ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
|
|
|
- Carmella Skinner
- 6 years ago
- Views:
Transcription
1 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological Pathology The Johns Hopkins Medical Institutions
2 2 High Grade PIN vs. PIN-Like Ductal Adenocarcinoma Most prostatic ductal adenocarcinomas of the prostate are characterized by cribriform and/or papillary architecture lined by columnar pseudostratified malignant epithelium. PIN-like ductal adenocarcinomas closely resembles high-grade prostatic intraepithelial neoplasia (HGPIN) composed of simple glands with predominantly flat or tufting architecture. Cytologically, tumors are characterized by tall columnar atypical cells, basally located nuclei, and amphophilic cytoplasm. The tumors lack marked pleomorphism, necrosis, solid areas, cribriform formation, or true papillary fronds. No basal cells are present on p63 and/or high molecular weight cytokeratin staining. PIN-like ductal adenocarcinoma differs from HGPIN by the presence of cystically dilated glands, occasionally more crowded glands, a greater predominance of flat architecture, and less frequently prominent nucleoli. Verification often requires the immunohistochemical documentation of the absence of basal cells in numerous atypical glands. Although usual ductal adenocarcinoma is considered comparable to Gleason score 8, PIN-like ductal adenocarcinoma is accompanied by Gleason score 6 acinar carcinoma and behaves similar to Gleason score 6 acinar cancer. Recognition of this entity is critical to differentiate it from both HGPIN and conventional ductal adenocarcinoma. Tavora F, Epstein JI. High grade prostatic intraepithelial neoplasia-like ductal adenocarcinoma of the prostate: A clinicopathologic study of 28 cases. Am J Surg Pathol (July) 32: 1060,1067, 2008.
3 3 High Grade PIN vs. Intraductal Carcinoma (IDC-P) IDC-P is defined as malignant epithelial cells filling large acini and prostatic ducts, with preservation of basal cells. Its distinction from HGPIN is that it has: Solid or dense cribriform pattern or Loose cribriform or micropapillary pattern with either: Marked nuclear atypia: nuclear size 6 x normal Non-focal comedonecrosis IDC-P on prostate biopsies is frequently associated with high-grade cancer and poor prognostic parameters at radical prostatectomy as well as potentially advanced disease following other therapies. These findings support prior studies that IDC-P represents an advanced stage of tumor progression with intraductal spread of tumor. Consideration should be given to treat patients with IDC-P on biopsy aggressively even in the absence of documented infiltrating cancer.
4 4 Cribriform Acinar Adenocarcinoma Cribriform IDC-P Absence of contour or branching architecture of prostatic ducts Contour or branching architectures of prostatic ducts Irregular, infiltrating borders Rounded, circumscribed borders Absence of basal cells Basal cells present Ductal Adenocarcinoma IDC-P Cribriform with large slit-like lumina Cribriform with small rounded lumens Tall columnar cells Cuboidal cells Papillary fronds with fibrovascular cores Micropapillary tufts lacking fibrovascular cores Basal cells usually absent Basal cells always present Guo CC, Epstein JI. Intraductal carcinoma of the prostate: Histologic features and clinical significance. Mod Pathol (December). 19: , 2006.
5 5 Cribriform Gleason Pattern 3 Adenocarcinomas vs. Cribriform Gleason Pattern 4 Adenocarcinomas With the exception of cases of cribriform acinar prostate cancer with comedonecrosis, which is Gleason pattern 5, all cribriform acinar prostate cancer should be graded as Gleason pattern 4 for the following reasons. Even in a highly selected set of images thought to be the best candidates for cribriform pattern 3, most experts interpret the cribriform patterns as pattern 4. Most of the cribriform foci thought to be candidates for cribriform pattern 3 (73%) are associated with more definitive pattern 4 elsewhere on the needle biopsy specimen. Conceptually, one would expect the change in grade from pattern 3 to pattern 4 to be reflected in a distinct architectural paradigm shift where cribriform as opposed to individual glands are formed, rather than merely a subjective continuum of differences in size, shape and contour of cribriform glands. The only reason why cribriform pattern 3 even exists is because of the original Gleason schematic diagram, although Gleason never specifically studied the prognostic difference between what he called cribriform Gleason pattern 3 compared to Gleason pattern 4, and many of Gleason s cribriform Gleason pattern 3 cancers may not even have been infiltrating carcinomas due to the lack of availability of immunohistochemistry for basal cell markers. There is poor reproducibility amongst experts differentiating cribriform pattern 3 vs. pattern 4 due to: 1) Disagreement as to what are the key diagnostic features in a given case (ie. irregular distribution of lumina & variable slit-like lumina favor pattern 4 vs. small glands & regular contour favor pattern 3.
6 6 2) Disagreement as to assessment of given criteria: regular vs. irregular distribution of lumina Latour M, Amin MB, Billis A, Egevad L, Grignon DJ, Humphrey PA, Reuter VE, Sakr WA, Srigley JR, Wheeler TM, Yang XJ, Epstein JI. Grading of invasive cribriform carcinoma on prostate needle biopsy: An interobserver study among experts in genitourinary pathology. Am J Surg Pathol (October) 32: , 2008.
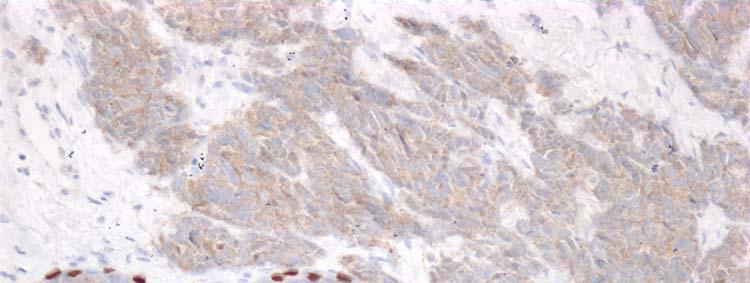
7 7 p63 Positive Prostate Adenocarcinoma vs. Basal Cell Carcinoma Rarely, prostate cancer can aberrantly express diffuse p63 staining in a nonbasal cell distribution leading to the erroneous diagnosis of atrophy or basal cell carcinoma. Over 90% show a distinctive morphology composed predominantly of glands, nests, and cords with atrophic cytoplasm, hyperchromatic nuclei, and visible nucleoli. The diagnosis of prostate cancer is based on the morphology and confirmed by the absence of high molecular weight cytokeratin staining and positivity for alpha-methylacyl-coa racemase (AMACR) in the atypical glands. Basal cell carcinoma usually differs from p63 positive cancer in its architectural patterns. Patterns unique to basal cell carcinoma include: 1) adenoid cystic pattern; 2) large solid basaloid nests with comedonecrosis; 3) nests surrounded by a rim of collagen where the there is a dual cell population of cells consisting of inner cells with eosinophilic cytoplasm and outer basaloid cells with scant cytoplasm; and 4) irregular sized and shaped basaloid nests often with a desmoplastic stromal response. There is one pattern of basal cell carcinoma that consists of individual small glands with multilayering that resembles basal cell hyperplasia and p63 positive prostate cancer. The lack of high molecular weight cytokeratin positivity (HMWCK) and positivity for PSA and AMACR rules out this pattern of basal cell carcinoma. There are several other situations where there is immunohistochemical labeling of prostate cancer with basal cell markers. Prostate cancer may show scattered cells positive for basal cell markers. The positivity is not in a basal cell distribution and represent aberrant staining of cancer cells. This phenomenon is more typically seen with HMWCK as compared to p63. More rarely, one can see adenocarcinoma of the prostate with focal retention of its basal cell layer. Only cases that are the most unequivocal prostate cancer based on architecture and cytology should be diagnosed in the face of basal cell staining.
8 8 Osunkoya AO, Hansel DE, Sun X, Netto GJ, Epstein JI. Aberrant diffuse expression of p63 in adenocarcinoma of the prostate on needle biopsy and radical prostatectomy: report of 21 cases. Am J Surg Pathol (March) 32: , Ali T, Epstein JI. False positive labeling of prostate cancer with high molecular weight cytokeratin: p63 a more specific immunomarker for basal cells. Am J Surg Pathol (December) 32:1890-5, Oliai BR, Kahane H, Epstein JI. Can basal cells be seen in adenocarcinoma of the prostate? An immunohistochemical study using high molecular weight cytokeratin. Am J Surg Pathol 26: , 2002.
