COMMON SKIN CANCERS Recognition and Management. Objectives. Structure of the Skin 2/3/2014. Marlyn J. Storch-Escott RN, BSN, MSN, ANP
|
|
|
- Violet Russell
- 6 years ago
- Views:
Transcription
1 COMMON SKIN CANCERS Recognition and Management Marlyn J. Storch-Escott RN, BSN, MSN, ANP Objectives List the most common types of skin cancers. Identify 2-3 clinical manifestations of each common skin cancer. Explain the difference between shave biopsy, punch biopsy, and excisional biopsy. Describe the treatment modalities for the common types of skin cancer. Structure of the Skin 1
2 Epidermis Outermost layer of the skin Composition Stratum basalis (separates dermis from epidermis) Stratum spinosum (spiny cell layer) Stratum granulosum (granular cell layer) Stratum corneum (cornified layer) Dermis Two layers Adventitial layer Reticular Functions Temperature control Mechanical Cutaneous sensation Subcutaneous Composition Distinct flat lobules Blood vessels, nerves, and lymphatics Functions Heat insulator Shock absorber 2

3 Ancillary Skin Structures Glands Sebaceous (sebum: antifungal properties) Eccrine (sweat) Apocrine (produce scent in axilla and perineum) Hair Nails General Functions of the Skin Sensation Protection»Thermoregulation Secretion Flexibility Sunlight and the Skin Photobiology 3
4 Photobiologic skin reactions and diseases Caused by ultraviolet light From the sun in the form of Solar radiation Solar Radiation Continuous spectrum of wave lengths of electromagnetic energy over 290 nm (nm = unit for measuring the wavelength of light = nanometer) Ultraviolet light Divided into: UVA ( nm) Constant throughout the day Penetrates window glass Interacts with topical and systemic chemicals and medications Produces immediate and delayed tanning Results in Photoaging Can reach dermis and subcutaneous fat (longer wavelenths) 4
5 UVB ( nm) Most intense between 10 AM and 4 PM Absorbed by window glass Prior exposure to UVA enhances sunburn reaction of UVB Primarily responsible for sunburn, suntan, and skin cancers Delivers high amount of energy to stratum corneum and superficial layers of the epidermis UVC ( nm) Absorbed by the ozone layer Only transmitted artificially in germicidal lamps and mercury arc lamps Effects of Sun Damaged Skin Photoaging Solar elastosis Course, deep wrinkling Skin thickens Persistent pigmentation Telangiectasia Maturation of keratinocytes Sun tan and sun burn Skin cancers 5


6 6
7 Tolerance to Sunlight Dependent on individual s skin type Estimated on response to first 30 minutes of exposure to summer sun Skin Types Type 1: always burns easily; never tans, very sensitive Type 2: usually burns easily; tans minimally, very sensitive Type 3: Burns moderately; tans gradually and uniformly, sensitive Type 4: burns minimally; always tans well, moderately sensitive Type 5: Rarely burns; tans profusely, minimally sensitive Type 6: Never burns: deeply pigmented, insensitive Types of skin lesions due to Solar radiation and/or tanning beds 7


8 Actinic Keratosis (AK) Appears as a poorly circumscribed, pink, red or tan papule that feels or looks scaly, crusty, or crumbly, generally rough and dry May itch or present with burning or pricking sensation Can bleed, but rarely May present as cutaneous horn Actinic cheilitis on lips 8

9 Located on sun-exposed areas of the skin Face, head, neck, arms, hands, and legs Mainly on skin types 1-3 Possibility on 4 and 5 May be visualized but mainly located by feel AKs considered pre-malignant lesions Regarded as precursor to SCC or BCC Mainly progress to SCC Estimates of transformation range from 0.025% to 20% per year 44% - 97% SCCs 36% BCCs Dictates need to treat these lesions 9
 Only if indurated")
10 AKs Seen more frequently in males Increase in numbers with age Skin types 1 3 mainly History of excessive sun exposure without protection Produce atypical squamous cells in the epidermis Penetration of the epidermis/dermis junction indicates development of SCC Diagnosis of AKs History of extreme frequent sun exposure Clinical picture Felt and/or visualized Biopsy (shave biopsy) Only if indurated lesion Would indicate SCC 10
11 Differential Diagnoses Seborrheic keratosis Bowen s disease BCC SCC 11
12 Treatment of AKs Cryotherapy Use of liquid nitrogen to freeze the lesions Boiling point of liquid nitrogen is 196 C Freezes lesions to about -50 C Administered by direct spray or contact swab 10 to 15 second exposure Margin beyond lesion of 1-3 mm Allow slow thawing seconds Pain is moderate to severe during freezing May produce dyspigmentation Cryotherapy after effects Erythema Edema (localized) Blister formation (7-10 days for formation) May experience fluid drainage Dry crust forms 99% cure rate fro treated lesions 12
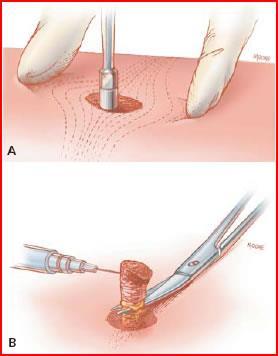
 Using a small size curet, held like a pencil, skin around the lesion is held taut with fingers of free hand Use smooth, firm strokes with curet until firm tissue base is acquired and")

