Critical Care Management of Acute Ischemic Stroke
|
|
|
- Mark Ramsey
- 5 years ago
- Views:
Transcription
1 Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California


2 USC Stroke Center
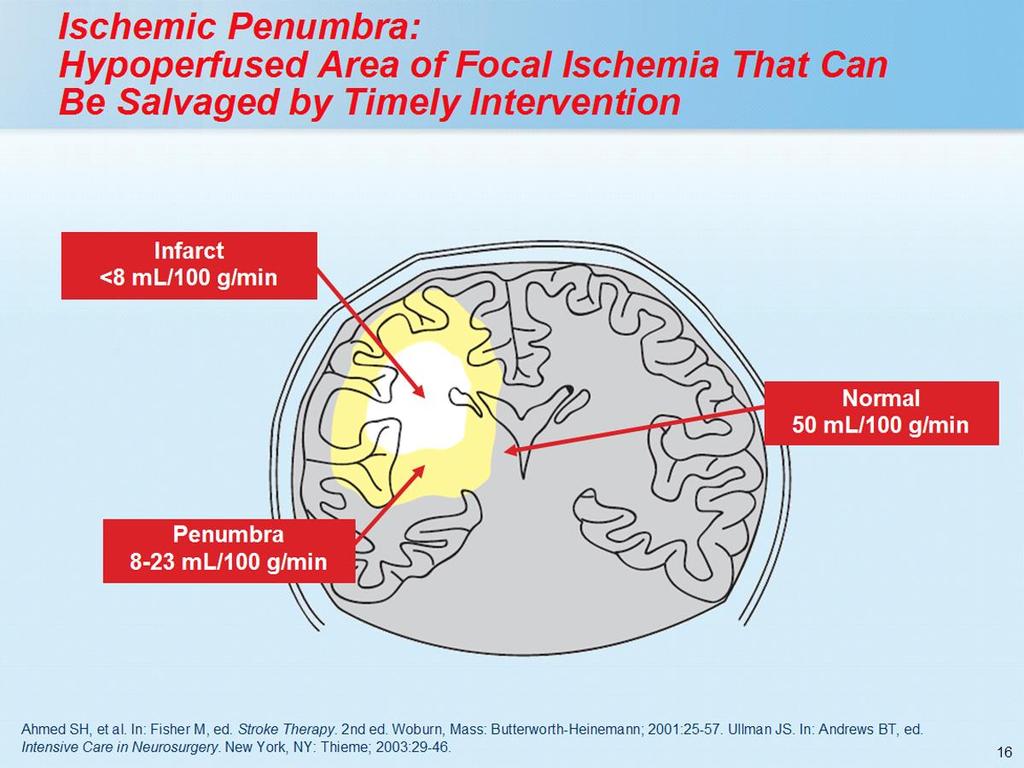
3 Acute Ischemic Stroke- Strategies The New Revolution: Reperfusion Neuroprotection
4 Glucose Fluids Temperature Blood Pressure Basic ICU Care
5 Glucose


6 Serum glucose > 200 mg/dl was associated with a 25% symptomatic hemorrhage rate >200 mg/dl

7 Admission glucose 140 mg/dl was associated with poor outcome among in reperfused patients.
8 Hyperglycemia RCT of 1,000 patients in a med-surg ICU (Van Den Berghe NEJM 2001) Intensive control mg/dl vs loose control<150 Decreased mortality in intensive glycemia group Subgroup analysis of 63 patients (Van Den Berghe Neurology 2005) Improved mortality in neurology patients
9 GIST Glucose Insulin in 21 centers, Stroke Trial <24 hrs after onset, ischemic stroke or ICH Baseline glc 6-17 mmol/l ( mg/dl) Tx GKI - 10% glucose, potassium, insulin N=933; 464 GKI 100 cc/hr, 469 control DM 16.5%, median tx 13.5 hrs, baseline glc 7.6 mmol/l (137mg/dl)
10 GIST tx regimen changes 74% Low glucose 41% 4 mmol/l (72 mg/dl) Mean reduction glc 0.57 mmol/l (10mg/dl) BP reduction 9 mm Hg
11 GIST Mortality: tx 30%, 27.3% mrs >3: tx 322, saline 339 BI<9: tx 309, saline 327 Subgroups: before/after 12 hrs Higher/lower 11 mmol/l 2007 ISC Gray CG
12 THIS Treatment of Hyperglycemia in Ischemic Stroke AIS & glc Insulin drip & glc goal vs sliding scale Trend toward benefit (46 pts total)
13 GRASP Glucose Regulation in Acute Stroke Patients Glc goals: (24), (25), <300 (24) AIS within 24 hrs Tight control had trend for benefit
14 SHINE Stroke Hyperglycemia Insulin Network Effort Insulin drip glc goal vs sliding scale glc goal <185 AIS within 12 hrs N=1400
15 SHINE Stroke Hyperglycemia Insulin Network Effort Begun 2012 Halted early for lack of effect N=1100 (1400)
16 ASA Guideline 2018 Glucose goal Monitor closely Treat Hypoglycemia aggressively
17 Fluids
18 Fluid Management Two antecubital peripheral IVs Use only 0.9NS Avoid 0.45 saline solution No D5 solution Euvolemia
19 ALIAS Albumin in Acute Ischemic Stroke AIS NIHSS>5 within 5 hrs stroke onset Albumin 2gm/kg in 2 hrs

20 Treatment of Cerebral Edema Traditional Treatments include: Hyperventilation Mannitol Sedation Paralysis Hypertonic Saline
21 Mannitol or Hypertonic Saline Mannitol gm/kg IV bolus for effect 2-3% NaCl infusion as maintenance fluid with Na goal % NaCl: Bolus for effect Hypertonic saline may be more effective than mannitol for midline shift (Manno et al 1999)
22 23.4% HS Refractory Intracranial HTN (RIA) Failure to conventional therapies - ICP < 50% (HV, Mannitol, Furosemide, Barbiturates) 8 Patients ( SAH - 5; TBI - 1; Hemangiopericytoma - 1; ICH -1); 20 episodes; Retrospective Analysis

23 Effect of 23.4% HS on ICP Suarez et al (1998)
24 Blood Pressure
25
26 Management of Hypertension in Acute Ischemic Stroke: Patients Not Eligible for Thrombolytic Therapy (2003) SBP <220 or DBP <120 No antihypertensive therapy SBP >220 or DBP= Labetalol or nicardipine to 10%- 15% reduction DBP >140 Nitroprusside to 10%-15% reduction (2007) aforementioned data suggest that the systolic blood pressure level that would prompt treatment would be >180 mm Hg pending more data, the consensus of the panel is that antihypertensive agents should be withheld unless the DBP > 120mmHg or SBP > 220 mmhg Adams HP, et al. Stroke. 2003;34:
27 Management of Hypertension in Acute Ischemic Stroke: Patients Not Eligible for Thrombolytic Therapy 2018 In patients with BP 220/120 mm Hg who did not receive IV alteplase or EVT and have no comorbid conditions requiring acute antihypertensive treatment, the benefit of initiating or reinitiating treatment of hypertension within the first 48 to 72 hours is uncertain. It might be reasonable to lower BP by 15% during the first 24 hours after onset of stroke.
28 Management of Hypertension in Acute Ischemic Stroke: Patients Eligible for Thrombolytic Therapy (2003) Prior to initiating teatment with TPA: SBP >185 or DBP >110 Labetalol or nitropaste During and after treatment with TPA: SBP= mm Hg or DBP= mm Hg Labetalol SBP >230 mm Hg or DBP= mm Hg Labetalol or nicardipine DBP >140 mm Hg Nitroprusside (2007) Eligible for tpa or other acute reperfusion tx SBP >185 or DBP >110 Labetolol or nitropaste or nicardipine During or after tx SBP= mm Hg or DBP= mm Hg labetolol SBP > 230 mm Hg or DBP mm Hg Labetolol or nicardipine If uncontrolled, consider nitroprusside Adams HP, et al. Stroke. 2003;34:
29 Management of Hypertension in Acute Ischemic Stroke: Patients Eligible for Thrombolytic Therapy 2018 Patients who have elevated BP and are otherwise eligible for treatment with IV alteplase should have their BP carefully lowered so that their systolic BP is <185 mm Hg and their diastolic BP is <110 mm Hg before IV fibrinolytic therapy is initiated.
30 Temperature
31 OR (95% CI) Fever and Stroke Mortality A Meta-Analysis: Hajat et al. Stroke. 2000;31: Reith Jorgensen Azzimondi Sharma MacWalter Combined OR * * ** ***
32 Fever and Stroke Outcome Infarct Volume Greater Deficit Poor Fx OR (95% CI) OR (95% CI) OR (95% CI) Covariates Age 1.02 ( ) 1.04 ( ) 1.08 ( ) Infection 0.72 ( ) 0.92 ( ) 1.49 ( ) Highest temp 2.81 ( ) 1.68 ( ) 1.85 ( ) Time at which hyperthermia was observed: 0 24 h 3.23 ( ) 3.06 ( ) 3.41( ) h 1.14 ( ) 1.47 ( ) 1.41( ) h 0.23 ( ) 0.33 ( ) 0.20 ( ) Castillo et al. Stroke. 1998;29:
33 Hyperthermia - BAD! Hypothermia - Good?
34 Authors Use of hypothermia in ischemic stroke: No of pts (H/C) Target temp Time from injury to start of cooling Severe stroke, mostly sedated patients in ICU setting Time to target temp Duration Re-warming rate Naritomi H et al (4 / 0) 33 o C < 5 hrs hrs. Schwab et al (20 / 0) Patient data included in subsequent study (Schwab et al. 1998, see below). Schwab et al (25 / 0) 33 o C 14±7 hrs, range hrs hrs 7-24 hrs median 18 Steiner T et al (15 / 0) o C 4-84 hrs, median hrs 72 hrs hrs Schwab et al (50 / 0) 33 o C 22 ± 9 hrs hrs hrs Passive 17 hrs Jian S et al (50 / 0) Patient data included in subsequent study (Schwab et al. 2001, see above). Georgiadis et al (6 / 0) 33 o C 28 ± 17 hrs 3±1 hrs, range hrs o C/hr Georgiadis et al (19 / 17) 33 o C 24 (range 18-24) 4 ± 1 hrs, range hrs Not stated De Georgia et al. 2004* 40 (18 / 22) 33 o C 8 59 ± 2 52 Variable; 24 hrs. 0.2 o C/hr Moderate Stroke (awake patients) Kammersgaard et al (17 / 56) 35.5 o C 3.25 ± 4.5 hrs 6 hrs 6 hrs 4 hrs Krieger et al. 2001* 19 (10 / 9) 32±1 o C 6.2 ± 1.3 hrs 3.5 ± (range 24-96) hrs o Ch Knoll et al (18 / 0) o C. 3.3 hrs 24 hrs N/A Els et al (12 / 13) 35 o C 15 ± 6 hrs 2±1 (range ) hrs 48 hrs Not stated Lyden et al. 2006* 18 (18 / 0) 33 o C 7.7 ± 3.1 hrs 7 hrs hrs 12 hrs Guluma et al (10 / 0) 33 o C <6 hrs 1.7±0.7 hrs 24 hrs 0.3 o C/hr Hemmen et al ICTuS-L * 58 (28 / 30) 33 o C <6 hrs 1.1 hrs (median) 24 hrs 0.33 o C/hr *Cooling combined with thrombolytics/reperfusion. Total number of cooled patients reported so far: 270. Malignant MCA infarction: 157. Less severe/moderate stroke: 113.
35 Ventilated patients N= Goal temperature C Time to Treatment (hours± SD) Duration of hypothermia Schwab, C 14±7 2-3 days Schwab, C 22±9 1-3 days Georgiadis, C 28± days Georgiadis, C 24 (18-14) 2-3 days Kollmar, Schwab, 2010
36 Awake patients Kammersgaard, 2000 Nhypothermia= Goal temperature in C Time to Treatment (hours+/-sd) 17 35,5 C 3±4 6 n Hypothermie -duration Krieger, ±1 C 6±1 1-4 days DeGeorgia, C 9±3 24h Lyden, C 8±3 24h Guluma, C 6±1 24h Kollmar, ,5 C 1,5 - Hemmen, C 24h Kollmar, Schwab, 2010
37 CHILI - Controlled Hypothermia in Large Infarction U.S.C. Columbia University U.M.D.N.J. Case Western Lehigh Valley Wayne State University Via Christi Regional Medical Center
38 Large hemispheric stroke Within 72 hours of onset no herniation CHILI Immmediate cooling to 35.0 for 3 days 0.5 C q12 hr rewarming Uniform shivering prophylaxis Measure: GCS, NIHSS, CT, Rankin, Barthel, Mortality, discharge location, LOS/costs
39 Hypothermia after Cardiac Arrest Two studies reported in NEJM 21 Feb 02 European Study: C Australian Study: 33 C 1 endpoint: neurological function, 5-point scale 2 endpoint: mortality & complications
40 Patients Cardiac Arrest European Study 6-mo neurological outcome: 41% relative improvement N = 137 N = 136 p = % 55% 20 0 Normothermia Hypothermia Good Outcome Poor Outcome Holzer M, Sterz F, et. al. NEJM 346(8):
41 Patients Cardiac Arrest European Study 6-mo mortality: 26% relative reduction N = 138 N = 137 p = % 41% 20 0 Normothermia Hypothermia Dead Alive Holzer M, Sterz F, et. al. NEJM 346(8):
42 Patients Cardiac Arrest Australian Study 30-day neurological outcome: 88% relative improvement N = 34 26% p = N = 43 49% Good Outcome Poor Outcome Normothermia Hypothermia Bernard SA, et. al. NEJM 346(8):
43 Hypothermia: Side effects Decreased cardiac output Increased systemic vascular resistance Thrombocytopenia Bradycardia Pneumonia
44 Hypothermia: Cooling Techniques Traditional Surface cooling Rate of core temperature decrease of o C/hr Inconvenient for medical and nursing staff Intravascular Rapid infusion of large volume (30 ml/kg), ice-cold (4 o C) LR decrease core temp by 1.6 o C over 25 min Intravascular catheter devices
45
46 64% reduction in fever burden using catheter No need for heavy sedation or paralysis Minimal Shivering response

47 Past Dr Temple Fay 1941

48 Zoll Intravascular Temperature Management


49 MEDIVANCE
50 INTREPID Impact of Fever Prevention in Brain Injured Patients
51 INTREPID International Randomized Controlled Trial of aggressive fever prevention AIS, ICH and SAH N=1200
52 INTREPID Fever burden ( C-hour; defined as the area under the temperature curve above 37.9 C) 3-, 6-, and 12-month follow-up neurologic assessment Mortality rates [7-day (or hospital discharge), 3-month, 6-month, 12-month] ICU and hospital lengths of stay

53 Multilumen Spray Catheter B E N E C H I L L


54 B E N E C H I L L PFC Intranasal Cooling Schematic O 2 PFC
55 Basic ICU Care Glucose Fluid Management Hemodynamics Temperature
Hypothermia for Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Director, Division of Neurocritical Care and Stroke
 Hypothermia for Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Director, Division of Neurocritical Care and Stroke University of Southern California FEVER Harmful Inflammatory
Hypothermia for Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Director, Division of Neurocritical Care and Stroke University of Southern California FEVER Harmful Inflammatory
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Current status of temperature management in the neuro-icu
 Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Cold Topic: Advanced Treatment Modalities in Acute Stroke
 Cold Topic: Advanced Treatment Modalities in Acute Stroke William M. Coplin, MD, FCCM Associate Prof, Neurology & Neurosurgery Wayne State University Chief, Neurology Medical Director, Neurotrauma & Critical
Cold Topic: Advanced Treatment Modalities in Acute Stroke William M. Coplin, MD, FCCM Associate Prof, Neurology & Neurosurgery Wayne State University Chief, Neurology Medical Director, Neurotrauma & Critical
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Nuts for Neuro and why I hate EMR
 Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
3/6/2017. Endovascular Selective Cerebral Hypothermia First-in-Human Experience
 Endovascular Selective Cerebral Hypothermia First-in-Human Experience Ronald Jay Solar, Ph.D. San Diego, CA 32 nd Annual Snowmass Symposium March 5-10, 2017 Introduction Major limitations in acute ischemic
Endovascular Selective Cerebral Hypothermia First-in-Human Experience Ronald Jay Solar, Ph.D. San Diego, CA 32 nd Annual Snowmass Symposium March 5-10, 2017 Introduction Major limitations in acute ischemic
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction
 Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Hypothermia After Cardiac Arrest: Where Are We Now?
 Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
SYSTEM-WIDE POLICY & PROCEDURE MANUAL. Policy Title: Hypothermia Post Cardiac Arrest Policy Number: PC-124. President & CEO Page 1 of 9
 Approved By: President & CEO Date Page 1 of 9 POLICY: PURPOSE: To define and describe the implementation of induced hypothermia post cardiac arrest and the nursing assessment and interventions required
Approved By: President & CEO Date Page 1 of 9 POLICY: PURPOSE: To define and describe the implementation of induced hypothermia post cardiac arrest and the nursing assessment and interventions required
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Mild. Moderate. Severe. 32 to to and below
 Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Hypertensive Crises. Controlling high blood pressure prevents disease. Recognition and Management of Acute Hypertensive Emergencies
 Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Hypothermia Protocols: The Big Chill AARON ELLENBOGEN, DO, MPH, FACN
 Hypothermia Protocols: The Big Chill AARON ELLENBOGEN, DO, MPH, FACN And you thought the brain freeze from a Slurpee was bad 2 u Hypothermia u Hypo, meaning under, less than, beneath u Thermia meaning
Hypothermia Protocols: The Big Chill AARON ELLENBOGEN, DO, MPH, FACN And you thought the brain freeze from a Slurpee was bad 2 u Hypothermia u Hypo, meaning under, less than, beneath u Thermia meaning
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
2016 Top Papers in Critical Care
 2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest. Objectives: U.S. stats
 Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
10/15/ ) Discuss changes in new guidelines for management of acute ischemic stroke patients.
 Discuss changes in new guidelines for management of acute ischemic stroke patients.") 1) Discuss changes in new guidelines for management of acute ischemic stroke patients. Ischemic Stroke Care Erin Brinser, CRNP 2) Evaluate management techniques of complex stroke care. 3) Present current
1) Discuss changes in new guidelines for management of acute ischemic stroke patients. Ischemic Stroke Care Erin Brinser, CRNP 2) Evaluate management techniques of complex stroke care. 3) Present current
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
CEREBROVASCULAR ACCIDENT (CVA)
") Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
CARES Targeted Temperature Management (TTM) Module
 Module") CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia for acute ischaemic stroke An ischaemic stroke happens
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of therapeutic hypothermia for acute ischaemic stroke An ischaemic stroke happens
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care
 Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Therapeutic Hypothermia after Resuscitated Cardiac Arrest
 Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial
 Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial Jiang He, Yonghong Zhang, Tan Xu, Weijun Tong, Shaoyan Zhang, Chung-Shiuan Chen, Qi Zhao, Jing Chen for CATIS
Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial Jiang He, Yonghong Zhang, Tan Xu, Weijun Tong, Shaoyan Zhang, Chung-Shiuan Chen, Qi Zhao, Jing Chen for CATIS
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association
 POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group
 Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
New Therapeutic Hypothermia Techniques
 New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
13. Surgery for acute stroke 13.2 Surgical referral for decompressive hemicraniectomy Reference Gupta R, Connolly ES, Mayer S et al. Hemicraniectomy for massive middle cerebral artery territory infarction:
Hypothermia Induction Methods
 Hypothermia Induction Methods Advantages and Disadvantages Xia Luo, M.D. Vice President, Clinical Education ZOLL Corporation Targeted Temperature Management (TTM) Temperature is one of the four vital signs
Hypothermia Induction Methods Advantages and Disadvantages Xia Luo, M.D. Vice President, Clinical Education ZOLL Corporation Targeted Temperature Management (TTM) Temperature is one of the four vital signs
CRS Center for Resuscitation Science
 Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Induced Hypothermia for Cardiac Arrest. Heather Hand RN,CCRN,CNRN,ATCN,LNC
 Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Case Presentation. Cooling. Case Presentation. New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation
 New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of