Application of endoscopic CO2 laser surgery for early malignant tumours of the larynx
|
|
|
- Sharon Black
- 5 years ago
- Views:
Transcription

1 Lasers in Medicine and Life Sciences Summer School (LAMELIS) Principles and practice of laser surgery Application of endoscopic CO2 laser surgery for early malignant tumours of the larynx Miklós Csanády MD. PhD. associate professor Department of Otorhinolaryngology, Head and Neck Surgery, University of Szeged LAMELIS 2016, Szeged, Hungary


2 LASER - Light Amplification by Stimulated Emission of Radiation Low energy laser: soft laser High energy laser Cut, coagulation laser Impuls, continuous mode Laser
3 Human application of lasers Gas lasers: CO μm larynx, pharynx, trachea, nose, ear, He-Neon (soft laser), Ion lasers: Argon nm, Krypton nm - dermatology Diode laser : 808 nm Dye laser: different wavelength Excimer laser: - ear Neodym YAG: 1064nm, Neodym doped - Yttrium- Aluminium-Granat-Laser, fiberoptic trachea, brochi Combi laser: Nd:YAG+CO2 pharynx trachea, brochi KTP laser: 532 nm - Potassium Titanyl Phosphate nose


4 Specification of CO2 laser CO2 laser - wavelength: 10.6 μm Cutting laser, up to 0.5 mm diameter of vessel coagulation High energy, W mm spot burning tissue Straight spread of laser beam (flexible optic also available) Coupled with microscope easy and exact manipulation
5 CO2 laser applications for transoral surgery of the larynx: - Benign lesions - Early malignant tumours of the larynx

")
 Subglottic tumours")
6 Tumours of the larynx: Localization, distribution and prognosis Glottic tumours vocal fold (about 48%) Supraglottic tumours (about 50%) Subglottic tumours (1-2%) p r o g n o s i s
7 Carcinoma of the larynx Cancers of the larynx account for the majority of head and neck cancers; however, head and neck cancers account for only about 9% of all cancers diagnosed annually. In the United States, there are more cancers affecting the glottic larynx than the supraglottic larynx. Conversely, in Europe and many other parts of the world, supraglottic cancers outnumber glottic cancers. Cancers of the glottic larynx are more likely to be detected early because even small lesions produce voice changes readily noticeable by the patient and his/her family members; however, patients with smoking-related chronic laryngitis who are used to a chronically hoarse voice may not detect voice changes produced by an early cancer at this location. The supraglottis tends to be a more silent location because tumors here do not affect the voice until they are significantly more advanced. Patients with tumors in this area may present with a sore throat, pain on swallowing (odynophagia), or ear pain (otalgia).
8 Carcinoma of the larynx Carcinoma planocellulare laryngis Prevalence of the laryngeal tumour: most frequent of the malignancies in adults. Predisposition: Inherited genetic conditions (inherited, aquired, DNA mutation) Incidence in countries (continents) Habits: smoking - tobacco use (abuse)!!, alcohol consumption (lesion of the liver), chemicals, feeding, hygiene of the mouth Profession, pollution. Appearence: age of years, Men-women ratio: 20:1 (USA: 5:1)
9 Pathogenesis Invasive carcinoma may develop from dysplasia and transforms to cancer (in situ) Precancerosis: Keratosis without atypia, Keratosis with atypia (I-III.), Cc. in situ Dysplasia I.- dysplasia II.- dyplasia III = in situ carcinoma More than 92% of laryngeal carcinoma: established as a squamous cell carcinoma Minority of the layngeal malignant epithelial tumours: verrucous carcinoma, adenocarcinoma, basal cell carcinoma, carcinosarcoma Sarcoma is extremly rare: fibro-, myo-, chondrosarcoma, rhabdomyosarcoma
10 Prognosis of the laryngeal cancer depends on: Localization (supraglottic, glottic, subglottic site) Staging, TNM classification Differentiation of the tumour Metastasis formation
11 TNM classification Laryngeal cancers are staged and classified according to the TNM system as explained in the latest manual of the ICD-O (International Classification of Diseases for Oncology) WHO, TNM Classification for Malignant Tumours UICC and American Joint Commission on Cancer. There is a separate staging system for cancers that affect different subdivisions of the larynx. Subglottic cancer is quite rare and so we focus on cancers affecting the glottic and supraglottic larynx. Clinical evaluation: ctnm, pathological finding: ptnm Hungarian issue for laryngeal tumour classification: A gége- és hypopharynx-laphámrák osztályozása, kivizsgálása és kezelési javaslata Magyar Onkológia, 46, 4, , 2002
12 Laryngeal Cancer T staging T1, T2 tumours: transoral laser surgery Glottic Cancers T1a: Tumour is confined to one vocal cord with normal mobility T1b: Tumour involves both vocal cords but mobility is normal T2: Extension of the tumour from the vocal cords to the supraglottic or subglottic larynx or impaired vocal cord mobility T3: Tumour is confined to the larynx but there is fixation of the vocal cord T4: There is invasion through thyroid cartilage and/ or other tissues beyond larynx (e.g., trachea, thyroid, pharynx, soft tissue of neck).
13 Laryngeal Cancer T staging T1, T2 tumours: transoral laser Supraglottic Cancers T1: Tumour is confined to one subsite of the supraglottic larynx and there is normal vocal cord mobility T2: Tumour invades mucosa of more than one adjacent subsite of supraglottis but vocal cord mobility remains normal T3: Tumour is limited to the larynx with vocal cord fixation and/or extension to postcricoid area or preepiglottic tissues. T4: Tumour invades through thyroid cartilage, and/or extends into soft tissues of the neck, thyroid, and/or esophagus Staging of regional metastases (N) is as follows: N0: No evidence of regional metastases to cervical lymph nodes N1: Single neck node up to 3 cm in greatest dimension N2: Single node greater than 3 cm (but less than 6 cm), or multiple lymph nodes N3: Any node greater than 6 cm in greatest dimension
14 TNM Stage, application of transoral laser surgery The stage is assigned according to the following scheme: In general, the more advanced the overall stage the worse the prognosis. Prognosis is best for those who have no regional metastases (N0) and worst for those who have distant metastases (M1). Cancers of the supraglottic larynx and Morgagni sac are more likely to have regional neck metastases than are cancers of the glottic larynx. T1 N0 M0 Stage I - transoral laser surgery T2 N0 M0 Stage II - transoral laser surgery T1-2N1M0 Stage III - transoral laser surgery + neck management T3 N0 M0 Stage III T3 N1 M Stage III T4, N0-N1 M0 Stage IVA T1-4, N2 M0 Stage IVA T1-4, N3 M0 Stage IVB T1-4, N0-3, M1 Stage IVC
15 Diagnostic in laryngeal neck tumours Case history: personal, familiar, social questionaire, feeding Clinical examination: indirect - and direct laryngoscopy, endoscopy, palpation of the neck (metastasis) Pathology (primary tumour - biopsy, metastasis - fine needle aspiration) Imaging (CT, MRI, sonography of the neck, chest X-ray, sonography of the belly) Staging Research: Examination of DNA (PCR), gen chips Investigation of immun cells Tumour markers
16 Symptoms, clinical patterns Vocal cord cancer Supraglottic cancer Subglottic cancer hoarseness dysphagia referred pain in the ear - otalgia irradiata (supplied by n. vagus) dyspnoe hoarseness voice disorder dyspnoe
17 Diagnostic, evaluation, therapy: endoscopy of the larynx Indirect laryngoscopy Direct laryngoscopy: Rigid endoscopy - diagnostic Flexible endoscopy - diagniostic Laryngomicroscopy diagnostic and therapy Laryngostroboscopy - phonation Photodynamic endoscopy - oncology Contact endoscopy - oncology, etc.






