ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
|
|
|
- Isaac Matthews
- 5 years ago
- Views:
Transcription
1 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
2
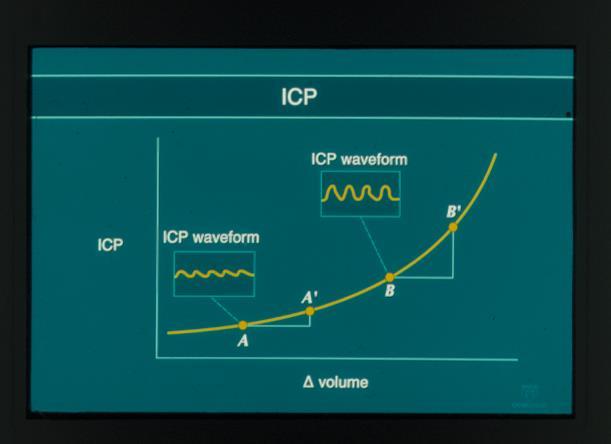
3 ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume 3 components of intracranial volume Normal ICP 20 cm H20 15 mm Hg CSF 150 ml Blood 150 ml Parenchyma 1200 ml
4 Causes of Increased ICP: Space Occupying Lesion Increased CSF Inc. Blood Volume (Vasogenic edema) Inc. Brain Volume (Cytotoxic edema) Hematoma, Tumor, Abscess Hydrocephalus Trauma, Tumor, Abcess, Hypertensive encephalopathy Infarction, Ischemia
5 Methods to Reduce Elevated ICP Remove Mass Lesion Surgical Evacuation Reduce CSF Volume Ventricular Drainage Reduce Cerebral Blood Volume Reduce Parenchymal Volume Hyperventiation, Barbiturates, Hypothermia Osmotic Diuretics (Mannitol, Hypertonic Saline)
6
7
8 Cerebral Blood Flow (ml/100 g/min) ICP (mm Hg) CPP can influence ICP when you run out of room Passive Collapse Maximum Dilatation Zone of Normal Autoregulation Maximum Constriction GOAL Cerebral Perfusion Pressure (mm Hg)) Stephan A. Mayer, MD
9 Cerebral Blood Flow (ml/100 g/min) ICP (mm Hg) CPP can influence ICP when you run out of room Passive Collapse Vasodilatory Cascade Zone Maximum Dilatation Zone of Normal Autoregulation Autoregulation Breakthrough Zone Maximum Constriction GOAL Cerebral Perfusion Pressure (mm Hg)) Stephan A. Mayer, MD
10 Post neurological outcome % Post neurological outcome % Early neurological deterioration % Early neurological deterioration % Outcome after Acute Ischemic Stroke by A Admission Blood Pressure n = 18 n = 29 < n = n = n = Systolic BP on admission (mm Hg) n = 87 > 200 B Castillo J, et al. Stroke. 2004;35: n = 38 < 70 n = n = n = n = Diastolic BP on admission (mm Hg) n = 102 > 110 C n = 18 n = 29 < n = n = n = n = 87 > D n = 38 < 70 n = n = n = n = n = 102 > 110 Systolic BP on admission (mm Hg) Diastolic BP on admission (mm Hg)
 and clonidine (.5 mcg/kg prn) Dihydroergotamine.1-.")
11 Lund protocol Reduce CMRO 2 with sedation Miazolam, thiopental, fentanyl Reduce BP and capillary hydrostatic pressure (CPP mm Hg) IV Metoprolol (.2 mg/kg/hr) and clonidine (.5 mcg/kg prn) Dihydroergotamine.1-.8 mcg/kg/hr Maintain normal hematocritt, CVP, and albumin levels

12 MMM: Imaging Vasodilatory Cascade Physiology MAP GOAL

13 MMM: Imaging Perfusion Pressure Breakthrough Physiology MAP GOAL
14 Indications for ICP Monitoring Coma (Glasgow Coma Scale score 8) CT evidence of intracranial mass effect Extra-axial mass lesion Midline shift Effacement of basal cisterns Exception: severe TBI with motor posturing Prognosis is such that aggressive ICU care is warranted
15 Clinical Signs Increased ICP Depressed level of consciousness Pressor response Projectile vomiting CN 6 palsies Brainstem herniation CN 3 palsey Motor posturing Lower extremity rigidity Loss of lateral EOMs Hyperventilation

16 Ventricular catheter Epidural Monitor Parenchymal Micosensor Richmond Bolt
17 ICP/CPP Treatment Thresholds Guideline ICP treatment should be initiated at an upper threshold of 20 mm Hg. Option Cerebral Perfusion Pressure should be maintained at a minimum of 60 mm Hg.
18 Emergency Treatment of Increased ICP Un-monitored patient with clinical signs of herniation Elevate head of bed 30 Normal saline 100 ml/hr Intubate and hyperventilate (pco2 30 mm Hg) Mannitol 20% 1.0 to 1.5 g/kg rapid IV infusion Foley catheter CT scan and neurosurgical evaluation
 Consider Repeating CT Scan YES YES Intracranial Hypertension? Mannitol (0.25-1.0 g/kg IV) Intracranial Hypertension?")
19 Critical Pathway for Treatment of Intracranial Hypertension in the Severe Head Injury Patient (Treatment Option) Insert ICP Monitor Maintain CPP 70 mmhg YES Intracranial Hypertension?* NO Ventricular Drainage (if available) Consider Repeating CT Scan YES YES Intracranial Hypertension? Mannitol ( g/kg IV) Intracranial Hypertension? NO NO May Repeat Mannitol if Serum Osmolarity < 320 mosm/l & Pt euvolemic Carefully Withdraw ICP Treatment Hyperventilation to PaCO mmhg YES Intracranial Hypertension? NO Other Second Tier Therapies High Dose Barbiturate therapy Hyperventilation to PaCO2 < 30 mmhg Monitoring SjO2, AVDO2, and/orcbf Recommended Second Tier Therapy

20 ICP PROTOCOL
21 Columbia Stepwise ICP Protocol CPP OPTIMIZATION SEDATION PENTOBARBITAL HYPERVENTILATION OSMOTHERAPY HYPOTHERMIA SURGICAL DECOMPRESSION

22 Revised Columbia Stepwise ICP Protocol CPP OPTIMIZATION SEDATION HYPOTHERMIA HYPERVENTILATION OSMOTHERAPY PENTOBARBITAL SURGICAL DECOMPRESSION

23 1 3-way stopcock turned off to drainage system transpac positioned at ear level LEVEL drainage bag 100cc syringe of sterile water Ventricular Drainage
24 2 ICU Intravenous sedation Goal is reversibility to allow repeated neurologic assessment Alternatives (in intubated pts): Fentanyl or Remifentanyl Midazolam Propofol» Ultrashort acting» Allows wake-up in 5-15 mins» Reduces ICP, CMRO2» Drawbacks: hypotension, infection




25 HYPOTHERMIA IS PENTOBARBITAL IS Complications of pentobarbital Hypotension Immunosuppression An extra 4 weeks in coma ICU neuromyopathy
26 3 CPP OPTIMIZATION: Dopamine infusion resulting in increased MAP and CPP, and decreased ICP
27 4 Osmotherapy Mannitol 0.25 to 1.5 g/kg IV wide open Dose up to Q1H on an as-needed basis Mechanisms:» Acute dehydrating effect (osmotic gradient across BBB)» Secondary hyperosmolality (diuretic effect)» Reflex vasoconstriction (viscosity effect) Hypertonic Saline Varying concentrations: 3%, 7.5%, 10%, and 23.4% Optimal dosing not known


28 30 ml 23.4% Bullets
29 Effect of Hypertonic Saline in CBF in SAH patients TSENG M-Y, Stroke 2003;34:1389.) 10 poor grade SAH patients 2 ml/kg of 23.5% saline ICP fell 74% CPP rose 27% CBF rose 23% Peak minutes MAP CPP CVR ICP TCD
30 5 Hyperventilation HYPERVENTILATION IS THE MOST RAPID WAY TO REDUCE ICP EXCESSIVE HYPERVENTILATION CAN WORSEN CEREBRAL ISCHEMIA MECHANISM OF ACTION: HYPOCARBIA INDUCES SERUM AND CSF ALKALOSIS ALKALOSIS INDUCES CEREBRAL VASOCONSTRICTION VASOCONSTRICTION REDUCES CEREBRAL BLOOD VOLUME TIME COURSE: ICP IS REDUCED ALMOST IMMEDIATELY PEAK REDUCTION IN 5-10 MINUTES Hyperventilation Can Have Sustained Effects In Patients With Vasodilatory Vasogenic Cerebral Edema
31 6 Hypothermia MECHANISM OF ACTION: PROFOUNDLY REDUCES REDUCES CEREBRAL METABOLISM, AND HENCE CEREBRAL BLOOD VOLUME TARGET C INDICATION PENTOBARBITAL-REFRACTORY ICP COMPLICATIONS: ARRYTHMIA AND CARDIOVASCULAR DEPRESSION IMMUNOSUPPRESSION COAGULOPATHY METABOLIC: SHIVERING AND REWARMING
32 HYPOTHERMIA FOR ICP CONTROL: TRAUMATIC BRAIN INJURY Shiozaki (J Neurosurg 1993) Randomized controlled study of hypothermia (34 C) for ICP refractory to pentobarbital (N=33). Hypothermia resulted in:»lower ICP (36.9 to 26.5 mm Hg)»Increased CPP»Reduced CBF and CMRO2»Reduced arteriojugular venous oxygen differences Survival was 50% in hypothermia patients compared to 18% in the control group (P<.05).
33
34 6 SECOND TIER Step Up HYPOTHERMIA TO TARGET 35 C THIRD TIER Advance as Needed HYPOTHERMIA TO TARGET 33 C 4 5 HYPERVENTILATION (HV) TO pco mm Hg BOLUS OSMOTHERAPY TO SERUM OSMS <320 MMM-GUIDED HV <30 mm Hg and/or THAM BOLUS OSMOTHERAPY TO SERUM OSMS >320 3 SEDATION to RASS -4 to -5 (Quiet, Motionless State) PARALYSIS and/or BARBITURATES 2 TARGET CPP mm Hg MMM-GUIDED CPP OPTIMIZATION 1 CSF DRAINAGE and/or RESCUE CRANIOTOMY HEMICRANIECTOMY or SALVAGE CRANIOTOMY
35 3 4 5 SECOND TIER 6 HYPOTHERMIA TO TARGET 35 C HYPERVENTILATION (HV) TO pco mm Hg BOLUS OSMOTHERAPY TO SERUM OSMS <320 SEDATION to RASS -4 to -5 (Quiet, Motionless State) Advance first-tier ICP interventions in stepwise fashion to avoid missing essential steps 2 TARGET CPP mm Hg 1 CSF DRAINAGE and/or RESCUE CRANIOTOMY
36 Advance second-tier ICP interventions as needed to fit available resources and the clinical situation THIRD TIER HYPOTHERMIA TO TARGET 33 C MMM-GUIDED HV <30 mm Hg or THAM BOLUS OSMOTHERAPY TO SERUM OSMS >320 PARALYSIS and/or BARBITURATES MMM-GUIDED CPP OPTIMIZATION HEMICRANIECTOMY or SALVAGE CRANIOTOMY
37 Three very bad options for a very bad situation: medically refractory ICP! THIRD TIER HYPOTHERMIA TO TARGET 33 C MMM-GUIDED HV <30 mm Hg or THAM BOLUS OSMOTHERAPY TO SERUM OSMS >320 PARALYSIS and/or BARBITURATES MMM-GUIDED CPP OPTIMIZATION HEMICRANIECTOMY or SALVAGE CRANIOTOMY
38 What About the Latest Trials?

39 BEST-TRIP TRIAL
40 BEST-TRIP TRIAL 324 patients 13 years of age or older with severe TBI in Bolivia or Ecuador Protocol treating ICP based on ICP monitoring Protocol for treating ICP based on standing therapy, imaging and clinical examination Six-month mortality was 39% in the pressuremonitoring group and 41% in the imaging clinical examination group (P = 0.60). Median length of stay in the ICU was similar in the two groups
41 BEST-TRIP TRIAL Number of days of brain-specific treatments (e.g., administration of hyperosmolar fluids and the use of hyperventilation) in the ICU was higher in the imaging clinical examination group than in the pressure-monitoring group (4.8 vs. 3.4, P = 0.002). Serious adverse events was similar in the two groups.
42 BEST-TRIP Conclusion For patients with severe traumatic brain injury, care focused on maintaining monitored intracranial pressure at 20 mm Hg or less was not shown to be superior to care based on imaging and clinical examination.
43 Survival at 14 days MUCH better with ICP monitoring!
44 Survival at 14 days better with ICP monitoring
45
46


47 Aneurysmal SAH with associated suddural hematoma and bilateral motor posturing
48 DECRA 155 TBI patients Early bifrontal craniectomy vfersus standard care Surgical group had Lower ICPs Fewer ICP interventions Fewer ICU days WORSE outcomes despite similar mortality
49
50 DEAD FULL RECOVERY



51 Communicating hydrocephalus is an almost universal finding in patients after hemicraniectomy
52
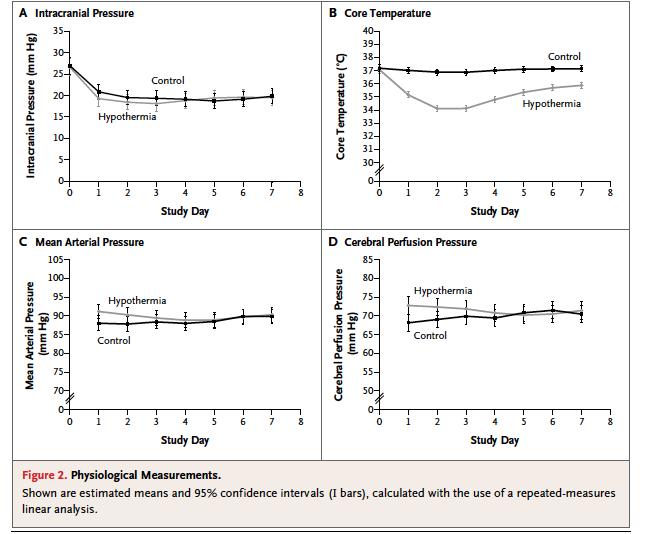
53 EUROTHERM severe TBI patients Randomization trigger: first episode of ICP >20 mm Hg Hypothermia group Died more Less likely to survive with good outcome 26% vs 37% Cause of this worse outcome is unclear
54
55
56 RESCUEicp Trial
57 Conclusion When the going gets tough, when ICP is medically refractory, easy options are hard to find All three THIRD TIER options likely cause harm when performed early without a trial of ICU care Prophylactic barbiturate coma Straight to the OR for hemicraniectomy Cool to C at the first sign of ICP elevation My preference for definitive salvage intervention when ICU care is failing go to the OR
58 RESCUEicp Trial 408 severe TBI patients Age Randomization trigger: Medically refractory ICP >25 mm Hg for 1-12 hours Time to randomization >72 hours after injury in 45% Hemicraniectomy group Absolute 22% reduction in mortality Better ICP control: 5 vs 17 hours with ICP >25 mm Hg More complications (mostly surgical related): 16% vs 9%

59 RESCUEicp Trial: Craniectomy vs Barbiturates

60 Rescue Hemicraniectomy Creates a 22% chance of converting death to survival in a vegetative state or with severe disability
61 4 5 6 SECOND TIER HYPOTHERMIA TO TARGET 35 C HYPERVENTILATION (HV) TO pco mm Hg BOLUS OSMOTHERAPY TO SERUM OSMS <320 Advance first-tier ICP interventions in stepwise fashion to avoid missing essential steps 3 SEDATION to RASS -4 to -5 (Quiet, Motionless State) 2 TARGET CPP mm Hg 1 CSF DRAINAGE and/or RESCUE CRANIOTOMY
62 SECOND TIER THIRD TIER HYPOTHERMIA to 35 C Option: TARGET 33 C HYPERVENTILATION (HV) Option: MMM-Guided HV <30 BOLUS OSMOTHERAPY Option: PUSH OSMS >320 SEDATION to RASS -4 to -5 Option: ADD PARALYTICS TARGET CPP to mm Hg Option: MMM-TARGETED CPP Ultimately, once you realize that you are losing the battle, there is really only one effective third tier therapy for ICP: pop the lid! 1 CSF DRAINAGE and/or RESCUE CRANIOTOMY HEMICRANIECTOMY or SALVAGE CRANIOTOMY


63 Neurocritical Care Society
ICP. A Stepwise Protocol
 ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
11 th Annual Cerebrovascular Symposium 5/11-12/2017. Hypertonic Use D E R E K C L A R K
 Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Decompressive craniectomy following traumatic brain injury
 Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS
 Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS The intracranial compartment consists of predominantly brain parenchyma
Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS The intracranial compartment consists of predominantly brain parenchyma
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along?
 Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along? Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this
Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along? Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury
 Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Raised Intracranial Pressure (ICP): Management in Emergency Department
: Management in Emergency Department") Raised Intracranial Pressure (ICP): Management in Emergency Department Author: Dr. Shruti Sangani*, Dr. Samira Parikh** INTRODUCTION: Elevated intracranial pressure (ICP) is a potentially devastating complication
Raised Intracranial Pressure (ICP): Management in Emergency Department Author: Dr. Shruti Sangani*, Dr. Samira Parikh** INTRODUCTION: Elevated intracranial pressure (ICP) is a potentially devastating complication
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Retired Brigadier of the Croatian Army (HV), War Commander of the Surgical Team of the Croatian Ministry of Internal Affairs (MUP) Special Police 2
, War Commander of the Surgical Team of the Croatian Ministry of Internal Affairs (MUP) Special Police 2") Acta Chir Croat 0; 9: 9-5 Ozljede glave Running head: Head injuries Josip Husar, Israel Oserohwovo Introduction The prognosis of brain injuries is good in patients who respond to simple commands, are not
Acta Chir Croat 0; 9: 9-5 Ozljede glave Running head: Head injuries Josip Husar, Israel Oserohwovo Introduction The prognosis of brain injuries is good in patients who respond to simple commands, are not
Proceedings of the Southern European Veterinary Conference - SEVC -
 www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 29-Oct. 2, 2011, Barcelona, Spain Next SEVC Conference: Oct. 18-21, 2012 - Barcelona, Spain Reprinted in the IVIS website
www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 29-Oct. 2, 2011, Barcelona, Spain Next SEVC Conference: Oct. 18-21, 2012 - Barcelona, Spain Reprinted in the IVIS website
Emergency Management of the Head
 Emergency Management of the Head Trauma Patient Adam Schneider, DVM Neurology and Neurosurgery Blue Pearl 9500 Marketplace Rd Fort Myers Head trauma Common cause of morbidity and mortality 25% of blunt
Emergency Management of the Head Trauma Patient Adam Schneider, DVM Neurology and Neurosurgery Blue Pearl 9500 Marketplace Rd Fort Myers Head trauma Common cause of morbidity and mortality 25% of blunt
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
The Lund Concept in 1999
 The Lund Concept in 1999 Carl-Henrik Nordström, M.D., Ph.D. Department of Neurosurgery Lund University Hospital S-221 85 Lund Sweden A new therapeutic approach to reduce increased ICP, denoted the Lund
The Lund Concept in 1999 Carl-Henrik Nordström, M.D., Ph.D. Department of Neurosurgery Lund University Hospital S-221 85 Lund Sweden A new therapeutic approach to reduce increased ICP, denoted the Lund
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Reducing intracranial pressure in patients with traumatic brain injury
 Reducing intracranial pressure in patients with traumatic brain injury Learn how to identify rising intracranial pressure early to promote appropriate interventions. By Cindy L. Zerfoss, MSN, RN, ACNP-CS
Reducing intracranial pressure in patients with traumatic brain injury Learn how to identify rising intracranial pressure early to promote appropriate interventions. By Cindy L. Zerfoss, MSN, RN, ACNP-CS
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Critical Care Management of Acute Ischemic Stroke
 Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
THREE HUNDRED AND ten TBI patients with a
 Acute Medicine & Surgery 2014; 1: 31 36 doi: 10.1002/ams2.5 Original Article Outcome prediction model for severe traumatic brain injury Jiro Iba, 1 Osamu Tasaki, 2 Tomohito Hirao, 2 Tomoyoshi Mohri, 3
Acute Medicine & Surgery 2014; 1: 31 36 doi: 10.1002/ams2.5 Original Article Outcome prediction model for severe traumatic brain injury Jiro Iba, 1 Osamu Tasaki, 2 Tomohito Hirao, 2 Tomoyoshi Mohri, 3
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury
 J Med Dent Sci 2010; 57: 133-138 Original Article Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury Hiroyuki Masaoka Department of Neurosurgery,
J Med Dent Sci 2010; 57: 133-138 Original Article Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury Hiroyuki Masaoka Department of Neurosurgery,
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency
 Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery
 Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP?
 7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
Traumatic Brain Injury Protocol
 Traumatic Brain Injury Protocol Section 1. Pre-PICU Management Sources: Guidelines for Pre-Hospital Management of Traumatic Brain Injury 2000: BrainTrauma Foundation New York. Recommendations for the Transfer
Traumatic Brain Injury Protocol Section 1. Pre-PICU Management Sources: Guidelines for Pre-Hospital Management of Traumatic Brain Injury 2000: BrainTrauma Foundation New York. Recommendations for the Transfer
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)