Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia
|
|
|
- Helena Roberts
- 5 years ago
- Views:
Transcription
1 Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007
2 Topics Covered Today Intracranial Pressure Intracranial Compliance Cerebral Metabolism Cerebral Blood Flow Blood Brain Barrier Evoked Potentials

3 Neuroanesthesia at Upstate Everyone does a Neuro rotation Please read a textbook prior to neurorotation Neuroanesthesia is not complex; however small errors lead to big price to pay in terms of poor outcome
4 Intracranial Pressure The cranial vault is a rigid structure. It is consists o the brain (80%), blood (12%) and CSF (8%) Any increase in one component is offset by an equivalent decrease in another or else ICP increase Normal ICP is 0-10 mmhg
5
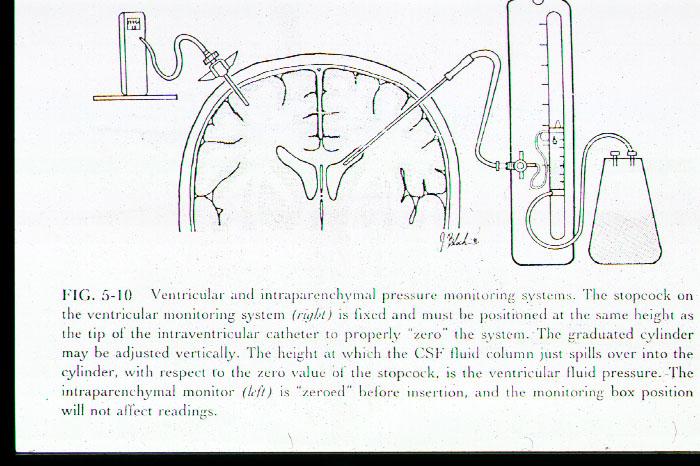
6 Use of ICP monitor Fiberoptic ICP monitor Standard ICP monitor hooked to our HP monitors Ask for help on how to use the equipment Sometimes the ICP is to be left open Overdrainage as well as underdrainage has been a problem at SUNY Do not inject anything into the catherter Please aspirate SLOW if asked by surgeons
7 Intracranial Compliance As intracranial pressure increases, the body compensates: Shift CSF to spinal canal Increase CSF absorption Decrease CSF production Decrease Ce vv capacitance Can Compliance be measured?? Saline Test 1:4 ratio
8 Herniation Sites Sustained increases in ICP can lead to herniation and cerebral ischemia/infarction Cingulate gyrus Uncinate gyrus Cerebellar tonsils thru foramen magnum Any skull defect as in trauma
9 Topics Covered Today Intracranial Pressure Intracranial Compliance Cerebral Metabolism < Cerebral Blood Flow Blood Brain Barrier Evoked Potentials
10 Cerebral Metabolism CMRO 2 parallels activity of brain cells CMRO 2 is greatest in the grey matter of CCx CMRO 2 is 3-5 ml/100gm/minute in adults= 50ml/min Brain uses 20% of total body oxygen consumption, most of it for ATP production
11
12 Cerebral Metabolism 90% of brain metabolism is aerobic O2 reserves are low, consumption is high Narrow margin of safety with hypoxia Primary fuel is glucose and oxygen Hypoglycemia is not well tolerated Hyperglycemia leads to cellular acidosis during ischemia
13 IV Anesthetic and CMRO 2 Anesthetic /PHYSILO EFFECT CMRO2 CeBF CeBV I C P Barbitrates* DDDD DDD DD DDD Opiods** N N N N, I Etomidate***DDDD DD DD DD Benzodiazepin DD D D D Propofol DDDD DDDD DD DD Ketamine I I I I I I I I I Vasopressors Vasodilators 0 I dose dep. I dose dep. I dose dep. NMB N N N N, I Lidocaine D D D D D=Decrease I= Increase N=No change * These are beneficial; Antiseizure, role in preventing focal not Global ** All change if hypoventilate ***Causes myoclonus not seizures; It can cause seizures in patients w * * * * except trimethapan only secondary effects
14 Volatile Anesthetic and Cerebral Physiology Isoflurane* D In neocortex CMRO 2 CeBF CeBV ICP CO2 responsivenes s I I I ~20% at 1 MAC Maintain Enflurane D or I Seizures** II II I Maintain Halothane D III III I 200% at 1 MAC Maintain N 2 O I I I I Maintain * Sevoflurane and Desflurane similar ** 2 MAC and hypocapnia
15 Topics Covered Today Intracranial Pressure Intracranial Compliance Cerebral Metabolism Cerebral Blood Flow: A sometimes confusing topic Blood Brain Barrier Evoked Potentials