18 Endoscopy of the larynx with 70º rigid optic and fiberoscopy visualizing the larynx fiberoscopy laryngoscopy Video-endoscopy: tumour of the vocal fold, outpatient



19 Direct laryngoscopy: laryngomicroscopy general anaethesia (ITN) or JET narcosis Application of microscope and rigid, long optic for the preop. diagnostic Laryngomicroscopy

20 Method Preoperative investigations: Endoscopy of the larynx, sonography and CT scan of the neck (MRI) Instruments: TLS 61 Tungsram laser, Lasram and later Daeshin DS 40UB laser surgical devices Opton, Leica microscopes Kleinsasser and Weerda laryngoscopes, Laryngomicroscopic instruments General anaesthesia (intratracheal narcosis)
21 Basic treatment options for eraly laryngeal carcinoma Surgery Radiation therapy Chemotherapy Combined treatments By Onco-Team board consultation, decision!
22 Treatment options of early malignancies of the larynx - Surgery Surgical interventions: transoral (endoscopic) versus open approach surgery/radiation therapy Goals to achieve: 1. Good oncological result 2. Functional results: preserving the laryngeal functions (vocal cord), acceptable voice, swallowing without feeding tube and tracheacanule 3. Aesthetic results: no tracheostomy, no scar on the neck (endoscopic surgery), 4. Cost-benefit relations
23 Endoscopic CO2 laser technique Introduction of transoral laser resection to the laryngology USA: Jako, Strong, Vaughan, Davis, Zeitels Europe: Steiner, Ambrosch, Rudert, Thumfart, Eckel, Werner, Motta, Bernard-Sperkelsen, etc. Hungary: Bánhídy, Kásler, Czigner, Élő, Lichtenberger, Répássy
 glottic carcinoma - laser cordectomy Csanády M., Czigner J., Sávay L.: Endolaryngeal CO2 laser microsurgery of early vocal cord cancer. A retrospective study.")
24 20 years experience with transoral CO2 laser surgery of laryngeal tumours at the University of Szeged Early glottic cancer: endoscopic CO2 laser surgery was introduced at our department in 1987 by professor Czigner -T1a, T1 b, (T2) glottic carcinoma - laser cordectomy Csanády M., Czigner J., Sávay L.: Endolaryngeal CO2 laser microsurgery of early vocal cord cancer. A retrospective study. In: Rudert H., Werner J.A. (eds.): Lasers in Otorhinolaryngology and in Head and Neck Surgery. Adv. Otorhinolaryngol, Karger, Basel, vol. 49, pp Supraglottic and marginal laryngeal tumours (T1, T2) Csanády M., Czigner J., Iván L.: Endoscopic CO2 laser therapy in selected cases of supraglottic tumors. Eur. Arch. Otorhinolaryngol. 1999, 256, Csanády M., Vass G, Czigner J., Jóri J.: Endoscopic CO2 laser management of selected supraglottic marginal tumors and neck dissection Eur. Arch. Otolaryngol

