Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
|
|
|
- Milton Hudson
- 6 years ago
- Views:
Transcription
1 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology
2 Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and recovery

3 Head-of-bed position HeadPoST (International Stroke Conference 2017) Designed to compare lying flat vs. sitting up in first 24 hours 11,094 patients with AIS or ICH from 114 centers in 9 countries No difference in functional outcomes at 90 days Median NIHSS score 4 (0-42) Wahlgren et al. Cerebrovasc Dis 1994;4:

4 Blood pressure management Defining the problem: Stroke is heterogeneous. Optimal BP management remains unclear. Should we raise or reduce the BP? What threshold should we use to treat the BP? How long after stroke should we start treatment? How aggressive should the treatment be? Should we stop or continue home antihypertensives?
5 Cerebral autoregulation Maintenance of constant CBF despite changes in CPP CPP = MAP ICP CPP: Cerebral perfusion pressure MAP: Mean arterial pressure ICP: Intracranial pressure CPP and MAP have a linear relationship with slope = 1.
6 Cerebral autoregulation Arteriole diameter Cerebral Blood Flow (ml/100g/min) Cerebral Perfusion Pressure (mm Hg)
7 Cerebral autoregulation Normotension Cerebral Blood Flow (ml/100g/min) min) Cerebral ischemia Chronic hypertension Cerebral Perfusion Pressure (mm Hg)
8 Case 1 56-y.o. woman with smoking and dyslipidemia Diagnosed with hypertension and started on treatment Recurrent right-sided weakness and speech difficulties BP 120/77 mm Hg on arrival
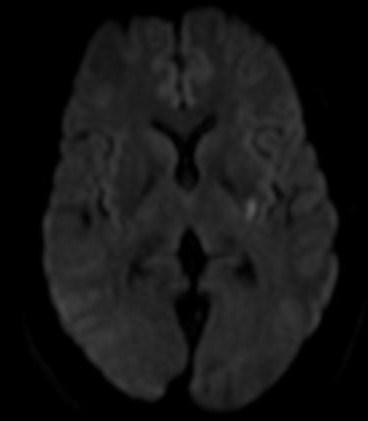
9 Case 1
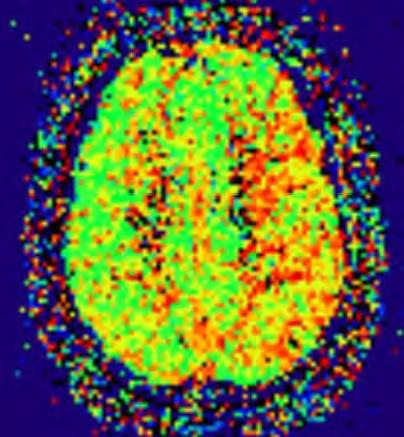
10 Case 1
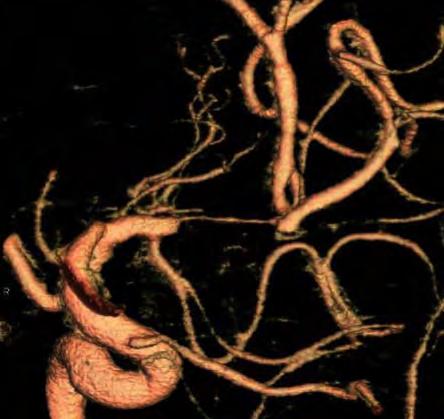
11 Case 1
12 Natural history 3/4 patients present with elevated BP. BP tends to normalize in the first 7 days. 1/3 of patients experience a reduction in first 24 hours. Indirect evidence for poor outcome if BP too high or low. Wallace et al. JAMA 1981;246(19):
13 Observational data IST In first 48 hours, 54% of patients had SBP > 160. U-shaped relationship between BP and mortality Excess mortality 3.8% for every 10 mm Hg above SBP 150 Excess mortality 17.9% for every 10 mm Hg below SBP 150 Leonardi-Bee et al. Stroke 2002;33(5):
14 Empirical data INWEST Designed to test neuroprotective effect of nimodipine in stroke Planned enrollment 600 at 34 centers Patients enrolled within 24 hours of stroke onset Randomized to placebo vs. 1 or 2 mg/hr followed by 30 mg q6h 2 mg/hr group had significantly worse outcomes than placebo. 1 mg/hr group also had worse outcomes, though not significant. Stopped early after enrolling 295 patients Wahlgren et al. Cerebrovasc Dis 1994;4:
15 Empirical data ACCESS Designed to assess safety of 10-15% BP reduction first 24 hrs after acute ischemic stroke Planned enrollment 500 at 53 centers SBP/DBP 200/110 within 6-24 hours, or SBP/DBP 180/105 within hours Randomized to candesartan vs. placebo on day 1 Followed by candesartan +/- other agent(s) on day 7 Stopped early after analysis of 342 randomized patients No difference in BP between groups No difference in functional outcome at 3 months Lower 1-year mortality and event rate in candesartan group Schrader et al. Stroke 2003;34(7):

16 Empirical data CHHIPS Designed to test feasibility, safety, and efficacy of two agents 179 patients with AIS (80%) or ICH (20%) and SBP > 160 Randomized 2:1 to lisinopril, labetalol, or placebo within 36 hours for 14 days All patients placed on ACE inhibitor at 14 days Target SBP , or 15 mm Hg reduction from baseline 21 vs. 11 mm Hg drop in SBP in first 24 hours in treated vs. placebo (p = 0.004) No difference in death or dependency at 2 weeks No early neurologic deterioration or SAE seen with BP reduction Treated group had 50% RRR in mortality at 3 months (p = 0.05). Potter et al. Lancet Neurology 2009;8:48-56.

17 Empirical data COSSACS Designed to test safety and efficacy of stopping or continuing home BP medications 763 patients presenting with AIS (92%) or ICH (8%) Randomized to continue or stop BP medications for 2 weeks Difference of 13 mm Hg in SBP and 8 mm Hg in DBP at 2 weeks (p < ) No difference in death or dependency at 2 weeks No difference in serious adverse events No difference in mortality at 6 months Robinson et al. Lancet Neurology 2010;9:
18 Empirical data SCAST Designed to test effectiveness of BP reduction in acute stroke 2029 patients with AIS (86%) or ICH (14%) and SBP > 140 Randomized to candesartan vs. placebo within 30 hrs for 7 days Primary endpoints: Composite endpoint of vascular death, MI, or stroke at 6 months Functional outcome at 6 months (mrs) Target SBP , or 15 mm Hg reduction from baseline 147/82 vs. 152/84 in candesartan vs. placebo (p < ) No difference in composite vascular outcome at 6 months Higher risk of poor functional outcome at 6 months in candesartan group (OR 1.17, 95% CI , p = 0.048) Sandset et al. Lancet 2011;377:
19 Empirical data Effect of Blood Pressure Lowering in Early Ischemic Stroke Meta-analysis of trials published between 1966 and randomized trials including 12,703 subjects All studies started BP lowering within 3 days of AIS onset Primary outcome: death or dependency at 3 months Secondary outcome: recurrent vascular events Early BP lowering had no effect on primary or secondary outcome Lee et al. Stroke 2015;46(7):
20 Empirical data Induced hypertension: Randomized pilot study 15 patients randomized 2:1 to ihtn vs. standard care Inclusion: AIS 7 days and DWI-PWI mismatch > 20% MAP increased by mm Hg in ihtn arm (max 140 mm Hg) Stopping antihypertensives Administering IV fluids Administering IV phenylephrine Target improvement in NIHSS score 2 NIHSS scores better in ihtn arm, day 3 (5.6 vs. 12.3, p = 0.01). By week 6 to 8, NIHSS scores were 2.8 vs. 9.7 (p < 0.04). No significant adverse events, 6 of 9 treated patients were responders. Hillis et al. Cerebrovasc Dis 2003;16(3):
21 Current guidelines Benefits of treating BP in AIS not well established (Class IIb; Level of Evidence C) If BP markedly elevated, a 15% reduction is reasonable in first 24 hours. Consider treatment for SBP 220, or DBP 110. (Class I; Level of Evidence C) Resuming BP medications in patients with hypertension after 24 hours is reasonable. (Class IIa; Level of Evidence B) No clear evidence for choice of medications to lower BP (Class IIa; Level of Evidence C) Stroke 2013;44:

22 Antiplatelet therapy IST (Lancet 1997) 19,435 randomized within 48 hours to ASA 300 mg vs. avoid ASA for up to 14 days. Primary endpoint: death within 14 days, death or dependency at 6 months. Results: 4 fewer deaths per 1000 at 14 days in ASA group 11 fewer deaths or nonfatal strokes per 1000 at 14 days in ASA group Lower death and disability at 6 months if adjusted for prognosis CAST (Lancet 1997) 21,106 randomized within 48 hours to ASA 160 mg vs. placebo for up to 4 weeks. Primary endpoint: Death or dependence at discharge, or death at 4 weeks. Results: 5.4 fewer deaths per 1000 at 4 weeks in ASA group 9 fewer deaths or nonfatal strokes per 1000 at 4 weeks in ASA group 13 fewer dead or dependent per 1000 at discharge Conclusion: ASA therapy results in about 10 fewer deaths or recurrent strokes per 1000 in first few weeks, so start ASA as soon as possible after acute ischemic stroke.

23 Anticoagulation TOAST (JAMA 1998) 1,281 randomized to ORG vs. placebo for 7 days. No difference in functional outcomes at 30 days. Increased ICH risk (14 vs. 4, p = 0.05), esp. in those with NIHSS score > 15 Subgroup analysis suggested benefit in those with large vessel disease. Heparin for hot carotid hypothesis HAEST (Lancet 2000) 449 with AF randomized within 30 days of AIS to dalteparin vs. ASA 160 mg Primary endpoint: Recurrent ischemic stroke in first 14 days Recurrent stroke occurred in 8.5% of dalteparin vs. 7.5% of ASA group. No difference in symptomatic ICH or functional outcomes at 14 days or 3 months CADISS (Lancet 2015) 250 with cervical ICA or VA dissection randomized to antiplatelet vs. warfarin within 7 days Primary endpoint: Ischemic stroke attributable to dissection, or death No difference in outcomes or adverse events

24 Statin therapy SPARCL (NEJM 2006) 4,731 randomized within 6 months to atorvastatin 80 mg vs. placebo Primary outcome: Recurrent stroke over 5 years Occurred in 11.2% of those on atorvastatin vs. 13.1% on placebo ARR 2.2% and RRR 16% over 5 years LDL reduced to 73 vs. 129 with atorvastatin vs. placebo ASSORT (International Stroke Conference 2017) 257 randomized to statin therapy within 24 hours vs. 7 days Primary endpoint: 90-day disability by mrs Results: No harm or benefit with early initiation Statins used: atorvastatin 20 mg, rosuvastatin 5 mg, pitavastatin 4 mg Conclusion: High-dose, high-potency statin therapy reduces recurrent stroke risk in the long run. Unclear how soon statin therapy needs to be started after ischemic stroke, but starting immediately does not appear to confer significant risk at 90 days.

25 Rehabilitation and recovery FLAME (Lancet 2011) 118 with AIS randomized within 5-10 days to 90-day course of fluoxetine 20 mg vs. placebo Primary outcome: Change in FMMS score over 90 days Improvement of 34.0 vs points (p = 0.003) in FMMS score in fluoxetine group More depression in placebo group AVERT (Lancet 2015) 2,014 with AIS and ICH randomized to frequent, higher-dose, very early mobilization (within 24 hours) vs. usual stroke unit care Primary endpoint: mrs score 2 at 3 months 92% vs. 59% mobilized within 24 hours in VEM vs. usual care group Median time to mobilization 18.5 vs hours in VEM vs. usual care group Fewer favorable outcomes in VEM group at 3 months (46% vs. 50%, p = 0.004)
26 Summary Head of bed elevation probably harmless unless exam position-dependent. With blood pressure and AIS, one size does not fit all. Start antiplatelet and statin therapy as soon as possible. No role for acute anticoagulation in most cases. Consider fluoxetine in patients with severe hemiparesis. Very early and aggressive mobilization may be harmful.
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE
 BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
The Effect of Statin Therapy on Risk of Intracranial Hemorrhage
 The Effect of Statin Therapy on Risk of Intracranial Hemorrhage JENNIFER HANIFY, PHARM.D. PGY2 CRITICAL CARE RESIDENT UF HEALTH JACKSONVILLE JANUARY 23 RD 2016 Objectives Review benefits of statin therapy
The Effect of Statin Therapy on Risk of Intracranial Hemorrhage JENNIFER HANIFY, PHARM.D. PGY2 CRITICAL CARE RESIDENT UF HEALTH JACKSONVILLE JANUARY 23 RD 2016 Objectives Review benefits of statin therapy
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
The Impact of Smoking on Acute Ischemic Stroke
 Smoking The Impact of Smoking on Acute Ischemic Stroke Wei-Chieh Weng, M.D. Department of Neurology, Chang-Gung Memorial Hospital, Kee-Lung, Taiwan Smoking related mortality Atherosclerotic vascular disease
Smoking The Impact of Smoking on Acute Ischemic Stroke Wei-Chieh Weng, M.D. Department of Neurology, Chang-Gung Memorial Hospital, Kee-Lung, Taiwan Smoking related mortality Atherosclerotic vascular disease
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Hemorrhage. Dr. Al Jin Nov. 17, 2015
 Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Updates from 2017 International Stroke Conferences
 Updates from 2017 International Stroke Conferences Ravi Menon, MD Swedish Neuroscience Institute May 11, 2017 Seattle, WA 1 Disclosures No relevant financial disclosures Clinical trial involvement: Former
Updates from 2017 International Stroke Conferences Ravi Menon, MD Swedish Neuroscience Institute May 11, 2017 Seattle, WA 1 Disclosures No relevant financial disclosures Clinical trial involvement: Former
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Treatment Update for 2008
 Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Best Medical Therapy for asymptomatic carotid disease
 Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Early mobilization after stroke What do we know (so far)?
?") NICIS Neurosciences in Critical Care International Symposium 19 th June, 2015 Early mobilization after stroke What do we know (so far)? Peter Langhorne, Professor of stroke care, Glasgow University Acknowledgements
NICIS Neurosciences in Critical Care International Symposium 19 th June, 2015 Early mobilization after stroke What do we know (so far)? Peter Langhorne, Professor of stroke care, Glasgow University Acknowledgements
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
ACUTE STROKE MANAGEMENT
 ACUTE STROKE MANAGEMENT. Before the Specialist Arrives C A R L O S L C H U A, M D, F P N A UP- P H I L I P P I N E G E N E R A L H O S P I T A L P R E S I D E N T, S T R O K E S O C I E T Y O F T H E P
ACUTE STROKE MANAGEMENT. Before the Specialist Arrives C A R L O S L C H U A, M D, F P N A UP- P H I L I P P I N E G E N E R A L H O S P I T A L P R E S I D E N T, S T R O K E S O C I E T Y O F T H E P
AVERT Trial Debate: Implications for Practice Have we AVERT ed the real message?
 AVERT Trial Debate: Implications for Practice Have we AVERT ed the real message? Jackie Bosch, PhD, OT Reg(Ont) School of Rehabilitation Science McMaster University Vince DePaul PT PhD School of Rehabilitation
AVERT Trial Debate: Implications for Practice Have we AVERT ed the real message? Jackie Bosch, PhD, OT Reg(Ont) School of Rehabilitation Science McMaster University Vince DePaul PT PhD School of Rehabilitation
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Review Article Unsolved Issues in the Management of High Blood Pressure in Acute Ischemic Stroke
 International Hypertension Volume 2013, Article ID 349782, 5 pages http://dx.doi.org/10.1155/2013/349782 Review Article Unsolved Issues in the Management of High Blood Pressure in Acute Ischemic Stroke
International Hypertension Volume 2013, Article ID 349782, 5 pages http://dx.doi.org/10.1155/2013/349782 Review Article Unsolved Issues in the Management of High Blood Pressure in Acute Ischemic Stroke
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO
 La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
김광일 서울대학교의과대학내과학교실 분당서울대학교병원내과
 치매예방을위한만성질환관리전략 김광일 서울대학교의과대학내과학교실 분당서울대학교병원내과 A sharp rise in the death rate from Alzheimer s disease Ivan Casserly & Eric Topol, Lancet 2004 Potential for primary prevention of Alzheimer s disease Alzheimer
치매예방을위한만성질환관리전략 김광일 서울대학교의과대학내과학교실 분당서울대학교병원내과 A sharp rise in the death rate from Alzheimer s disease Ivan Casserly & Eric Topol, Lancet 2004 Potential for primary prevention of Alzheimer s disease Alzheimer
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Sex Differences in Stroke Risk and Quality of Life after Stroke
 Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Stroke Therapy: What s s Proven, What s Not and What s s Hot. Lise Labiche, MD Stroke Program Medical City Dallas May 20, 2008
 Stroke Therapy: What s s Proven, What s Not and What s s Hot Lise Labiche, MD Stroke Program Medical City Dallas May 20, 2008 Acute Stroke Therapy What s s Proven IV tpa Intra-arterial arterial thrombolysis
Stroke Therapy: What s s Proven, What s Not and What s s Hot Lise Labiche, MD Stroke Program Medical City Dallas May 20, 2008 Acute Stroke Therapy What s s Proven IV tpa Intra-arterial arterial thrombolysis
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
Impact of Resting Heart Rate on Mortality, Disability and Cognitive Decline in Patients after Ischemic Stroke
 Impact of Resting Heart Rate on Mortality, Disability and Cognitive Decline in Patients after Ischemic Stroke Data from PROFESS M. Böhm Daniel Cotton, Lydia Foster, Florian Custodis, Ulrich Laufs, Ralph
Impact of Resting Heart Rate on Mortality, Disability and Cognitive Decline in Patients after Ischemic Stroke Data from PROFESS M. Böhm Daniel Cotton, Lydia Foster, Florian Custodis, Ulrich Laufs, Ralph
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
10/21/2014. Disclosures. Introduction. Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management
 Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management Daniel T Lackland Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension
Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management Daniel T Lackland Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension
What can we learn from the AVERT trial (so far)?
?") South West Stroke Network Event, 29 th April, 2015 What can we learn from the AVERT trial (so far)? Peter Langhorne, Professor of stroke care, Glasgow University Disclosure PL was AVERT investigator and
South West Stroke Network Event, 29 th April, 2015 What can we learn from the AVERT trial (so far)? Peter Langhorne, Professor of stroke care, Glasgow University Disclosure PL was AVERT investigator and
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease
 Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Top 5 (Topics) Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008
 Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008") Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Liping Liu Dpet. of Neurology and Stroke Center Beijing Tiantan Hospital Capital Medical University
 Liping Liu Dpet. of Neurology and Stroke Center Beijing Tiantan Hospital Capital Medical University Disclosures Conflict of interest disclosures: No Disclosures Funding The CHANCE trial is funded by the
Liping Liu Dpet. of Neurology and Stroke Center Beijing Tiantan Hospital Capital Medical University Disclosures Conflict of interest disclosures: No Disclosures Funding The CHANCE trial is funded by the
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come
: What we know, what we think and what s to come") A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging
 The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
Epidemiology and Prevention of Stroke
 Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University