12/7/2011. Pathological mimics of malignancy in the GI tract. Professor Neil A Shepherd President, British Division of the IAP
|
|
|
- Christal Melton
- 5 years ago
- Views:
Transcription
1 Pathological mimics of malignancy in the GI tract Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 How do we become aware of the problems and the errors? in house: double reporting, casual second opinion, etc review at multidisciplinary meetings and network reviews second expert opinion practice medicolegal practice duty of care and GMC reviews the literature brave papers, Lesson of the Month Mimics of neoplasia in the GI tract problems with reactive v dysplasia just as common if not more so than benign v malignant implications of an erroneous diagnosis often just as severe (cf HGD and oesophageal resection) we will stick with just five important mimics 1



2 Basil C Morson, doyen of GI pathologists It s your job to control surgeons Peter G Isaacson, doyen of lymphoma pathologists 2


3 Mimics numbers 1 & 2 Type 1 lesions: only in the stomach. Superficial ulceration with irregular and atypical acinar structures fading into regular regenerative glands Type 2 lesions: oesophagus, stomach and rectum Abnormal stromal cells associated with ulceration Isaacson PG. Histopathology 1982; 6: Mimic number 1 - Reactive gastritis with erosions Overdiagnosis of cancer Reactive gastritis with erosions is the commonest cause of misdiagnosis of gastric cancer Isaacson et al,



4 Reactive gastritis mimicking dysplasia it s all dysplastic!! Overdiagnosis of dysplasia Reactive gastritis with intestinal metaplasia Overdiagnosis of cancer Reactive gastritis with malorientation/ tangential sectioning 4

5 Isaacson type 1 this week s case Mimic number 1 - Reactive gastritis with erosions never diagnose dysplasia or cancer when the dodgy cells are in fibrinous material context are the clinical and endoscopic features suggestive of cancer? what helps? histochemistry and immunohistochemistry do not help much what to do second opinion, expert opinion, ASK FOR ANOTHER BIOPSY (especially after treatment) Mimic number 2 Type 2 lesions: oesophagus, stomach and rectum Abnormal stromal cells associated with ulceration Isaacson PG. Histopathology 1982; 6: especially in association with proliferative epithelium (usually squamous but sometimes glandular) 5






6 Inflammatory polyp at the OGJ It is both proliferative squamous (sometimes glandular) epithelium and the bizarre stromal cells that cause the trouble Isaacson et al, 1982 Al-Sam, Lakhani & Davies, 1998 Gill, Piris & Warren, 2003 The stromal cells Gloucestershire can be really Cellular Pathology bizarre Laboratory and very worrying.. 6 oesophagectomies: 3 local/network/second opinion 3 medicolegal 6
 This week s OGJ polyp This week s")
7 Mimic number 2 bizarre stromal cells with/without proliferative epithelium context are the clinical and endoscopic features suggestive of cancer? what helps? immunohistochemistry what to do discuss in MDTM, second opinion, expert opinion, ASK FOR ANOTHER BIOPSY (especially after treatment) This week s OGJ polyp This week s OGJ polyp CK 7
8 Inflammatory polyp at the OGJ immunos helpful: cytokeratin versus ASMA, vimentin, CD10 if in doubt, ask for a second biopsy/emr CD10 Inflammatory polyp at the OGJ immunos helpful: cytokeratin versus ASMA, vimentin, CD10 Mimic number 2 bizarre stromal cells with/without proliferative epithelium context are the clinical and endoscopic features suggestive of cancer? what helps? immunohistochemistry what to do discuss in MDTM, second opinion, expert opinion, ASK FOR ANOTHER BIOPSY (especially after treatment) but don t get too hung up on mimics because occasionally the mimic is the real thing.. 8