25 More than 20 years experience with CO2 laser surgery of the early glottic cancer (327 laser cordectomy) 375 laser cordectomy was performed (324 patients), in patients with Tis-T2 vocal cord cancer between 1987 and patients with a minimum of 5 years follow up were analysed. Preoperative investigations: Endoscopy of the larynx, sonograpy and CT scan of the neck (MRI) Laryngomicroscopy: Tungsram TLS61, Lasram laser and Daeshin DS 40UB laser devices, Opton microscope, Kleinsasser and Weerda laryngoscopes, rigid optics Laser cordectomies were divided after the ELS classification into 6 types The resected specimen was sent oriented and marked for pathological examination Patient s material, method
26 Cancer of the vocal fold patients Ratio - Male : Female = 5:1 (USA) At the Dept. ORL-HNS Szeged: male (87% ) : female (13%) ratio = 7.5:1 Age: years - 81% Predisposing factors smoking + alcohol consumption (75%) alcohol (4%) no reported (21%) Other etiology (gas, chemicals, dust profession, irritation)
27 Risk factor analysis: smoking and alcohol in a case-control study (odds ratio-or) SMOKING ALCOHOL 22% CASE GROUP CASE GROUP 48% 52% 78% CONTROL GROUP 26% CONTROL GROUP 25% 74% OR=(78x74)/(22x26)=10 10x RISK 75% OR=(48x75)/(52x25)= x RISK


28 T classification of early vocal cord cancers 289 patients underwent transoral laser surgery Tis - 21 patients T1a patients T1b - 57 patients T2-32 patients Laser device: Daeshin DS 40UB Microspot Ultra pulse mode
 (ELS classification) I.")


 V.")
 VI.")
29 6 types of laser cordectomy in our patient s material (%) (ELS classification) I. Subepithelial excision - 16% II. Subligamental excision III. Intramuscular excision - 34% (type II., III.) IV. Total cordectomy - 38% V. a, Extension: anterior commissure V. b, Extension: arytenoid (vocal process) V. c, Extension: subglottis V. d, Extension: ventricle (Morgagni sac) VI. Anterior commissure - 12% Eur Arch Otorhinolaryngol (2000) 257, Endoscopic cordectomy, proposal for a classification by the Working Committee (ELS)

30 At the begining of the CO2 laser application endolaryngeal laser surgery was used for T1a glottic tumours

,")


31 T1a vocal cord tumour (ALA), laser cordectomy, type II.


32 Vocal cord tumour T1a, type I. laser cordectomy (ALA)




33 T2 vocal cord tumour, type V. laser cordectomy (ALA)




34 T1a vocal cord carcinoma, laser cordectomy type II.-III. (AF)





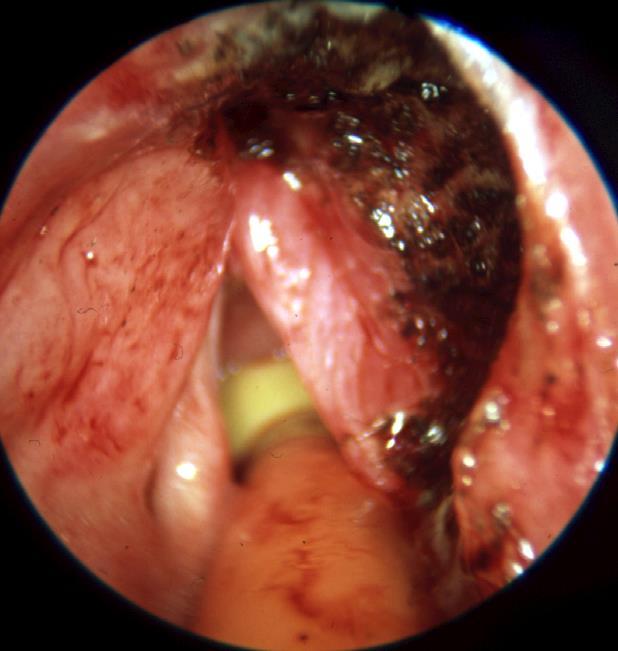
35 T1b tumour, vocal cord: laser resection, anterior commissure, thyroid cartilage