9 9 Partial Atrophy vs. Prostate Cancer Partial atrophy is the most common mimicker of prostate cancer. Partial atrophy may still retain the lobular pattern of post-atrophic hyperplasia, or have more of a disorganized diffuse appearance. Partial atrophy lacks the basophilic appearance of fully developed atrophy as the nuclei are more spaced apart. The presence of crowded glands with pale cytoplasm may lead to an overdiagnosis of low-grade adenocarcinoma. At higher power, however, the glands have benign features characterized by undulating luminal surfaces with papillary infolding. Most carcinomas have more straight, even luminal borders. In addition, the glands are partially atrophic with nuclei in areas reaching the full height of the cytoplasm. The nuclear features in partial atrophy tend to be relatively benign without prominent nucleoli, although nuclei may appear slightly enlarged with small nucleoli. One should hesitate diagnosing cancer when the nuclei occupy almost the full cell height and the cytoplasm has the same appearance as surrounding more obvious benign glands. Partial atrophy typically has a patchy basal cell layer and may express racemase and in small foci on needle biopsy no basal cells may be present, mimicking the staining pattern seen with prostate cancer. Wang W, Sun X, Epstein JI. Partial atrophy on prostate needle biopsy: A morphological and immunohistochemical study. Am J Surg Pathol (June) 32: , Oppenheimer JR, Epstein JI. Partial atrophy in prostate needle cores-another diagnostic pitfall for the surgical pathologist. Am J Surg Pathol 22: , 1998.
10 10 Gastrointestinal Stromal Tumors (GIST) vs. Other Prostatic Stromal Tumors Gastrointestinal stromal tumors (GISTs) are typically not included in the differential diagnosis of spindle cell tumors seen on prostate needle biopsy. However, their recognition is critical due to their unique clinical management. Rectal or extraintestinal GIST can result in a clinical impression of a prostatic lesion. One should consider CD117 (c-kit) in the immunohistochemical panel to exclude GIST before diagnosing a solitary fibrous tumor, leiomyosarcoma, or specialized prostatic stromal tumor on prostate needle biopsy. Herawi H, Montgomery EA, Epstein JI. Gastrointestinal stromal tumors (GIST) on prostate needle biopsy: a clinicopathologic study of 8 cases. Am J Surg Pathol (November) 30: , 2006.
11 1 Large Cell Neuroendocrine Versus Small Cell Carcinoma: When, Whether and How to Make the Distinction Jeffrey L. Myers, M.D. A. James French Professor and Director, Division of Anatomic Pathology The University of Michigan, Ann Arbor, MI Objectives At the end of this presentation attendees will understand, 1) current criteria for separating large cell neuroendocrine from small cell carcinoma, and 2) the clinical, biological, histologic and phenotypic overlap between the two. Key Points Small cell carcinoma (SCLC) is defined on basis of cytologic criteria. Large cell neuroendocrine carcinoma (LCNEC) is defined by a combination of histologic (i.e. neuroendocrine morphology, necrosis) and cytologic (i.e. large cell size, cytoplasm, nucleoli, coarse chromatin, high mitotic rate) criteria as well as the presence of neuroendocrine differentiation demonstrated using immunohistochemistry. LCNEC is separated from atypical carcinoid tumors based primarily on consistent presence of necrosis and higher mitotic rate. SCLC and LCNEC overlap in their clinical, biological, histopathologic, immunophenotypic, and genetic characteristics making separation difficult, and perhaps unimportant, in some patients. INTRODUCTION 1-4 A revised WHO classification of lung tumors was published in 1999 and again in 2004, building on the popular foundation provided in the 1981 version. Like its predecessors, the updated WHO classification scheme relies heavily on routine light microscopy for tumor classification. Immunohistochemical stains have been established as an important diagnostic adjunct for certain tumor types, particularly tumors with neuroendocrine differentiation. The current scheme does not specifically categorize neuroendocrine neoplasms together, separating carcinoid tumors (typical and atypical) from more conventional forms of carcinomas. Small cell carcinoma (SCLC) remains a distinct carcinoma category, while large cell neuroendocrine carcinomas (LCNEC) are a subset of the larger group of large cell carcinomas. This review focuses on the two high grade variants of neuroendocrine neoplasms and those features that separate SCLC from LCNEC. SMALL CELL CARCINOMA 5-29 Small cell lung cancer (SCLC) accounts for around 15% of all bronchogenic carcinomas, and is considered a high grade representative of the family of neuroendocrine lung tumors. Small cell carcinoma is strongly associated with cigarette smoking. Men are affected more commonly than women by a ratio of about 2:1, and most patients present in the 6 th or 7 th decade of life. Nearly all patients have advanced stage disease at presentation, and for that reason surgery is reserved for rare patients in whom tumor is
12 2 confined to the lung. In a review limited to patients who underwent some sort of surgical procedure, survival for stage I and II ( limited ) disease was 50% at two years, but only 14% at 5 years. The survival at 5 years was not significantly different from that seen in patients with extensive (stage III and IV) disease. Combination chemotherapy with or without radiation remains the mainstay of therapy in most patients. Small cell carcinoma is a highly malignant epithelial neoplasm composed of relatively small cells with distinctive round to oval nuclei characterized by a diffuse ("salt and pepper") chromatin pattern and inconspicuous nucleoli. Cell size is variable, however, and comprises a range that merges with that seen in non-small cell carcinomas. In addition, a minor population of larger cells with prominent but small nucleoli is common in surgical specimens and does not, by itself, exclude the diagnosis. The cells generally have only scant cytoplasm and are arranged in broad sheets which frequently show necrosis. Focal areas demonstrating various growth patterns associated with neuroendocrine neoplasia (i.e. nested/organoid, peripheral palisading, trabecular, rosettes) occur in a substantial number of sufficiently preserved tumors. Extensive crush artifact and basophilic staining of blood vessel walls (Azzopardi phenomenon) are characteristic but not pathognomonic of this tumor. Cytogenetic and molecular studies fail to demonstrate a single specific abnormality, although abnormalities in p53, bcl2/bax, cyclin D1, RB loss and LOH at 3p occur in a high percentage of both SCLC and large cell neuroendocrine carcinomas (see below). Three variants of SCLC were recognized by the 1981 WHO classification: 1) oat cell ("lymphocyte-like") carcinoma which corresponds to the classically described small cell carcinoma, 2) intermediate cell type which differs in that the cells tend to have more cytoplasm, are less regular in contour, and are often polygonal or fusiform, 3) combined small cell carcinoma in which definite small cell carcinoma is admixed with a clearly identifiable squamous cell, adenocarcinoma or large cell component. The Pathology Committee of the International Association for the Study of Lung Cancer (IASLC) proposed separating SCLC into, 1) SCLC (pure or classical type), 2) mixed small cell/large cell carcinoma, and 3) combined small cell/non-small cell (i.e. squamous cell or adeno-) carcinoma. Although SCLC can be distinguished from non-small cell carcinomas with a great deal of consistency by light microscopy, subclassification using previously proposed categories was subject to frequent interobserver disagreement. Furthermore, a number of studies demonstrated no significant clinical, therapeutic, or prognostic differences between subtypes. The revised WHO classification scheme includes only combined SCLCs as a distinct variant. Diagnosis of SCLC can be made with confidence and a high degree of interobserver agreement in greater than 90% of cases. In difficult cases the differential diagnosis includes other forms of intermediate and high grade neuroendocrine (i.e. atypical carcinoid tumors and large cell neuroendocrine carcinomas see below) and nonneuroendocrine (i.e. squamous cell, adeno-, and large cell) carcinomas. Immunostains for neuroendocrine-associated proteins (e.g. chromogranin, synaptophysin) are of limited value since a substantial subset of SCLCs lack immunohistochemical evidence of neuroendocrine differentiation, and a minor subset of non-small cell carcinomas are
13 3 positive. Keratin profiles can be helpful in selected cases. In the end, however, there is no single stain and no combination of stains that consistently and categorically allows separation of these entities, a differential diagnosis that still hinges primarily on a combination of cytologic and histologic findings. LARGE CELL NEUROENDOCRINE CARCINOMA Small cell carcinoma and atypical carcinoid tumors can usually be diagnosed on the basis of light microscopy alone. Immunohistochemical staining for neuropeptides (i.e. neuron specific enolase, chromogranin, synaptophysin, serotonin, bombesin) can be helpful in difficult cases but are not required for diagnosis. Application of these techniques to nonsmall cell carcinomas will reveal neuroendocrine differentiation in two additional groups of tumors -- so-called large cell neuroendocrine carcinomas (LCNEC) and non-small cell carcinomas with neuroendocrine differentiation. Large cell neuroendocrine carcinoma refers to a subset of high grade neuroendocrine tumors characterized by, 1) a "neuroendocrine" histological growth pattern (i.e. organoid, palisading, trabecular, rosette-like); 2) "large" polygonal cells with lower N:C ratio than SCLC, coarse vesicular chromatin, and conspicuous nucleoli; 3) high (> 10/2 mm 2 ) mitotic rate; 4) necrosis; 5) immunophenotypic and/or ultrastructural evidence of neuroendocrine differentiation. Historically tumors of this type were referred to by a variety of terms (e.g. atypical carcinoid tumors, intermediate variant of SCLC, large cell neuroendocrine tumor, and large cell carcinoma with neuroendocrine differentiation), indicating the difficulty in identifying these poorly differentiated carcinomas as a distinct nosological entity. Nonetheless, LCNECs appear to be highly aggressive bronchogenic carcinomas with a prognosis similar to that for SCLC. Rates of interobserver agreement for the diagnosis of LCNEC are low, a feature that sets it apart from SCLC. This likely reflects the considerable histologic and cytologic overlap between LCNEC and SCLC at one end of a spectrum, and overlap with other forms of non-small cell lung carcinoma at the other. Perhaps the most difficult criteria to apply is the presence of a neuroendocrine growth pattern, something that frequently resides within the eye of the beholder. Cytologic features by themselves do not reliably separate LCNEC from SCLC; several studies have shown substantial overlap in cell size. Immunohistochemical studies are of limited value in that certain proteins (e.g. CD117, bcl-2, PAX-5, CRMP5) are expressed more frequently in high grade rather than lower grade neuroendocrine lung tumors but do not consistently separate LCNEC from SCLC. While difficulty in separating LCNEC from SCLC may be the bad news, the good news is that large retrospective case series suggest that there may be limited value in making the distinction at all. A number of studies have shown survival rates for patients who undergo surgery for early stage LCNEC that are superimposable on those reported for rare patients with early stage SCLC treated surgically. The survival rates for both are lower than that observed in patients with other forms of early stage but high grade nonneuroendocrine lung carcinoma. Comparisons of patients with late stage disease also show a similar survival experience that is different from lower grade forms of neuroendocrine lung tumors but similar to that seen in other types of late stage nonneuroendocrine lung carcinoma.
14 4 Table: Summary of Neuroendocrine Lung Neoplasms typical carcinoid atypical carcinoid SCLC LCNEC Age (yrs) M:F 1:1 1:1 2:1 4:1 Smokers (%) 30-50% 60-70% >95% >95% Central 75% 60% >90% 40% Stage I II 90% 10% 60% 40% <10% 90% 45% 55%
15 5 REFERENCES 1. Asamura H, Kameya T, Matsuno Y, et al. Neuroendocrine neoplasms of the lung: a prognostic spectrum. Journal of Clinical Oncology 2006;24(1): Devesa SS, Bray F, Vizcaino AP, Parkin DM. International lung cancer trends by histologic type: male:female differences diminishing and adenocarcinoma rates rising. International Journal of Cancer 2005;117(2): Flieder DB. Neuroendocrine tumors of the lung: recent developments in histopathology. Current Opinion in Pulmonary Medicine 2002;8(4): Travis W, Brambilla E, Muller-Hermelink H, Harris C. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. Lyon, France: IARC Press; Badzio A, Kurowski K, Karnicka-Mlodkowska H, Jassem J. A retrospective comparative study of surgery followed by chemotherapy vs. non-surgical management in limited-disease small cell lung cancer. European Journal of Cardio-Thoracic Surgery 2004;26(1): Bepler G, Neumann K, Holle R, Havemann K, Kalbfleisch H. Clinical relevance of histologic subtyping in small cell lung cancer. Cancer 1989;64(1): Brock MV, Hooker CM, Syphard JE, et al. Surgical resection of limited disease small cell lung cancer in the new era of platinum chemotherapy: Its time has come. Journal of Thoracic & Cardiovascular Surgery 2005;129(1): Camps C, Sirera R, Bremnes RM, et al. Analysis of c-kit expression in small cell lung cancer: prevalence and prognostic implications. Lung Cancer 2006;52(3): Coe BP, Henderson LJ, Garnis C, et al. High-resolution chromosome arm 5p array CGH analysis of small cell lung carcinoma cell lines. Genes, Chromosomes & Cancer 2005;42(3): Fraire AE, Johnson EH, Yesner R, Zhang XB, Spjut HJ, Greenberg SD. Prognostic significance of histopathologic subtype and stage in small cell lung cancer. Human Pathology 1992;23(5): Gephardt GN, Grady KJ, Ahmad M, Tubbs RR, Mehta AC, Shepard KV. Peripheral small cell undifferentiated carcinoma of the lung. Clinicopathologic features of 17 cases. Cancer 1988;61(5): Giltnane JM, Murren JR, Rimm DL, King BL. AQUA and FISH analysis of HER-2/neu expression and amplification in a small cell lung carcinoma tissue microarray. Histopathology 2006;49(2): Gouyer V, Gazzeri S, Bolon I, Drevet C, Brambilla C, Brambilla E. Mechanism of retinoblastoma gene inactivation in the spectrum of neuroendocrine lung tumors. American Journal of Respiratory Cell & Molecular Biology 1998;18(2):
16 6 14. Henderson LJ, Coe BP, Lee EH, et al. Genomic and gene expression profiling of minute alterations of chromosome arm 1p in small-cell lung carcinoma cells. British Journal of Cancer 2005;92(8): Inoue M, Miyoshi S, Yasumitsu T, et al. Surgical results for small cell lung cancer based on the new TNM staging system. Thoracic Surgery Study Group of Osaka University, Osaka, Japan.[see comment]. Annals of Thoracic Surgery 2000;70(5): Lassen U, Hansen HH. Surgery in limited stage small cell lung cancer. Cancer Treatment Reviews 1999;25(2): Lopez-Martin A, Ballestin C, Garcia-Carbonero R, et al. Prognostic value of KIT expression in small cell lung cancer. Lung Cancer 2007;56(3): Nicholson SA, Beasley MB, Brambilla E, et al. Small cell lung carcinoma (SCLC): a clinicopathologic study of 100 cases with surgical specimens.[see comment]. American Journal of Surgical Pathology 2002;26(9): Olejniczak ET, Van Sant C, Anderson MG, et al. Integrative genomic analysis of small-cell lung carcinoma reveals correlates of sensitivity to bcl-2 antagonists and uncovers novel chromosomal gains. Molecular Cancer Research: MCR 2007;5(4): Przygodzki RM, Finkelstein SD, Langer JC, et al. Analysis of p53, K-ras-2, and C-raf-1 in pulmonary neuroendocrine tumors. Correlation with histological subtype and clinical outcome. American Journal of Pathology 1996;148(5): Sehested M, Hirsch FR, Osterlind K, Olsen JE. Morphologic variations of small cell lung cancer. A histopathologic study of pretreatment and posttreatment specimens in 104 patients. Cancer 1986;57(4): Shepherd FA, Crowley J, Van Houtte P, et al. The International Association for the Study of Lung Cancer lung cancer staging project: proposals regarding the clinical staging of small cell lung cancer in the forthcoming (seventh) edition of the tumor, node, metastasis classification for lung cancer. Journal of Thoracic Oncology: Official Publication of the International Association for the Study of Lung Cancer 2007;2(12): Sturm N, Rossi G, Lantuejoul S, et al. 34BetaE12 expression along the whole spectrum of neuroendocrine proliferations of the lung, from neuroendocrine cell hyperplasia to small cell carcinoma. Histopathology 2003;42(2): Szczesny TJ, Szczesna A, Shepherd FA, Ginsberg RJ. Surgical treatment of small cell lung cancer. Seminars in Oncology 2003;30(1): Taniwaki M, Daigo Y, Ishikawa N, et al. Gene expression profiles of small-cell lung cancers: molecular signatures of lung cancer. International Journal of Oncology 2006;29(3):
17 7 26. Twijnstra A, Thunnissen FB, Lassouw G, Volovics A, Ten Velde GP. The role of the histologic subclassification of tumor cells in patients with small cell carcinoma of the lung and central nervous system metastases. Cancer 1990;65(8): Vollmer RT, Birch R, Ogden L, Crissman JD. Subclassification of small cell cancer of the lung: the Southeastern Cancer Study Group experience. Human Pathology 1985;16(3): Vollmer RT, Ogden L, Crissman JD. Separation of small-cell from non-small-cell lung cancer. The Southeastern Cancer Study Group pathologists' experience. Archives of Pathology & Laboratory Medicine 1984;108(10): Zhang H, Liu J, Cagle PT, Allen TC, Laga AC, Zander DS. Distinction of pulmonary small cell carcinoma from poorly differentiated squamous cell carcinoma: an immunohistochemical approach. Modern Pathology 2005;18(1): Araki K, Ishii G, Yokose T, et al. Frequent overexpression of the c-kit protein in large cell neuroendocrine carcinoma of the lung. Lung Cancer 2003;40(2): Battafarano RJ, Fernandez FG, Ritter J, et al. Large cell neuroendocrine carcinoma: an aggressive form of non-small cell lung cancer. Journal of Thoracic & Cardiovascular Surgery 2005;130(1): Doddoli C, Barlesi F, Chetaille B, et al. Large cell neuroendocrine carcinoma of the lung: an aggressive disease potentially treatable with surgery. Annals of Thoracic Surgery 2004;77(4): Dresler CM, Ritter JH, Patterson GA, Ross E, Bailey MS, Wick MR. Clinical-pathologic analysis of 40 patients with large cell neuroendocrine carcinoma of the lung. Annals of Thoracic Surgery 1997;63(1): Fernandez FG, Battafarano RJ. Large-cell neuroendocrine carcinoma of the lung. Cancer Control 2006;13(4): Graziano SL, Mazid R, Newman N, et al. The use of neuroendocrine immunoperoxidase markers to predict chemotherapy response in patients with non-small-cell lung cancer. Journal of Clinical Oncology 1989;7(10): Gugger M, Burckhardt E, Kappeler A, Hirsiger H, Laissue JA, Mazzucchelli L. Quantitative expansion of structural genomic alterations in the spectrum of neuroendocrine lung carcinomas. Journal of Pathology 2002;196(4): Hammond ME, Sause WT. Large cell neuroendocrine tumors of the lung. Clinical significance and histopathologic definition. Cancer 1985;56(7): Hiroshima K, Iyoda A, Shibuya K, et al. Prognostic significance of neuroendocrine differentiation in adenocarcinoma of the lung. Annals of Thoracic Surgery 2002;73(6):
18 8 39. Igarashi T, Jiang SX, Kameya T, et al. Divergent cyclin B1 expression and Rb/p16/cyclin D1 pathway aberrations among pulmonary neuroendocrine tumors. Modern Pathology 2004;17(10): Iyoda A, Hiroshima K, Moriya Y, et al. Prognostic impact of large cell neuroendocrine histology in patients with pathologic stage Ia pulmonary non-small cell carcinoma. Journal of Thoracic & Cardiovascular Surgery 2006;132(2): Iyoda A, Hiroshima K, Moriya Y, et al. Prospective study of adjuvant chemotherapy for pulmonary large cell neuroendocrine carcinoma.[see comment]. Annals of Thoracic Surgery 2006;82(5): Iyoda A, Hiroshima K, Toyozaki T, Haga Y, Fujisawa T, Ohwada H. Clinical characterization of pulmonary large cell neuroendocrine carcinoma and large cell carcinoma with neuroendocrine morphology. Cancer 2001;91(11): Jiang SX, Kameya T, Shoji M, Dobashi Y, Shinada J, Yoshimura H. Large cell neuroendocrine carcinoma of the lung: a histologic and immunohistochemical study of 22 cases. American Journal of Surgical Pathology 1998;22(5): Kobayashi Y, Tokuchi Y, Hashimoto T, et al. Molecular markers for reinforcement of histological subclassification of neuroendocrine lung tumors. Cancer Science 2004;95(4): LaPoint RJ, Bourne PA, Wang HL, Xu H. Coexpression of c-kit and bcl-2 in small cell carcinoma and large cell neuroendocrine carcinoma of the lung. Applied Immunohistochemistry & Molecular Morphology 2007;15(4): Linnoila RI, Mulshine JL, Steinberg SM, et al. Neuroendocrine differentiation in endocrine and nonendocrine lung carcinomas. American Journal of Clinical Pathology 1988;90(6): Marchevsky AM, Gal AA, Shah S, Koss MN. Morphometry confirms the presence of considerable nuclear size overlap between "small cells" and "large cells" in high-grade pulmonary neuroendocrine neoplasms.[see comment]. American Journal of Clinical Pathology 2001;116(4): Mazieres J, Daste G, Molinier L, et al. Large cell neuroendocrine carcinoma of the lung: pathological study and clinical outcome of 18 resected cases. Lung Cancer 2002;37(3): Nitadori J, Ishii G, Tsuta K, et al. Immunohistochemical differential diagnosis between large cell neuroendocrine carcinoma and small cell carcinoma by tissue microarray analysis with a large antibody panel. American Journal of Clinical Pathology 2006;125(5): Okubo C, Minami Y, Tanaka R, et al. Analysis of differentially expressed genes in neuroendocrine carcinomas of the lung. Journal of Thoracic Oncology: Official Publication of the International Association for the Study of Lung Cancer 2006;1(8):780-6.
19 9 51. Paci M, Cavazza A, Annessi V, et al. Large cell neuroendocrine carcinoma of the lung: a 10- year clinicopathologic retrospective study. Annals of Thoracic Surgery 2004;77(4): Pelosi G, Pasini F, Sonzogni A, et al. Prognostic implications of neuroendocrine differentiation and hormone production in patients with Stage I nonsmall cell lung carcinoma. Cancer 2003;97(10): Rossi G, Cavazza A, Marchioni A, et al. Role of chemotherapy and the receptor tyrosine kinases KIT, PDGFRalpha, PDGFRbeta, and Met in large-cell neuroendocrine carcinoma of the lung. Journal of Clinical Oncology 2005;23(34): Schleusener JT, Tazelaar HD, Jung SH, et al. Neuroendocrine differentiation is an independent prognostic factor in chemotherapy-treated nonsmall cell lung carcinoma. Cancer 1996;77(7): Sundaresan V, Reeve JG, Stenning S, Stewart S, Bleehen NM. Neuroendocrine differentiation and clinical behaviour in non-small cell lung tumours. British Journal of Cancer 1991;64(2): Takei H, Asamura H, Maeshima A, et al. Large cell neuroendocrine carcinoma of the lung: a clinicopathologic study of eighty-seven cases.[see comment]. Journal of Thoracic & Cardiovascular Surgery 2002;124(2): Travis WD, Linnoila RI, Tsokos MG, et al. Neuroendocrine tumors of the lung with proposed criteria for large-cell neuroendocrine carcinoma. An ultrastructural, immunohistochemical, and flow cytometric study of 35 cases. American Journal of Surgical Pathology 1991;15(6): Veronesi G, Morandi U, Alloisio M, et al. Large cell neuroendocrine carcinoma of the lung: a retrospective analysis of 144 surgical cases. Lung Cancer 2006;53(1): Visscher DW, Zarbo RJ, Trojanowski JQ, Sakr W, Crissman JD. Neuroendocrine differentiation in poorly differentiated lung carcinomas: a light microscopic and immunohistologic study. Modern Pathology 1990;3(4): Vollmer RT. The effect of cell size on the pathologic diagnosis of small and large cell carcinomas of the lung. Cancer 1982;50(7): Wick MR, Berg LC, Hertz MI. Large cell carcinoma of the lung with neuroendocrine differentiation. A comparison with large cell "undifferentiated" pulmonary tumors. American Journal of Clinical Pathology 1992;97(6): Zacharias J, Nicholson AG, Ladas GP, Goldstraw P. Large cell neuroendocrine carcinoma and large cell carcinomas with neuroendocrine morphology of the lung: prognosis after complete resection and systematic nodal dissection. Annals of Thoracic Surgery 2003;75(2):
20 63. Meyronet D, Massoma P, Thivolet F, et al. Extensive expression of collapsin response mediator protein 5 (CRMP5) is a specific marker of high-grade lung neuroendocrine carcinoma. Am J Surg Pathol 2008;32(11):
21 Arthur Purdy Stout Society Large Cell Neuroendocrine vs Small Cell Carcinoma When, Whether and How to Make the Distinction March 8, 2009 Jeffrey L. Myers, M.D. A. James French Professor and Director, Anatomic Pathology University of Michigan, Ann Arbor, MI
22 Large Cell Neuroendocrine vs Objective Small Cell Carcinoma At the end of this talk attendees will understand, current criteria for separating large cell neuroendocrine from small cell carcinoma, and the clinical, biological, histologic and phenotypic overlap between the two
23 WHO Classification of Lung Tumors* Neuroendocrine Lung Neoplasms small cell carcinoma large cell carcinoma large cell neuroendocrine carcinoma carcinoid tumor typical carcinoid tumor atypical carcinoid tumor *Travis et al (editors). WHO Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARC Press, Lyon 2004.
24 Neuroendocrine Lung Tumors Comparison* Age (yrs( yrs) M:F Smokers (%) Central Stage I II typical carcinoid 45 1: % 75% 90% 10% atypical carcinoid 55 1: % 60% 60% 40% SCLC 62 2:1 >95% >90% <10% 90% LCNEC 63 4:1 >95% 40% 45% 55% *modified after Flieder. Curr Opin Pulm Med 2002; 8:
 central >> peripheral")
25 SMALL CELL CARCINOMA General cigarette smoking ~ 15% of incident cases men women (~1-2:1) central >> peripheral
26 SMALL CELL CARCINOMA small cell ca rates in US in men in white women in black women (since 1990) from Devesa Int J Cancer 2005; 117: 294
27 SMALL CELL CARCINOMA Survival* cstage I II III IV % of pts 7% 4% 32% 57% survival 1 year 5 years 41% 28% 73% 21% 54% 11% 22% 1% *from Shepherd et al. J Thorac Oncol 2007