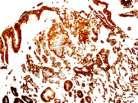
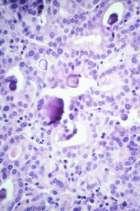
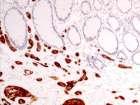
9 Mimic number 3 64 F. Polyp with superficial ulcer in stomach. not Gloucestershire slides! Mimic number 3 64 F. Polyp with superficial ulcer in stomach. Mimic number 3 64 F. Polyp with superficial ulcer in stomach. cytokeratin 9




10 Mimic number 3 64 F. Polyp with superficial ulcer in stomach. Here comes the total gastrectomy.. Mimic number 3 64 F. Polyp with superficial ulcer in stomach. Here comes the total gastrectomy.. synaptophysin ET/NET/carcinoid v carcinoma Four types of gastric chronic atrophic Zollinger-Ellison syndrome sporadic intrinsic abnormality of parietal cells The first is the commonest, is benign (unless..) and treated very conservatively (EMR/nothing) 10



11 Context in gastric ETs 46M. Mass in D2. EMR resection. Is this pancreatic adenocarcinoma or metastatic prostatic carcinoma? 11
12 PAS 12
 distant metastasis very uncommon very good prognosis")
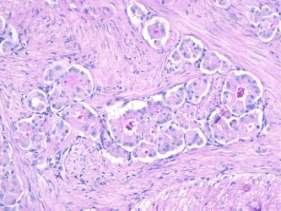
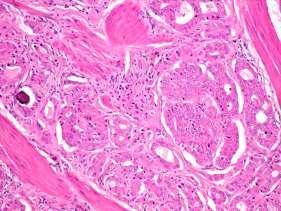
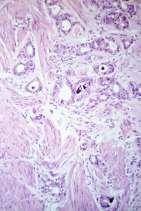
13 ? synaptophysin somatostatin Duodenal D-cell ETs glandular architecture PAS-positive luminal cell borders psammoma bodies non-argentaffin non-argyrophil by Grimelius synaptophysin positive usually chromogranin A positive somatostatin positive Duodenal D-cell ETs tumours of low grade malignancy lymph node metastasis in ~25% (usually >2 cm) distant metastasis very uncommon very good prognosis after local excision 13




14 62M. Polyp in the rectum. Mimic number 3 62M. Polyp in the rectum. Mimic number 3 cytokeratin chromogranin Mimic number 3 62M. Polyp in the rectum. Here comes the anterior resection synaptophysin 14

15 Context in rectal carcinoids Mimic number 3 Endocrine tumours of the GI tract context are the clinical and endoscopic features suggestive of cancer? context what does the adjacent gastric mucosa show? What is the serum gastrin? Does the patient have pernicious anaemia? what helps? immunohistochemistry, certainly, but understand the results.. what to do discuss in MDTM, second opinion, expert opinion, ASK FOR ANOTHER BIOPSY Mimic number 3 ETs of the GI tract BUT don t forget that the occasional mimic is the real thing 15







16 63M. Polyp in stomach. Biopsies. called carcinoid, possibly arising in CAG BUT obstructed picture and CT showed large mass in proximal stomach total gastrectomy 63M. Total gastrectomy. At gastrectomy 16

17 Mimic number 3 ETs of the GI tract don t forget that the occasional mimic is the real thing chronic atrophic gastritis predisposes to carcinoma of the stomach. you can get composite tumours and neuro-endocrine carcinomas be careful, context is all important but don t overcall benign gastric and rectal endocrine tumours Mimic number 4 mucosal prolapse all encompassing pathological concept du Boulay, Fairbrother & Isaacson, 1983 fibro-muscular proliferation in the lamina propria, epithelial hyperplasia, superficial ulceration with secondary inflammation and relative paucity of inflammation solitary ulcer (mucosal prolapse) syndrome, inflammatory cloacogenic polyps, at stomata, in the sigmoid colon associated with diverticular disease & elsewhere Lobert & Appelman, 1981; du Boulay et al, 1983; Saul, 1987; Chetty et al, 1993 epithelial hyperplasia & villiform architecture mimics villous adenoma in the colorectum, especially in inflammatory cloacogenic polyp mucosal prolapse often accompanied by misplaced epithelium, in the colon and rectum (so-called colitis cystica profunda) and at stomata mimics carcinoma Ileostomy nodule 17




