Current issues in Barrett s oesophagus and the oesophago-gastric junction
|
|
|
- Abraham Henderson
- 5 years ago
- Views:
Transcription
1 Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May
2 The changing role of the pathologist in the management of Barrett s oesophagus Suzanne A Hopcroft & Neil A Shepherd Histopathology 2014; 65: Published October 2014
3 Nomenclature and definitions of Barrett s oesophagus and OGJ diseases What do we call it? USA: Barrett s esophagus (BE) Europe: Columnar epithelium-lined lower oesophagus (CELLO) UK: not BO but columnar-lined oesophagus (CLO) Definitions: Traditional/classical CLO (CLO) arbitrary 3 cms (sometimes 2) Short segment CLO (SSCLO) from short tongues to < 3 cms Ultrashort segment CLO (USSCLO) IM in the cardia, cardia IM (CIM)
4 Prevalence of reflux and CLO in the West Adult heartburn 22-39% GORD (reflux disease) 10-12% CLO at endoscopy 0.5-2% SSCLO at endoscopy 8-17% USSCLO at endoscopy 15-32% CLO at autopsy 5%

5
6 The OGJ and the gastric cardia controversy personified
7 The gastric cardia: does it exist? studies of perinatal and paediatric subjects no history of GORD/Barrett's oesophagus these papers showed that the cardia is a normal structure (although it is small) Kilgore et al, Am J Gastroenterol 2000 de Hertogh et al, Gut 2003
8 The gastric cardia - for definite it exists as a normal structure it's very short (mm, not cm) often a transitional mucosa with admixture of cardiac and fundic glands is it gastric or is it oesophageal?
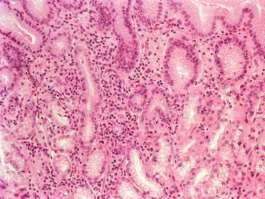
9 What is carditis? acute inflammatory cells chronic inflammatory cells regenerative epithelial changes Definition: An expansion of the lamina propria by chronic inflammatory cells with or without acute inflammatory cells and regenerative epithelial changes

10
11 Carditis: roles of GORD & H pylori GORD HP Öberg + - Genta N/A + Goldblum - + Wang - + Hackelsberger N/A +

12 Time to speculate.
13 The gastric cardia and carditis definite and less definite the cardia exists as a normal structure it's very short (mm, not cm) often a transitional mucosa with admixture of cardiac and fundic glands carditis in the upper stomach is strongly related to HP infection the cardia is a gastric anatomic structure but may also be metaplastic in the lower oesophagus here it is usually inflamed (96% in Oberg s study) GORD and HP infection may both have a role in its genesis and that of carditis here

14 IM at the cardia/cardia IM/ultrashort segment Barrett s oesophagus Do not let them biopsy the endoscopically normal OGJ. In 16-32% of cases, you will show cardia IM and we have no idea of its significance or management RCPath guidelines, 2002 Riddell & Odze, 2009

15 Cancers close to or at the GOJ
16 Cardia IM/ IM at the cardia/cim this is a gastric disease: IM in the cardia it is not Barrett s oesophagus (although pathologists will say it is if clinicians/endoscopists don t give them the right information) the evidence is now weighted towards the thesis that this is primarily related to gastric HP infection it remains uncertain how important GORD is in its genesis it is much commoner than classical and short segment Barrett s oesophagus: 16-30% of an endoscopic population in the West it is by definition a pathological diagnosis: the demonstration of IM (with or without inflammation) in cardiac mucosa below a normally positioned SCJ/OGJ
17 Cardia IM/ IM at the cardia/cim we have no idea, currently, of its significance and neoplastic potential it is now a national and international recommendation that this disease is NOT diagnosed outside the research setting please don t let them biopsy the endoscopically normal OGJ (unless for research)..
18 The changing role of pathology in the management of Barrett s oesophagus diagnosis the effects of treatment the management of neoplasia
19 The changing role of pathology in the management of Barrett s oesophagus diagnosis: a short history the effects of treatment the management of neoplasia