28 SMALL CELL CARCINOMA WHO Definition malignant epithelial tumor consisting of, small cells with scant cytoplasm, ill-defined cell borders usually less than the size of three small resting lymphocytes

29 WHO size rule 3 x lymphocyte diameter
30 SMALL CELL CARCINOMA WHO Definition small cells with scant cytoplasm, illdefined cell borders
31 SMALL CELL CARCINOMA WHO Definition small cells with scant cytoplasm, illdefined cell borders finely granular nuclear chromatin, and absent or inconspicuous nucleoli

32 finely granular chromatin absent/inconspicuous nucleoli

33 In 29 cases, a varying percentage of cells demonstrated nucleoli that were conspicuous but small. Nicholson et al. AJSP 2002
34 SMALL CELL CARCINOMA WHO Definition small cells with scant cytoplasm, illdefined cell borders finely granular nuclear chromatin, and absent or inconspicuous nucleoli cells are round, oval and spindleshaped; prominent nuclear molding

35 round, oval and spindle-shaped

36 prominent nuclear molding

37 high mitotic count (>10/2 mm 2 )
38 SMALL CELL CARCINOMA WHO Definition small cells with scant cytoplasm, illdefined cell borders finely granular nuclear chromatin, and absent or inconspicuous nucleoli cells are round, oval and spindleshaped; prominent nuclear molding mitotic count is high (>10/2 mm 2 )
39 SMALL CELL CARCINOMA Histologic Variants WHO IASLC WHO (1981) (1988) ( ) oat cell small cell small cell intermediate cell mixed small/large cell combined combined combined small cell small cell small cell

40 SMALL CELL CARCINOMA Immunohistochemical Profile small cell ca squamous cell ca adca keratin dot-like, perinuclear staining pattern
41 SMALL CELL CARCINOMA Immunohistochemical Profile small cell ca squamous cell ca adca keratin CRG +/ /+ /+ SYN +/ /+ /+
42 NE Differentiation in Non-small Cell Lung Carcinomas Using TMAs* CRG SYN CD56 Sq cell ca 1 (0.4%) 10 (4.3%) 29 (12.4%) Adenoca 1 (0.4%) 23 (11.2%) 11 (5.1%) *Ionescu et al. Am J Surg Pathol 2007; 31: 26
43 NE Differentiation in Non-small Cell Lung Carcinomas CRG* SYN* CRG/SYN/ CD57 (leu 7) Sq cell ca 4% 28% 41% Adenoca 6% 25% 35% *Data collected from 10 peer reviewed publication, Schleusener et al. Cancer 1996; 77: 1284.
44 SMALL CELL CARCINOMA Immunohistochemical Profile small cell ca squamous cell ca adca keratin CRG +/ /+ /+ SYN +/ /+ /+ 34βE12 + p63 + TTF-1 +



")



45 combined small cell + squamous cell ca TTF-1 p63 34βE12 (ker903)
46 SMALL CELL CARCINOMA Immunohistochemical Profile small cell ca squamous cell ca adca keratin CRG +/ /+ /+ SYN +/ /+ /+ 34βE12 + p63 + TTF-1 + +
47 Large Cell Carcinoma WHO 2004 poorly differentiated NSCLC that lacks cytologic and architectural features of SCLC and glandular or squamous differentiation 5 variants: large cell neuroendocrine basaloid carcinoma lymphoepithelioma-like carcinoma clear cell carcinoma large cell ca with rhabdoid phenotype
48 Large Cell Neuroendocrine Carcinoma Definition neuroendocrine morphology necrosis (extensive)




49

50
51 Large Cell Neuroendocrine Carcinoma Definition neuroendocrine morphology necrosis (extensive) >10 mitosis/2 mm 2 (10 hpf) cytologic features of NSCLC: large size, low N:C, nucleoli, coarse chromatin
52 large cell neuroendocrine carcinoma vs. atypical carcinoid tumor
53 ATYPICAL CARCINOID TUMOR Definition* neuroendocrine growth pattern uniform cytology ± atypia 2-10 mits/2 mm 2 ± necrosis *Travis et al (editors). WHO Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARC Press, Lyon 2004.
54 Large Cell Neuroendocrine Carcinoma Comparison with Atypical Carcinoid Asamura et al. J Clin Oncol 2006; 24: 70-6 NE morphology necrosis atypia mitotic rate atypical carcinoid 2-10/2 mm 2 LCNEC >10/2 mm 2
 of 106 cases had < 2 mits/2 mm 2 Beasley et al Hum")


55 ATYPICAL CARCINOID TUMOR Definition* 9 (8.5%) of 106 cases had < 2 mits/2 mm 2 Beasley et al Hum Pathol 2000; 31: 1255 neuroendocrine growth pattern uniform cytology ± atypia 2-10 mits/2 mm 2 *Travis et al (editors). WHO Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARC Press, Lyon 2004.