")
18 Beware the inflamed ileostomy with mucosal prolapse Nodule on colostomy Solitary ulcer (mucosal prolapse) syndrome 18
 hyperplasia traps the unwary into calling them large villous adenomas may be seen in")
 with florid proctitis cystica profunda Inflammatory")
19 Polypoid mucosal prolapse lower rectal/anal most common: inflammatory cloacogenic polyp epithelial (villous) hyperplasia traps the unwary into calling them large villous adenomas may be seen in association with diverticulosis, at stomas, in SUMPS, etc Inflammatory cloacogenic polyp (polypoid mucosal prolapse at the anorectal junction) with florid proctitis cystica profunda Inflammatory cloacogenic polyp 19




20 Mimic number 4 mucosal prolapse BUT don t forget that the occasional mimic is the real thing the changes of classical solitary ulcer (mucosal prolapse) syndrome may occur as a complication of associated carcinoma Li & Hamilton, 1998 Polypoid mucosal prolapse at the anorectal junction a word of warning with inflammatory cloacogenic polyp 4 cases of adenomas of the lower rectum causing secondary polypoid mucosal prolapse Parfitt & Shepherd, 2008 a b c Ki-67 d p53 20





21 a b c Ki-67 d p53 Mimic number 5 epithelial misplacement in intestinal polyps misplacement of epithelium into the submucosa and beyond is a potent mimic of malignancy there are clues to the appropriate diagnosis Peutz-Jeghers polyps in the small intestine small hyperplastic polyps in the left colon and rectum larger serrated polyps in the right colon (especially into lymphoglandular complexes) adenomas, ESPECIALLY LARGE ONES IN THE SIGMOID COLON Peutz-Jeghers syndrome 21

 same epithelium as surface,")


22 ileum duodenum Epithelial misplacement in adenomas 85% in sigmoid colon unusual in rectum (unless there has been previous meddling) same epithelium as surface, accompanied by lamina propria, haemosiderin deposition what about misplaced epithelium at the diathermy margin? this is the biggest difficult diagnostic issue in BCSP 22



23 Epithelial misplacement vs invasive carcinoma There is a very important adage in pathology: why make two diagnoses when one will do? BSCP case sigmoid colonic polyp in 62M superficial ulceration and inflammation with epithelial misplacement 64M. BCSP. Descending colonic polyp epithelial misplacement in a lympho-glandular complex just like in inverted hyperplastic polyps 23

 national expert panel has been established, funded by BCSP, to deal with the very difficult")
24 Artefactual epithelial misplacement Enhancement of dysplastic change with inflammation and superficial ulceration Mimic number 5 epithelial misplacement in intestinal polyps misplacement of epithelium into the submucosa and beyond is a potent mimic of malignancy there are clues to the appropriate diagnosis, especially in adenomas: site and size haemosiderin and accompaniment by lamina propria cytology similar to surface neoplasm but don t get too hooked up on mimics it may be the real thing.. sigmoid colonic polyps with such changes are selected into BCSP (they bleed) national expert panel has been established, funded by BCSP, to deal with the very difficult cases we are seeing in BCSP 24



25 Overdiagnosis of cancer Large craggy gastric ulcer.? malignant. Gastric biopsies. Overdiagnosis of cancer Large craggy duodenal ulcer. Duodenal cytology and biopsies. 38 F. Appendicectomy for acute appendicitis. Six months later small bowel resection for obstruction. 25



26 Low power of mucosa and overlying fibrinous exudate Higher power of mucosa Note the pale cells and the red cells! Higher power of mucosa 26




27 these are goblet cells other surviving cells are endocrine cells and Paneth cells they are selectively preserved, presumably because of their less need for oxygen but become strikingly dissociated 35F. Small bowel resection. CK7 This is subacute ischaemia with necrosis of most epithelial cells and survival and dispersal of goblet cells 27
28 Survival and dispersal of goblet cells in small and large intestinal ischaemia, mimicking signet ring cell carcinoma Biedrzycki et al. Lesson of the Month: Isolated intramucosal goblet cells in subacute ischaemic enteritis: mimicry of signet ring cell carcinoma. Histopathology 2005; 46: also seen in pseudomembranous colitis: Abdulkader et al. Signet-ring cells associated with pseudomembranous colitis. Virchows Arch 2003; 442: Avoiding the pitfalls know of them and recognise them correlate with clinical data think of the context do levels, do special stains: routine (AB)PAS immunohistochemistry cytokeratin, synaptophysin, stromal markers, etc molecular biology, especially for malignant lymphoma in stomach Avoiding the pitfalls be honest and use clinically useful categories: indefinite for dysplasia, please repeat! ask for a bigger biopsy such as EMR much easier interpretation.. MDTM discussion double reporting ask a friend (or an expert if he/she ain t a friend) subspecialisation (my friend Bryan Warren has seen hundreds of these and he doesn t get them wrong.) 28



29 The three most important factors when assessing problematic GI biopsies: CONTEXT CONTEXT CONTEXT Take home messages there are any number of conditions that mimic malignancy in the GI tract reactive conditions mimicking dysplasia are as common and cause as many problems as those that mimic malignancy & the implications of an erroneous diagnosis may be just as severe all pathologists must be aware of the implications of their diagnoses: if the implication of a diagnosis is major surgery, then pathologists need to ensure that they recognise all mimics of malignancy don t get too fixated with mimics: occasionally the mimic is the real thing!! 29
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Pseudoinvasion and how to deal with it
 Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Pseudoinvasion and how to deal with it Professor Neil A Shepherd Gloucester & Cheltenham, UK European Society of Pathology Bilboa, 12 June 2018 Enterprise Interest None Pseudoinvasion and how to deal with
Polypoid lesions of the gastrointestinal tract
 Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
The pathology of neuroendocrine tumours of the gut
 The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
The pathology of neuroendocrine tumours of the gut Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The pathology of neuroendocrine tumours (NETs)
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
05/07/2018. What colorectal cancer screening is all about. Not so simple pathology: issues from the screening programme
 Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Primary mucinous adenocarcinoma developing in an ileostomy stoma
 Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
polyps of the colon and rectum
 J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
J. clin. Path., 1973, 26, 25-31 Pseudo-carcinomatous invasion in adenomatous polyps of the colon and rectum T. MUTO, H. J. R. BUSSEY, AND B. C. MORSON From St Mark's Hospital, London SYNOPSIS The histology
Small Bowel Cases. Introduction. Introduction, Continued 12/7/2011. Lesions Found on endoscopic biopsies Just Like Signing Out
 Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Pitfalls in the Diagnosis of Inflammatory Bowel Disease
 Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects
 Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
The Kristin Henry Lecture. Colorectal cancer screening: extraordinary conundra for pathology
 The Kristin Henry Lecture Colorectal cancer screening: extraordinary conundra for pathology Professor Neil A Shepherd Gloucester & Cheltenham, UK Edinburgh Pathology 2013 Friday, 21 June 2013 British Division
The Kristin Henry Lecture Colorectal cancer screening: extraordinary conundra for pathology Professor Neil A Shepherd Gloucester & Cheltenham, UK Edinburgh Pathology 2013 Friday, 21 June 2013 British Division
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Commonly Encountered Neuro-Endocrine Tumors of the Gut
 Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
The Kamal Ishak Lecture. The pathology of bowel cancer screening
 The Kamal Ishak Lecture The pathology of bowel cancer screening Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November
The Kamal Ishak Lecture The pathology of bowel cancer screening Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November
EDUCATIONAL CASES E1 & E2. Natasha Inglis 20/03/15
 EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Condyloma Acuminatum. Mimics of Bladder Cancer. Squamous Papilloma. Squamous epithelium in bladder
 Mimics of Bladder Cancer Murali Varma Cardiff, UK wptmv@cf.ac.uk Squamous epithelium in bladder Non-keratinising vaginal type mucosa common in trigone region in women Normal variant Sarajevo Nov 2013 Squamous
Mimics of Bladder Cancer Murali Varma Cardiff, UK wptmv@cf.ac.uk Squamous epithelium in bladder Non-keratinising vaginal type mucosa common in trigone region in women Normal variant Sarajevo Nov 2013 Squamous
2nd week. preexam. GIT system. Atyaf group. Qs team
 2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Pathology of the oesophagus and the stomach. Neil A Shepherd Gloucester, UK. Bristol Pathology 1 st Year Training School, The layers of the GI tract
 Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Inverted hyperplastic polyposis of the colon
 56 J Clin Pathol 1993;46:56-60 Inverted hyperplastic polyposis of the colon N A Shepherd Department of Histopathology, Gloucestershire Royal Hospital, Great Western Road, Gloucester, GL1 3NN N A Shepherd
56 J Clin Pathol 1993;46:56-60 Inverted hyperplastic polyposis of the colon N A Shepherd Department of Histopathology, Gloucestershire Royal Hospital, Great Western Road, Gloucester, GL1 3NN N A Shepherd
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
In-situ and invasive carcinoma of the colon in patients with ulcerative colitis
 Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Gastrointestinal Malignancies. Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline
 Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Tumors of the Intestines. Malignant Lesion. Adenocarcinoma. sessile Serrated Adenomas
 Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract
 Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Original Report. Carcinoid Tumors of the Stomach: A Clinical and Radiographic Study
 Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
CT Evaluation of Bowel Wall Thickening. Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University.
 CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
CT Evaluation of Bowel Wall Thickening By Dr: Adel El Badrawy; M.D. Lecturer of Radio Diagnosis Faculty of Medicine Mansoura University. The CT findings of bowel wall thickening includes 1 Degree of thickening.
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications
 Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Stage 4 gastric adenocarcinoma icd 10
 > Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
> Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
27
 26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis
 Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis ALAN P. LYSS, MD,* JOHN J. THOMPSON, MD,t AND JOHN H. GLICK, MD* F Patients with ulcerative colitis are at increased risk of
Adenocarcinoid Tumor of the Colon Arising in Preexisting Ulcera tive Colitis ALAN P. LYSS, MD,* JOHN J. THOMPSON, MD,t AND JOHN H. GLICK, MD* F Patients with ulcerative colitis are at increased risk of
Update on the pathological classification of gastritis. Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada
 Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Jesse K. McKenney, MD
 Jesse K. McKenney, MD Outline Microscopic anatomy of the urinary bladder Diagnosing invasion Subtle patterns (variants) of carcinoma Clinically important variants of carcinoma Microanatomy of Bladder Initial
Jesse K. McKenney, MD Outline Microscopic anatomy of the urinary bladder Diagnosing invasion Subtle patterns (variants) of carcinoma Clinically important variants of carcinoma Microanatomy of Bladder Initial
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Upper GIT IV Gastric cancer
 Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Circulation: Y Case number: 601 Number of responses: 80 Date: 30 NOV 12
 Circulation: Y Case number: 600 Number of responses: 70 Date: 30 NOV 12 Male, aged 34 Previous right empyema. Central right lung cancer Right Pneumonectomy Right lung containing an ill-defined tumour 120
Circulation: Y Case number: 600 Number of responses: 70 Date: 30 NOV 12 Male, aged 34 Previous right empyema. Central right lung cancer Right Pneumonectomy Right lung containing an ill-defined tumour 120