13 Electrodesication and Curettage (ED&C) Requires local anesthesia (Lidocaine with epinephrine) Equipment required: Electricator, Hyfrecator, Bantam Bovie, Ritter coagulator Sharp dermal curets (1 7 mm) Using a small size curet, held like a pencil, skin around the lesion is held taut with fingers of free hand Use smooth, firm strokes with curet until firm tissue base is acquired and resistance occurs Then dessication is achieved by inserting needle of electrosurgical unit into the tissue Char produced result in hemostasis Care of ED&C site Heals by secondary intention Wound should be cleansed daily with soap and water Antibiotic ointment may be applied Light dressing in place until dry Follow-up visit in 7-10 days Patient should be instructed in signs of infection 13
 Provides uniform blue light distribution for 1000 sec Power density fixed at 10mW/cm2 Tissue oxygen PDT Functions by light activating the drug in the tissue which")
14 Photodynamic Therapy (PDT) Light therapy for treatment of lesions Requires Photosensitizing drug and light source 20% 5-aminolevulinic acid (hydrochloride salt) and a vehicle Light of proper wave length and power» Blue light (BLU-U) Provides uniform blue light distribution for 1000 sec Power density fixed at 10mW/cm2 Tissue oxygen PDT Functions by light activating the drug in the tissue which creates a singlet oxygen which is highly cytotoxic, results in tissue destruction Safety precautions Protective eye goggles for both patient and provider 14
15 Patient discomfort with PDT Stinging and burning occurs most severely in the initial stages; plateaus at approximately 6 minutes Symptoms diminish at completion of treatment Within 24 hours discomfort should abate entirely PDT Discomfort Relief Measures NSAIDs prior to or after procedure May also use acetaminophen, diazepam, dipherhydramine HCl, hydrocodone Use of topical lidocaine 4% or ELA-Max Ice packs Cold compresses Post treatment topical steroid cream Common local responses to PDT Crusting Pruritus Scaling Rarely, vesicle or blister formation 15
16 TOPICAL MEDICATIONS for Actinic Keratosis 5-FU 5%, 1%, 0.5% cream Applied QD or BID for 3-5 weeks Inhibits thymidylate synthetase thus preventing cell proliferation and causing selective cell death Produces inflammation, erythema, and edema initially Continued until erosion, necrosis, and ulceration of lesions occurs Complete healing in 1-2 months after cessation of medication Adverse reactions are local: burning, crusting, and allergic contact dermatitis May use weekly pulse dosing Apply BID two consecutive days a week F/U in 3 4 weeks 16


17 17
18 IMIQUIMOD Cream 5% Applied 3x / week at HS for 4 6 weeks Left on 8 hours and then washed off Produces interferon which destroys precancerous and cancer cells, is an immune response modifier More readily accepted by patient Lesser number of applications Skin response less intense than 5-FU Similar results to 5-FU Diclofenac Sodium Gel 3% Applied BID for days Inhibits cyclooxygenase and acts through induction of apoptosis, inhibition of angiogenesis and up-regulation of arachidonic acid pathway Adverse reactions: contact dermatitis, dry skin, edema, exfoliation, pain, paresthesia, pruritis, rash 18
19 CHEMICAL PEEL for Actinic Keratosis Alpha hydroxy acids topically cause epidermolysis and elimination or keratosis Includes 30 70% Glycolic acid Trichloroacetic acid 35 % Jessner s solution 5-FU often used for 5 7 days prior to peel to light up the lesions Acid is applied to the lesions with cotton swab and left on for 5 10 minutes Then removed with alcohol Produces a controlled, partial thickness exfoliation of epidermis and outer dermis Local complications of chemical peel Pigmentation changes Scarring Milia Ectropion Infection Activation of herpes simplex Toxic shock syndrome 19
20 Chemical facial exfoliation can be: DEEP Phenol in Baker s formula is used Burn extends 2 3 mm May cause cardiac arrhythmias Full epithelialization occurs in 6 7 days Provides substantial improvement in rhytidosis and actinic damage MEDIUM DEPTH Trichloroacetic acid 35% - 50% Lightens pigmentation and improves rhytides Minimal systemic toxicity Local complications: scarring and pigmentation problems. SUPERFICIAL Trichloroacetic acid 10% - 25% or Glycolic acid 50% - 70% Depth of penetration titrated by timed duration of acid placement Left on 3 7 minutes Repeated 3-4 times Removes AKs, fine wrinkles, lentigines, melasma, and seborrheic keratoses 20