56 ATYPICAL CARCINOID TUMOR Definition* 71 (67%) of 106 cases had necrosis Beasley et al Hum Pathol 2000; 31: 1255 neuroendocrine growth pattern uniform cytology ± atypia 2-10 mits/2 mm 2 ± necrosis *Travis et al (editors). WHO Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARC Press, Lyon 2004.
57 Large Cell Neuroendocrine Carcinoma Comparison with Atypical Carcinoid atypical carcinoid LCNEC 10 mits/2 mm 2
58 Large Cell Neuroendocrine Carcinoma Definition neuroendocrine morphology necrosis (extensive) >10 mitosis/2 mm 2 (10 hpf) cytologic features of NSCLC: large size, low N:C, nucleoli, coarse chromatin immunohistochemical confirmation

59 Chromogranin
60 Large Cell Neuroendocrine Carcinoma Definition neuroendocrine morphology necrosis (extensive) >10 mitosis/2 mm 2 (10 hpf) LCNEC vs other NSCLC cytologic features of NSCLC: large size, low N:C, nucleoli, coarse chromatin LCNEC vs SCLC immunohistochemical confirmation
61 Large Cell Neuroendocrine Carcinoma Definition Is cell size a reliable criterion for separating large cell neuroendocrine carcinoma from small cell carcinoma?
62 n = 12 LCNEC and 16 SCLC measured tumor cell (TC) and lymphocyte (L) nuclear areas histograms for each peak TC/L: A = B = 3 C = 4 D = E = 6 F no peak Marchevsky et al. Am J Clin Pathol 2001; 116: 466. SCLC vs LCNEC Nuclear Size Overlap* 0 e.g. type A (peak TC/L = 2)
63 SCLC vs LCNEC Nuclear Size Overlap* small 5 (31%) of 16 SCLC had predominant population SCLC of cells 4-6 times larger LCNEC than lymphocytes 4 3 large 2 * * 1 * 0 TC/L = 2 (Type A) TC/L = 3 (Type B) TC/L = 4 (Type C) TC/L = 5 (Type D) TC/L = 6 (Type E) no peak (Type F) Marchevsky et al. Am J Clin Pathol 2001; 116: 466.
 overlaps with LCNEC (3.22 ± 0.86) *Hiroshima et al. Mod Pathol 2006; 19: 1358")
64 LCNEC SCLC vs LCNEC Nuclear Size Overlap* SCLC The frequency distribution of tumor nuclear diameter/ lymphocyte size ratios in SCLC (2.75 ± 0.86) overlaps with LCNEC (3.22 ± 0.86) *Hiroshima et al. Mod Pathol 2006; 19: 1358
65 Large Cell Neuroendocrine Carcinoma Definition Is cell size a reliable criterion for separating large cell neuroendocrine carcinoma from small cell carcinoma? NO!
66 Large Cell Neuroendocrine Carcinoma Definition Is immunohistochemistry useful for separating large cell neuroendocrine carcinoma from small cell carcinoma?
67 SCLC vs LCNEC Role of Immunohistochemistry* 100% 80% SCLC LCNEC p.0018 p.0422 p % p.0022 p % 20% 0% CRG SYN CD56 mash1 NeuroD TTF p63 p16 PTEN *Hiroshima et al. Mod Pathol 2006; 19: 1358
68 SCLC vs LCNEC Role of Immunohistochemistry* 100% 50% c-kit pos bcl-2 pos c-kit/bcl-2 pos c-kit/bcl-2 expression in SCLC & LCNEC 0% typical carcinoid (16) atypical carcinoid (6) small cell ca (7) LCNEC (14) *LaPoint et al. Appl IHC Mol Morphol 2007; 15: 401-6
69 SCLC vs LCNEC Role of Immunohistochemistry* 90% 60% 30% Diffuse (> 10%) 2-3+ intensity PAX-5 expression in SCLC & LCNEC 0% typical carcinoid (44) atypical carcinoid (7) small cell ca (26) LCNEC (3) *Sica et al. Am J Clin Pathol 2008; 129:
70 Large Cell Neuroendocrine Carcinoma Conclusion Neither cell size nor immunohistochemistry are useful for separating large cell neuroendocrine carcinoma from small cell carcinoma?
71 NEUROENDOCRINE LUNG TUMORS Diagnostic Reproducibility* Unanimous Majority (5 of 5) (4 of 5) typical carcinoid 58% 92% atypical carcinoid 50% 75% SCLC 70% 90% LCNEC 40% 50% *Travis et al. Hum Pathol 1998; 29: 272
72 Does separating LCNEC from SCLC have value? If so, when?
73 LCNEC versus SCLC? Survival P =.9147 Asamura, 2006 J Clin Oncol 24: 70-6
74 Impact of LCNEC Histology on Survival in Early Stage Disease? Large cell neuroendocrine histology has a significant adverse prognostic impact on pathologic stage Ia non-small cell carcinoma. Iyoda 2006
75 Takei 2002 LCNEC versus SCLC? Survival in Stage I Disease P =.1851 Asamura 2006
76 Fig 5. Kaplan-Meier curves for overall survival stratified according to chemotherapeutic protocols in the adjuvant setting and tumor stage Rossi, G. et al. J Clin Oncol; 23: SCLC-based = platinum-etoposide LCNEC is more likely to respond to chemotherapeutic strategies targeting SCLC Copyright American Society of Clinical Oncology
77 SCLC vs LCNEC Summary of cytological criteria for LCNEC, only the presence of cytoplasm is useful no consistent difference at level of protein expression low rates of interobserver agreement among experts no difference in therapeutic response or natural history
78 SCLC vs LCNEC Summary of cytological criteria for LCNEC, only the presence of cytoplasm is useful no consistent difference at level of protein expression low rates of interobserver agreement among experts no difference in therapeutic response or natural history
79 SCLC vs LCNEC Summary of cytological criteria for LCNEC, only the presence of cytoplasm is useful no consistent difference at level of protein expression low rates of interobserver agreement among experts no difference in therapeutic response or natural history
80 SCLC vs LCNEC Summary of cytological criteria for LCNEC, only the presence of cytoplasm is useful no consistent difference at level of protein expression low rates of interobserver agreement among experts no difference in therapeutic response or natural history
81 Large Cell Neuroendocrine Carcinoma Practical Approach? LCNEC? any way to make this SCLC? finely dispersed chromatin? inconspicuous nucleoli? scant cytoplasm? is cell size the only issue? clinical context? central mass in smoker with mediastinal adenopathy?
82 Large Cell Neuroendocrine Carcinoma Practical Approach? any way to make this SCLC? YES! SCLC
83 Large Cell Neuroendocrine Carcinoma Practical Approach? any way to make this SCLC? NO compelling reason to acknowledge neuroendocrine differentiation? LCNEC already diagnosed IHC stains and it really, really looks neuroendocrine but atypical carcinoid been called SCLC but it isn t
84 Large Cell Neuroendocrine Carcinoma Practical Approach? LCNEC any way to make this SCLC? NO compelling reason to acknowledge neuroendocrine differentiation? YES!



85 Large Cell Neuroendocrine Carcinoma Practical Approach? LCC, sq cell ca, adca any way to make this SCLC? NO NO compelling reason to acknowledge neuroendocrine differentiation?
86 SCLC vs LCNEC Key Points SCLC is defined on the basis of cytologic criteria LCNEC is defined by a combination of histologic and cytologic criteria + proof of NE differentiation (immunohistochemistry) LCNEC is separated from atypical carcinoid based on consistent presence of necrosis and higher mitotic rate SCLC and LCNEC overlap in clinical, biological, histopathologic, immunophenotypic and genetic characteristics
87 1 Triple negative and basal-like breast cancer: one or many diseases? Implications for surgical pathologists Jorge S Reis-Filho, MD PhD FRCPath The Breakthrough Breast Cancer Research Centre Institute of Cancer Research London, SW3 6JB, UK Jorge.Reis-Filho@icr.ac.uk Take home messages - The majority of basal-like breast cancers have a triple negative phenotype and the vast majority of triple negative cancers display a basal-like transcriptome, however the two are not synonymous. - Basal-like and triple negative breast cancers comprise a heterogeneous group of diseases, which are characterised by a constellation of morphological features. - Not all basal-like and triple negative breast cancers have a poor outcome. - The precursors of invasive breast carcinomas of basal-like and triple negative phenotype include ductal carcinoma in situ harbouring a similar phenotype and, possibly, a subgroup of microglandular adenosis. - A subgroup of basal-like and triple negative breast cancers displays an exquisite sensitivity to anthracycline-based neoadjuvant chemotherapy. - Defects in the p53, prb and p16 pathways are found in a significant proportion of basal-like and triple negative cancers. - BRCA1 pathway dysfunction is found in a substantial proportion of basal-like and triple negative breast cancers and can be exploited therapeutically (e.g. inhibitors of the PARP enzyme and cross-linking agents) Introduction Breast cancer is a heterogeneous disease, encompassing a plethora of entities which not only have distinct morphological features but also clinical behaviour. In recent years, it has become apparent that this diversity may be underpinned by distinct patterns of genetic, epigenetic and transcriptomic aberrations 1-4. In fact, the marriage of pathology and genetics has led to the establishment of clear examples of genotypic-phenotypic correlations. For instance, secretory carcinomas of the breast consistently harbour a t(12;15)(p13;q25) translocation, leading to the formation of a fusion transcript ETV6-NTRK3 1,5-8. Lobular carcinomas have been shown to be characterised by inactivation of the CDH1 gene, which encodes E-cadherin, a transmembrane adhesion molecule that mediates homophilichomotypic adhesions. A recent conditional mouse model has provided strong circumstantial
88 2 evidence to suggest that CDH1 gene inactivation is not only involved in the characteristic discohesiveness of lobular lesions, but may be also involved in the peculiar metastatic pattern of invasive lobular carcinomas 9. Although morphology is often associated with the pattern of molecular aberrations in breast cancers, it is also clear that tumours of the same histological type display remarkably different clinical behaviour. This is most evident in invasive ductal carcinomas of no special type (IDC-NST), where even tumours of the same histological grade may have distinct outcome and remarkably different responses to systemic therapy 2,3. With the boom of high throughput technologies and the apocalyptic promise of microarray analysis, several groups endeavoured in devising a new taxonomy solely based on the molecular features of breast cancers. The gene expression microarray-based class discovery studies pioneered by the Stanford group have led to the identification of at least five subgroups of breast cancer: luminal A, luminal B, normal breast-like, HER2 and basal-like breast cancer This taxonomy was devised based on the analysis of IDC-NSTs and a limited number of lobular carcinomas and has proven to be of prognostic significance. Although based on the analysis of a rather limited number of samples and with varying definitions in each study, this classification has captured the attention of oncologists, pathologists and scientists alike, with some authorities in the field claiming that the gold standard for the classification of breast cancers is microarray-based gene expression profiling. It should be noted, however, that this taxonomy identified subgroups of breast cancer that were to some extent already known. In fact, the most robust distinction observed by microarray analysis is between the transcriptome of oestrogen receptor (ER)-positive and ER-negative breast cancers. Luminal tumours are described as those that show expression patterns reminiscent of normal luminal epithelial cells of the mammary gland, including consistent expression of low molecular weight cytokeratins 8/18, ER and genes associated with an active ER pathway 11,12,15,16. At least two subgroups of luminal tumours have been identified: luminal A, which are usually of low histological grade, have an excellent prognosis and show high levels of expression of ER-activated genes; and luminal B, which are more often of higher histological grade, have higher proliferation rates and a significantly worse prognosis than luminal A tumours 11,12, Normal breast-like cancers are rather poorly characterised; one of the defining features of these tumours is that they consistently cluster together with samples of fibroadenomas and normal breast. The clinical significance of normal breast-like tumours is yet to be determined 11,12,14-16 and some have suggested that this subgroup may be a mere artefact of expression profiling (i. e. disproportionally high content of stromal cells). HER2 tumours are usually ER-negative and characterised by
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Pathology of the Prostate. PathoBasic Tatjana Vlajnic
 Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
Pathology of the Prostate PathoBasic 24.01.17 Tatjana Vlajnic Overview Adenocarcinoma of the prostate Grading Special variants Mimickers of prostate adenocarcinoma Atrophy Inflammatory conditions Granulomatous
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Neuroendocrine neoplasms of the lung
 Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Neuroendocrine (NE) lung tumors represent a broad
 lung tumors represent a broad") Large Cell Neuroendocrine Carcinoma of the Lung: A 10-Year Clinicopathologic Retrospective Study Massimiliano Paci, MD, Alberto Cavazza, MD, Valerio Annessi, MD, Innocenza Putrino, MD, Guglielmo Ferrari,
Large Cell Neuroendocrine Carcinoma of the Lung: A 10-Year Clinicopathologic Retrospective Study Massimiliano Paci, MD, Alberto Cavazza, MD, Valerio Annessi, MD, Innocenza Putrino, MD, Guglielmo Ferrari,
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE. Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT
 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE Peter A. Humphrey, MD, PhD Yale University School of Medicine New Haven, CT 2016 WHO CLASSIFICATION OF TUMOURS OF THE PROSTATE AUTHORS : PROSTATE CHAPTER
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability. Michael den Bakker Erasmus MC
 Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
Small cell lung cancer and large cell neuroendocrine tumours interobserver variability Michael den Bakker Erasmus MC PPC London 2007 WEB presentation Pulmonary pathology Club presentation, London, November
5/21/2018. Difficulty in Underdiagnosing Prostate Cancer. Diagnosis of Prostate Cancer. Evaluation of Prostate Cancer and Atypical on Needle Biopsy
 Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
Evaluation of Prostate Cancer and Atypical on Needle Biopsy Jonathan I. Epstein Difficulty in Underdiagnosing Prostate Cancer Limited tissue on needle biopsy (1 cm. x
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Prostatic ductal adenocarcinoma is a subtype of
 ORIGINAL ARTICLE High-grade Prostatic Intraepithelial Neoplasialike Ductal Adenocarcinoma of the Prostate: A Clinicopathologic Study of 28 Cases Fabio Tavora, MD* and Jonathan I. Epstein, MD*w z Abstract:
ORIGINAL ARTICLE High-grade Prostatic Intraepithelial Neoplasialike Ductal Adenocarcinoma of the Prostate: A Clinicopathologic Study of 28 Cases Fabio Tavora, MD* and Jonathan I. Epstein, MD*w z Abstract:
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Although current American Cancer Society guidelines
 ORIGINAL ARTICLE Diffuse Adenosis of the Peripheral Zone in Prostate Needle Biopsy and Prostatectomy Specimens Tamara L. Lotan, MD* and Jonathan I. Epstein, MD*w z Abstract: We have observed a group of
ORIGINAL ARTICLE Diffuse Adenosis of the Peripheral Zone in Prostate Needle Biopsy and Prostatectomy Specimens Tamara L. Lotan, MD* and Jonathan I. Epstein, MD*w z Abstract: We have observed a group of
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung
 Case Reports Jpn J Clin Oncol 2011;41(6)797 802 doi:10.1093/jjco/hyr034 Advance Access Publication 16 March 2011 Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung Taichiro
Case Reports Jpn J Clin Oncol 2011;41(6)797 802 doi:10.1093/jjco/hyr034 Advance Access Publication 16 March 2011 Combined Large Cell Neuroendocrine Carcinoma and Spindle Cell Carcinoma of the Lung Taichiro