20 Norman Pasty Barrett Consultant Surgeon St Thomas Hospital London, UK Barrett NR. Chronic peptic ulcer of the oesophagus and oesophagitis. Br J Surg 1950; 38:

21 1950 congenitally short oesophagus 1970s true glandular metaplasia due to reflux of gastric contents: ACID and OTHER PEPTIC CONTENTS 1990s reflux of duodenal contents: BILE and ALKALI

22 recognition of intestinal metaplasia in CLO Bosher LH, Taylor FH; 1951 first description of association of Barrett s oesophagus with adenocarcinoma Morson BC, Belcher JR; 1952



23 recognition of the three phenotypes of Barrett s oesophagus cardiac, fundic & intestinal Paull et al, 1976
24 The history of the goblet cell story.
25 Some time in the late 1980s intestinal metaplasia/goblet cells became enshrined in the definition of CLO and its/their demonstration was required for the diagnosis?!? introduced by US physicians who did not understand the subtleties of pathological assessment, sampling and correlation with endoscopy Spechler SJ, Goyal RK. Barrett's esophagus. New Engl J Med 1986; 315:
26 The goblet cell question should Barrett s be defined/diagnosed by showing intestinal metaplasia/goblet cells on biopsy?
27 British Society of Gastroenterology guidelines, 2005 although CLO may be diagnosed with reasonable accuracy either by endoscopic appearance, histological corroboration of endoscopically visible columnarisation results in highest diagnostic accuracy. no requirement for the demonstration of goblet cells/im Watson, Heading & Shepherd, 2005

28 British Society of Gastroenterology guidelines, 2005 why no requirement for the demonstration of goblet cells/im? all long segment CLO shows intestinalisation somewhere a lack of IM in biopsies merely represents a sampling issue Watson, Heading & Shepherd, 2005

29 Flejou, 2008
30 You don t need to see IM to get cancer Takubo K, Aida J, Naomoto Y,.. & Vieth M. Cardiac rather than intestinal-type background in endoscopic resection specimens of minute Barrett adenocarcinoma. Hum Pathol 2009; 40: Aida J, Vieth M, Shepherd NA, et al. Is carcinoma in columnar-lined esophagus always located adjacent to intestinal metaplasia? Am J Surg Pathol 2015: 39;

31 You don t need to see IM to get cancer
32 The influence of the number of biopsies on the demonstration of IM in classical CLO % with IM vs number of biopsies taken Harrison et al, 2007
33 The influence of the number of biopsies on the demonstration of IM in classical CLO >9 No of Biopsies UK Barrett s Oesophagus Registry (UKBOR) study diagnostic biopsies of 200 patients Mandalia & Shepherd, 2016 (in Lowes, Somarathna & Shepherd, 2017)
34 But... goblet cells/im still required by the AGA for the definition/ diagnosis of CLO (in North America) change in the distal esophageal epithelium of any length that can be recognized as columnar-type mucosa at endoscopy and confirmed to have intestinal metaplasia by biopsy of the tubular esophagus Wang KK, Sampliner RE. Updated guidelines 2008 for Barrett's esophagus. Am J Gastronterol 2008; 103: AGA Position Statement, 2011 Spechler, 2012
35 Then... Riddell RH, Odze RD. Definition of Barrett's esophagus: time for a rethink - is intestinal metaplasia dead? Am J Gastroenterol 2009; 104:
36 goblet cells are uncommon in pediatric patients with BE small percentage of adults have CLO without goblet cells the chances of detecting goblet cells proportional to the length of CLO sampling error common interpretation & differentiation of goblet cells vs. pseudogoblet cells difficult goblet cells have been shown to wax and wane over the natural history of BE background non-goblet epithelium in BE is biologically intestinalised background non-goblet epithelium in BE shows molecular abnormalities similar to the goblet cell-containing epithelium well-defined risk of neoplasia in patients with esophageal columnar metaplasia without goblet cells a diagnosis of BE should not require demonstration of goblet cells in mucosal biopsies don t biopsy the normal OGJ: cardia IM is common and we don t have any idea of its surveillance Riddell & Odze, 2009
37 Intestinal differentiation in metaplastic, non-goblet columnar epithelium in the esophagus 89 patients with CLO immunohistochemistry for markers of intestinal differentiation: MUC2, DAS-1, villin and cdx2 metaplastic esophageal columnar epithelium without goblet cells shows phenotypic evidence of intestinal differentiation supports the theory that squamous epithelium converts initially to non-goblet columnar epithelium before goblet cell metaplasia Hahn HP et al. Am J Surg Pathol, 2009

38 And we ain t no good at detecting goblet cells... goblet cells pseudo-goblet cells blue cells Wang H, et al. Poor agreement for detection of goblet cells in esophageal and GEJ biopsies. PUBLISHED ONLY IN ABSTRACT FORM
39 Oesophageal/OGJ biopsies Inter-observer variability features 7 international GI pathologists Kappa Value goblet cells 0.35 pseudo-goblet cells 0.10 gland type 0.54 Barrett s 0.15 Wang H, Brown I, Kumarasinghe P, Langner C, Lauwers G, Shepherd N, Vieth M, Srivastava A, Odze R; Modern Pathology 2012; 184A

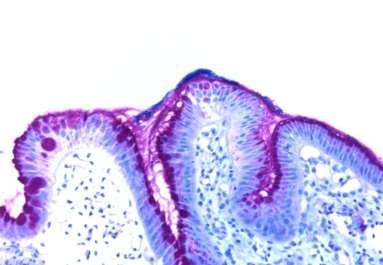
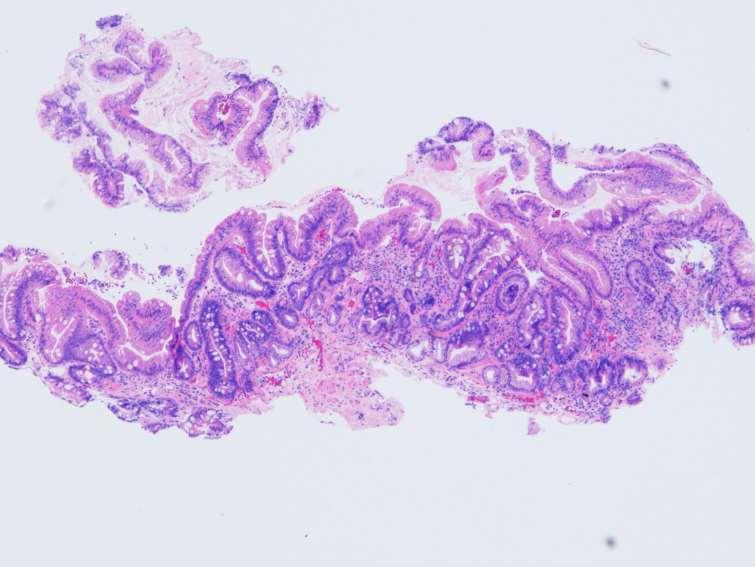
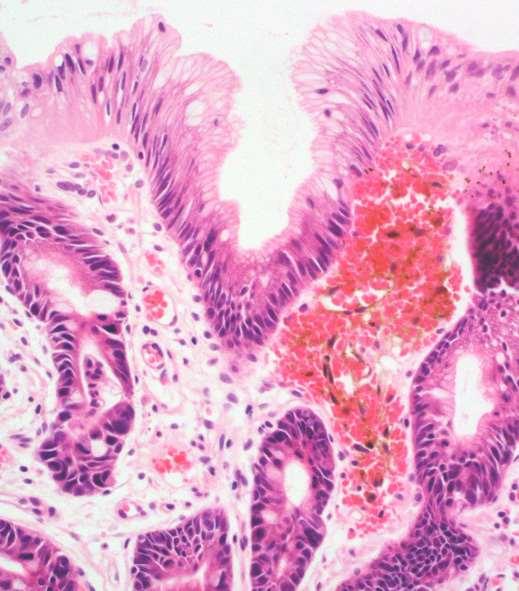
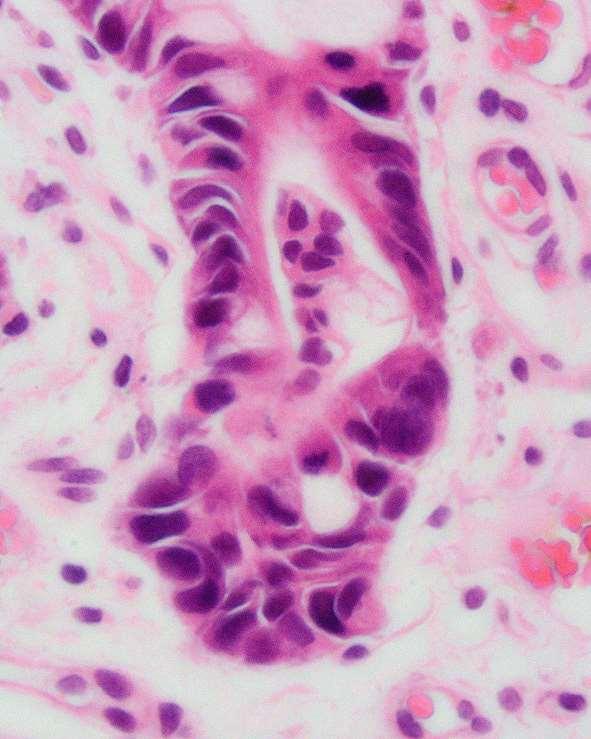
40 Is this intestinalisation? H & E ABPAS


41 Is this intestinalisation? H & E ABPAS

42

43

44 Call me cynical.
45 What about the new BSG Barrett s oesophagus management guidelines? In the event the new guidelines are disappointing, to the senior author of this review at least, in some of the pathology aspects. despite the major reservations about the usefulness of the pathological demonstration of IM, its pathological demonstration has been reintroduced in the new guidelines in defining pathological diagnostic terms, despite the sampling issues, the very poor levels of agreement in the demonstration of goblet cells/im, even by experts, and the fact that apparently non-intestinalised epithelium is actually intestinalised anyway in immunohistochemical and molecular studies Fitzgerald et al, 2014 Hopcroft & Shepherd, 2014
46 Barrett s oesophagus: pathological conundra If goblet cells are not specific, are there any specific pathological features of Barrett s oesophagus and, if there are, which are they?

47 Juxtaposition of glandular mucosa to native oesophageal structures seen in about 10-15% of biopsy sets diagnostic of CLO Takubo et al, 1995

48 Multilayered epithelium said to be specific to CLO and a suggestion that it is a precursor of CLO Glickman et al, 2001; Srivastava et al, 2007 no doubt that it is seen at the normal OGJ Takubo et al, 2008

49 Pancreatic phenotype more recently recognised as the fourth phenotype of CLO no doubt that it is also seen at the normal OGJ Takubo et al, 2008

50 Hybrid glands said to be specific to CLO Srivastava et al, 2007

51 Hybrid glands



52 Hybrid glands in the gastric antrum
53 recent evidence that glands with a pyloric-type phenotype are the initial CLO metaplasia (as Riddell and Odze suggested) and that hybrid glands represent the evolution of intestinalisation from these gastric-type glands proliferation in the middle of Barrett s glands, diminishing to the surface & base IdU dynamics demonstrate bidirectional migration, similar to gastric glands distribution of MUC5AC, TFF1, MUC6 and TFF2 in Barrett s mirrors pyloric glands LGR5 mrna is detected in the middle of Barrett s glands suggesting a stem cell niche in this locale, similar to that in the gastric pylorus both gastric and intestinal cell lineages within Barrett s glands are clonal, indicating derivation from a single stem cell Lavery D, Nicholson A, Poulsom R, Jeffery R, Hussain A, Gay L, Jankowski J, Zeki S, Barr H, Harrison R, Going J, Kadirkamanathan S, Davis P, Underwood T, Novelli M, Rodriguez Justo M, Shepherd N, Jansen M, Wright NA, McDonald SAC, 2014

54 The cardia feet of CLO Jansen et al, 2015

55 The Barrett s tree Jansen et al, 2015
56

57 Cardia feet or basal buds in CLO


58 This week s case
59 Specific to CLO? hybrid glands, multilayered epithelium, pancreatic phenotype none of these are specific but they are relatively more common in CLO compared to the stomach/ogj specialised intestinal metaplasia tends to infer that the IM of CLO is specific, and perhaps pathognomonic, to that condition. is there any feature, whether identified by morphological, histochemical, immunohistochemical or any other methodology, that is exclusive for CLO and not seen, for instance, in IM (especially incomplete) in the stomach?
60 Special techniques and specialised intestinal metaplasia complete IM unusual: Paneth cells rare electron microscopy intermediate cells, etc Takubo et al 1995 Levine et al 1989 immunohistochemistry: villin, colonic-type phenotype Das et al 1994, MacLennan et al 1999 cytokeratin immunohistochemistry Ormsby et al 1999 & (many) others


61 Cytokeratin immunohistochemistry in CLO cytokeratin 7 cytokeratin 20

62 Are cytokeratin subsets useful for distinguishing CLO from IM in the stomach? Antonioli DA Das KM El Zimaity H Falk GW Flejou J-F Goldblum JR Goyal RK Graham DH Jankowski JAZ Odze RD Richter JE Riddell RH Spechler SJ
63 Specificity of specialised epithelium of CLO There is no phenotype, however elucidated, that demonstrates that the epithelium of Barrett s oesophagus is specific to CLO and different to IM in the gastric mucosa Barrett s mucosa is therefore identical, in phenotype, to incomplete intestinal metaplasia in the stomach Jass, 2002
64 The role of histology in the diagnosis of CLO: the index endoscopy cardia IM/USSCLO but we should not seek this when there is endoscopic doubt: endoscopic inexperience stricturing ulceration hiatus hernia RCPath, 2002; Riddell & Odze, 2009 if we are not requiring the demonstration of IM, if there are no entirely specific histological features of CLO (excepting juxtaposition to native structures in 10-15% of biopsies) and if the diagnosis is essentially an endoscopic one...



65 WHY BIOPSY CLASSICAL BARRETT S OESOPHAGUS AT THE INDEX ENDOSCOPY?

66 The role of histology in the diagnosis of CLO: the index endoscopy you do see dysplasia HGD at index endoscopy one day, there will be a biomarker.. we won t stop them...
67 Pathological diagnosis of CLO is critically dependent on the amount of information from endoscopy demands adequate size and number of biopsies should not be reliant on the demonstration of IM, not because it isn t important but because many cases of CLO will be excluded if biopsy numbers are low demands a reporting strategy BSG Management Guidelines for Barrett s oesophagus,
68 Reporting CLO diagnostic for CLO corroborative of an endoscopic diagnosis of CLO biopsies in keeping with, but not specific for, CLO no evidence of CLO BSG Management Guidelines for Barrett s oesophagus,
69 Shepherd reporting CLO These biopsies show a combination of oesophageal-type squamous mucosa and glandular mucosa featuring cardiac and intestinal phenotypes. The histological features serve to corroborate the endoscopic diagnosis of Barrett's oesophagus. There is no evidence of dysplasia or malignancy.
70 The changing role of pathology in the management of Barrett s oesophagus diagnosis the effects of treatment the management of neoplasia


71 CLO: assessing response to treatment Ablation methodology: KTP laser, argon beam coagulation, photodynamic therapy, radiofrequency ablation all require concomitant acid suppression with PPIs cause squamous re-epithelialisation which may conceal underlying CLO mucosa -? neoplastic risk Biddlestone et al, 1998


72 CLO: assessing response to treatment Ablation methodology: KTP laser, argon beam coagulation, photodynamic therapy, radiofrequency ablation may cause mimicry of dysplasia and malignancy
73 The changing role of pathology in the management of Barrett s oesophagus diagnosis the effects of treatment the management of neoplasia
74 Neoplasia in Barrett s oesophagus indefinite for dysplasia low grade dysplasia high grade dysplasia intramucosal carcinoma invasive adenocarcinoma after Riddell et al 1983 Reid et al 1988
75 The problems of dysplasia in CLO often endoscopically normal and yet multifocal demands Levine/Seattle biopsy protocols current imaging techniques poor at diagnosing early malignancy


76 Long segment CLO surveillance with Seattle biopsies: Two biopsies from each quadrant every 2 cms 40 biopsy pots 352 individual sections
77 Dysplasia in CLO HGD was associated with co-existent adenocarcinoma in 30-55% of cases (now lower 25% quoted in 2008) has been an indication for oesophagectomy in management guidelines in Europe & North America inter-observer agreement good (amongst experts) for HGD (kappa 0.65) but LGD and indefinite have lower levels of I-O agreement Reid et al 1988; Montgomery et al, 2001; Treanor et al, 2007 HGD diagnosis to be confirmed by two experienced pathologists Loft, Alderson & Heading, 2005; Treanor et al, 2007 management of dysplasia should always be discussed in the Upper GI MDTM
78 Traditional management of CLO dysplasia Indefinite for dysplasia early re-evaluation with extensive biopsies following a course of PPI. Low grade dysplasia extensive biopsies after intensive acid suppression for 8-12 weeks. 6-monthly surveillance as long as disease is stable. High grade dysplasia if changes persist after intensive acid suppression and HGD is confirmed by two pathologists, oesophagectomy in specialised unit recommended (ablative therapy for patients unfit for surgery) BUT THIS IS CHANGING
79 Recently recognised dysplasia variants in CLO crypt dysplasia with surface maturation foveolar dysplasia serrated dysplasia
80 7% prevalence basal crypt dysplasia-like atypia (BCDA) 3 year surveillance period: 87% BCDA had previous or concurrent HGD/Ca v 59% controls developed HGD/Ca
81
82 Basal crypt dysplasia in Barrett s oesophagus we need more data some GI pathologists in the UK have evidence to support the Odze data in the UK, we recommend a designation of mucosa indefinite for dysplasia and await events with excellent endoscopy, EMR and good ablation, you won t go far wrong
 are absent can be")

83 Foveolar dysplasia assessment of grade of dysplasia difficult as main criteria (eg loss of nuclear polarity) are absent can be associated with conventional dysplasia elsewhere the conventional dysplasia is usually high grade foveolar dysplasia is biologically high grade
84 What about biomarkers? All biomarkers are currently regarded as experimental Riddell, 1996 Until randomised controlled evidence is available, biomarker panels cannot yet be recommended as routine of care BSG management guidelines, 2014
85 Newer techniques for the in-situ detection of neoplastic change in CLO magnification and high resolution endoscopy chromo-endoscopy auto-fluorescence endoscopy narrow band imaging microscopic tools: confocal microscopy; multiphoton microscopy in situ molecular analysis: FISH spectroscopic analysis: fluorescence spectroscopy; light scattering spectroscopy; optical coherence spectroscopy; Raman (inelastic) spectroscopy

86 Standard endoscopic view of CLO with HGD: no lesion identified

87 Chromo-endoscopy with indigo carmine dye-spray: HGD on histology
")
88 Endoscopic mucosal resection (EMR or ER) in CLO
89 How is the management of neoplasia complicating CLO changing? more conservative about surgery (30 day mortality 5-10%) increasing evidence that HGD only predicts concurrent carcinoma in about 20% of cases and is no longer a definitive indication for surgery better endoscopy: chromo-endoscopy, auto-fluorescence endoscopy and narrow band imaging: trimodal endoscopy localises and identifies dysplastic lesions, even if flat EMR, ESD and much better ablative therapy there is a lot less surgery..



90 The management of low and high grade dysplasia (and even intramucosal carcinoma) is very similar now not sure definite dysplasia & IMC invasive carcinoma Hopcroft & Shepherd, 2014
91 Management of neoplasia in CLO: the present and the future less major surgery trimodal endoscopy means the endoscopist spends the time and not the pathologist!! directed biopsies after such endoscopy and not random Seattle simpler pathological classifications fun EMRs (or ERs) for pathologists to look at more sensible patient-directed management
92 Barrett s oesophagus and the OGJ: take home messages there s more of it about & there s a lot more cancer definitions are changing and the diagnosis requires pathology less don t accept biopsies from the normal OGJ surveillance is recommended but is unproven and costly in endoscopic and pathological time the management of dysplasia has required laborious biopsy protocols, pathological sense, two (? expert) pathologists and MDTM discussion we now have the advent of smart endoscopes & clever techniques for the accurate diagnosis of CLO neoplasia and we have EMR to stop unnecessary surgery

93
94 Definition, derivation & diagnosis of Barrett s oesophagus: pathological perspectives H Lowes, T Somarathna & Neil A Shepherd A chapter for Stem Cells, Pre-Neoplasia & Early Cancer of the Upper GI Tract edited by Sir Nicholas A Wright & Marnix Jansen
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Pathology of the oesophagus and the stomach. Neil A Shepherd Gloucester, UK. Bristol Pathology 1 st Year Training School, The layers of the GI tract
 Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Henry Moon was one of the giants in academic pathology during my early years.
 Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Barrett esophagus is a premalignant condition resulting
 Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Handling of Upper GI Cancer Specimens
 Handling of Upper GI Cancer Specimens Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016 Pathology of oesophageal cancer Epidemiology Classification
Handling of Upper GI Cancer Specimens Prof Ray McMahon Histopathology Department Manchester Royal Infirmary Bryan Warren School Sarajevo November 2016 Pathology of oesophageal cancer Epidemiology Classification
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
The increasing incidence of esophageal adenocarcinoma
 GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues
 Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues Robert D. Odze, MD, FRCPC BULLET POINTS The gastric cardia is the area of mucosa located distal to the GEJ (proximal aspect of gastric
Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues Robert D. Odze, MD, FRCPC BULLET POINTS The gastric cardia is the area of mucosa located distal to the GEJ (proximal aspect of gastric
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
The presence of intestinal-type goblet cells (ITGCs) in
 in") Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Histological Features of Gastric Cardia in Adults: an Autopsy
 original PAPERs Histological Features of Gastric Cardia in Adults: an Autopsy Study Zorica M. Stojsic 1, Radmila M. Stevanovic 1, Martina M. Stojanovic 1, Aleksandar D. Stanojevic 2, Dragoljub T. Bacetic
original PAPERs Histological Features of Gastric Cardia in Adults: an Autopsy Study Zorica M. Stojsic 1, Radmila M. Stevanovic 1, Martina M. Stojanovic 1, Aleksandar D. Stanojevic 2, Dragoljub T. Bacetic
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
During the past 30 years, the incidence of esophageal ORIGINAL ARTICLES
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:38 43 ORIGINAL ARTICLES Optical Coherence Tomography to Identify Intramucosal Carcinoma and High-Grade Dysplasia in Barrett s Esophagus JOHN A. EVANS,* JOHN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:38 43 ORIGINAL ARTICLES Optical Coherence Tomography to Identify Intramucosal Carcinoma and High-Grade Dysplasia in Barrett s Esophagus JOHN A. EVANS,* JOHN
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
Barrett s s Dysplasia
 Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Intestinal metaplasia at the gastro-oesophageal junction: Helicobacter pylori gastritis or gastro-oesophageal reflux disease?
 Gut 1998;43:17 21 17 Gastroenterology, Hepatology, and Infectious Diseases A Hackelsberger V Schultze G Manes J-E Dominguez-Muñoz P Malfertheiner Pathology, Otto-von-Guericke University, Magdeburg, Germany
Gut 1998;43:17 21 17 Gastroenterology, Hepatology, and Infectious Diseases A Hackelsberger V Schultze G Manes J-E Dominguez-Muñoz P Malfertheiner Pathology, Otto-von-Guericke University, Magdeburg, Germany
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
Pseudoinvasion and how to deal with it
 Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the
Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease
 Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging
 Alimentary Pharmacology & Therapeutics Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging G. K. ANAGNOSTOPOULOS*, K. YAO*, P. KAYE,
Alimentary Pharmacology & Therapeutics Novel endoscopic observation in Barrett s oesophagus using high resolution magnification endoscopy and narrow band imaging G. K. ANAGNOSTOPOULOS*, K. YAO*, P. KAYE,
Division of Anatomic Pathology & Molecular Oncology, University of Utah and ARUP Laboratories, Huntsman Cancer Institute, Salt Lake City, UT, USA
 REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Current challenges in Barrett s esophagus
 MEDICAL GRAND ROUNDS TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY Current challenges in Barrett s esophagus GARY W. FALK, MD * Director, Center for Swallowing and Esophageal
MEDICAL GRAND ROUNDS TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY Current challenges in Barrett s esophagus GARY W. FALK, MD * Director, Center for Swallowing and Esophageal
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
Gastric adenocarcinoma of the
 Comment From the Editors Spasmolytic Polypeptide- Expressing Metaplasia and Intestinal Metaplasia: Time for Reevaluation of Metaplasias and the Origins of Gastric Cancer Gastric adenocarcinoma of the intestinal
Comment From the Editors Spasmolytic Polypeptide- Expressing Metaplasia and Intestinal Metaplasia: Time for Reevaluation of Metaplasias and the Origins of Gastric Cancer Gastric adenocarcinoma of the intestinal
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Stage 4 gastric adenocarcinoma icd 10
 > Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
> Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
The esophagogastric junction (EGJ), the region between
, the region between") Review Article Definition of the Esophagogastric Junction A Critical Mini Review Qin Huang, MD, PhD N Context. Accurate diagnosis of diseases involving the esophagogastric junction (EGJ) is challenging
Review Article Definition of the Esophagogastric Junction A Critical Mini Review Qin Huang, MD, PhD N Context. Accurate diagnosis of diseases involving the esophagogastric junction (EGJ) is challenging
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
05/07/2018. What colorectal cancer screening is all about. Not so simple pathology: issues from the screening programme
 Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
32 Adenocarcinoma of the oesophagogastric junction
 Adenocarcinoma of the oesophagogastric junction S.J. Spechler P. Hainaut M.F. Dixon R. Lambert R. Genta R. Siewert Definition Adenocarcinomas that straddle the junction of the oesophagus and stomach are
Adenocarcinoma of the oesophagogastric junction S.J. Spechler P. Hainaut M.F. Dixon R. Lambert R. Genta R. Siewert Definition Adenocarcinomas that straddle the junction of the oesophagus and stomach are
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
University Mainz. Early Gastric Cancer. Ralf Kiesslich. Johannes Gutenberg University Mainz, Germany. Early Gastric Cancer 15.6.
 Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Esophageal submucosal mass icd 10
 Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
The incidence of esophageal adenocarcinoma is rising in the ENDOSCOPY CORNER
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:843 847 ENDOSCOPY CORNER Acetic Acid Spray Is an Effective Tool for the Endoscopic Detection of Neoplasia in Patients With Barrett s Esophagus GAIUS LONGCROFT
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Table 2.9. Case control studies of helicobacter pylori infection and oesophageal adenocarcinoma
 Characteristics of Characteristics of controls Detection Chow et al (1998) 1993-1995 129 of newly diagnosed oesophageal/gastric cardia (OGC) adenocarcinoma. 224 population controls selected by random digit
Characteristics of Characteristics of controls Detection Chow et al (1998) 1993-1995 129 of newly diagnosed oesophageal/gastric cardia (OGC) adenocarcinoma. 224 population controls selected by random digit
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
evidence note Radiofrequency ablation for Barrett s oesophagus with highgrade What is an evidence note Key points Literature search Introduction
 In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
In response to an enquiry from the National Cancer Waiting Times Delivery Group What is an evidence note Evidence notes are rapid reviews of published secondary clinical and cost-effectiveness evidence
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert