrition, enteral nutrition) Addition or removal of medications (i.e., spironolactone, furosemide, insulin) IV fluids and piggybacks (i.e., normal saline with potassium) Underlying disease states (i.e., acute
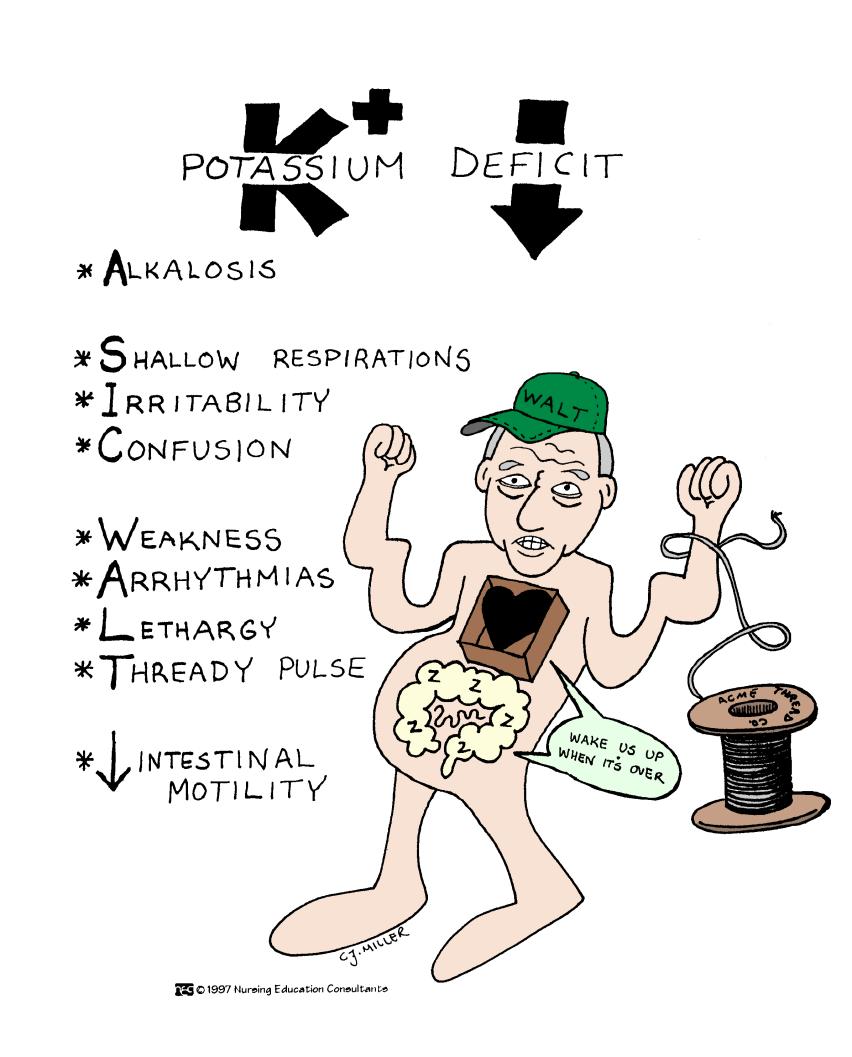
47 Pathophysiology Decrease in K+ causes decreased excitability of cells, therefore cells are less responsive to normal stimuli
48 Contributing factors: Diuretics Shift into cells Digitalis Water intoxication Corticosteroids Diarrhea Vomiting
49
50 Interventions Assess and identify those at risk Encourage potassium-rich foods K+ replacement (IV or PO) Monitor lab values D/c potassium-wasting diuretics Treat underlying cause
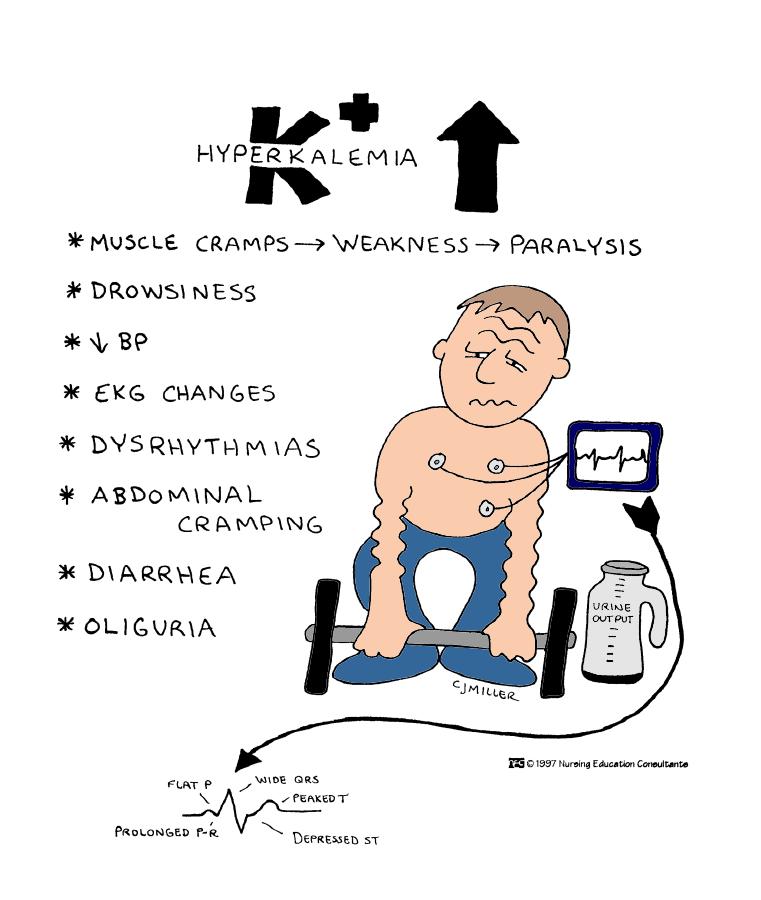
51 Pathophysiology An inc. in K+ causes increased excitability of cells.
52
53 Interventions/Treatment Restore Na levels to normal and prevent further decreases in Na. Drug Therapy (FVD) - IV therapy to restore both fluid and Na. If severe may see 2-3% saline. (FVE) Administer osmotic diuretic (Mannitol) to excrete the water rather than the sodium. Increase oral sodium intake and restrict oral fluid intake.
54 Contributing Factors Hyperaldosteronism Renal failure Corticosteroids Increase in oral Na intake Na containing IV fluids Decreased urine output with increased urine concentration
55 Contributing factors (cont d): Diarrhea Dehydration Fever Hyperventilation
56 Assessment findings: Neuro - Spontaneous muscle twitches. Irregular contractions. Skeletal muscle wkness. Diminished deep tendon reflexes Resp. Pulmonary edema CV Diminished CO. HR and BP depend vascular volume. on
57 GU Dec. urine output. Inc. specific gravity Skin Dry, flaky skin. Edema r/t fluid volume changes.
58 Interventions/Treatment Drug therapy (FVD).45% NSS. If caused by both Na and fluid loss, will administer NaCL. If inadequate renal excretion of sodium, will administer diuretics. Diet therapy Mild Ensure water intake
59 Contributing factors: Dec. oral intake Lactose intolerance Dec. Vitamin D intake End stage renal disease Diarrhea
60 Assessment findings: Neuro Irritable muscle twitches. Resp. Resp. failure, muscle tetany. CV Decreased HR., decreased BP, diminished peripheral pulses GI Increased motility. Increased BS. Diarrhea
61 Contributing factors: Excessive calcium intake Excessive vitamin D intake Renal failure Hyperparathyroidism Malignancy Hyperthyroidism
62 Assessment findings: Neuro Disorientation, lethargy, coma, profound muscle weakness Resp. Ineffective resp. movement CV Increased HR, Increased BP., Bounding peripheral pulses, Positive Homan s sign. Late Phase Bradycardia, Cardiac arrest GI Dec. motility. Dec. BS. Constipation GU Inc. urine output. Formation of renal calculi
63 Interventions/Treatment Eliminate calcium administration Drug Therapy Isotonic NaCL (Inc. the excretion of Ca) Diuretics Calcium reabsorption inhibitors (Phosphorus) Cardiac Monitoring Oral - Low-calcium diet IV - Increased infusion of NS
64 Contributing Factors: Malnutrition Starvation Hypercalcemia Renal failure Uncontrolled DM
65 Assessment findings Neuro Irritability, confusion CV Decreased contractility Resp. Shallow respirations Musculoskeletal destruction of muscle cells Hematologic Increased bleeding Decreased platelet aggregation
66 Interventions Treat underlying cause Oral replacement with vit. D IV phosphorus (Severe) Diet therapy Foods high in oral phosphate
67 Causes few direct problems with body function. Care is directed to hypocalcemia. Rarely occurs
68 Contributing factors: Malnutrition Starvation Diuretics Aminoglcoside antibiotics Hyperglycemia Insulin administration
69 Assessment findings: *Neuro - Hyperreflexia. Seizures *CV ECG changes. Dysrhythmias. HTN *Resp. Shallow resp. *GI Decreased motility. Anorexia. Nausea
70 Interventions: Eliminate contributing drugs IV MgSO4 Assess DTR s hourly with MgSO4 Diet Therapy
71 Contributing factors: Malnutrition Starvation Diuretics Aminoglcoside antibiotics Hyperglycemia Insulin administration
72 Assessment findings: *Neuro - Positive Trousseau s sign. Positive Chvostek s sign. Hyperreflexia. Seizures *CV ECG changes. Dysrhythmias. HTN *Resp. Shallow resp. *GI Dec. motility. Anorexia. Nausea
73 Electrolyte Normal Range Equations Corrected magnesium (Mg2+) 1.7 to 2.5 mg/dl Serum Mg2+ x 0.005(40 serum albumin mg/dl) Corrected calcium 8.0 to 11.0 mg/dl ([4 serum albumin (g/dl)] x 0.8) + measured calcium (mg/dl) Total body water (TBW) n/a (men) = 0.6 L/kg x weight in kg(women) = 0.5 L/kg x weight in kg Sodium deficit (meq) n/a TBW x (140 measured serum sodium concentration meq/l) Water deficit (in L) n/a TBW x ([serum sodium concentration meq/l/140] 1) Serum osmolality (sosm) 280 to 300 mosm/l (2 x serum sodium in meq/l) + (serum glucose in mg/dl/18) + (BUN in mg/dl/2.8) HCO3- deficit (mmol) n/a 0.5 x ([HCO3-] normal [HCO3- ] measured
74 Electrolyte Elevation Depletion Calcium Present in concentrations >11 mg/dl; lethargy, anorexia, nausea, vomiting, polyuria, confusion, coma Phosphorus Magnesium Sodium Potassium Anorexia, nausea, vomiting, hyperactive reflexes, tetany, tachycardia, muscle weakness Nausea, vomiting, diaphoresis altered mental status, coma, muscle weakness Increased thirst, fatigue, restlessness, muscle irritability, seizures, coma and death Muscle cramping, weakness, electrocardiographic changes, arrhythmia Hyperactive reflexes, muscle cramps numbness with tingling of fingers, tetany, convulsion Confusion, seizures, coma, chest pain, difficulty speaking or breathing, weakness, joint stiffness Weakness, lethargy, muscle cramps, mood changes, confusion, vomiting Nausea, vomiting, headache, muscle cramps, disorientation, weakness, lethargy, confusion, dizziness, seizure, coma and death Constipation, lethargy, weakness, leg cramps
75 Electrolyte Elevation Depletion Calcium Phosphorus Oral - Low-calcium diet IV - Increased infusion of NS Oral-.Low-phosphorus diet. Phosphate binders IV Assess the need for volume repletion Magnesium Oral Oral Oral- 1,000 to 1,500 mg/day IV(tetany present) 10 to 20 ml of 10% calcium gluconate over 4 hrs Oral- Increased dietary intake Oral supplementation (i.e., Na3PO4) IV Moderate) 0.32 to 0.64 mmol/kg (maximum, 30 mmol)na3po4 slowly over 6 hrs IV (Severe) 1 mmol/kg (maximum, 80 mmol) Na3PO4 slowly over 8 to 12 hrs

76 Substrate mmol/l Sodium 90 Potassium 20 Bicarbonate 30 Chloride 80 Glucose 111

77 Ingredients 1 L (33 oz) water 3 4 tsp table salt (sodium chloride) 1 tsp baking power (or 2 tsp baking soda) 4 tbsp sugar (sucrose) 1 2 tsp 20% potassium chloride* Sugar-free Kool-AidR or Crystal LightR to taste Directions Pour all ingredients into a blender or pitcher. Mix well.
78
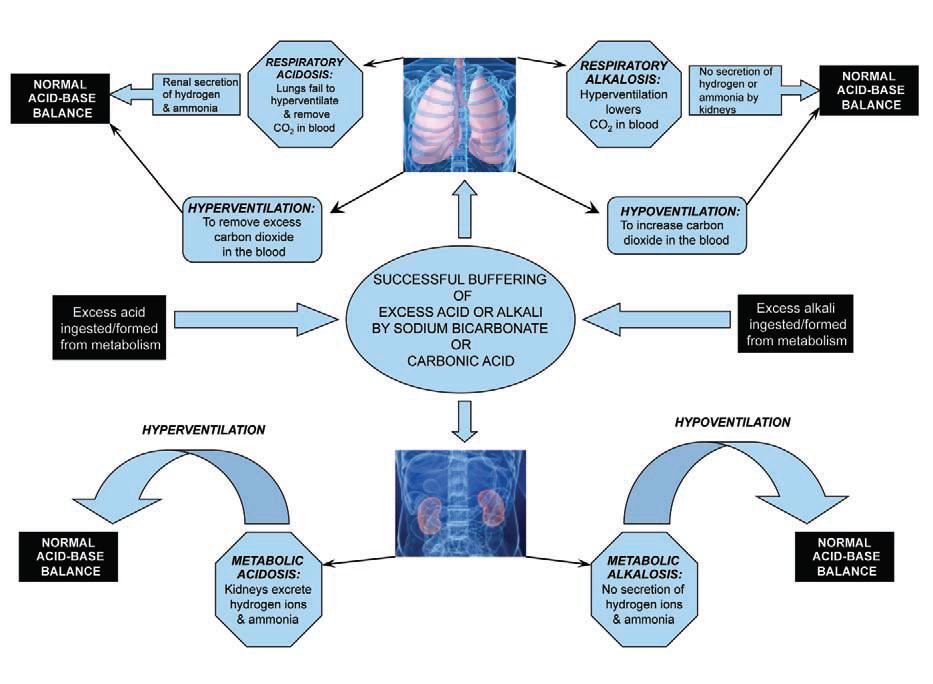
 Alkalosis: process that raises extracellular ph (elevation in HCO 3 or fall in pco")
79 Primary Compensating Acid-Base Disorder ph Change Reaction Metabolic acidosis HCO3 PCO2 Metabolic alkalosis HCO3 PCO2 Respiratory acidosis PCO2 HCO3 Respiratory alkalosis PCO2 HCO3 Acidosis: process that lowers the extracellular fluid ph (reduction in HCO 3 or elevation in pco 2 ) Alkalosis: process that raises extracellular ph (elevation in HCO 3 or fall in pco 2 )
80 Step 1: Analyze the ph Normal blood ph is 7.4±0.05, forming the range 7.35 to Step 2: Analyze the CO2 Normal Pco2 values are 35 to 45 mm Hg. Below 35 mm Hg is alkalotic; above 45 mm Hg is acidic. Step 3: Analyze the HCO3 A normal HCO3 is 22 to 26 meq/l. If the HCO3 is below 22 meq/l, the patient is acidotic. If the HCO3 is above 26 meq/l, the patient is alkalotic. Step 4: Match the CO2 or the HCO3 with the ph Matching either the Pco2 or the HCO3 with the ph can determine the acid-base disorder. For example, if the ph is acidotic and the CO2 is acidotic, the acid-base disturbance is being caused by the respiratory system and represents respiratory acidosis. If the ph is alkalotic and the HCO3 is alkalotic, the acid-base disturbance is being caused by the metabolic (or renal) system and represents metabolic alkalosis. Step 5: Does the CO2 or HCO3 go in the opposite direction of the ph? If the CO2 or HCO3 goes in the opposite direction of the ph, compensation is occurring. For example, when the ph is acidotic, the CO2 is acidotic, and the HCO3 is alkalotic, the CO2 matches the ph,making the primary acid-base disorder respiratory acidosis. The HCO3 being the opposite of the ph is evidence of compensation fromthemetabolic system. Step 6: Analyze the Po2 and the O2 saturation If the PaO2 and O2 saturation are below normal, there is evidence of hypoxemia.
81 Understanding the relationship between electrolytes and their movement within TBW during altered hydration status, electrolyte imbalances, or acid-base imbalance is key to developing a thorough nutrition plan care. With this knowledge, electrolyte abnormalities can be prevented or treated safely
82 A diet rich in highly alkaline fruits and vegetables helps reduce a marker of metabolic acidosis and preserve kidney function in patients with chronic kidney disease.... ACE inhibitors were given to patients to control blood pressure If your alkalosis is caused by a loss of chemicals such as chloride or potassium, you ll be prescribed medications or supplements to replace these chemicals. Some cases of alkalosis result from an electrolyte imbalance, which may be corrected by drinking plenty of fluids or drinks that contain electrolytes. If you have an advanced case of electrolyte imbalance, it will need to be treated in the hospital.
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Disclaimer. Chapter 3 Disorder of Water, Electrolyte and Acid-base Professor A. S. Alhomida. Disorder of Water and Electrolyte
 Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Principles of Fluid Balance
 Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Pediatric Dehydration and Oral Rehydration. May 16/17
 Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Acid Base Balance by: Susan Mberenga RN, BSN, MSN
 Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Fluid, electrolyte, and acid-base balance
 Fluid, electrolyte, and acid-base balance Chapter 50 Ra'eda Almashaqba 1 Fluid, electrolyte, and acid-base balance About 46% to 60%of the average adult's weight is water, which is vital to health and normal
Fluid, electrolyte, and acid-base balance Chapter 50 Ra'eda Almashaqba 1 Fluid, electrolyte, and acid-base balance About 46% to 60%of the average adult's weight is water, which is vital to health and normal
Fluids, Electrolytes and Hydration. Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University
 Fluids, Electrolytes and Hydration Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Discuss optimum hydration and effects of dehydration
Fluids, Electrolytes and Hydration Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Discuss optimum hydration and effects of dehydration
Acids, Bases, and Salts
 Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing Pediatrics Case Studies: Child Dehydration
 Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Symptoms of Tissue Disease
 Pathophysiology JP Advis DVM, Ph.D. Bartlett Hall, Animal Sciences, Cook, 932-9240, advis@aesop.rutgers.edu 02 Course website: rci.rutgers.edu/~advis Lectures, tests, grades, office hours, textbook, Material
Pathophysiology JP Advis DVM, Ph.D. Bartlett Hall, Animal Sciences, Cook, 932-9240, advis@aesop.rutgers.edu 02 Course website: rci.rutgers.edu/~advis Lectures, tests, grades, office hours, textbook, Material
Fluid and Electrolytes P A R T 4
 Fluid and Electrolytes P A R T 4 Mechanisms that control acid-base homeostasis Acids and bases continually enter and leave body Hydrogen ions also result from metabolic activity Acids Hydrogen ion donors
Fluid and Electrolytes P A R T 4 Mechanisms that control acid-base homeostasis Acids and bases continually enter and leave body Hydrogen ions also result from metabolic activity Acids Hydrogen ion donors
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Acid-Base Balance Workshop. Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli
 Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013 Cells form 4 basic tissue groups: 1. Epithelial 2. Connective
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013 Cells form 4 basic tissue groups: 1. Epithelial 2. Connective
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Liquid Consumption, Your Health, And Hyponatremia
 Liquid Consumption, Your Health, And Hyponatremia It is vital to remain hydrated at all times. The consumption of water is the most common way to do so. De-Hydrated Hydrated Over-Hydrated TWI: Total Water
Liquid Consumption, Your Health, And Hyponatremia It is vital to remain hydrated at all times. The consumption of water is the most common way to do so. De-Hydrated Hydrated Over-Hydrated TWI: Total Water
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Acid-Base Imbalance-2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD
 Yanal A. Shafagoj MD. PhD") AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
STAYING HYDRATED Serious effects of dehydration
 STAYING HYDRATED Serious effects of dehydration Belinda Kerr Marketing Director Ashley Piercy Scurry County Extension Agent What percentage of your body is water? 10% 25% 50% 75% 95% Functions of water
STAYING HYDRATED Serious effects of dehydration Belinda Kerr Marketing Director Ashley Piercy Scurry County Extension Agent What percentage of your body is water? 10% 25% 50% 75% 95% Functions of water
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
Body water content. Fluid compartments. Regulation of water output. Water balance and ECF osmolallty. Regulation of water intake
 Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Chapter 24 Water, Electrolyte and Acid-Base Balance
 Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
 Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + )
") Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
Dehydration and Oral Rehydration Solutions
 Health Professional Training Guide Up to 75% less sugar and 4x more electrolytes vs. the leading sports drinks Wide range of innovate formats and great tasting flavors Lasts for 30 days in the refrigerator
Health Professional Training Guide Up to 75% less sugar and 4x more electrolytes vs. the leading sports drinks Wide range of innovate formats and great tasting flavors Lasts for 30 days in the refrigerator
Part 1 The Cell and the Cellular Environment
 1 Chapter 3 Anatomy and Physiology Part 1 The Cell and the Cellular Environment 2 The Human Cell The is the fundamental unit of the human body. Cells contain all the necessary for life functions. 3 Cell
1 Chapter 3 Anatomy and Physiology Part 1 The Cell and the Cellular Environment 2 The Human Cell The is the fundamental unit of the human body. Cells contain all the necessary for life functions. 3 Cell
Salicylate (Aspirin) Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes
 Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes") Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Fluid & Electrolyte Therapy. Prof. Soliman Ali Hassan Prof. of Surgery Taibah university
 Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Acid-Base Balance Dr. Gary Mumaugh
 Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Unit 11. Objectives. Indications for IV Therapy. Intravenous Access Devices & Common IV Fluids. 3 categories. Maintenance Replacement Restoration
 Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
BIOL 221 Chapter 26 Fluids & Electrolytes. 35 slides
 BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender
 BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
BIOL 221 Chapter 26 Fluids & Electrolytes 35 slides 1 Body Water Content Total Body Water is the percentage of a person s weight that is water. TBW can easily vary due to: gender males have higher TBW
Exercise increases water loss
 Exercise increases water loss During normal breathing, water is added to inspired air to protect delicate respiratory cells from drying out. Increased breathing during exercise increase this loss Heat
Exercise increases water loss During normal breathing, water is added to inspired air to protect delicate respiratory cells from drying out. Increased breathing during exercise increase this loss Heat
Module 8: Practice Problems
 Module 8: Practice Problems 1. Convert a blood plasma level range of 5 to 20 µg/ml of tobramycin (Z = 467.52) to µmol/l. 5 µg/ml = 10.7 µmol/l 20 µg/ml = 42.8 µmol/l 2. A preparation contains in each milliliter,
Module 8: Practice Problems 1. Convert a blood plasma level range of 5 to 20 µg/ml of tobramycin (Z = 467.52) to µmol/l. 5 µg/ml = 10.7 µmol/l 20 µg/ml = 42.8 µmol/l 2. A preparation contains in each milliliter,
Assessment of the Patient with Endocrine Dysfunction. Objective. Endocrine. Endocrine Facts. Physical Assessment 10/3/2013
 Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017
 ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
CHAPTER. Nursing Care of Clients with Altered Fluid, Electrolyte, and Acid Base Balance MEDIALINK
 CHAPTER 10 Nursing Care of Clients with Altered Fluid, Electrolyte, and Acid Base Balance LEARNING OUTCOMES Describe the functions and regulatory mechanisms that maintain water and electrolyte balance
CHAPTER 10 Nursing Care of Clients with Altered Fluid, Electrolyte, and Acid Base Balance LEARNING OUTCOMES Describe the functions and regulatory mechanisms that maintain water and electrolyte balance
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
DISTRIBUTED SIMULATION PROJECT Management of IV Fluids and Electrolytes. Joy Hills 2013 RN, BSN, MSN (Cancer), SpecCertCR (Onc)
, SpecCertCR (Onc)") DISTRIBUTED SIMULATION PROJECT Management of IV Fluids and Electrolytes Joy Hills 2013 RN, BSN, MSN (Cancer), SpecCertCR (Onc) Professional responsibilities Obtaining and adhering to organisational guidelines.
DISTRIBUTED SIMULATION PROJECT Management of IV Fluids and Electrolytes Joy Hills 2013 RN, BSN, MSN (Cancer), SpecCertCR (Onc) Professional responsibilities Obtaining and adhering to organisational guidelines.
Fluid and Electrolytes P A R T 2
 Fluid and Electrolytes P A R T 2 Fluid Shifts Extracellular fluid distribution is dynamic Interstitial fluid formation is continuous Venous system Large veins (capacitance vessels) Small veins (capacitance
Fluid and Electrolytes P A R T 2 Fluid Shifts Extracellular fluid distribution is dynamic Interstitial fluid formation is continuous Venous system Large veins (capacitance vessels) Small veins (capacitance
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline
 BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD
 Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Dysnatremias: All About the Salt? Internal Medicine Resident Lecture 1/12/16 Steve Schinker, MD Water or salt? Dysnatremias In general, disorder of water balance, not sodium balance Volume status is tied
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Division 1 Introduction to Advanced Prehospital Care
 Division 1 Introduction to Advanced Prehospital Care Topics Fluids & fluid imbalances IV Therapy Hypoperfusion Shock Fluids and Fluid Imbalances 1 Water is the most abundant substance in the human body.
Division 1 Introduction to Advanced Prehospital Care Topics Fluids & fluid imbalances IV Therapy Hypoperfusion Shock Fluids and Fluid Imbalances 1 Water is the most abundant substance in the human body.
Module 8: Electrolyte Solutions
 PHARMACEUTICAL CALCULATIONS FALL 207 Contents General Vocab & Definitions... 2 Milliequivalent Calculations... 2 Millimole and Micromole Calculations... 5 Osmolarity... 6 Daily Water Requirement Calculations
PHARMACEUTICAL CALCULATIONS FALL 207 Contents General Vocab & Definitions... 2 Milliequivalent Calculations... 2 Millimole and Micromole Calculations... 5 Osmolarity... 6 Daily Water Requirement Calculations
Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are
 Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Water, Electrolytes, and Acid-Base Balance
 Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Instruct patient and caregivers: Need for constant monitoring Potential complications of drug therapy
 Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Fluid and Electrolytes: Parenteral
 Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Correction of hypervolaemic hypernatraemia by inducing negative Na + and K + balance in excess of negative water balance: a new quantitative approach
 Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
BUFFERING OF HYDROGEN LOAD
 BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available