36 CT and pathlogical section: evaluation of the anterior commissure



37 After laser cordectomy left Recurrent tumour: vocal cord - T2:


")
38 T1 vocal cord cancer laser cordectomy (video)
 cc. verrucosum (3%) cc.")
39 Pathological establishment of T1, T2 vocal cord cancers after laser cordectomy Squamous cell cancer - cc. planocellulare (96%) cc. verrucosum (3%) cc. mucoepidermoid (1%)
40 Postoperative oncological and functional results Laser cordectomy, types I.-VI.: Survival Mobility of the vocal cords Phonation Quality of voice depends on the extension of excision
 laser surgery 1987 1989 1991 1993 1995 1997 1999 2001")
41 Surgery of the early glottic cancer : open approach, vertical partial laryngectomy was replaced by transoral (endoscopic) laser surgery
42 Results 289 laser cordectomy: 5 years survival: Tis tumours 100%, T1a 92%, T1b 77% and T2 83% For 87% of our patients with early glottic cancer CO2 laser excision proved to be a successful treatment, as a primary endoscopic surgery Types of laser cordectomy: I. type - 16%, II.-III. type - 34%, IV. type - 38%, V. type -12% 13% 87% Tumor free Recurrence
43 Results after salvage therapy - laser cordectomy Survival after salvage therapy: 97%. In 96% of our patients larynx and voice have been preserved 5 years laser specific survival: 93% Salvage therapies (13%): Repeated laser resection 6% Hemilaryngectomy 3% Laryngectomy 3% Radiation therapy, fronto-lat. resection 1% Neck management: RND 3% 3% 97% Tumor free Recurrence




44 Phonation after laser cordectomy, types I., III., IV. I. III. IV. III.



 III.")
45 Laser cordectomy types III., IV., V. (removal of vestibular fold) III. IV. IV. V.


46 Endoscopy, phonation post type IV.,V. laser cordectomy Scar formation (anterior comissure) Granulation - phonation with false cord phonation deteriorated

 Voice Handicap")
47 Functional results subjective voice analysis Telephone questionnaire (n=30) Voice Handicap Index (n=23)

48 Functional results Objective voice analysis with programme Praat
49 Cost benefit: transoral laser resection of tumours of the vocal cord Time of endoscopic surgical resection - laser cordectomy: min. Hospitalization: 1-3 days Costs: Laser cordectomy: Ft versus external approach surgery or radiation therapy: Ft
50 Conclusions Laser cordectomy represents a minimally invasive, transoral surgical method with good oncological and good (type I,II,III) or acceptable (type IV,V,VI) functional results (quality of life). There was no swallowing disorder Smoking plays an important role in the development of glottic cancer in our patients too.
51 20 years experience with endolaryngeal CO2 laser surgery of the early supraglottic tumours Introduction of the transoral laser surgery of the T1, T2 supraglottic tumours (1989-)
: transoral CO2 laserresection (1989-2010) 85%")

52 Patient s material: T1, T2 supraglottic tumours ( ) 63 Patients (15%): transoral CO2 laserresection ( ) 85% of patients with supraglottic tumour underwent external approach surgical intervention (supraglottic laryngectomy, laryngectomy)
53 63 patients - staging Transoral CO2 laser-resection 40 patients with tumour of the epiglottis (36 T1N0, 4 T1N1), 4 pat. - tumour of the ventricular fold (4 T1N0), 13 pat. with supraglottic-vallecula tumour (10 T2N0, 3 T2N1) and 6 pat. with supraglottic-aryepiglottic fold (3 T2N0, 3 T2N1) Localization supraglott. tumour Staging Epiglottis Ventricular fold Supraglott.- vallecula Supraglott.- aryepiglott. fold T1N0 T1N1 36 patients 4 patients 4 patients T2N0 T2N1 10 patient 3 patients 3 patients 3 patient Total 40 pat. 4 pat. 13 pat. 6 pat. = total of 63 patients
54 Patient s material: supraglottic tumours of the larynx ( ) Transoral laser resection in 63 patients (40 patients with epiglottis tumour, 4 with ventricular fold, 13 with supraglottic-vallecula and 6 with aryepiglottic fold tumour) Of the 63 supraglottic carcinoma 10 patients underwent endolaryngeal laser excision which was combined with simultaneous modified neck dissection (mrnd), (4 patients with tumour of the epiglottis (T1N1), 3 supraglottic-vallecula (T2N1) and 3 supraglotticaryepglottic fold tumour (T2N1) + primary neck metastases) 20 patients got radiation therapy
55 Supraglottic cancer T1 tumour of the epiglottis and after CO2 laserresection (partial epiglottectomy)


56 Supraglottic CO2 laser resection
 in the transoral")
 supraglottic")

57 Role of imaging (CT, MRI) in the transoral laser surgery of early (T1, T2) supraglottic tumours without infiltration of the preepiglottic space



58 Infrahyoid carcinoma of the epiglottis, early and late postoperative results after transoral laser resection Laser epiglottectomy (video) Without spreading to the preepiglottic space/ no detectable metastasis



59 Carcinoma of the supraglottic-vallecula Endoscopic CO2 laser resection + mrnd (video)



60 Tumour of supraglottic-aryepiglottic fold Transoral laser resection (video)


")

61 Endoscopic laser resection and horizontal supraglottic laryngectomy: Endoscopic supraglottic laser resection (epiglottectomy) postoperative results Horizontal supraglottic laryngectomy (external approach)

62 Role of CT in the follow up: detection of late neck metastasis 6 years after transoral supraglottic laser resection





63 Post transoral supraglottic laser resection: late neck metastasis, ND

 No aspiration, glottis")
64 Late postoperative functional result after transoral laser resection of supraglottic tumour (video) No aspiration, glottis closure is intact
65 Cost benefit of transoral laser supraglottic resection Time of endoscopic surgical resection (laser supraglottic resection): 0.5-1h (versus horizontal supraglottic laryngectomy h) Hospitalization: 3-8 days Average hospitalization time of transoral laser supralgottic resection: 6 days versus horizontal supraglottic laryngectomy 17 days Costs: Laser supraglottic resection Ft + (neck dissection) Horizontal supraglottic resection: Ft- Depending on complications
66 Hospitalization after laser supraglottic resection (TLR), horizontal supraglottic resection (HSPR) and total laryngectomy (TL) Hospitalization time d d a a y y s s hosp. time Salvage laryngectomy hosp. time with complication
67 Dysphagia, aspiration after TLR, HSPR, TL Dysphagia, aspiration post TLR, HSPR and TL




