Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
|
|
|
- Virginia Cannon
- 6 years ago
- Views:
Transcription

1 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
2 Background 30% of patients have history of hypertension prior to stroke 80% will present with elevated B/P In normotensive patients, cerebral blood flow is maintained over a wide range of MAP mm Hg Chronically hypertensive patients require higher MAP to maintain normal cerebral blood flow
3 Mental Stress Long standing chronic hypertension Impaired Neurogenic CV Control Autonomic Dysregulation Elevated B/P Pain Reflex Response to Cerebral Ischemia Baroreflex Failure Increased Sympathetic Drive Increased ICP
4 A major component of stroke care should focus upon strategies to limit neurological damage within the ischemic penumbra by controlling abnormal physiology
5 What is Cerebral Autoregulation? Mechanism by which cerebral blood flow (CBF) remains constant across a wide range of cerebral perfusion pressures (CPP) Reflex vasoconstriction or vasodilation of the cerebral arterioles in response to changes in perfusion pressure If ICP is constant and not elevated, MAP and CPP are proportional
6
7 Eames and Colleagues Evidence shows that autoregulation is impaired in stroke patients Global impairment in dynamic autoregulation found in all stroke patients but not in controls Dysfunction occurred in both hemispheres
8 Cerebral Blood Flow Cerebral blood flow is dependent on systemic blood pressure systemic blood pressure = cerebral blood flow = perfusion = neuronal death When cerebral blood flow is less than 12ml/100 g/min, neuronal death is likely to occur
9 Cerebral Blood Flow Not homogenous in the area of infarction Critical threshold below which neurons cease to function May continue to survive for a short time May return to normal functional state if blood flow is restored Time period for reversal may be first several hours May depend on the location of the occlusion, rapidity of occlusion, adequacy of collateral blood flow

10 Cerebral Blood Flow
11 What does research show? Contradictory results Some show association of poor outcomes in patients who are hypertensive on admission Others note decreased risk of deterioration from stroke with higher B/P and worse outcomes in those patients whose B/P is decreased after admission Does higher B/P reflect greater stroke severity rather than causing worse outcomes?
12 What does the research show? Patients with lacunar or large artery atheroembolic /cardioembolic strokes had better outcomes when B/P was higher U-shaped relationship between B/P and mortality Very low or high admission B/P linked to poor outcomes
13 Minnesota Project Lit Review 3 sets of guidelines related to B/P management in the acute phase AHA/ASA ISH (International Society of Hypertension) EUSI (European Stroke Initiative) AHA/ASA and ISH guidelines are identical
14 Summery of Guidelines ASA guideline: Treat cautiously and only when systolic BP (SBP) >220 mm Hg or diastolic BP (DBP) >120 mm Hg or mean BP >130 mm Hg. EUSI guideline: Treatment is to be withheld unless SBP >180 mm Hg or DBP >105mm Hg at the least, although higher thresholds are acceptable.
15
16 Barriers No clear time window for leaving B/P elevated Potential Exceptions Hypertensive encephalopathy Aortic dissection Acute MI Acute renal failure Acute pulmonary edema B/P control in post-acute period is not addressed in guidelines Timing for resumption of prestroke regimen ignored
17 A delicate balance Low CPP Ischemia Occurs High CPP Increased ICP Increased Intracranial Blood Volume Vasogenic Edema
18 Factors to Consider Type of Neurovascular Injury Level of hypertension Blood Pressure History Perceived condition of native autoregulatory system
19 Kathy start Applying this evidence and knowledge
20 Why Do We Treat HTN? Reduce formation of brain edema Reduce risk of hemorrhagic transformation Prevent further vascular damage Aggressive lowering of BP can cause a reduction of perfusion in the ischemic zone, which may expand the region of infarction
21 Basic Points Don t treat isolated BP Always recheck value prior to treating BP Too High What is the cause? Antihypertensives Too Low What is the cause? Fluid Boluses, vasopressors
22 Mental Stress Autonomic Dysregulation Anger frustration Agitation Overstimulation confusion Long standing chronic hypertension fear Elevated B/P Foley ET tube Impaired Neurogenic CV Control EVD IV Pain crani SCDs HA Reflex Response to Cerebral Ischemia Baroreflex Failure Increased Sympathetic Drive Increased ICP
23 Titratable Anti-Hypertensives DRUG MECHANISM DOSE ONSET Nicardipine L-type CCB (dihydropyridine) 5-15 mg/h infusion 5-10 min Labetalol α 1 β 1 β 2 antagonist mg bolus q 10min; max 300 mg; mg/min infusion Esmolol β 1 antagonist 500 μg/kg bolus; μg/kg/min infusion Enalaprilat Ace Inhibitor mg bolus, then mg q 6h 5-10 min 1-2 min min

24 Provider Practice Fear of letting B/P run high End organ damage ICH More comfortable with low BP Patient looks fine
25 Challenges Case load how to manage increased work load of frequent monitoring of BP with aggressive treatment regimen Other causes of high or low BP Time required to ferret out the specific cause and take action Level of care change for aggressive BP management Patients being moved from one area to another Clarity of orders what do they mean? MAP vs SBP Provider doesn t take action when notified of BP outside of range
26 Challenges Standards for ischemic different from hemorrhagic management HOB elevation Acceptable high/low ranges Evidence suggests age-related differences in outcomes at 3 months SBP reductions >27 mmhg within first 8 hours Poor outcomes likelihood: 6x greater age 70-76; 10x greater age 76-80; 15x greater >age 80 SBP reductions mmhg better outcomes until age >76 years
27 Challenges HOB recommendations related to recanalization Incomplete recanalization pts should have HOB 0 Increases mean flow velocity Complete recanalization pts should have HOB 30 Variability of BP management Higher variability at 72 hours shown to increase risk of death or dependent outcomes Co-medication of antihypertensive agents associated with unfavorable outcomes (ECASS-II)
28 Challenges Tough to link BP mismanagement with outcomes Tough to get acute care nurses to appreciate that the results of their actions may only be evident months after discharge
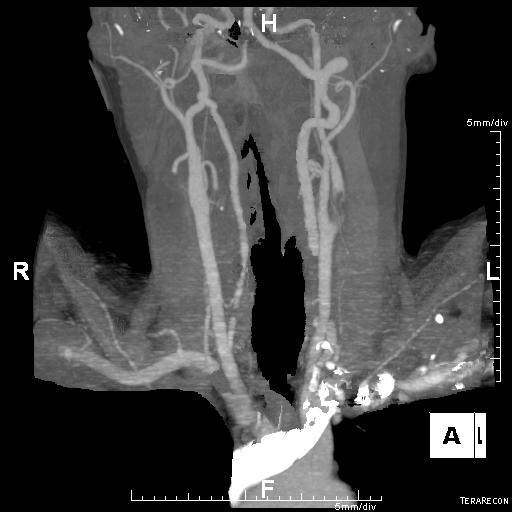
29 Case Review: Q TW is a 33year old female transferred in with right hemiplegia Patient was evaluated via LionNet telestroke NIHSS was 17 on arrival to ED Patient restless Intubated and sedated to complete CTA
30 Case Review CTA showed large perfusion defect in left MCA territory without evidence of penumbra Plan for hypothermia Goal temp 35 C MAP goals

31 Case Review
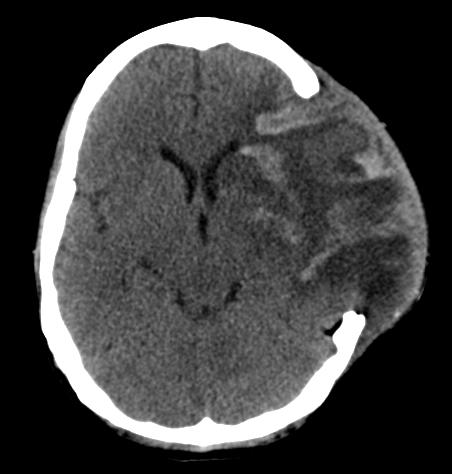
32 Case Review 1.8% NaCl started for cerebral edema MRI showed hemorrhagic conversion of left MCA infarct Patient went to OR for decompressive hemicraniectomy on Day #2 Post-op, hypothermia continued through Day #3

33 Case Review
34 Case Review Discharged to Acute Rehab on Day #13 NIHSS was 15 on discharge NIHSS at 90 day visit was 14 Living at home with mother s help

35 Post-op hemicraniectomy Albumin 250mg x 2 Dobutamine Norepinephrine MRI

36 Management of BP A Delicate Balance Hypertension may promote hemorrhage Treating hypertension may exacerbate ischemia
37 So what do we do now? Throw our hands up and stomp our feet Recognize that BP control is within our scope of practice Be/become familiar with medications Know your patient s specific orders for BP management Commit to monitoring and responding to your patient s BP

38 The ultimate endpoint Limiting neurological damage within the ischemic penumbra by controlling abnormal physiology save the brain.
39 References Bhalla, A., Wolfe, Rudd, A.G. (2001). Management of acute physiological parameters after stroke. QJM, 2001 (94), Lakshminarayan, K., Anderson, D.C., Borbas, C., Duval, S. & Luepoker, L.V. (2007). Blood pressure management in acute ischemic stroke. Journal of Clinical Hypertension, 9 (6), Caulfield, A. & Wijman, C. (2008). Management of Acute Ischemic Stroke. Neurologic Clinics, (26), Goldstein, L.B. (2004). Blood Pressure Management in Patients with Acute Ischemic Stroke. Hypertension (43), Semplicini, A. & Calo, L. (2005). Administering antihypertensive drugs after acute ischemic stroke: timing is everything. CMAJ, 172 (5), Urrutia, V.C. & Wityk, R.J. (2007). Blood Pressure Management in Acute Stroke. Critical Care Cinics, 22,
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Hypertensive Crises. Controlling high blood pressure prevents disease. Recognition and Management of Acute Hypertensive Emergencies
 Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE
 BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Children with Hypertension in ED
 Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Critical Care Management of Acute Ischemic Stroke
 Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
Acute Stroke Treatment Update for 2008
 Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Brain under pressure Impact of vasopressors
 Brain under pressure Impact of vasopressors Brain dysfunction in sepsis Incidence: - Varying nomenclature: sepsis-associated encephalopathy, delirium, brain dysfunction - Consistently recognized as frequent:
Brain under pressure Impact of vasopressors Brain dysfunction in sepsis Incidence: - Varying nomenclature: sepsis-associated encephalopathy, delirium, brain dysfunction - Consistently recognized as frequent:
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Hemorrhage. Dr. Al Jin Nov. 17, 2015
 Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
ACUTE STROKE MANAGEMENT
 ACUTE STROKE MANAGEMENT. Before the Specialist Arrives C A R L O S L C H U A, M D, F P N A UP- P H I L I P P I N E G E N E R A L H O S P I T A L P R E S I D E N T, S T R O K E S O C I E T Y O F T H E P
ACUTE STROKE MANAGEMENT. Before the Specialist Arrives C A R L O S L C H U A, M D, F P N A UP- P H I L I P P I N E G E N E R A L H O S P I T A L P R E S I D E N T, S T R O K E S O C I E T Y O F T H E P
Part I. Acute Management of Neurological Emergencies COPYRIGHTED MATERIAL
 Part I Acute Management of Neurological Emergencies COPYRIGHTED MATERIAL 1 Hypertensive Emergency Laurie McWilliams Neurocritical Care Unit, Cerebrovascular Center, Department of Neurology and Neurosurgery,
Part I Acute Management of Neurological Emergencies COPYRIGHTED MATERIAL 1 Hypertensive Emergency Laurie McWilliams Neurocritical Care Unit, Cerebrovascular Center, Department of Neurology and Neurosurgery,
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Franklin Delano Roosevelt. Learning Objectives. Severe hypertension is relatively common. Current State of Hypertensive Crisis Management
 3 3:45 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know about Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related to
3 3:45 pm Presenter Disclosure Information What Every Primary Care Clinician Needs to Know about Hypertension Crises SPEAKER Karol E. Watson, MD, PhD, FACC The following relationships exist related to
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium
 CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Objectives: HYPERTENSIVE EMERGENCIES:
 HYPERTENSIVE EMERGENCIES: Acute Care Evaluation and Management Charles V. Pollack, Jr., MD Christopher J. Rees, MD Department of Emergency Medicine, Pennsylvania Hospital University of Pennsylvania, Philadelphia,
HYPERTENSIVE EMERGENCIES: Acute Care Evaluation and Management Charles V. Pollack, Jr., MD Christopher J. Rees, MD Department of Emergency Medicine, Pennsylvania Hospital University of Pennsylvania, Philadelphia,
Agenda. Management of Accelerated Hypertension (Updated in 2017) Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017
 Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017") Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Prevention and Management of hypertensive stroke. Content. What are the clinical and radiological manifestations for HT-related stroke?
 Prevention and Management of hypertensive stroke Dr. LO, Man-wai MBChB (CUHK) MRCP (UK) MPH (CUHK) FHKCP FHKAM (Medicine) Specialist in Neurology Dept. of Medicine Queen Elizabeth Hospital 4 Dec 2006 Content
Prevention and Management of hypertensive stroke Dr. LO, Man-wai MBChB (CUHK) MRCP (UK) MPH (CUHK) FHKCP FHKAM (Medicine) Specialist in Neurology Dept. of Medicine Queen Elizabeth Hospital 4 Dec 2006 Content
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial
 Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial Jiang He, Yonghong Zhang, Tan Xu, Weijun Tong, Shaoyan Zhang, Chung-Shiuan Chen, Qi Zhao, Jing Chen for CATIS
Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial Jiang He, Yonghong Zhang, Tan Xu, Weijun Tong, Shaoyan Zhang, Chung-Shiuan Chen, Qi Zhao, Jing Chen for CATIS
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Non Categorized SUB Sub Phase (SUB)* Non Categorized Quality Measures STK Diet ED NPO Until Bedside Swallow Screen passed Nursing Orders Activate Code Stroke Vital Signs Q15MINS Int
DRUG AND TREATMENT Non Categorized SUB Sub Phase (SUB)* Non Categorized Quality Measures STK Diet ED NPO Until Bedside Swallow Screen passed Nursing Orders Activate Code Stroke Vital Signs Q15MINS Int
Cold Topic: Advanced Treatment Modalities in Acute Stroke
 Cold Topic: Advanced Treatment Modalities in Acute Stroke William M. Coplin, MD, FCCM Associate Prof, Neurology & Neurosurgery Wayne State University Chief, Neurology Medical Director, Neurotrauma & Critical
Cold Topic: Advanced Treatment Modalities in Acute Stroke William M. Coplin, MD, FCCM Associate Prof, Neurology & Neurosurgery Wayne State University Chief, Neurology Medical Director, Neurotrauma & Critical
CEREBROVASCULAR ACCIDENT (CVA)
") Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Special circulations, Coronary, Pulmonary. Faisal I. Mohammed, MD,PhD
 Special circulations, Coronary, Pulmonary Faisal I. Mohammed, MD,PhD 1 Objectives Describe the control of blood flow to different circulations (Skeletal muscles, pulmonary and coronary) Point out special
Special circulations, Coronary, Pulmonary Faisal I. Mohammed, MD,PhD 1 Objectives Describe the control of blood flow to different circulations (Skeletal muscles, pulmonary and coronary) Point out special
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Hypertension in the ED - management tips that will bring down your own BP
 27th Annual Update in Emergency Medicine Hypertension in the ED - management tips that will bring down your own BP February 24, 2014 Clare Atzema, MD MSc FRCPC Staff Physician, Sunnybrook Health Sciences
27th Annual Update in Emergency Medicine Hypertension in the ED - management tips that will bring down your own BP February 24, 2014 Clare Atzema, MD MSc FRCPC Staff Physician, Sunnybrook Health Sciences