21 BASAL CELL CARCINOMA (BCC) Most common form of skin cancer Locally invasive, aggressive, and destructive Extremely rare metastasis Persistently bleeding and scabbing, nonhealing papule is most common presentation 21
 Over 40 years of age Location of BCCs Head and neck: most commonly 25 30% on the nose Shoulders Back Upper chest Arms and legs")
22 Risk Factors for BCC Fair skin (mainly types 1-3) Degree of sun exposure Men have higher incidence than women Tanning beds ( emit both UVA and UVB radiation) Over 40 years of age Location of BCCs Head and neck: most commonly 25 30% on the nose Shoulders Back Upper chest Arms and legs 22
 Micronodular (15%) Infiltrative (7%) Morpheaform (1%) Histologic Types Mixed pattern can be present in 38.")
23 Pathophysiology of BCC Arises from basal keratinocytes of the epidermis and adnexal structures (hair follicles and eccrine sweat ducts) Nodular (21%) Superficial (17%) Micronodular (15%) Infiltrative (7%) Morpheaform (1%) Histologic Types Mixed pattern can be present in 38.5% if the lesions of BCC 23


24 Morphology of BCC Papule or nodule with rolled border Translucent or pearly with possible crust Round or ovoid with depressed center Erythematous (red to pink) Telangiectasia present May be pigmented brown, black, or blue Generally firm or hard 24

25 Diagnosis of BCC Visual exam Good lighting, hand magnifier, palpation Biopsy Shave biopsy Removal of small piece of suspect lesion Excisional biopsy Removal of entire suspect lesion Punch biopsy Removal of entire suspect lesion down to subcutaneous level All biopsies require local anesthesia Generally Lidocaine with epinephrine A scalpel blade or a punch instrument if punch biopsy being performed Medication for hemostasis 25% - 30% aluminum chloride Silver nitrate sticks Sutures if punch biopsy or excisional biopsy performed 25


26 26

27 Differential diagnoses for BCCs Sebaceous hyperplasia Seborrheic keratosis Bowen s disease Granuloma annulare Actinic keratosis Nevus Melanoma 27
 Topical medications (5-FU or Imiquimod) Rarely radiation or laser surgery Variant of BCC Gorlin s syndrome Basal cell nevoid syndrome Rare inherited disease Autosomal")
28 Treatment Modalities for BCC Excisional surgery Moh s Micrographic surgery ED&C (can be combined with cryotherapy or topical medications) Cryotherapy (can be combined with topical medications) Photodynamic Therapy (PDT) Topical medications (5-FU or Imiquimod) Rarely radiation or laser surgery Variant of BCC Gorlin s syndrome Basal cell nevoid syndrome Rare inherited disease Autosomal dominant Gene located on chromosome 9q22.3q31 Characterized by Multiple nevoid BCCs Pits in palms of hands and soles of feet Multiple jaw cysts Facial structure changes Skeletal abnormalities 28


29 29

30 SQUAMOUS CELL CARCINOMA (scc) Second most common form of skin cancer Lesion is metastatic 5 year survival rate 14 39% Matastasizes to regional lymph nodes Then to liver, lungs, bone, and brain Most common in sun-exposed areas Scalp, dorsal hands, and pinna 30


31 Risk Factors of SCC Sun exposure, especially UVB radiation Immunosuppression Other lesions: AKs, Bowen s disease, keratoacanthomas, lichen sclerosis et atrophicus (vulva), leukoplakia Chemical exposure: arsenic and therapeutic tar Sites of chronic infections: sinus tracks and bone 31


32 Location of SCC Most commonly: rim of ear and lips Face and neck Bald scalp Shoulders, arms, hands Back 32
33 Pathophysiology of SCC Originates in epidermis from keratinocytes Proliferates indefinitely Penetrated the epidermal basement membrane Proliferates into the dermis Histologic Types of SCC Highly differentiated SCC Firm or hard on palpation Poorly differentiated SCC Fleshy, granulomatous, and soft on palpation Morphology of SCC Indurated papule, plaque, or nodule May have thick keratotic scale or hyperkeratosis Firm, hard, often freely moveable or soft and, fleshy Erythematous base, yellowish skin color Polygonal, oval, round or umbilicated Telangiectasia Freckling Dry, scaly atrophic skin Regional lymphadenopathy 33

34 Diagnosis of SCC Visual examination Palpate lymph nodes Biopsy Shave Excisional Punch Differential Diagnosis of SCC Keratoacanthoma Wart Seborrheic keratosis Nummular eczema Psoriasis Paget s disease 34



35 35


36 Treatment Modalities for SCC Excisional surgery Mohs micrographic surgery Radiation ED&C Photodynamic therapy (PDT) Topical medication: 5-FU or Imiquimod Laser surgery 36
37 Variables for Recurrence and Metastasis of SCC Size: <2cm or >2cm Depth: <4mm/Clark level I to II or >4mm/Clark level of IV or V Differentiation: well differentiated or poorly differentiated (greater risk with poorly) Site: Ear (greater for recurrence) or lip (greater for metastasis) Scar carcinoma (metastasis) Previous treatment Perineural involvement Immunosuppression (metastasis) Variants of SCC Bowen s disease (SC in situ) Erythroplasia (Queyrat) Marjolin s ulcer 37


38 MALIGNANT MELANOMA 38

39 One of the most dangerous tumors Ability to metastasize to any organ Can present anywhere on the body May arise from a newly developed lesion or a pre-existing lesion Only common cancer in the US whose incidence is increasing Most common cancer in adults aged and second most common in ages Risk Factors for Melanoma High levels of sun exposure TANNING BEDS Experiencing sunburns (more than 3 in lifetime) Having numerous nevi (moles) White race History of melanoma in first degree relative Immunosuppression Previous cutaneous melanoma Sun sensitivity 39

40 Location of melanoma ANYWHERE on the body Be especially vigilant with feet, between toes, perineal area, gluteal fold, and mouth 40

41 Pathophysiology of Melanoma Originates in melanocytes Primarily found in basal layer of skin Also located in GI tract, eyes, ears, and oral and genital mucosa Melanocyte degenerates and becomes neoplastic Then can move into any area 41
 Most common in 60 or 70 year olds Mainly on the facial area Mainly radial growth Mainly brown or black in color")
42 Histologic Types Type I: Superficial spreading (70%) Most common in middle age Occurs anywhere on the body Upper back, both sexes Women s legs Bizarre lesion shapes, especially over time Multiple colors, including dull red Type II: Lentigo maligna (10%) Most common in 60 or 70 year olds Mainly on the facial area Mainly radial growth Mainly brown or black in color 42


43 Type III: Acral lentiginous melanoma (2-8%) Seen in 29% to 72% in black and Asian patients Found on palms, soles, terminal phalanges, and mucous membranes Sudden appearance of Hutchinson s sign Pigmented band in proximal nail fold 43

44 Type IV: Nodular melanoma (10 15%) Multiple colors: Blue-black, purple, red-brown, flesh-colored Raised above the skin May be ulcerated, crusty, and frequently bleeds More frequent in males Dome-shaped, polyploidy, pedunculated 44


45 Morphology of Melanoma ABCDs of melanoma A: asymmetry B: border C: color D: diameter E: elevation and enlargement Changes in surface characteristics Development of symptoms Itching (pruritus), tenderness, pain 45



46 46

47 Diagnosis of Melanoma Visual examination Using ABCDs of melanoma Use of dermatoscopy Apply fluid to skin Position dermatoscope over lesion Three point checklist (novice) Asymmetry of color and structure Atypical network of cells Blue-white structure Pattern analysis Biopsy Total excisional biopsy with narrow margins Punch biopsy Differential Diagnosis of Melanoma Congenital nevus Common acquired nevus Superficial spreading nevus Clark s nevus Blue nevus Spitz nevus Pigmented BCC Pyogenic granuloma 47


48 48



49 49
50 Treatment Modalities for Melanoma Depends upon staging of melanoma Looks at thickness, depth, and spread Diagnostic Indicators Clark s level I: confined to the epidermis II: invasion of papillary dermis (upper) III: filling of the papillary dermis (lower) IV: extending into the reticular dermis V: invasion of the subcutaneous tissue Breslow Thickness Better melanoma stage diagnostic indicator Measure (in millimeters) of the vertical depth of tumor measured from the granular cell (very top) layer downward Breslow thickness and Survival rate < 1mm: 5 year survival is % 1 2mm: 5 year survival is 80 96% 2.1 4mm: 5 year survival is 60 75% > 4mm: 5 year survival is 37 50% Staging of Tumor Process used to describe the extent of the disease Consider thickness, depth, and spread Guides providers to appropriate treatment plan and determines prognosis Goes from 0 to 4 Key information indicators T = tumor (thickness, number assigned, appearance of tumor [letter assigned] N = lymph nodes ( 0 3) M = metastasis (spread of tumor) 50
51 Types of Therapy for Melanoma Surgical excision Simple excision Mohs surgery Wide local excision Excision with sentinel lymph node biopsy Immunotherapy Treats the whole body Use of biologic agents that stimulated the immune system Include interferons and interleukins Interferon alpha 2-b: Stage II and III Interleukin 2: Stage IV» Requires hospitalization» Two cycles of high dose IV therapy drug» Must be closely monitored Chemotherapy Decarbazine (DTIC) Taxanes (docetaxel and paclitaxes) Platinum agents May be administered by isolated limb perfusion (ILP) Radiation therapy Gamma knife Cyber knife Regional perfusion (ILP) Melphalen: drug gold standard for ILP Clinical trials Side Effects of Melanoma Treatment Pain Scarring Infection Lymphedema Fatigue GI discomfort Nausea, vomiting, diarrhea, constipation 51
52 On-going Melanoma Monitoring Total body skin exams by dermatologist Q 3 months first year Q 6 months 2 5 years Yearly 6 years and on Lab Studies CBC, electrolytes, renal function, liver function and LDH levels Annual chest x-rays Radiologic imaging Bone scan, CT scans, MRIs, PET scans General Skin Cancer Prevention Avoid sun exposure during peak sun hours Wear sun protectant clothes Always wear wide-brimmed hat Utilize sunscreen daily SPF (Sun protection factor) Ratio of time required to produce erythema through a sunscreen product to the time required to produce the same degree of erythema without the sunscreen SPF ranges from or 70 SPF 15 provides 50% protection SPF 34 provided 97% protection Agents for Protection Against Solar Radiation UVB protective agents Para-aminobenzoic acid (PA PABA esters Cinnamates Salicylates Phenylbenzimidazole sulfonic acid UVA protectant agent Benzophenes Dibenzolmethanes Avobenzones 52
53 Physical Blockers Zinc oxide Titanium dioxide Iron oxide Kaolin Veterinary petrolatum Thank You for Your Attention ANY QUESTIONS? 53
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer - Non-Melanoma
 Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
General information about skin cancer
 Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Describe the functions of the vertebrate integumentary system. Discuss the structure of the skin and how it relates to function.
 Chapter 5 Describe the functions of the vertebrate integumentary system. Discuss the structure of the skin and how it relates to function. Explain the basis for different skin colors. Describe the structure
Chapter 5 Describe the functions of the vertebrate integumentary system. Discuss the structure of the skin and how it relates to function. Explain the basis for different skin colors. Describe the structure
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer
 Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
CH 05 THE INTEGUMENTARY SYSTEM
 CH 05 THE INTEGUMENTARY SYSTEM This system consists of skin and its derivatives. The skin is one of the largest organs of the body in terms of surface area. The functions of the integumentary system include:
CH 05 THE INTEGUMENTARY SYSTEM This system consists of skin and its derivatives. The skin is one of the largest organs of the body in terms of surface area. The functions of the integumentary system include:
Integumentary System-Skin and Body Coverings
 Integumentary System-Skin and Body Coverings List the four types of epithelial or connective membranes. The epithelial cutaneous includes your and is exposed to the. Its function is to. An example is..
Integumentary System-Skin and Body Coverings List the four types of epithelial or connective membranes. The epithelial cutaneous includes your and is exposed to the. Its function is to. An example is..
Integumentary System
 Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Skin and Body Membranes
 4 Skin and Body Membranes PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Skin and Body Membranes
4 Skin and Body Membranes PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Skin and Body Membranes
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Lumps and Bumps: An Organized Approach to Diagnosis and Management. Disclosure. Introduction. References. Structure of Skin.
 Lumps and Bumps: An Organized Approach to Diagnosis and Management Nothing to disclose Disclosure Tammy Pifer Than, MS, OD, FAAO Carl Vinson VAMC tammythan@bellsouth.net References Fitzpatrick's Color
Lumps and Bumps: An Organized Approach to Diagnosis and Management Nothing to disclose Disclosure Tammy Pifer Than, MS, OD, FAAO Carl Vinson VAMC tammythan@bellsouth.net References Fitzpatrick's Color
Skin Cancer. There are many types of diseases. From a simple cold to the deadly disease
 Skin Cancer Skin Cancer 1 There are many types of diseases. From a simple cold to the deadly disease Mesothelioma. Some diseases are almost harmless and some can kill you in less than a year. There are
Skin Cancer Skin Cancer 1 There are many types of diseases. From a simple cold to the deadly disease Mesothelioma. Some diseases are almost harmless and some can kill you in less than a year. There are
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs
 Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Skin Malignancies. Presented by Dr. Douglas Paauw
 Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 5 The Integumentary System Introduction The organs of the integumentary system include the skin and its accessory structures including hair, nails,
Principles of Anatomy and Physiology 14 th Edition CHAPTER 5 The Integumentary System Introduction The organs of the integumentary system include the skin and its accessory structures including hair, nails,
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Nonmelanoma skin cancers
 Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Skin Cancer Awareness
 Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Limit Direct Sun Exposure
 Summer is Too Hot. We love to be outdoors in the spring and the summer!!! We must take caution and protect our skin. May is Skin Cancer awareness month.. Skin Cancer Most avoidable of all cancers, skin
Summer is Too Hot. We love to be outdoors in the spring and the summer!!! We must take caution and protect our skin. May is Skin Cancer awareness month.. Skin Cancer Most avoidable of all cancers, skin
Disclosures. I have no conflicts of interest to disclose
 Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Non-melanoma Skin Cancer
 Non-melanoma Skin Cancer Understanding your diagnosis 1 888 939-3333 cancer.ca Non-melanoma Skin Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid.
Non-melanoma Skin Cancer Understanding your diagnosis 1 888 939-3333 cancer.ca Non-melanoma Skin Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid.
SKIN HISTOLOGY AND FUNCTION
 SKIN HISTOLOGY AND FUNCTION THREE LAYERS : EPIDERMIS BASEMENT MEMBRANE DERMIS EPIDERMIS : COMPOSED OF KERATINOCYTES NO MATRIX DEEP BASAL LAYER MITOTICALLY ACTIVE SPINOUS LAYER MATURE HYALIN HORNY LAYER
SKIN HISTOLOGY AND FUNCTION THREE LAYERS : EPIDERMIS BASEMENT MEMBRANE DERMIS EPIDERMIS : COMPOSED OF KERATINOCYTES NO MATRIX DEEP BASAL LAYER MITOTICALLY ACTIVE SPINOUS LAYER MATURE HYALIN HORNY LAYER
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 5 Annie Leibovitz/Contact Press Images 2013 Pearson Education,
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 5 Annie Leibovitz/Contact Press Images 2013 Pearson Education,
All the Rest. What is All the Rest? Integumentary System. First are the FUNCTI0NS. THERMOREGULATION function. PROTECTION function 10/12/16
 What is All the Rest? Integumentary System All the Rest Integumentary System Homeostatic Imbalances Skin Cancer Burns First are the FUNCTI0NS Chemical, Physical/Mechanical, Biological Thermoregulation
What is All the Rest? Integumentary System All the Rest Integumentary System Homeostatic Imbalances Skin Cancer Burns First are the FUNCTI0NS Chemical, Physical/Mechanical, Biological Thermoregulation
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
THE INTEGUMENTARY SYSTEM. Body Membranes & Skin
 THE INTEGUMENTARY SYSTEM Body Membranes & Skin TYPES OF MEMBRANES Epithelial Membranes includes layer of epithelial cells and connective tissue Serous Cutaneous Mucous Connective Tissue Membranes solely
THE INTEGUMENTARY SYSTEM Body Membranes & Skin TYPES OF MEMBRANES Epithelial Membranes includes layer of epithelial cells and connective tissue Serous Cutaneous Mucous Connective Tissue Membranes solely
Unit 4 - The Skin and Body Membranes 1
 Unit 4 - The Skin and Body Membranes 1 I. Unit 4: Skin and Body Membranes A. Body Membranes 1. Function of body membranes a) Cover body surfaces b) Line body cavities c) Form protective sheets around organs
Unit 4 - The Skin and Body Membranes 1 I. Unit 4: Skin and Body Membranes A. Body Membranes 1. Function of body membranes a) Cover body surfaces b) Line body cavities c) Form protective sheets around organs
Skin and Body Membranes
 Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 4 Skin and Body Membranes Slides 4.1 4.32 Lecture Slides in PowerPoint by Jerry L. Cook Skin and Body Membranes Function
Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 4 Skin and Body Membranes Slides 4.1 4.32 Lecture Slides in PowerPoint by Jerry L. Cook Skin and Body Membranes Function
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College Skin and Body Membranes
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College Skin and Body Membranes 4 Body Membranes Function of body membranes Cover body surfaces Line body cavities
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College Skin and Body Membranes 4 Body Membranes Function of body membranes Cover body surfaces Line body cavities
Introduction. Skin and Body Membranes. Cutaneous Membranes Skin 9/14/2017. Classification of Body Membranes. Classification of Body Membranes
 Introduction Skin and Body Membranes Body membranes Cover surfaces Line body cavities Form protective and lubricating sheets around organs Classified in 5 categories Epithelial membranes 3 types- cutaneous,
Introduction Skin and Body Membranes Body membranes Cover surfaces Line body cavities Form protective and lubricating sheets around organs Classified in 5 categories Epithelial membranes 3 types- cutaneous,
11/8/2012. Chapter 6 Part 1 Objectives: Skin = Integument = Cutaneous Membrane. The Structure of Skin. Epidermis
 Chapter 6 Part 1 Objectives: Define organ, and associate the skin as an organ of the integumentary system. List the general functions of the skin. Describe the structure of the layers of the skin. Summarize
Chapter 6 Part 1 Objectives: Define organ, and associate the skin as an organ of the integumentary system. List the general functions of the skin. Describe the structure of the layers of the skin. Summarize
Lid Lesions: Relax or Refer
 Lid Lesions: Relax or Refer Blair Lonsberry, MS, OD, MEd., FAAO Professor of Optometry Pacific University College of Optometry blonsberry@pacificu.edu Agenda Benign vs. Malignant lesions Benign Eyelid
Lid Lesions: Relax or Refer Blair Lonsberry, MS, OD, MEd., FAAO Professor of Optometry Pacific University College of Optometry blonsberry@pacificu.edu Agenda Benign vs. Malignant lesions Benign Eyelid
Integumentary System (Skin) Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition)
 Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition)") Integumentary System (Skin) Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition) 1 Learning Objectives Identify the major components (anatomy) of skin Differentiate between the two types of skin glands Explain
Integumentary System (Skin) Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition) 1 Learning Objectives Identify the major components (anatomy) of skin Differentiate between the two types of skin glands Explain
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Malignant Cutaneous Neoplasms
 Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP All slides Kathleen Haycraft Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology
Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP All slides Kathleen Haycraft Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology
Integumentary System
 Integumentary System Physiology of Touch Skin: our most sensitive organ Touch: first sense to develop in embryos Most important but most neglected sense How many sensory receptors do we have? (We have
Integumentary System Physiology of Touch Skin: our most sensitive organ Touch: first sense to develop in embryos Most important but most neglected sense How many sensory receptors do we have? (We have
Treatments used Topical including cleansers and moisturizer Oral medications:
 Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
CHAPTER 5 INTEGUMENTARY
 CHAPTER 5 INTEGUMENTARY skin under the skin other stuff cutaneous layer hypodermis (subcutaneous) accessory structures Cutaneous layer = skin epithelial layers = connective tissue layer = dermis Subcutaneous
CHAPTER 5 INTEGUMENTARY skin under the skin other stuff cutaneous layer hypodermis (subcutaneous) accessory structures Cutaneous layer = skin epithelial layers = connective tissue layer = dermis Subcutaneous
Dual Wavelength Phototherapy System
 Dual Wavelength Phototherapy System The AKLARUS Blue and Red Combination System is an effective, drugfree alternative for treating acne & photodamaged skin. The non-invasive Aklarus treatment has been
Dual Wavelength Phototherapy System The AKLARUS Blue and Red Combination System is an effective, drugfree alternative for treating acne & photodamaged skin. The non-invasive Aklarus treatment has been
EXCESSIVE SUN EXPOSURE A DANGER FACTOR FOR THE SKIN
 EXCESSIVE SUN EXPOSURE A DANGER FACTOR FOR THE SKIN When the weather warms up, we all like to get more sunshine. While better weather can make us feel brighter, we must also be aware of the dangers as
EXCESSIVE SUN EXPOSURE A DANGER FACTOR FOR THE SKIN When the weather warms up, we all like to get more sunshine. While better weather can make us feel brighter, we must also be aware of the dangers as
Ch. 4: Skin and Body Membranes
 Ch. 4: Skin and Body Membranes I. Body Membranes A. Function of body membranes 1. Cover body surfaces 2. Line body cavities 3. Form protective sheets around organs II. Classification of Body Membranes
Ch. 4: Skin and Body Membranes I. Body Membranes A. Function of body membranes 1. Cover body surfaces 2. Line body cavities 3. Form protective sheets around organs II. Classification of Body Membranes
Integumentary System
 Integumentary System Integumentary System Skin, hair, and nails. Skin: Epidermis: outer layer. Dermis: also called corium, or true skin. Subcutaneous fascia: innermost layer. Integumentary Glands Sudoriferous:
Integumentary System Integumentary System Skin, hair, and nails. Skin: Epidermis: outer layer. Dermis: also called corium, or true skin. Subcutaneous fascia: innermost layer. Integumentary Glands Sudoriferous:
Due next week in lab - Scientific America Article Select one article to read and complete article summary
 Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Disclosures. Melanoma and Non melanoma Skin Cancer: What You Need to Know. I have no conflicts of interest to disclose
 Disclosures Melanoma and Non melanoma Skin Cancer: What You Need to Know I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department
Disclosures Melanoma and Non melanoma Skin Cancer: What You Need to Know I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Review of Cutaneous Malignancies
 Review of Cutaneous Malignancies Tanya Nino, MD Department of Dermatology Did You Know? More than 3.5 million skin cancers are diagnosed in the US annually Melanoma incidence rates have been increasing
Review of Cutaneous Malignancies Tanya Nino, MD Department of Dermatology Did You Know? More than 3.5 million skin cancers are diagnosed in the US annually Melanoma incidence rates have been increasing
Skin Cancers Emerging Trends and Treatment Approaches
 Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
B. Incorrect! The ectoderm does not produce the dermis. C. Incorrect! The dermis is derived from the mesoderm.
 Human Anatomy - Problem Drill 04: The Integumentary System Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. From the inner cell
Human Anatomy - Problem Drill 04: The Integumentary System Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. From the inner cell
Cornell Notes Name: Date: Topic: CH 4
 *We are revisiting Ch 3B on body tissues (Connective) prior to our study of Ch 4 Integumentary. Start on p.90 I. Connective Tissue A. Functions of Connective 1. Protection 2. Support 3. Binding Together
*We are revisiting Ch 3B on body tissues (Connective) prior to our study of Ch 4 Integumentary. Start on p.90 I. Connective Tissue A. Functions of Connective 1. Protection 2. Support 3. Binding Together
Actinic Keratoses and Bowen s disease
 Actinic Keratoses and Bowen s disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Actinic Keratoses and Bowen s disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Premalignant skin tumours
 Chapter 14: Premalignant skin tumours page: 434 Premalignant skin tumours page: 435 Solar keratoses (senile keratoses) Raised red and well-defined plaques with a rough surface covered in scales of varying
Chapter 14: Premalignant skin tumours page: 434 Premalignant skin tumours page: 435 Solar keratoses (senile keratoses) Raised red and well-defined plaques with a rough surface covered in scales of varying
Anatomy Ch 6: Integumentary System
 Anatomy Ch 6: Integumentary System Introduction: A. Organs are body structures composed of two or more different tissues. B. The skin and its accessory organs make up the integumentary system. Types of
Anatomy Ch 6: Integumentary System Introduction: A. Organs are body structures composed of two or more different tissues. B. The skin and its accessory organs make up the integumentary system. Types of
SKIN. 3. How is the skin structured around the finger joints to allow for flexible movement of the fingers?
 SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
BACK TO TABLE OF CONTENTS FOCUS ON MELANOMA Oncology Annual Report BAPTIST HEALTH LEXINGTON ONCOLOGY ANNUAL REPORT
 FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
Doctors of Optometry Course Notes
 Doctors of Optometry Course Notes OD19 1CE COPE: 43871-AS Eyelid Lumps and Bumps Sunday, February 26, 2017 2:40 pm 3:30 pm Regency C 3 rd Floor Presenter: Blair Lonsberry, OD, FAAO Dr. Lonsberry is a Full
Doctors of Optometry Course Notes OD19 1CE COPE: 43871-AS Eyelid Lumps and Bumps Sunday, February 26, 2017 2:40 pm 3:30 pm Regency C 3 rd Floor Presenter: Blair Lonsberry, OD, FAAO Dr. Lonsberry is a Full
The Integumentary System. Mosby items and derived items 2010, 2006, 2002, 1997, 1992 by Mosby, Inc., an affiliate of Elsevier Inc.
 The Integumentary System The Skin Structure two primary layers called epidermis and dermis Epidermis Outermost and thinnest primary layer of skin Composed of several layers of stratified squamous epithelium
The Integumentary System The Skin Structure two primary layers called epidermis and dermis Epidermis Outermost and thinnest primary layer of skin Composed of several layers of stratified squamous epithelium
See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C
 See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C Learning objectives Discuss malignant skin lesions commonly seen in primary care. Identify common treatments
See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C Learning objectives Discuss malignant skin lesions commonly seen in primary care. Identify common treatments
Steven Robinson. Steven Robinson Memorial Endowment at
 fchwmt.org Steven Robinson Steven Robinson Memorial Endowment at Fair hair and skin Steven s story Grew up around water and loved being outdoors Experienced several sunburns as a child and young adult
fchwmt.org Steven Robinson Steven Robinson Memorial Endowment at Fair hair and skin Steven s story Grew up around water and loved being outdoors Experienced several sunburns as a child and young adult
Sun Safety and Skin Cancer Prevention. Maryland Skin Cancer Prevention Program
 Sun Safety and Skin Cancer Prevention Maryland Skin Cancer Prevention Program Do You Know the Facts About Skin Cancer? Skin cancer is the most common cancer but also the most preventable Childhood sunburn
Sun Safety and Skin Cancer Prevention Maryland Skin Cancer Prevention Program Do You Know the Facts About Skin Cancer? Skin cancer is the most common cancer but also the most preventable Childhood sunburn
Chapter 6 Skin and the Integumentary System. Skin Cells. Layers of Skin. Epidermis Dermis Subcutaneous layer beneath dermis not part of skin
 Chapter 6 Skin and the Integumentary System Composed of several tissues Maintains homeostasis Protective covering Retards water loss Regulates body temperature Houses sensory receptors Contains immune
Chapter 6 Skin and the Integumentary System Composed of several tissues Maintains homeostasis Protective covering Retards water loss Regulates body temperature Houses sensory receptors Contains immune
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Chapter 05. Lecture Outline. See separate PowerPoint slides for all figures and tables pre-inserted into PowerPoint without notes.
 Chapter 05 Lecture Outline See separate PowerPoint slides for all figures and tables pre-inserted into PowerPoint without notes. Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction
Chapter 05 Lecture Outline See separate PowerPoint slides for all figures and tables pre-inserted into PowerPoint without notes. Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction
Some Facts Who should be protected? When should we protect ourselves?
 Melanie Sharon Melanie Sharon Pharm.D Candidate 2011 Some Facts Who should be protected? Why should we protect ourselves? When should we protect ourselves? How to protect yourself? How to apply sunscreen?
Melanie Sharon Melanie Sharon Pharm.D Candidate 2011 Some Facts Who should be protected? Why should we protect ourselves? When should we protect ourselves? How to protect yourself? How to apply sunscreen?
Have a Voice in Your Choice!
 Have a Voice in Your Choice! BLU-U Blue Light Photodynamic Therapy The LEVULAN KERASTICK for Topical Solution plus blue light illumination using the BLU-U Blue Light Photodynamic Therapy Illuminator is
Have a Voice in Your Choice! BLU-U Blue Light Photodynamic Therapy The LEVULAN KERASTICK for Topical Solution plus blue light illumination using the BLU-U Blue Light Photodynamic Therapy Illuminator is
Preparing for Mohs Micrographic Surgery Tracy M. Campbell, M.D.
 Preparing for Mohs Micrographic Surgery Tracy M. Campbell, M.D. What is Skin Cancer? Skin cancer is the most prevalent of all cancers. More than one million Americans develop skin cancer every year. While
Preparing for Mohs Micrographic Surgery Tracy M. Campbell, M.D. What is Skin Cancer? Skin cancer is the most prevalent of all cancers. More than one million Americans develop skin cancer every year. While
SKIN HISTOLOGY the microscopic anatomy of the Integument. Mikrogeo. com
 SKIN HISTOLOGY the microscopic anatomy of the Integument Mikrogeo. com Hair follicles, sweat glands, sebaceous glands (even teeth) are products of the epidermis,embryologically speaking ectododerm, that
SKIN HISTOLOGY the microscopic anatomy of the Integument Mikrogeo. com Hair follicles, sweat glands, sebaceous glands (even teeth) are products of the epidermis,embryologically speaking ectododerm, that
Chapter 6: Integumentary System
 Chapter 6: Integumentary System 6.1 Introduction Why is skin considered to be an organ? What makes up the integumentary system? Integumentary System Skin (cutaneous membrane) Skin derivatives Sweat glands
Chapter 6: Integumentary System 6.1 Introduction Why is skin considered to be an organ? What makes up the integumentary system? Integumentary System Skin (cutaneous membrane) Skin derivatives Sweat glands