68 Social life questionaire (The EuroQol Group - EQ-5D-3L questionaire) Postop. daily activity Psychologic problems Average satisfaction after surgeries Feeding, gastrostomy, PEG perioperative chronic
69 Results 47 (75%) patients with early supraglottic cancer became free of tumor after single laser resection 16 patients (25%) developed local recurrence 1 patient had irresecable neck metastasis (tumor free supraglottis), who died of metastases Salvage-therapies (16 patients): 7 repeated laserresections, 3 radiation therapies, 4 horizontal supraglottic laryngectomies, 2 total laryngectomies, 5 RNDs (late neck metastases) after salvage therapies there is no sign of recurrence Local tumor free survival: 85% Survival after salvage therapy: 98% Larynx sparing treatment: 96%
70 85% local tumour-free survival of supraglottic cancer patients after a transoral CO2 laser resection (Kaplan- Meier curve) 63 patients T1, T2 supraglottic tumours
71 Conclusions In selected patients with early supraglottic tumour (63 patients/15%) transoral laser resection proved to be a good endoscopic surgical option versus horizontal supraglottic laryngectomy In 10 patients transoral laser method was combined with neck dissection in one session There was no need for tracheostomy and postoperative aspiration was rarely severe depending on the extension of the resection Postoperative quality of life of transoral laser resection highly exceeds of external approach, horizontal supraglottic laryngectomy
72 Advantages of transoral CO2 laser technique Minimally-invasive surgical intervention - faster recovery No need for tracheostomy Minimal intraoperative bleeding No or moderate edema rarely developed Moderate (severe) aspiration, but less deglutition problem than after open access surgery (partial laryngectomy) Acceptable - good swallowing and voice Feeding tube or PEG is rarely required, only after extensive transoral supraglottic resection Shorter hospitalization: 2-8 days vs. 1-3 weeks - cost benefit!



73 FUTURE: TRANSORAL ROBOT ASSISTED SURGERY (TORS)! DA VINCI SURGICAL ROBOT DIA ALCÍM Bullet Point Lorem ipsum dolor sit amet, consectetur adipiscing elit. Curabitur nec nisi vestibulum, interdum leo vitae, consequat ligula. Mauris ultrices elit vitae metus llentesque, sit amet vulputate nisl commodo. Bullet Point 2 Quat ligula. Mauris ultrices elit vitae metus pellentesque Bullet Point 3 QUAT LIGULA. MAURIS ULTRICES ELIT VITAE METUS PELLENTESQUE Mauris ultrices elit vitae metus pellentesque, sit amet



74 TRANSORAL ROBOT ASSISTED SURGERY (TORS) DA VINCI



75 Thank you for your attention!
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Early Glottic Cancer
 Early Glottic Cancer Mark S. Courey, MD Professor, UCSF Department of OHNS Director, Division of Laryngology Definition High-grade grade dysplasia Carcinoma in situ Micro-invasive invasive carcinoma Invasive
Early Glottic Cancer Mark S. Courey, MD Professor, UCSF Department of OHNS Director, Division of Laryngology Definition High-grade grade dysplasia Carcinoma in situ Micro-invasive invasive carcinoma Invasive
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
SmartXide 2 - SmartXide HS
 SmartXide 2 - SmartXide HS Laryngeal Microsurgery with Scanner-Assisted CO 2 Laser White Paper - October 2011 White Paper SmartXide 2 - SmartXide HS October 2011 Laryngeal Microsurgery with Scanner-Assisted
SmartXide 2 - SmartXide HS Laryngeal Microsurgery with Scanner-Assisted CO 2 Laser White Paper - October 2011 White Paper SmartXide 2 - SmartXide HS October 2011 Laryngeal Microsurgery with Scanner-Assisted
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Original Article Analysis of surgical methods and their long-term effect on laryngeal carcinoma
 Int J Clin Exp Med 2016;9(2):4491-4496 www.ijcem.com /ISSN:1940-5901/IJCEM0013482 Original Article Analysis of surgical methods and their long-term effect on laryngeal carcinoma Hong-Bing Liu *, Chun-Ping
Int J Clin Exp Med 2016;9(2):4491-4496 www.ijcem.com /ISSN:1940-5901/IJCEM0013482 Original Article Analysis of surgical methods and their long-term effect on laryngeal carcinoma Hong-Bing Liu *, Chun-Ping
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
1/14/2019 CRITICAL PATHWAYS IN HEAD AND NECK CANCER DISCLOSURES OBJECTIVES
 CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
Learning objectives Describe anatomically and clinically the di ifference between laryngeal cancer and hypopharyngeal cancer Be able to describe clini
 Laryngeal cancer Hanwei PENG, MD, PhD Thyroid Surgery Research Center, SU UMC Head and Neck Department, Cancer Hospital, SUMC Learning objectives Describe anatomically and clinically the di ifference between
Laryngeal cancer Hanwei PENG, MD, PhD Thyroid Surgery Research Center, SU UMC Head and Neck Department, Cancer Hospital, SUMC Learning objectives Describe anatomically and clinically the di ifference between
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue
 Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Carcinoma of the larynx L 4. Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%.
 L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Mohammed AlEssa MBBS,FRCSC Consultant Otolaryngology,Head & Neck Surgery King Saud University- medical city National guard health affairs KAMC
 Mohammed AlEssa MBBS,FRCSC Consultant Otolaryngology,Head & Neck Surgery King Saud University- medical city National guard health affairs KAMC 1.7% of all cancer in male in KSA ** Laryngeal cancer affects
Mohammed AlEssa MBBS,FRCSC Consultant Otolaryngology,Head & Neck Surgery King Saud University- medical city National guard health affairs KAMC 1.7% of all cancer in male in KSA ** Laryngeal cancer affects
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
MULTIDISCIPLINARY MGMT. OF INTERMEDIATE STAGE LARYNGEAL CANCER, ROBERT L. FERRIS, MD 1
 CANCER, ROBERT L. FERRIS, MD 1 Thank you Dr. Johnston, good morning. I m pleased to present the grand rounds for the University of Pittsburgh, the Division of Head and Neck Surgery, and the topic for this
CANCER, ROBERT L. FERRIS, MD 1 Thank you Dr. Johnston, good morning. I m pleased to present the grand rounds for the University of Pittsburgh, the Division of Head and Neck Surgery, and the topic for this
Hoarseness. Evidence-based Key points for Approach
 Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Treatment Considerations for Early Glottic Carcinoma: Lessons Learned and a Primer for the General Otolaryngologist
 Commentary Treatment Considerations for Early Glottic Carcinoma: Lessons Learned and a Primer for the General Otolaryngologist Otolaryngology Head and Neck Surgery 2014, Vol. 150(2) 169 173 Ó American
Commentary Treatment Considerations for Early Glottic Carcinoma: Lessons Learned and a Primer for the General Otolaryngologist Otolaryngology Head and Neck Surgery 2014, Vol. 150(2) 169 173 Ó American
Head and Neck Cancer. What is head and neck cancer?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
What is head and neck cancer? How is head and neck cancer diagnosed and evaluated? How is head and neck cancer treated?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Evaluation of CO 2 Laser Surgery for Early Carcinoma Larynx
 10.5005/jp-journals-10001-1066 RESEARCH ARTICLE Evaluation of CO 2 Laser Surgery for Early Carcinoma Larynx Evaluation of CO 2 Laser Surgery for Early Carcinoma Larynx 1 Vijay K Sharma, 2 Ajith Nilakantan
10.5005/jp-journals-10001-1066 RESEARCH ARTICLE Evaluation of CO 2 Laser Surgery for Early Carcinoma Larynx Evaluation of CO 2 Laser Surgery for Early Carcinoma Larynx 1 Vijay K Sharma, 2 Ajith Nilakantan
Hypopharynx. 1. Introduction. 1.1 General Information and Aetiology
 Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Endoscopic CO -Laser Surgery for Vocal Cord Cancer
 Diagnostic and Therapeutic Endoscopy, Vol. 1, pp. 69-74 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in Malaysia
Diagnostic and Therapeutic Endoscopy, Vol. 1, pp. 69-74 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in Malaysia
LARYNGEAL DYSPLASIA. Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital
 LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
LARYNGEAL DYSPLASIA Tomas Fernandez M; 3 rd year ENT resident, Son Espases University Hospital INTRODUCTION Laryngeal cancer constitutes 1-2% of all malignancies diagnosed worldwide Survival is related
If You Have Head or Neck Cancer
 EASY READING If You Have Head or Neck Cancer What is head and neck cancer? Cancer can start any place in the body. Cancer that starts in the head and neck can have many names. It depends on where the cancer
EASY READING If You Have Head or Neck Cancer What is head and neck cancer? Cancer can start any place in the body. Cancer that starts in the head and neck can have many names. It depends on where the cancer
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Clinico-etiopathological and management profile of laryngeal tumours in a tertiary care centre
 International Journal of Otorhinolaryngology and Head and Neck Surgery Pal P et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):913-917 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Original
International Journal of Otorhinolaryngology and Head and Neck Surgery Pal P et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):913-917 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Original
Chirurgia conservativa. Vice Direttore Scientifico Direttore Divisione Testa e Collo Istituto Europeo di Oncologia
 Chirurgia conservativa Fausto Chiesa Mohssen Ansarin Vice Direttore Scientifico Direttore Divisione Testa e Collo Istituto Europeo di Oncologia Laryngeal Cancer: 51% of H&N cancer H&N Cancer 4.7% of all
Chirurgia conservativa Fausto Chiesa Mohssen Ansarin Vice Direttore Scientifico Direttore Divisione Testa e Collo Istituto Europeo di Oncologia Laryngeal Cancer: 51% of H&N cancer H&N Cancer 4.7% of all
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Transoral Laser Microsurgery in Carcinomas of the Oral Cavity, Pharynx, and Larynx
 The indications and approach using CO 2 laser surgery in carcinomas of the upper aerodigestive tract are reviewed. Lu Jian Jun. The Dulcimer, 2000. Oil on canvas, 36 48. Courtesy of Weinstein Gallery,
The indications and approach using CO 2 laser surgery in carcinomas of the upper aerodigestive tract are reviewed. Lu Jian Jun. The Dulcimer, 2000. Oil on canvas, 36 48. Courtesy of Weinstein Gallery,
Katsuro Sato. Department of Speech, Language and Hearing Sciences, Niigata University of Health and Welfare, Niigata, Japan
 Report Niigata Journal of Health and Welfare Vol. 12, No. 1 Retrospective analysis of head and neck cancer cases from the database of the Niigata Prefecture Head and Neck Malignant Tumor Registration Committee
Report Niigata Journal of Health and Welfare Vol. 12, No. 1 Retrospective analysis of head and neck cancer cases from the database of the Niigata Prefecture Head and Neck Malignant Tumor Registration Committee
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Case Report A Case of Typical Carcinoid of the Larynx
 Case Reports in Otolaryngology Volume 2012, Article ID 717251, 5 pages doi:10.1155/2012/717251 Case Report A Case of Typical Carcinoid of the Larynx Shintaro Sato, 1 Yuichiro Kuratomi, 1 Fumio Yamasaki,
Case Reports in Otolaryngology Volume 2012, Article ID 717251, 5 pages doi:10.1155/2012/717251 Case Report A Case of Typical Carcinoid of the Larynx Shintaro Sato, 1 Yuichiro Kuratomi, 1 Fumio Yamasaki,
Transoral Laser Surgery for Supraglottic Carcinoma
 RA() Med Laser 2013;2(1):1-7 pissn 2287-8300ㆍeISSN 2288-0224 Transoral Laser Surgery for Supraglottic Carcinoma Jong Chul Hong 1 Kang Dae Lee 2 1 Department of Otolaryngology-Head and Neck Surgery, Dong-A
RA() Med Laser 2013;2(1):1-7 pissn 2287-8300ㆍeISSN 2288-0224 Transoral Laser Surgery for Supraglottic Carcinoma Jong Chul Hong 1 Kang Dae Lee 2 1 Department of Otolaryngology-Head and Neck Surgery, Dong-A
Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over
 Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
CODING STAGE: TNM AND OTHER STAGING SYSTEMS. Liesbet Van Eycken Otto Visser
 CODING STAGE: TNM AND OTHER STAGING SYSTEMS Liesbet Van Eycken Otto Visser OVERVIEW PART I Introduction What is stage? Why stage? History and publications of TNM Classification Clinical and pathologic
CODING STAGE: TNM AND OTHER STAGING SYSTEMS Liesbet Van Eycken Otto Visser OVERVIEW PART I Introduction What is stage? Why stage? History and publications of TNM Classification Clinical and pathologic
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
TREATMENT OF PATIENTS WITH. Early-Stage Glottic Cancer. Oncological Results and Margins in Laser Cordectomy. CME course available at
 Early-Stage Glottic Cancer ORIGINAL ARTICLE Oncological Results and Margins in Laser Cordectomy Elizabeth Sigston, MBBS, FRACS; Erwan de Mones, MD; Emmanuel Babin, MD; Stéphane Hans, MD, PhD; Dana M. Hartl,
Early-Stage Glottic Cancer ORIGINAL ARTICLE Oncological Results and Margins in Laser Cordectomy Elizabeth Sigston, MBBS, FRACS; Erwan de Mones, MD; Emmanuel Babin, MD; Stéphane Hans, MD, PhD; Dana M. Hartl,
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Protocol for the Examination of Specimens from Patients with Carcinomas of the Larynx
 Protocol for the Examination of Specimens from Patients with Carcinomas of the Larynx Protocol applies to all invasive carcinomas of the larynx, including supraglottis, glottis, and subglottis. Mucosal
Protocol for the Examination of Specimens from Patients with Carcinomas of the Larynx Protocol applies to all invasive carcinomas of the larynx, including supraglottis, glottis, and subglottis. Mucosal
Case Presentation. Faysal Ghazzay Ahmed
 Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
NAACCR Webinar Series 1. Instructors Q&A 10/6/2011. Collecting Cancer Data: Larynx Including Mucosal Melanoma of Larynx.
 NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
LARYNGEAL CANCER AT THE KORLE BU TEACHING HOSPITAL ACCRA GHANA
 LARYNGEAL CANCER AT THE KORLE BU TEACHING HOSPITAL ACCRA GHANA * E.D. KITCHER, J. YARNEY 1, R.K. GYASI 2 AND C. CHEYUO Departments of Surgery and 2 Pathology, University of Ghana Medical School, P O Box
LARYNGEAL CANCER AT THE KORLE BU TEACHING HOSPITAL ACCRA GHANA * E.D. KITCHER, J. YARNEY 1, R.K. GYASI 2 AND C. CHEYUO Departments of Surgery and 2 Pathology, University of Ghana Medical School, P O Box
11/7/2014. Disclosure Dr. Walvekar, I have the following relationship(s) with commercial interests.
 with commercial interests.") TORS & Supraglottic Laryngectomy Disclosure Dr. Walvekar, I have the following relationship(s) with commercial interests. Hood Laboratories Rec. Royalties Cook Industries Rec. Honoraria Medtronic Rec.
TORS & Supraglottic Laryngectomy Disclosure Dr. Walvekar, I have the following relationship(s) with commercial interests. Hood Laboratories Rec. Royalties Cook Industries Rec. Honoraria Medtronic Rec.
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
ORIGINAL ARTICLE. a transcervical supraglottic partial. least as far as early supraglottic cancer is concerned the surgical therapy
 Transoral Laser Surgery of Supraglottic Cancer Follow-up of 141 Patients ORIGINAL ARTICLE Heinrich Iro, MD; Frank Waldfahrer, MD; Annelore Altendorf-Hofmann, MD; Manfred Weidenbecher, MD; Rolf Sauer, MD;
Transoral Laser Surgery of Supraglottic Cancer Follow-up of 141 Patients ORIGINAL ARTICLE Heinrich Iro, MD; Frank Waldfahrer, MD; Annelore Altendorf-Hofmann, MD; Manfred Weidenbecher, MD; Rolf Sauer, MD;
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
CO 2 LASER SURGERY IN THE TREATMENT OF GLOTTIC CANCER
 CO 2 LASER SURGERY IN THE TREATMENT OF GLOTTIC CANCER Giovanni Motta, MD, 1 Erik Esposito, MD, 2 Sergio Motta, MD, 1 Gianpaolo Tartaro, MD, 3 Domenico Testa, MD 1 1 Institute of Otorhinolaryngology, Ateneo
CO 2 LASER SURGERY IN THE TREATMENT OF GLOTTIC CANCER Giovanni Motta, MD, 1 Erik Esposito, MD, 2 Sergio Motta, MD, 1 Gianpaolo Tartaro, MD, 3 Domenico Testa, MD 1 1 Institute of Otorhinolaryngology, Ateneo
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
(loco-regional disease)
") (loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
(loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Glottic carcinoma of the larynx is the most common
 Laser carbon dioxide cordectomy versus open surgery in the treatment of glottic carcinoma: Our results MAURIZIO MAURIZI, MD, GIOVANNI ALMADORI, MD, GAETANO PLAUDETTI, MD, DE CORSO EUGENIO, MD, and JACOPO
Laser carbon dioxide cordectomy versus open surgery in the treatment of glottic carcinoma: Our results MAURIZIO MAURIZI, MD, GIOVANNI ALMADORI, MD, GAETANO PLAUDETTI, MD, DE CORSO EUGENIO, MD, and JACOPO
Tongue cancer. Patient information
 What is cancer? The human body is made up of billions of cells. In healthy people, cells grow, divide and die. New cells constantly replace old ones in an orderly way. This process ensures each part of
What is cancer? The human body is made up of billions of cells. In healthy people, cells grow, divide and die. New cells constantly replace old ones in an orderly way. This process ensures each part of
RESEARCH ARTICLE. Abstract. Introduction
 DOI:10.22034/APJCP.2017.18.8.2035 Clinicopathologic Findings and Treatment Outcome of Laryngectomized Patients RESEARCH ARTICLE Clinicopathologic Findings and Treatment Outcome of Laryngectomized Patients
DOI:10.22034/APJCP.2017.18.8.2035 Clinicopathologic Findings and Treatment Outcome of Laryngectomized Patients RESEARCH ARTICLE Clinicopathologic Findings and Treatment Outcome of Laryngectomized Patients
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
A retrospective review in the management of T3 laryngeal squamous cell carcinoma: an expanding indication for transoral laser microsurgery
 Butler et al. Journal of Otolaryngology - Head and Neck Surgery (2016) 45:34 DOI 10.1186/s40463-016-0147-1 ORIGINAL RESEARCH ARTICLE Open Access A retrospective review in the management of T3 laryngeal
Butler et al. Journal of Otolaryngology - Head and Neck Surgery (2016) 45:34 DOI 10.1186/s40463-016-0147-1 ORIGINAL RESEARCH ARTICLE Open Access A retrospective review in the management of T3 laryngeal
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Treatment of T1b glottic SCC: laser vs. radiationa Canadian multicenter study
 Taylor et al. Journal of Otolaryngology - Head and Neck Surgery 2013, 42:22 ORIGINAL RESEARCH ARTICLE Open Access Treatment of T1b glottic SCC: laser vs. radiationa Canadian multicenter study S Mark Taylor
Taylor et al. Journal of Otolaryngology - Head and Neck Surgery 2013, 42:22 ORIGINAL RESEARCH ARTICLE Open Access Treatment of T1b glottic SCC: laser vs. radiationa Canadian multicenter study S Mark Taylor
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Esophageal cancer. What is esophageal cancer? Esophageal cancer is a disease in which malignant (cancer) cells form in the tissues of the esophagus.
 cells form in the tissues of the esophagus.") Esophageal Cancer Esophageal cancer What is esophageal cancer? What are risk factors? Signs and symptoms Tests for esophageal cancer Stages of esophageal cancer Treatment options What is esophageal cancer?
Esophageal Cancer Esophageal cancer What is esophageal cancer? What are risk factors? Signs and symptoms Tests for esophageal cancer Stages of esophageal cancer Treatment options What is esophageal cancer?