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens
 is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens") Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Large cell neuroendocrine carcinoma: retrospective analysis of 24 cases from four oncology centers in Turkey
 Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Large cell neuroendocrine carcinoma: retrospective analysis of 24 cases from four oncology centers in Turkey Bala Başak Oven Ustaalioglu 1, Arife Ulas 2,
Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Large cell neuroendocrine carcinoma: retrospective analysis of 24 cases from four oncology centers in Turkey Bala Başak Oven Ustaalioglu 1, Arife Ulas 2,
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Although partial atrophy is one of the most common
 ORIGINAL ARTICLE Partial Atrophy on Prostate Needle Biopsy Cores: A Morphologic and Immunohistochemical Study Wenle Wang, MD, PhD,* Xinlai Sun, MD,w and Jonathan I. Epstein, MD*zy Abstract: Partial atrophy
ORIGINAL ARTICLE Partial Atrophy on Prostate Needle Biopsy Cores: A Morphologic and Immunohistochemical Study Wenle Wang, MD, PhD,* Xinlai Sun, MD,w and Jonathan I. Epstein, MD*zy Abstract: Partial atrophy
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Large-Cell Neuroendocrine Carcinoma of the Lung
 Accurate classification of this malignancy will help to guide management decisions regarding resection and adjuvant therapy. Manus Island Tree Snail_2281. Photograph courtesy of Henry Domke, MD. www.henrydomke.com.
Accurate classification of this malignancy will help to guide management decisions regarding resection and adjuvant therapy. Manus Island Tree Snail_2281. Photograph courtesy of Henry Domke, MD. www.henrydomke.com.
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Molecular classification of breast cancer implications for pathologists. Sarah E Pinder
 Molecular classification of breast cancer implications for pathologists Sarah E Pinder Courtesy of CW Elston Histological types Breast Cancer Special Types 17 morphological special types 25-30% of all
Molecular classification of breast cancer implications for pathologists Sarah E Pinder Courtesy of CW Elston Histological types Breast Cancer Special Types 17 morphological special types 25-30% of all
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA
 Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA Learners Objectives u Latest changes per ISUP 2014 that impact
Gleason Scoring System 2017 JASREMAN DHILLON, MD ASSOCIATE PROFESSOR, DEPARTMENT OF ANATOMIC PATHOLOGY, MOFFITT CANCER CENTER, TAMPA, FLORIDA Learners Objectives u Latest changes per ISUP 2014 that impact
Prostate Immunohistochemistry. Literature Interpretation: Caveats. Must be aware of staining pattern of antibody in the relevant tissue
 IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT
 Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT during follow- up. ALT, AST, Alk Phos and bilirubin were
Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT during follow- up. ALT, AST, Alk Phos and bilirubin were
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Case 1. ACCME/Disclosure. Clinical History. Dr. Mulligan has nothing to disclose
 Breast Evening Specialty Conference USCAP, 2016 Case 1 Anna Marie Mulligan University Health Network, Toronto University of Toronto ACCME/Disclosure Dr. Mulligan has nothing to disclose Clinical History
Breast Evening Specialty Conference USCAP, 2016 Case 1 Anna Marie Mulligan University Health Network, Toronto University of Toronto ACCME/Disclosure Dr. Mulligan has nothing to disclose Clinical History
Epithelial Columnar Breast Lesions: Histopathology and Molecular Markers
 29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
University Journal of Pre and Para Clinical Sciences
 ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
Tumors of the Lungs and Pleura
 5 Tumors of the Lungs and Pleura Saul Suster and Cesar Moran Introduction Carcinoma of the lung is a common malignant tumor. Histological typing of lung tumors has long been a source of controversy in
5 Tumors of the Lungs and Pleura Saul Suster and Cesar Moran Introduction Carcinoma of the lung is a common malignant tumor. Histological typing of lung tumors has long been a source of controversy in
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
1 NORMAL HISTOLOGY AND METAPLASIAS
 1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly
 Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly Melinda F. Lerwill, MD CRITERIA FOR DISTINGUISHING LOW-GRADE DUCTAL CARCINOMA IN SITU FROM USUAL DUCTAL HYPERPLASIA CYTOLOGY Low-grade
Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly Melinda F. Lerwill, MD CRITERIA FOR DISTINGUISHING LOW-GRADE DUCTAL CARCINOMA IN SITU FROM USUAL DUCTAL HYPERPLASIA CYTOLOGY Low-grade
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Basaloid Carcinoma of the Lung: A Really Dismal Histologic Variant?
 Carcinoma of the Lung: A Really Dismal Histologic Variant? Dae Joon Kim, MD, Kil Dong Kim, MD, Dong Hwan Shin, MD, Jae Y Ro, MD, and Kyung Young Chung, MD Departments of Thoracic and Cardiovascular Surgery,
Carcinoma of the Lung: A Really Dismal Histologic Variant? Dae Joon Kim, MD, Kil Dong Kim, MD, Dong Hwan Shin, MD, Jae Y Ro, MD, and Kyung Young Chung, MD Departments of Thoracic and Cardiovascular Surgery,
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Non-Small Cell Lung Carcinoma - Myers
 Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
MOLECULAR AND CLINICAL ONCOLOGY 1: , 2013
 MOLECULAR AND CLINICAL ONCOLOGY 1: 437-443, 2013 Clinicopathological features and the impact of the new TNM classification of malignant tumors in patients with pulmonary large cell neuroendocrine carcinoma
MOLECULAR AND CLINICAL ONCOLOGY 1: 437-443, 2013 Clinicopathological features and the impact of the new TNM classification of malignant tumors in patients with pulmonary large cell neuroendocrine carcinoma
USCAP 2012: Companion Meeting of the AAOOP. Update on lacrimal gland neoplasms: Molecular pathology of interest
 USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology
 XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
Grading Prostate Cancer: Recent Changes and Refinements
 USPSTF: 2012 Report on serum PSA Screening Recommendation rating of D Reduced screening, Reduced biopsies, reduced incidence Refinements currently occurring in 2017. WHY? Grading Prostate Cancer: Recent
USPSTF: 2012 Report on serum PSA Screening Recommendation rating of D Reduced screening, Reduced biopsies, reduced incidence Refinements currently occurring in 2017. WHY? Grading Prostate Cancer: Recent
Uropathology January Jon Oxley
 Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
ROLE OF PROSTATIC BASAL CELL MARKER IN DIAGNOSIS OF PROSTATIC LESIONS
 Original Research Article Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 ROLE OF PROSTATIC BASAL CELL MARKER IN DIAGNOSIS OF PROSTATIC LESIONS SUBATHRA K* Department of pathology,
Original Research Article Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 ROLE OF PROSTATIC BASAL CELL MARKER IN DIAGNOSIS OF PROSTATIC LESIONS SUBATHRA K* Department of pathology,
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
What s New in Pathology of Genitourinary Tumors. Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine
 What s New in Pathology of Genitourinary Tumors Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine Kidney Tumors Multilocular cystic renal neoplasm of low malignant potential
What s New in Pathology of Genitourinary Tumors Jiaoti Huang, MD, PhD Department of Pathology Duke University School of Medicine Kidney Tumors Multilocular cystic renal neoplasm of low malignant potential
Mammary analogue secretory carcinoma of salivary gland A case report of new entity
 Case Report Mammary analogue secretory carcinoma of salivary gland A case report of new entity Vaibhav Bhika Bari 1*, Sandhya Unmesh Bholay 2 1 Assistant Professor, 2 Associate Professor Rajiv Gandhi Medical
Case Report Mammary analogue secretory carcinoma of salivary gland A case report of new entity Vaibhav Bhika Bari 1*, Sandhya Unmesh Bholay 2 1 Assistant Professor, 2 Associate Professor Rajiv Gandhi Medical
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Columnar Cell Lesions
 Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA
 + NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA + INTRODUCTION + NEUROENDOCRINE FEATURES IN BREAST CARCINOMA Incidence of 2-5% Seen in various histopathological types of breast carcinoma Seen in both
+ NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA + INTRODUCTION + NEUROENDOCRINE FEATURES IN BREAST CARCINOMA Incidence of 2-5% Seen in various histopathological types of breast carcinoma Seen in both
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Diagnosis, pathology and prognosis including variant pathology
 PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
Synchronous squamous cell carcinoma of the breast. and invasive lobular carcinoma
 Sentani K et al. 1 Letter to the editor Synchronous squamous cell carcinoma of the breast and invasive lobular carcinoma Kazuhiro Sentani, 1 Takashi Tashiro, 2 Naohide Oue, 1 Wataru Yasui 1 1 Department
Sentani K et al. 1 Letter to the editor Synchronous squamous cell carcinoma of the breast and invasive lobular carcinoma Kazuhiro Sentani, 1 Takashi Tashiro, 2 Naohide Oue, 1 Wataru Yasui 1 1 Department
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory