CASE PRESENTATION. Kārlis Rācenis MD - Latvia
|
|
|
- Cleopatra Skinner
- 5 years ago
- Views:
Transcription


1 CASE PRESENTATION Kārlis Rācenis MD - Latvia
2 o Patient men, 32-years-old o Admitted to the hospital at due to kidney biopsy no complains Admitted to the hospital Acute kidney injury use of NSAIDs T.Ibuprofeni mg, 3 weeks arterial hypertension (BP 210/100 mmhg) July September BP with treatment 140/90 mmhg Over the months Creatinine µmol/l (62-115) GFR (MDRD) 19 ml/min Ca 3,5 mmol/l (2,08-2,65)

3 Medical history I Mental disease since he was 14/15 years old During childhood pneumonia Every day medication: o T.Pregabalini 75 mg qd o T.Quetiapini 25 mg qd o T.Tianeptini 12,5 mg qd o T.Clonazepami 2 mg qd o T.Amlodipini 10 mg qd o T.Moxonidini 0,4 mg bid o T.Bisoprololi 5 mg qd Creatinine µmol/l (62-115) GFR (MDRD) 20 ml/min Ca 3,9 mmol/l (2,08-2,65)
?")

4 Thoughts? Increased bone resorption o o o o o o Malignancy (lung cancer, myeloma, lymphoma)? Paget disease? Primary hyperparathyroidism (sporadic, familial, MEN1, MEN2)? Familial hypocalciuric hypercalcemia? Lithium? Other? Increased intestinal absorption o Milk-alkali syndrome o Granulomatous disease (tuberculosis, sarcoidosis, leprosy) o Vitamin D intoxication Decreased renal excretion o AKI? o Pheochromocytoma? o Thiazide diuretics? o Other?
 20 ml/min/1,73m^2 Blood gas analysis ph 7,505 7,336 7,438 pco2 34,5 35,7 45,7 mmhg po2 112.")
5 Further investigation I Biochemical analysis Alpha amylase U/l Creatinine kinase U/L LDH U/L CRO 0,0 0 5 mg/l Glucose 5,7 4,1 5,9mmol/l Creatinine µmol/ml GFR (MDRD) 20 ml/min/1,73m^2 Blood gas analysis ph 7,505 7,336 7,438 pco2 34,5 35,7 45,7 mmhg po ,2 97,2 mmhg Ca (ionised) 1,81 1,15 1,27 mmol/l SO 2 98,5% Total bilirubin 12,4 5,1 20,5 µmol/ml BUN 13,1 1,8 7,1 mmol/l K 4, mmol/l Na 137, mmol/l Ca 3,90 2,08 2,65 mmol/l P 1,5 0,9 1,5 mmol/l Alkaline phosphatase U/L FT3 3,29 2,3 4,2 pg/ml FT4 1,26 0,89 1,76 ng/ml PTH 14, pg/ml Total protein g/l Albumin 36, g/l Urine analysis 24 hour urine amount 7,1 l Urine calcium 27,76 2,2-2,6 mmol/24h
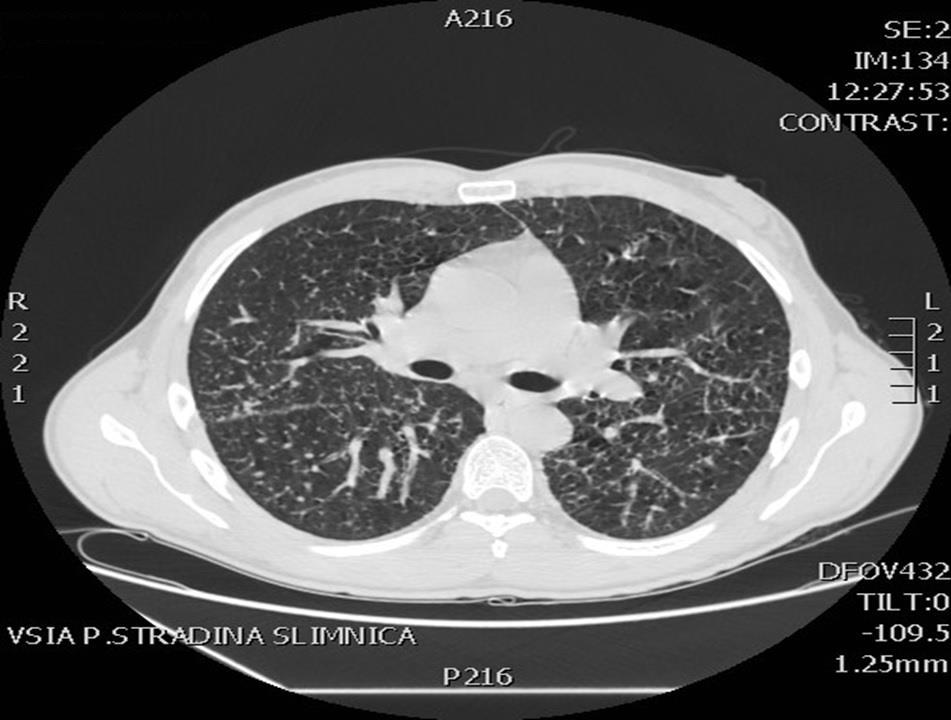
6 Further investigation I Skeletal scintigraphy strong metabolic activity around bone epiphysis, not typical for inflammation, more likely due to metabolic disease. Native chest CT most likely sarcoidosis with cervical, axillar, mediastinal lymphadenopathy (Ø 1 1,3 cm) that should be differentiated between miliary tuberculosis. Native abdomen CT typical kidney cysts. Angiolipoma of right kidney. Inguinal and retroperitoneal lymphadenopathy (Ø 1,1 1,2 cm).
7


8 Tuberculosis Europe < 5 per to 9 per to 19 per to 49 per per Not reporting





9 Bronchoscopy lung biopsy Bronchoscopy - within normal range Transbronchial lung biopsy left lower lobe Bronchial washing for tuberculosis diagnostics Epithelioid granuloma formation Lung tissue with fully formed epithelioid granulomas and surrounding tissue fibrosis. Giant cells Calcification Multinucleated giant cells with intracytoplasmic mineralization are visible.



10 Kidney biopsy The sample contains renal cortex and medulla, 28 glomeruli, 3 of them are globally sclerosed. Calcified deposits are positive in Van Kossa histochemical staining, which shows that this material is calcium phosphates. Immunofluorescence: non specific and very focal findings. The interstitium is focally expanded with mononuclear cell infiltrates occupying approx 20% of cortical area. Few calcified deposits in the interstitium. surrounded by small groups of giant cells.

11 Bronchial washing: Final diagnosis? Microscopy for ARB negative GeneXpert TBC negative BACTEC M.tuberculosis negative Lung biopsy result - lung sarcoidosis Kidney biopsy result mild chronic interstitial inflammation with focal calcification Lung sarcoidosis stage 2 Chronic interstitial nephritis with focal calcinosis Treatment Tab.Prednisoloni 60 mg qd

12 Neurosarcoidosis?? Head MRI: No evidence for pathological changes in native MRI are found.
13 Thank you!
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Acute renal failure and unknown cause hypercalcemia (case report)
") Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-25 U/L 10-35 U/L 10-30 U/L 10-25 U/L 10-30 U/L 10-35 U/L 10-25 U/L 10-35 U/L 10-25 U/L 10-20 U/L 10-35 U/L Albumin 0-6
Chemistry Reference Ranges and Critical Values
 Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
Alanine Aminotransferase (ALT, SGPT) 3-9 years 9-18 years 1-9 years 9-18 years 10-30 U/L 10-30 U/L 10-20 U/L Albumin 0-6 days 6 days - 37 months 37 months - 7 years 7-20 years 2.6-3.6 g/dl 3.4-4.2 g/dl
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Clinical biochemistry of calcium and vitamin D
 Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Hiroyuki Kamiya 1), Soichiro Ikushima 1), Tetsu Sakamoto 1), Kozo Morimoto 1), Tsunehiro Ando 1), Masaru Oritsu 1), Atsuo Goto 2), Tamiko Takemura 3)
, Soichiro Ikushima 1), Tetsu Sakamoto 1), Kozo Morimoto 1), Tsunehiro Ando 1), Masaru Oritsu 1), Atsuo Goto 2), Tamiko Takemura 3)") 29 2001 ACE39.7IU/l X TBLB 2002 11 Langhans [ ] A Case of Granulomatous Interstitial Nephritis with Progressive Renal Impairment Due to Sarcoidosis in the Course of Spontaneous Improvement of Pulmonary
29 2001 ACE39.7IU/l X TBLB 2002 11 Langhans [ ] A Case of Granulomatous Interstitial Nephritis with Progressive Renal Impairment Due to Sarcoidosis in the Course of Spontaneous Improvement of Pulmonary
WHAT IS YOUR DIAGNOSIS?
 WHAT IS YOUR DIAGNOSIS? A 21 month old, female neutered Cockapoo presented with a 5 day history of trembling. The dog had been in the owners possession since a 7 week old puppy, and was up-to-date with
WHAT IS YOUR DIAGNOSIS? A 21 month old, female neutered Cockapoo presented with a 5 day history of trembling. The dog had been in the owners possession since a 7 week old puppy, and was up-to-date with
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
New aspects of acid-base disorders
 New aspects of acid-base disorders I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Division of Nephrology, Hypertension and Transplantation University of Florida College of Medicine
New aspects of acid-base disorders I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Division of Nephrology, Hypertension and Transplantation University of Florida College of Medicine
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Symptom management: Hypercalcemia
 Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Figure 2: Lymph node Cortical follicular (F) and paracortical (PC) atrophy, with narrowing of the cortex relative to the medulla (M).
 and paracortical (PC) atrophy, with narrowing of the cortex relative to the medulla (M).") Figure 1: Lymph node Follicular hyperplasia, with expansion of the follicular germinal centres (F) by large blast cells. Paracortical hyperplasia, with expansion of the paracortex (PC) by small lymphocytes.
Figure 1: Lymph node Follicular hyperplasia, with expansion of the follicular germinal centres (F) by large blast cells. Paracortical hyperplasia, with expansion of the paracortex (PC) by small lymphocytes.
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
ROTUNDA HOSPITAL DEPARTMENT OF LABORATORY MEDICINE
 This active test table informs the user of Biochemistry tests available in house. s referred to other sites are recorded in the Referred Table. Issue date: 4 TH April 2016 Contact Phone Number ext.1345/2522
This active test table informs the user of Biochemistry tests available in house. s referred to other sites are recorded in the Referred Table. Issue date: 4 TH April 2016 Contact Phone Number ext.1345/2522
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Dana Lecture 2 Chronic Kidney Disease
 Medicine Dr. Dana Lecture 2 Chronic Kidney Disease Chronic Kidney Disease Assessment of renal function Classification of CKD Why Chronic renal failure tends to progress Risk factors for progression Management
Medicine Dr. Dana Lecture 2 Chronic Kidney Disease Chronic Kidney Disease Assessment of renal function Classification of CKD Why Chronic renal failure tends to progress Risk factors for progression Management
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Histopathology: granulomatous inflammation, including tuberculosis
 Histopathology: granulomatous inflammation, including tuberculosis These presentations are to help you identify basic histopathological features. They do not contain the additional factual information
Histopathology: granulomatous inflammation, including tuberculosis These presentations are to help you identify basic histopathological features. They do not contain the additional factual information
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
5/10/2014. Observation, control of blood pressure. Observation, control of blood pressure and risk factors.
 Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Protocol GTC : A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients.
 in Chronic Kidney Disease Patients.") Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY
 MHD I, Session VIII, Student Copy Page 1 MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY MHD I, Session VIII, Student Copy Page 2 Case #1 Chief Complaint: I have been feeling just lousy
MHD I, Session VIII, Student Copy Page 1 MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY MHD I, Session VIII, Student Copy Page 2 Case #1 Chief Complaint: I have been feeling just lousy
BC Cancer Protocol Summary for Therapy of Acute Myeloid Leukemia Using azacitidine and SORAfenib
 BC Cancer Protocol Summary for Therapy of Acute Myeloid Leukemia Using azacitidine and SORAfenib Protocol Code Tumour Group Contact Physician ULKAMLAS Leukemia/BMT Dr. Donna Hogge ELIGIBILITY: Acute myeloid
BC Cancer Protocol Summary for Therapy of Acute Myeloid Leukemia Using azacitidine and SORAfenib Protocol Code Tumour Group Contact Physician ULKAMLAS Leukemia/BMT Dr. Donna Hogge ELIGIBILITY: Acute myeloid
changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM.
 The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
Case 4 Generalised bone pain
 Case 4 Generalised bone pain C A 34- year- old woman presented complaining of multifocal pain in her chest and legs. The pain was intermittent, was aggravated by weight bearing. Initially was alleviated
Case 4 Generalised bone pain C A 34- year- old woman presented complaining of multifocal pain in her chest and legs. The pain was intermittent, was aggravated by weight bearing. Initially was alleviated
Chronic Kidney Disease in Primary Care
 Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
Tables of Normal Values (As of February 2005)
") Tables of Normal Values (As of February 2005) Note: Values and units of measurement listed in these Tables are derived from several resources. Substantial variation exists in the ranges quoted as normal
Tables of Normal Values (As of February 2005) Note: Values and units of measurement listed in these Tables are derived from several resources. Substantial variation exists in the ranges quoted as normal
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Sarcoidosis is a clinicopathologic syndrome resulting from dispersed
 Renal Involvement in Sarcoidosis Garabed Eknoyan Sarcoidosis is a clinicopathologic syndrome resulting from dispersed organ involvement by a noncaseating granulomatous process of unknown cause. The clinical
Renal Involvement in Sarcoidosis Garabed Eknoyan Sarcoidosis is a clinicopathologic syndrome resulting from dispersed organ involvement by a noncaseating granulomatous process of unknown cause. The clinical
MEMORANDUM. These reference ranges are effective immediately but sample requirements remain unchanged currently.
 MEMORANDUM Originating Department Chemical Pathology Issued By: Issued To: Subject: Details: Dr. Shari Srinivasan All Laboratory Service Users Change in Chemical Pathology Analysers Dear Colleague, As
MEMORANDUM Originating Department Chemical Pathology Issued By: Issued To: Subject: Details: Dr. Shari Srinivasan All Laboratory Service Users Change in Chemical Pathology Analysers Dear Colleague, As
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia
 BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
ESIM: Winter School in Riga Case report
 ESIM: Winter School in Riga 2015 Case report Imanta Ozola Zālīte Pauls Stradins Clinical University Hospital Latvia 29.01.2015. January, 2006 32 y., man 2-3 weeks fatigue fluidal stool 2 times per day
ESIM: Winter School in Riga 2015 Case report Imanta Ozola Zālīte Pauls Stradins Clinical University Hospital Latvia 29.01.2015. January, 2006 32 y., man 2-3 weeks fatigue fluidal stool 2 times per day
Long-Term Care Updates
 Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
Analytical Methods: the Kidney Early Evaluation Program (KEEP) The Kidney Early Evaluation program (KEEP) is a free, community based health
 The Kidney Early Evaluation program (KEEP) is a free, community based health") Analytical Methods: the Kidney Early Evaluation Program (KEEP) 2000 2006 Database Design and Study Participants The Kidney Early Evaluation program (KEEP) is a free, community based health screening program
Analytical Methods: the Kidney Early Evaluation Program (KEEP) 2000 2006 Database Design and Study Participants The Kidney Early Evaluation program (KEEP) is a free, community based health screening program
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Woman, 66, With Persistent Abdominal and Back Pain
 Woman, 66, With Persistent Abdominal and Back Pain Jennifer L. Osborne, MPAS, PA-C, David J. Klocko, MPAS, PA-C A 66-year-old Latin American woman presented to the emergency department (ED) with persistent
Woman, 66, With Persistent Abdominal and Back Pain Jennifer L. Osborne, MPAS, PA-C, David J. Klocko, MPAS, PA-C A 66-year-old Latin American woman presented to the emergency department (ED) with persistent
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
SUPPLEMENTARY FIGURES
 SUPPLEMENTARY FIGURES Supplementary Figure 1: immunoprecipitation with anti-casr antibody The Casr protein was expressed in transiently transfected HEK cells. Cell lysates from HEK cells were subjected
SUPPLEMENTARY FIGURES Supplementary Figure 1: immunoprecipitation with anti-casr antibody The Casr protein was expressed in transiently transfected HEK cells. Cell lysates from HEK cells were subjected
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Stability of VACUETTE Lithium Heparin Separator tubes with modified centrifugation conditions
 Stability of VACUETTE Lithium Heparin Separator tubes with modified centrifugation conditions Background: Greiner-Bio-One, Austria has been selling plastic evacuated tubes (VACUETTE ) for venous blood
Stability of VACUETTE Lithium Heparin Separator tubes with modified centrifugation conditions Background: Greiner-Bio-One, Austria has been selling plastic evacuated tubes (VACUETTE ) for venous blood
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
Hamilton Regional Laboratory Medicine Program
 Created: April 2002 of Review: February 2004 of Review: June 2006 of Review: July 2007, St. Joseph s Healthcare went live with Meditech as of June18, 2007. of Review: August 2009 of Review: December 2011;
Created: April 2002 of Review: February 2004 of Review: June 2006 of Review: July 2007, St. Joseph s Healthcare went live with Meditech as of June18, 2007. of Review: August 2009 of Review: December 2011;
Biochemistry Adult Reference Ranges
 Certified correct on 28/06/2016 Biochemistry Adult Reference Ranges Test Reference range Units Reference range from Traceable to standard reference material Albumin 35 50 g/l Pathology IRMM ERM-DA470k/IFCC
Certified correct on 28/06/2016 Biochemistry Adult Reference Ranges Test Reference range Units Reference range from Traceable to standard reference material Albumin 35 50 g/l Pathology IRMM ERM-DA470k/IFCC
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
RAPIDLY FAILING KIDNEYS. Dr Paul Johny 2 nd yr DNB Medicine Resident
 RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
CHRONIC KIDNEY FAILURE
 CHRONIC KIDNEY FAILURE Overview Chronic kidney disease, also called chronic kidney failure, describes the gradual loss of kidney function. Your kidneys filter wastes and excess fluids from your blood,
CHRONIC KIDNEY FAILURE Overview Chronic kidney disease, also called chronic kidney failure, describes the gradual loss of kidney function. Your kidneys filter wastes and excess fluids from your blood,
Functional Blood Chemistry & CBC Analysis
 Functional Blood Chemistry & CBC Analysis Session 10 Inflammation Markers The 19 Deadly Sins of Heart Disease 1. Excess LDL 2. Excess Total cholesterol 3. Low HDL 4. Excess Triglycerides 5. Oxidized LDL
Functional Blood Chemistry & CBC Analysis Session 10 Inflammation Markers The 19 Deadly Sins of Heart Disease 1. Excess LDL 2. Excess Total cholesterol 3. Low HDL 4. Excess Triglycerides 5. Oxidized LDL
BCH 450 Biochemistry of Specialized Tissues
 BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS
 Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Adams Memorial Hospital Decatur, Indiana EXPLANATION OF LABORATORY TESTS Your health is important to us! The test descriptions listed below are for educational purposes only. Laboratory test interpretation
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Hamilton Regional Laboratory Medicine Program
 Created: April 2002 of Review: February 2004 of Review: June 2006 of Review: July 2007, St. Joseph s Healthcare went live with Meditech as of June18, 2007. of Review: August 2009 of Review: December 2011;
Created: April 2002 of Review: February 2004 of Review: June 2006 of Review: July 2007, St. Joseph s Healthcare went live with Meditech as of June18, 2007. of Review: August 2009 of Review: December 2011;
Breakout Session C: Harmonisation of the Alert Table.
 Breakout Session C: Harmonisation of the Alert Table. RCPA-AACB High Risk Results Working Party Andrew Georgiou Craig Campbell Grahame Caldwell Hans Schneider Penelope Coates Que Lam Rita Horvath Robert
Breakout Session C: Harmonisation of the Alert Table. RCPA-AACB High Risk Results Working Party Andrew Georgiou Craig Campbell Grahame Caldwell Hans Schneider Penelope Coates Que Lam Rita Horvath Robert
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Analyte Specimen Demographic Reference Range Units
 Acetone Negative titer Alanine aminotransferase (ALT/SGPT) 10-49 U/L Albumin 3.2-4.8 g/dl Alcohol < 10 Alpha-fetoprotein (AFP) < 1.3-8.1 ng/ml Alkaline phosphatase 0 7 days 7 30 days 1 3 3 6 6 12 1 3 3
Acetone Negative titer Alanine aminotransferase (ALT/SGPT) 10-49 U/L Albumin 3.2-4.8 g/dl Alcohol < 10 Alpha-fetoprotein (AFP) < 1.3-8.1 ng/ml Alkaline phosphatase 0 7 days 7 30 days 1 3 3 6 6 12 1 3 3
Evaluation of VACUETTE SECONDARY Tubes
 Evaluation of VACUETTE SECODARY Tubes Background VACUETTE SECODARY Tubes are used as a secondary container for aliquoting, storing and transporting blood, blood components and urine from the primary tube
Evaluation of VACUETTE SECODARY Tubes Background VACUETTE SECODARY Tubes are used as a secondary container for aliquoting, storing and transporting blood, blood components and urine from the primary tube
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Clinician Blood Panel Results
 Page 1 of 7 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
Page 1 of 7 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
AGING KIDNEY IN HIV DISEASE
 AGING KIDNEY IN HIV DISEASE Michael G. Shlipak, MD, MPH Professor of Medicine, Epidemiology and Biostatistics, UCSF Chief, General Internal Medicine, San Francisco VA Medical Center Kidney, Aging and HIV
AGING KIDNEY IN HIV DISEASE Michael G. Shlipak, MD, MPH Professor of Medicine, Epidemiology and Biostatistics, UCSF Chief, General Internal Medicine, San Francisco VA Medical Center Kidney, Aging and HIV
Lithium toxicity. Dr Aude Servais Service de Néphrologie adulte Hôpital Necker, Paris
 Lithium toxicity Dr Aude Servais Service de Néphrologie adulte Hôpital Necker, Paris Lithium Use of lithium salts as salt substitutes but recall from the marketplace in 1949 Efficient in the treatment
Lithium toxicity Dr Aude Servais Service de Néphrologie adulte Hôpital Necker, Paris Lithium Use of lithium salts as salt substitutes but recall from the marketplace in 1949 Efficient in the treatment
MULTI-SYSTEM SARCOIDOSIS CAUSING PANHYPOPITUITARISM: RAPID IMPROVEMENT WITH CORTICOSTEROID THERAPY Rashid Mahboob, MD; Ali A.
 ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
CHRONIC KIDNEY DISEASE (CKD)
") CHRONIC KIDNEY DISEASE (CKD) CKD implies longstanding (more than 3 months), and usually progressive, impairment in renal function. In many instances, no effective means are available to reverse the primary
CHRONIC KIDNEY DISEASE (CKD) CKD implies longstanding (more than 3 months), and usually progressive, impairment in renal function. In many instances, no effective means are available to reverse the primary
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Important aspects of acid-base disorders
 Important aspects of acid-base disorders I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Division of Nephrology, Hypertension and Transplantation University of Florida College
Important aspects of acid-base disorders I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Division of Nephrology, Hypertension and Transplantation University of Florida College
The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels
 17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
Effect of Alkali on Metastatic Calcification Produced by Hypervitaminosis D
 Effect of Alkali on Metastatic Calcification Produced by Hypervitaminosis D Pages with reference to book, From 345 To 348 Gulshan Naheed ( Present Address: Khyber Medical College, Peshawar. ) N.A. Jafarey
Effect of Alkali on Metastatic Calcification Produced by Hypervitaminosis D Pages with reference to book, From 345 To 348 Gulshan Naheed ( Present Address: Khyber Medical College, Peshawar. ) N.A. Jafarey
Disclosures. Topics. Staging and GFR. K-DOQI Staging of Chronic Kidney Disease. Definition of Chronic Kidney Disease. Chronic Kidney Disease
 Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
Dosage in renal impairment Kalcipos-D chewable tablets should not be used in patients with severe renal impairment.
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as