16 CeBF and CMRO 2 CeBF is proportional to CMRO2 CeBF: Grey matter versus white matter Total CeBF is about 20% of CO =750 ml/min EEG is used clinically to judge adequate CeBF EEG Slowing in a normal brain > EEG slowing > isoelectric EEG <10 --> irreversible damage
17 CeBF and Children Newborn: lower than adults Infants and above CeBF: higher than adults Big Children (adults)= Average BF is 1 liter/min; Grey matter is 1.2l/min and white matter is 0.3l/min
18 Spinal Cord Blood Flow Grey matter: 60 ml/100gm/min Cerebral cortex --> 80ml/100 gm/min White matter ml/100gm/min
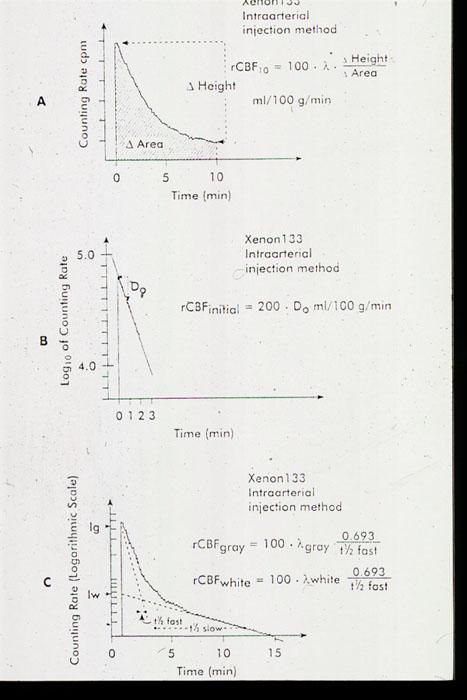
19 Measuring CeBF Inhale RA inert gases: N 2 0, Krypton and Xenon Intraaeterial injection of inert gas: 133 Xe PET Scanning (Positive emission tomography) Using radionucleotide that emits particles called positrons (11C, 15O, 13N, 18F) Injection or inhalation Need cyclotron NMR: Nuclear Magnetic Resonance; future promise
20
21 Regulation of CeBF Cerebral Perfusion Pressure Autoregulation Myogenic, metabolic (CMRO2) Extrinsic Mechanisms PaO 2, PaCO 2, Temp, and viscosity
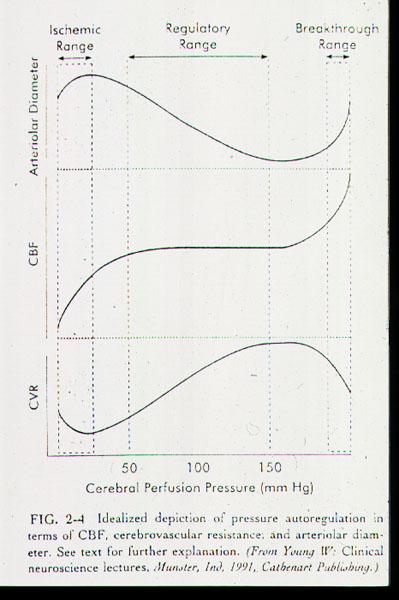
22 Cerebral Perfusion Pressure CeBF remains constant CeBF remains constant between mm Hg despite changes in CePP (CePP= MAP- ICP or CVP) Beyond these blood flow is pressure dependant Normal ICP= 10 mmhg CPP<50 mm Hg EEG slowing (w/ no anesthesia) CPP mm Hg EEG flat (w/ no anesthesia)
23 Autoregulation Mechanism for autoregulation: thought to be myogenic and metabolic Myogenic involves the intrinsic property of Ce vessels to control blood flow Property of cerebral blood vessels to keep blood flow constant between a MAP of mm Hg Beyond these, the blood flow becomes pressure dependant
24
25 Hypertension and CeBF/ICP Untreated HTN--> autoregulatory curve shifted to right If MAP>150--> Autoregulatory breakthrough As MAP increase, CeBF goes up as it is now pressure dependant BBB is disrupted and cerebral edema can ensue
26 Autoregulation Loss Hypoxia Hypercapnia Ischemia Trauma CVA
27 Extrinsic Mechanisms for control of CeBF: Blood Gas Tensions PaCO 2 : Direct proportion between CeBF changes 1-2 ml/100gm/1mm change in PaCO 2 Marked Hyperventilation: Cerebral Ischemia Marked Hypoventilation: pressure dependant CeBF Limitation of hyperventilation: after 6 hours, hyperventilation will not be effective
28 Extrinsic Mechanisms for control of CeBF: PaO2 PaO 2 < 50 causes a rapid increase in CeBF Hyperoxia has little effect on CeBF Spinal cord reacts the same way as the cortex
29
30 Extrinsic Mechanisms for control of CeBF:Temperature For every one deg decrease in body temp, CMRO 2 decreases 5%--> leads to fall in CeBF Brain temp of 20deg C--> isoelectric EEG
31 Extrinsic Mechanisms for control of CeBF:Viscosity Polycythemia is detrimental to CeBF and can cause a CVA HCTs less than 30 improve CeBF but at the expense of decrease O2 carrying capacity Studies suggest the optimal HCT to be between 30 and 40
32 Luxury/Steal Perfusion CMRO 2 parallels activity of brain cells; volatile agents uncouple metabolism from CeBF needs. This is then Luxury Perfusion Cerebral Steal: Blood is shunted from an area of that is ischemic to normal area. Setting: patient with CeVascular disease getting isoflurane dilates vasculature. Ischemic area gets blood shunted away from it
33 IV Anesthetic and CeBF Anesthetic /PHYSILO EFFECT CMRO2 CeBF CeBV I C P Barbitrates* DDDD DDD DD DDD Opiods** N N N N, I Etomidate***DDDD DD DD DD Benzodiazepin DD D D D Propofol DDDD DDDD DD DD Ketamine I I I I I I I I I Vasopressors Vasodilators 0 I dose dep. I dose dep. I dose dep. NMB N N N N, I Lidocaine D D D D D=Decrease I= Increase N=No change * These are beneficial; Antiseizure, role in preventing focal not Global ** All change if hypoventilate ***Causes myoclonus not seizures; It can cause seizures in patients w * * * * except trimethapan only secondary effects
34 Volatile Anesthetic and Cerebral Physiology Isoflurane* D In neocortex CMRO 2 CeBF CeBV ICP CO2 responsivenes s I I I ~20% at 1 MAC Maintain Enflurane D or I Seizures** II II I Maintain Halothane D III III I 200% at 1 MAC Maintain N 2 O I I I I Maintain * Sevoflurane and Desflurane similar ** 2 MAC and hypocapnia
 Extrinsic Mechanisms PaO 2, PaCO 2, Temp, and")
35 Review Regulation of CeBF Cerebral Perfusion Pressure Autoregulation Myogenic, metabolic (CMRO2) Extrinsic Mechanisms PaO 2, PaCO 2, Temp, and viscosity
36 Topics Covered Today Intracranial Pressure Intracranial Compliance Cerebral Metabolism Cerebral Blood Flow Blood Brain Barrier Evoked Potentials
37 Blood Brain Barrier What is the BBB? Rules governing transport across BBB Movement of water? Factors Disrupting the BBB? Vascular Endothelium that is fused Charge, lipid solubility, protein binding Bulk Flow; Role of Na + HTN, Tumor, Trauma, CVA, Ix, CO 2 and O 2
38 Topics Covered Today Intracranial Pressure Intracranial Compliance Cerebral Metabolism Cerebral Blood Flow Blood Brain Barrier Evoked Potentials
39 Last Topic: Evoked Potential
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia
 Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
CEREBRAL PHYSIOLOGY CEREBRAL PHYSIOLOGY REGULATION OF CBF REGULATION OF CBF REGULATION OF CBF. Cerebral Blood Flow (CBF)
") NEUROANESTHESIA: THE FAST-TRACK APPROACH Bruce Weiner, CRNA, MS Moffitt Cancer Center Tampa, FL LEARNER OUTCOMES Discuss the interaction between intracranial pathophysiology, cerebral perfusion and general
NEUROANESTHESIA: THE FAST-TRACK APPROACH Bruce Weiner, CRNA, MS Moffitt Cancer Center Tampa, FL LEARNER OUTCOMES Discuss the interaction between intracranial pathophysiology, cerebral perfusion and general
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED
 ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation
 Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Cerebral blood volume
 Alifia Tameem MBBS MD FRCA Hari Krovvidi MD FRCA Matrix reference 1A01, 1A02, 3F00 Key points The brain is enclosed in a rigid box with a fixed volume and an increase in the volume of any of its constituents
Alifia Tameem MBBS MD FRCA Hari Krovvidi MD FRCA Matrix reference 1A01, 1A02, 3F00 Key points The brain is enclosed in a rigid box with a fixed volume and an increase in the volume of any of its constituents
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
Pharmacokinetics. Inhalational Agents. Uptake and Distribution
 Pharmacokinetics Inhalational Agents The pharmacokinetics of inhalational agents is divided into four phases Absorption Distribution (to the CNS Metabolism (minimal Excretion (minimal The ultimate goal
Pharmacokinetics Inhalational Agents The pharmacokinetics of inhalational agents is divided into four phases Absorption Distribution (to the CNS Metabolism (minimal Excretion (minimal The ultimate goal
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL BLOOD FLOW AND METABOLISM
 Supported by: HURO/0901/069/2.3.1 HU-RO-DOCS CEREBRAL BLOOD FLOW AND METABOLISM Part 11. Cerebral blood flow Supplies cerebral metabolism demanded by neuronal function Is required for the production and
Supported by: HURO/0901/069/2.3.1 HU-RO-DOCS CEREBRAL BLOOD FLOW AND METABOLISM Part 11. Cerebral blood flow Supplies cerebral metabolism demanded by neuronal function Is required for the production and
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency
 Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Physiology and Monitoring of Intravascular Volume Status in the Neurosurgical Patient
 Physiology and Monitoring of Intravascular Volume Status in the Neurosurgical Patient David J. Stone MD I. Introduction and General Issues The focal point in the care of neurosurgical patients is the control
Physiology and Monitoring of Intravascular Volume Status in the Neurosurgical Patient David J. Stone MD I. Introduction and General Issues The focal point in the care of neurosurgical patients is the control
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Drug Choices and Outcomes in Neuroanesthesia
 Robert Breeze, MD Daniel Janik, MD Benjamin Scott, MD NEUROANESTHESIA PANEL CRASH 2015 Your Anesthetic? Balanced technique opiate/volatile? Nitrous/narcotic technique? TIVA propofol/opiate Does choice
Robert Breeze, MD Daniel Janik, MD Benjamin Scott, MD NEUROANESTHESIA PANEL CRASH 2015 Your Anesthetic? Balanced technique opiate/volatile? Nitrous/narcotic technique? TIVA propofol/opiate Does choice
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Proceedings of the Southern European Veterinary Conference - SEVC -
 www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 29-Oct. 2, 2011, Barcelona, Spain Next SEVC Conference: Oct. 18-21, 2012 - Barcelona, Spain Reprinted in the IVIS website
www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 29-Oct. 2, 2011, Barcelona, Spain Next SEVC Conference: Oct. 18-21, 2012 - Barcelona, Spain Reprinted in the IVIS website
Volatile Anaesthetic Agents (Basic Principles)
") Volatile Anaesthetic Agents (Basic Principles) KSS School of Anaesthesia Basic Science Course South Coast Training Group Dr S M Walton Consultant Anaesthetist Eastbourne What do you need to know about
Volatile Anaesthetic Agents (Basic Principles) KSS School of Anaesthesia Basic Science Course South Coast Training Group Dr S M Walton Consultant Anaesthetist Eastbourne What do you need to know about
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
Major Aortic Reconstruction; Cerebral protection and Monitoring
 Major Aortic Reconstruction; Cerebral protection and Monitoring N AT H A E N W E I T Z E L M D A S S O C I AT E P R O F E S S O R O F A N E S T H E S I O LO G Y U N I V E R S I T Y O F C O LO R A D O S
Major Aortic Reconstruction; Cerebral protection and Monitoring N AT H A E N W E I T Z E L M D A S S O C I AT E P R O F E S S O R O F A N E S T H E S I O LO G Y U N I V E R S I T Y O F C O LO R A D O S
CEREBRAL METABOLISM CEREBRAL BLOOD FLOW INTRACRANIAL PRESSURE.
 CEREBRAL METABOLISM CEREBRAL BLOOD FLOW INTRACRANIAL PRESSURE www.fisiokinesiterapia.biz CEREBRAL METABOLISM THE BRAIN AS A CONVERTER OF ENERGY It converts substrates (mainly glucose and oxygen) into the
CEREBRAL METABOLISM CEREBRAL BLOOD FLOW INTRACRANIAL PRESSURE www.fisiokinesiterapia.biz CEREBRAL METABOLISM THE BRAIN AS A CONVERTER OF ENERGY It converts substrates (mainly glucose and oxygen) into the
BASIC CONCEPT ON PEDIATRIC NEUROANESTHESIA INASNACC
 BASIC CONCEPT ON PEDIATRIC NEUROANESTHESIA INASNACC Newborn period is the first 24 hours of life. Neonatal period is the first 30 days of life and includes the newborn period. Infant is less than 1 year
BASIC CONCEPT ON PEDIATRIC NEUROANESTHESIA INASNACC Newborn period is the first 24 hours of life. Neonatal period is the first 30 days of life and includes the newborn period. Infant is less than 1 year
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
INHALATION AGENTS 2013/05/28 1
 INHALATION AGENTS 2013/05/28 1 2013/05/28 Isn t it romantic? 2 Administration 3 Physics Critical temperature Vapour vs. Gas Vapour pressure Blood Gas Partition Coefficient BGPC MAC 2013/05/28 4 Critical
INHALATION AGENTS 2013/05/28 1 2013/05/28 Isn t it romantic? 2 Administration 3 Physics Critical temperature Vapour vs. Gas Vapour pressure Blood Gas Partition Coefficient BGPC MAC 2013/05/28 4 Critical
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
INHALATIONAL ANESTHETICS Nitrous Oxide (N 2 O)
") INHALATIONAL ANESTHETICS Nitrous Oxide (N 2 O) -low molecular weight, clear, odorless, inert, inorganic gas -non-flammable but does support combustion -gas at room temperature, kept as liquid under pressure
INHALATIONAL ANESTHETICS Nitrous Oxide (N 2 O) -low molecular weight, clear, odorless, inert, inorganic gas -non-flammable but does support combustion -gas at room temperature, kept as liquid under pressure
Inhalational Anesthesia. Munir Gharaibeh, MD, PhD, MHPE School of Medicine The University of Jordan February, 2018
 Inhalational Anesthesia School of Medicine The University of Jordan February, 2018 mgharaib@ju.edu.jo Inhalational Anesthesia n Gases or volatile liquids n Administration and Elimination is by the lungs
Inhalational Anesthesia School of Medicine The University of Jordan February, 2018 mgharaib@ju.edu.jo Inhalational Anesthesia n Gases or volatile liquids n Administration and Elimination is by the lungs
Pharmacology of Inhaled Anesthetics
 Pharmacology of Inhaled Anesthetics Beverly K. Philip, M.D. Professor of Anaesthesia Harvard Medical School Founding Director, Day Surgery Unit Brigham and Women s Hospital Boston, USA Beverly K. Philip,
Pharmacology of Inhaled Anesthetics Beverly K. Philip, M.D. Professor of Anaesthesia Harvard Medical School Founding Director, Day Surgery Unit Brigham and Women s Hospital Boston, USA Beverly K. Philip,
Carbon Dioxide Transport. Carbon Dioxide. Carbon Dioxide Transport. Carbon Dioxide Transport - Plasma. Hydrolysis of Water
 Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
ADVANCES IN ANESTHESIA
 Advances in Anesthesia 30 (2012) 97 129 ADVANCES IN ANESTHESIA Modern and Evolving Understanding of Cerebral Perfusion and Autoregulation Nathaniel H. Greene, MD a, Lorri A. Lee, MD a,b, * a Department
Advances in Anesthesia 30 (2012) 97 129 ADVANCES IN ANESTHESIA Modern and Evolving Understanding of Cerebral Perfusion and Autoregulation Nathaniel H. Greene, MD a, Lorri A. Lee, MD a,b, * a Department
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neuroprotection in neuroanesthesia
 Neuroprotection in neuroanesthesia Federico Bilotta, MD, PhD Sapienza University of Rome, Rome, Italy Topical problems and innovational technologies in anesthesiology and emergency medicine 31 March, 2018
Neuroprotection in neuroanesthesia Federico Bilotta, MD, PhD Sapienza University of Rome, Rome, Italy Topical problems and innovational technologies in anesthesiology and emergency medicine 31 March, 2018
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
ANESTHESIA FOR SUPRATENTORIAL TUMOR
 ANESTHESIA FOR SUPRATENTORIAL TUMOR Diana Christine Lalenoh, MD, PhD, Neuroanesthesiologist consultant, Obstetric Anesthesia consultant Department of Anesthesiology & Intensive Care, Medical Faculty of
ANESTHESIA FOR SUPRATENTORIAL TUMOR Diana Christine Lalenoh, MD, PhD, Neuroanesthesiologist consultant, Obstetric Anesthesia consultant Department of Anesthesiology & Intensive Care, Medical Faculty of
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
BOLD signal dependence on blood flow and metabolism. Outline
 BOLD signal dependence on blood flow and metabolism R. Hoge, MGH NMR Center Outline physiological events accompanying neuronal activation factors affecting BOLD signal sensitivity BOLD response dynamics
BOLD signal dependence on blood flow and metabolism R. Hoge, MGH NMR Center Outline physiological events accompanying neuronal activation factors affecting BOLD signal sensitivity BOLD response dynamics
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Nuclear neurology. Zámbó Katalin Department of Nuclear Medicine
 Nuclear neurology Zámbó Katalin Department of Nuclear Medicine To refresh your memory Brain has a high rate of oxidative metabolism. It has no reserves either of oxygen or of glucose and has a very limited
Nuclear neurology Zámbó Katalin Department of Nuclear Medicine To refresh your memory Brain has a high rate of oxidative metabolism. It has no reserves either of oxygen or of glucose and has a very limited
SCINTIGRAPHY OF THE CENTRAL NERVOUS SYSTEM Part 1: Introduction and BBB studies
 SCINTIGRAPHY OF THE CENTRAL NERVOUS SYSTEM Part 1: Introduction and BBB studies George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine October 2009 FIRST
SCINTIGRAPHY OF THE CENTRAL NERVOUS SYSTEM Part 1: Introduction and BBB studies George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine October 2009 FIRST
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Current bedside monitors of brain blood flow and oxygen delivery
 24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
May 2013 Anesthetics SLOs Page 1 of 5
 May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Neuro Quiz 25 - Monitoring
 Neuro Quiz 25 - Monitoring This quiz is being published on behalf of the Education Committee of the SNACC Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey, PA Quiz Team Shobana
Neuro Quiz 25 - Monitoring This quiz is being published on behalf of the Education Committee of the SNACC Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey, PA Quiz Team Shobana
General anesthesia. No single drug capable of achieving these effects both safely and effectively.
 General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
Introduction to the Course and the Techniques. Jeffry R. Alger, PhD Ahmanson-Lovelace Brain Mapping Center Department of Neurology
 Introduction to the Course and the Techniques Jeffry R. Alger, PhD Ahmanson-Lovelace Brain Mapping Center Department of Neurology (jralger@ucla.edu) CTSI Neuroimaging April 2014 Rationale for the Course
Introduction to the Course and the Techniques Jeffry R. Alger, PhD Ahmanson-Lovelace Brain Mapping Center Department of Neurology (jralger@ucla.edu) CTSI Neuroimaging April 2014 Rationale for the Course
Intraoperative neurophysiological monitoring for the anaesthetist
 Intraoperative neurophysiological monitoring for the anaesthetist Part 2: A review of anaesthesia and its implications for intraoperative neurophysiological monitoring Abstract Van Der Walt JJN, MBChB,
Intraoperative neurophysiological monitoring for the anaesthetist Part 2: A review of anaesthesia and its implications for intraoperative neurophysiological monitoring Abstract Van Der Walt JJN, MBChB,
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
What is MH? Malignant Hyperthermia (MH)! Malignant Hyperthermia (MH) Malignant Hyperthermia (MH) ! The underlying physical mechanismintracellular
! Malignant Hyperthermia (MH) Malignant Hyperthermia (MH) ! The underlying physical mechanismintracellular") 10/2/13 What is MH? Libby Morse BSN RN CPAN An inherited disorder of skeletal muscle triggered in susceptible humans in most instances by inhalation agents and/ or succinylcholine, resulting in hypermetabolism,
10/2/13 What is MH? Libby Morse BSN RN CPAN An inherited disorder of skeletal muscle triggered in susceptible humans in most instances by inhalation agents and/ or succinylcholine, resulting in hypermetabolism,
This quiz is being published on behalf of the Education Committee of the SNACC.
 Shobana Rajan, M.D. Attending Anesthesiologist, Albany Medical Center, Albany, NY Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester, MA.
Shobana Rajan, M.D. Attending Anesthesiologist, Albany Medical Center, Albany, NY Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester, MA.
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Non-Invasive Techniques
 Non-Invasive Techniques Key: Does not hurt the organism Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides or view the video presentation
Non-Invasive Techniques Key: Does not hurt the organism Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides or view the video presentation
Non-Invasive Techniques
 Many Procedures Non-Invasive Techniques Key: Does not hurt the organism Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides or view the
Many Procedures Non-Invasive Techniques Key: Does not hurt the organism Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides or view the
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Emergency Management of the Head
 Emergency Management of the Head Trauma Patient Adam Schneider, DVM Neurology and Neurosurgery Blue Pearl 9500 Marketplace Rd Fort Myers Head trauma Common cause of morbidity and mortality 25% of blunt
Emergency Management of the Head Trauma Patient Adam Schneider, DVM Neurology and Neurosurgery Blue Pearl 9500 Marketplace Rd Fort Myers Head trauma Common cause of morbidity and mortality 25% of blunt
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Intracranial volume-pressure relationships during
 Journial of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 115-1111 Intracranial volume-pressure relationships during experimental brain compression in primates 3. Effect of mannitol and hyperventilation
Journial of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 115-1111 Intracranial volume-pressure relationships during experimental brain compression in primates 3. Effect of mannitol and hyperventilation
Brain Tumors. What is a brain tumor?
 Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
The Nervous System PART C. PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Nervous System 7 PART C Protection of the Central Nervous System Scalp and skin Skull and vertebral
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Nervous System 7 PART C Protection of the Central Nervous System Scalp and skin Skull and vertebral
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
ISPUB.COM. Review Of Currently Used Inhalation Anesthetics: Part II. O Wenker SIDE EFFECTS OF INHALED ANESTHETICS CARDIOVASCULAR SYSTEM
 ISPUB.COM The Internet Journal of Anesthesiology Volume 3 Number 3 O Wenker Citation O Wenker.. The Internet Journal of Anesthesiology. 1998 Volume 3 Number 3. Abstract SIDE EFFECTS OF INHALED ANESTHETICS
ISPUB.COM The Internet Journal of Anesthesiology Volume 3 Number 3 O Wenker Citation O Wenker.. The Internet Journal of Anesthesiology. 1998 Volume 3 Number 3. Abstract SIDE EFFECTS OF INHALED ANESTHETICS
Malignant Hyperthermia: What the ICU Needs to Know
 Malignant Hyperthermia: What the ICU Needs to Know Objectives 1. Compare the pathophysiology of malignant hyperthermia (MH) with presenting signs/symptoms in a critical care environment. 2. Identify critical,
Malignant Hyperthermia: What the ICU Needs to Know Objectives 1. Compare the pathophysiology of malignant hyperthermia (MH) with presenting signs/symptoms in a critical care environment. 2. Identify critical,
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission