Chronic Kidney Disease in Primary Care
|
|
|
- Dwight York
- 5 years ago
- Views:
Transcription




1 Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters


2 Dr Gerald Waters Renal Physician Chronic Kidney Disease

3 Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs in CKD Antihypertensives Proteinuria Cardiovascular Risk Calcium/Phosphate/Vit D Anaemia/Erythropoietin/Iron Drugs
4 Reduced kidney function lasting longer than 3 months Nephrons do not regenerate, once lost are lost forever Some hyperplasia however can occur, max 30-40% increase in function
5 Aims of management Slow progression (BP and proteinuria control) Address increased cardiovascular risk (Advanced CKD) - Manage Mineral and Bone Disorder, Anaemia, and plan for renal replacement therapy
6 (short version) Creatinine is a muscle protein, renally excreted, no other form of clearance* Serum creatinine depends on muscle mass and glomerular filtration rate = amount of blood filtered by the kidneys per unit time (ml/min, ml/sec, L/day) Easy to measure vs actual GFR measurement (radioisotope) * Also is secreted into tubule and therefore CrCl slightly overestimates GFR

7 25 yr old Male, Creatinine 140? GFR
8 GFR can be estimated from the serum creatinine using one of several formulas (Constant is 1.23 for men and 1.04 for women) (for Cr in mg/dl, k is 0.7 for females and 0.9 for males, a is for females and for males) 4 variable MDRD and CKD EPI widely used, weight not required. Not accurate for GFR>60, large or small people.
9 Rough estimate of normal range of GFR = (120-age) to (200-age) Cockroft and Gault has terrible performance 50-70% of C&G ecrcl is within 30% of true GFR compared with 83% of MDRD egfr. Conversely, 20% of MDRD egfr is more than 30% different from the true GFR. This error gets worse with increasing GFR.
10
 End Stage Renal Failure Need dialysis to survive.")
11 Stage 1 GFR>90ml/min and a kidney disease or proteinuria Stage 2 GFR Stage (3A, 45-60, 3B 30-45) Stage Stage 5 - <15, (5D on dialysis) End Stage Renal Failure Need dialysis to survive. Usually GFR<10 Can append a P for proteinuria if you like
12


13 4,200 8, , ,000 42, m Ack. Kelvin Lynn
14 45 CVD Risk with CKD > <15 Age-Standardized Rate of Cardiovascular Events (per 100 person-yr)


15 2-year follow-up and comparison with prevalent dialysis patients: risk of death vs. end-stage renal disease. Collins et al 2003
16 500x as likely to die! 10x as likely 30yr old = 85 yr old


17
18 Aims of treatment Slow progression Prevent complications of CKD Prevent death from CVD
19 Aggressive control of BP slows progression of CKD Targets <140/90 or 130/80 if proteinuria present CKD causes hypertension, HTN causes CKD Vicious circle Multiple drugs almost always needed
20 First line treatment in the setting of CKD especially with proteinuria / diabetes Antiproteinuric effect in addition to antihypertensive effect Alter blood flow through glomerulus physiological effect on GFR 20% reduction However over a longer time frame, slows deterioration of GFR (see next slide) Side effects can limit use persistent cough, angio-oedema, high K, others
21 30 10 Expected benefit of ACEI slower decline in GFR following the initial drop. This initial drop does not represent permanent nephron loss - GFR typically increases following discontinuation of ACEI
22
23 Group 1 Cr Group 2 Cr
24 Probably similar in effect to ACEI, without the cough Candesartan available on special authority Losartan does not need special authority

25 Rate of Rise more important than absolute level 6.0 or under no concern dietary restriction, hold ACEI/ARB >6.5 refer hospital Dietary restriction avoid bananas Cut up, boil, drain veges, avoid dried fruits, low K fruit/veges = apple, pear berries, canned, avoid hot chips, kumara, fruit/vege juices, milk, soups

26 (Low Potassium) (High Potassium)

27 Thiazides Less effective in CKD, still used however Combination with ACEI particularly effective Hence Inhibace Plus, Accuretic, Co-Renitec etc Thiazide-likes much better chlorthalidone long acting, probably better for HTN Loop diuretics - Frusemide, bumetanide Generally used in advanced CKD, for BP and fluid control Often combined with long acting thiazides or thiazide-like diuretics in advanced CKD
28 Dihydropyridine - Felodipine, amlodipine Non-dihydropyridine Diltiazem Most commonly used as a 2 nd or 3 rd line agent after ACEI/ARB and thiazide. The 2 types of CCB can be combined for additional antihypertensive effect if required (generally as a 5 th or 6 th - line agent)
29 3 rd or 4 th line treatment for HTN Not well tolerated by young patients Lethargy, erectile dysfunction Alpha blockers postural hypotension problematic in elderly Large doses may be required Combined alpha/beta carvedilol, labetolol Poorly tolerated
30 Spironolactone? avoided in CKD Hyperkalaemia, acute kidney injury due to dehydration However, good trial evidence of benefit in resistant hypertension Older antihypertensives rarely used, methyldopa, hydralazine etc Very poorly tolerated, long and nasty side effect list

31
32 Minor damage to glomeruli leads to leakage of protein Protein damages kidney tubules and leads to nephron loss Caused by diabetes, and many other diseases Nephrotic syndrome = heavy proteinuria (PCR>350, ACR>300) AND oedema AND low albumin (<30)
33
34 Reducing the amount of proteinuria slows progression of CKD ACEI, ARB primary drugs used Dual blockade (ACEI and ARB) (or super-dose ACEI) has additional antiproteinuric effect with minimal BP effect Aim for maximum tolerated does ACEI/ARB reduce other antihypertensives if needed
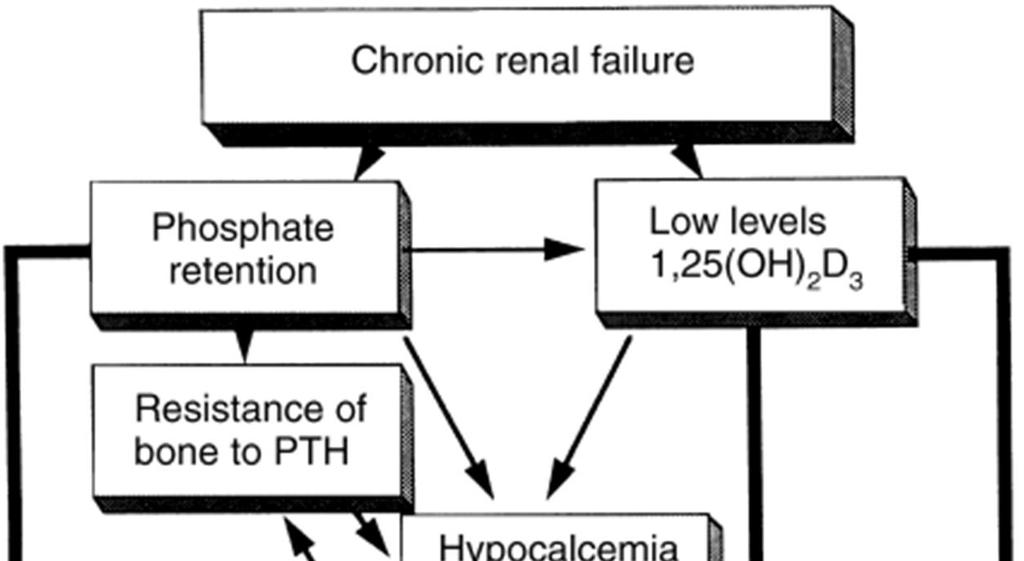
35 Mineral and Bone Disorder (MBD) CKD causes derangement of the Ca-Phos homeostatic mechanisms key problem is poor renal excretion of phosphate Secondary hyperparathyroidism can develop at GFR<80 despite normal serum calcium and phosphate Normalising phosphate prevents development of hyperparathyroidism and bone mineralisation disease.?? CVD
36 Phosphate level for people with kidney disease NOT ON DIALYSIS 3 years of high phosphate = 40% have died. Good phosphate 10-20% have died.
37 Phosphate and other levels for dialysis patients After 3 years on dialysis, good phosphate (etc) levels = 80% alive. Bad phosphate (etc) = 55% alive
38
39
40
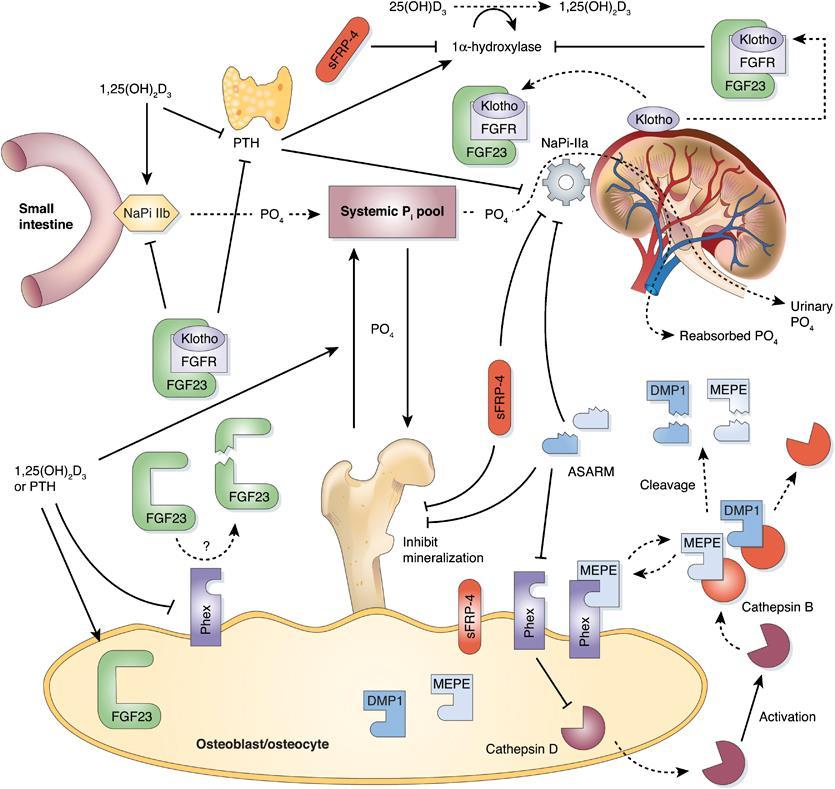
41 FGF-23
42 Main source of phosphate is dietary Dietary restriction of phosphate is most important measure Phosphate binders are secondary means of reducing phosphate Calcium carbonate and aluminium hydroxide Ca3(PO4)2 and Al(PO4) are insoluble hence not absorbed from the gut Sevelamer (Renagel), lanthanum carbonate used overseas, expensive, no better
43 Must be taken with meals, at the start of the meal immediately before eating. Should ideally be taken with every meal Patients often forget to take binders, particular with lunch or if away from home Serum calcium and Aluminium levels must be monitored. High Aluminium can cause bone disease
44 Cholecalciferol or unhydroxylated Vit D3 is the raw inactive form (the 1.25mg monthly form) Kidneys convert 25-hydroxy-Vit D3 to 1 alpha-25 hydroxy vit D which is the active form (also called calcitriol) Therefore patients with CKD require the active form (calcitriol or One Alpha which needs 25- hydroxylating) rather than cholecalciferol However, there is some suggestion that the inactive form does have some biological activity such as in the immune system, and therefore some Nephrologists prescribe cholecalciferol as well
45 1,25 vit-d3 suppresses Parathyroid hormone production, preventing hyperparathyroidism However, also increases dietary absorption of calcium and phosphate Administration 2 or 3 days per week maintains PTH suppression while minimising Ca/PO4 absorption

46 Vitamin D nomenclature Alfacalcidol ( One Alpha ) 1 hydroxycholecalciferol (needs double dose cf calcitriol)
47 Aim to maintain phosphate at or near normal range with binders, dietary restriction and dialysis Calcium normal range Calcium supplement Maintain PTH in normal range (?) Phosphate control, vitamin D, parathyroidectomy or calcimimetics Once on dialysis maintain at 2-9x normal KDIGO

48 Complex Iron deficiency common. IV Iron often required. Erythropoietin may be required at GFR < 45 in diabetics and GFR<30 in non diabetics. Over those GFR levels renal anaemia very rare. PHARMAC approval - Hb < 100, GFR <30, or <45 in diabetic Any specialist
49 High risk for cardiovascular disease Aspirin, statins, beta-blockers reduce risk of cardiovascular death in CKD patients. Once on dialysis, conventional risk reduction therapies show no benefit? Different mechanism? Phosphate driven? Statins show no benefit in primary prevention Warfarin for AF no benefit

50 Common drugs Metformin increased risk lactic acidosis Sotalol renal excretion, accumulation and bradycardia Digoxin monitor levels closely Gabapentin large dose reduction needed Antibiotics don t worry
51 NSAIDS Fibrates = bezalip Unexplained AKI? Interstitial nephritis Penicillins, cephalosporins, other antibiotics NSAIDS RARE: PPIs (omeprazole), allopurinol, others Chinese herbals with aristocholic acid

52
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Kidney damage with normal or increased GFR Kidney damage with mild reduction in GFR
 CHRONIC KIDNEY DISEASE Contents Stages of Chronic Kidney Disease Dosing adjustments Hyperphosphataemia management Secondary hyperparathyroidism Anaemias Hyperkalaemia Acidosis Hypertension STAGES OF CHRONIC
CHRONIC KIDNEY DISEASE Contents Stages of Chronic Kidney Disease Dosing adjustments Hyperphosphataemia management Secondary hyperparathyroidism Anaemias Hyperkalaemia Acidosis Hypertension STAGES OF CHRONIC
Chronic Kidney Disease The 6 Pillars. Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre
 Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
Long-Term Care Updates
 Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Renal Failure Update in Treatment Part 1. DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602)
") Renal Failure Update in Treatment Part 1 DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602) 263 5446 dwalton@akdhc.com DISCLOSURES NONE OFF LABEL USE POSSIBLY LEARNING OBJECTIVES USE
Renal Failure Update in Treatment Part 1 DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602) 263 5446 dwalton@akdhc.com DISCLOSURES NONE OFF LABEL USE POSSIBLY LEARNING OBJECTIVES USE
Disclosures. Topics. Staging and GFR. K-DOQI Staging of Chronic Kidney Disease. Definition of Chronic Kidney Disease. Chronic Kidney Disease
 Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
DIABETES AND YOUR KIDNEYS
 DIABETES AND YOUR KIDNEYS OR AS WE CALL IT DIABETIC NEPHROPATHY The latest guidelines to keep you safe, healthy, fit, and out of danger from needing dialysis A UCLA HEALTH EDUCATIONAL SEMINAR Ramy M. Hanna
DIABETES AND YOUR KIDNEYS OR AS WE CALL IT DIABETIC NEPHROPATHY The latest guidelines to keep you safe, healthy, fit, and out of danger from needing dialysis A UCLA HEALTH EDUCATIONAL SEMINAR Ramy M. Hanna
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Dana Lecture 2 Chronic Kidney Disease
 Medicine Dr. Dana Lecture 2 Chronic Kidney Disease Chronic Kidney Disease Assessment of renal function Classification of CKD Why Chronic renal failure tends to progress Risk factors for progression Management
Medicine Dr. Dana Lecture 2 Chronic Kidney Disease Chronic Kidney Disease Assessment of renal function Classification of CKD Why Chronic renal failure tends to progress Risk factors for progression Management
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Medicines for anaemia and mineral bone disease
 Patient Information: Medicines NHS Logo here Medicines for anaemia and mineral bone disease Health & care information you can trust The Information Standard Certified Member Working together for better
Patient Information: Medicines NHS Logo here Medicines for anaemia and mineral bone disease Health & care information you can trust The Information Standard Certified Member Working together for better
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
Figure 1 LVH: Allowed Cost by Claim Volume (Data generated from a Populytics analysis).
.") Chronic Kidney Disease (CKD): The New Silent Killer Nelson Kopyt D.O. Chief of Nephrology, LVH Valley Kidney Specialists For the past several decades, the health care needs of Americans have shifted from
Chronic Kidney Disease (CKD): The New Silent Killer Nelson Kopyt D.O. Chief of Nephrology, LVH Valley Kidney Specialists For the past several decades, the health care needs of Americans have shifted from
Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care
 Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care Paula D Souza Senior CKD Nurse Specialist Royal Devon and Exeter Healthcare Trust Introduction Background What
Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care Paula D Souza Senior CKD Nurse Specialist Royal Devon and Exeter Healthcare Trust Introduction Background What
Keeping your kidneys young
 Keeping your kidneys young Ramy M. Hanna MD FASN FACP Clinical Instructor David Geffen School of Medicine UCLA Health Department of Medicine Division of Nephrology June 25, 2018 The kidneys gets a lot
Keeping your kidneys young Ramy M. Hanna MD FASN FACP Clinical Instructor David Geffen School of Medicine UCLA Health Department of Medicine Division of Nephrology June 25, 2018 The kidneys gets a lot
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions. Jonathan Evans Paediatric Nephrologist
 The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Chronic Kidney Disease Mineral Bone Disease
 NHS Logo here Chronic Kidney Disease Mineral Bone Disease (CKD-MBD) Patient Information Health & care information you can trust The Information Standard Certified Member Working together for better patient
NHS Logo here Chronic Kidney Disease Mineral Bone Disease (CKD-MBD) Patient Information Health & care information you can trust The Information Standard Certified Member Working together for better patient
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Concept and General Objectives of the Conference: Prognosis Matters. Andrew S. Levey, MD Tufts Medical Center Boston, MA
 Concept and General Objectives of the Conference: Prognosis Matters Andrew S. Levey, MD Tufts Medical Center Boston, MA General Objectives Topics to discuss What are the key outcomes of CKD? What progress
Concept and General Objectives of the Conference: Prognosis Matters Andrew S. Levey, MD Tufts Medical Center Boston, MA General Objectives Topics to discuss What are the key outcomes of CKD? What progress
Applying clinical guidelines treating and managing CKD
 Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Section Questions Answers
 Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Transforming Diabetes Care
 Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
The biologic price of aging includes progressive
 The Aging Kidney: Physiological Changes The biologic price of aging includes progressive structural and functional deterioration of the kidney, and these changes are among the most dramatic of any organ
The Aging Kidney: Physiological Changes The biologic price of aging includes progressive structural and functional deterioration of the kidney, and these changes are among the most dramatic of any organ
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS WHO SHOULD BE TESTED FOR CKD Offer testing for CKD using egfr, serum creatinine and urinary ACR to people with any of the following risk factors: diabetes hypertension acute
CHRONIC KIDNEY DISEASE DIAGSIS WHO SHOULD BE TESTED FOR CKD Offer testing for CKD using egfr, serum creatinine and urinary ACR to people with any of the following risk factors: diabetes hypertension acute
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
CHRONIC KIDNEY DISEASE
 CHRONIC KIDNEY DISEASE Chronic kidney disease (CKD) is defined by a reduction in the glomerular filtration rate (GFR) and/or urinary abnormalities or structural abnormalities of the renal tract. The severity
CHRONIC KIDNEY DISEASE Chronic kidney disease (CKD) is defined by a reduction in the glomerular filtration rate (GFR) and/or urinary abnormalities or structural abnormalities of the renal tract. The severity
Chronic Kidney Disease. Basics of CKD Terms Diagnosis Management
 Chronic Kidney Disease Basics of CKD Terms Diagnosis Management Review the prevalence of chronic kidney disease (CKD) Review how CKD develops Review populations at risk for CKD Review CKD diagnosis Objectives
Chronic Kidney Disease Basics of CKD Terms Diagnosis Management Review the prevalence of chronic kidney disease (CKD) Review how CKD develops Review populations at risk for CKD Review CKD diagnosis Objectives
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree
 and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree") Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
5/10/2014. Observation, control of blood pressure. Observation, control of blood pressure and risk factors.
 Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Chronic kidney disease in cats
 Chronic kidney disease in cats What is chronic kidney disease (CKD)? Chronic kidney disease (CKD) is the name now used to refer to cats with kidney failure (or chronic kidney failure). CKD is one of the
Chronic kidney disease in cats What is chronic kidney disease (CKD)? Chronic kidney disease (CKD) is the name now used to refer to cats with kidney failure (or chronic kidney failure). CKD is one of the
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
COMMON MEDICINES USED IN CKD CHRONIC KIDNEY DISEASE
 CHRONIC KIDNEY DISEASE 1 This information is intended to help you understand why you need to take your medicines. There are multiple medicines that are used to control the symptoms related to CKD. You
CHRONIC KIDNEY DISEASE 1 This information is intended to help you understand why you need to take your medicines. There are multiple medicines that are used to control the symptoms related to CKD. You
Screen annually for patients with any of the following risk factors:
 CASE DEFINITION Chronic Kidney Disease (CKD) is either of the following, persisting for at least three months, repeated on at least two occasions: 1. Markers of kidney damage (e.g. proteinuria, haematuria
CASE DEFINITION Chronic Kidney Disease (CKD) is either of the following, persisting for at least three months, repeated on at least two occasions: 1. Markers of kidney damage (e.g. proteinuria, haematuria
Doncaster & Bassetlaw. AKI guidelines for primary care
 Doncaster & Bassetlaw AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE... 2 FLOW DIAGRAM: MANAGEMENT OF HYPERKALAEMIA.... 3 FLOW DIAGRAM:
Doncaster & Bassetlaw AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE... 2 FLOW DIAGRAM: MANAGEMENT OF HYPERKALAEMIA.... 3 FLOW DIAGRAM:
Renal Transporters- pathophysiology of drug - induced renal disorders. Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November
 Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC.
 Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
The future is here. It s just not widely distributed yet. William Gibson
 The future is here. It s just not widely distributed yet. William Gibson CHRONIC KIDNEY DISEASE MANAGEMENT A NEW PARADIGM Aaron Cass, MD, FRCPC Nephrologist, Fraser Health January 22, 2014 Where Are We
The future is here. It s just not widely distributed yet. William Gibson CHRONIC KIDNEY DISEASE MANAGEMENT A NEW PARADIGM Aaron Cass, MD, FRCPC Nephrologist, Fraser Health January 22, 2014 Where Are We
Nephrology Potpourri March 22, 2017
 Nephrology Potpourri March 22, 2017 http://soulscape.asia/give-flowers-more-life-by-making-your-own-potpourri Kantima Phisitkul, MD Clinical Assistant Professor Renal Diseases and Hypertension Division
Nephrology Potpourri March 22, 2017 http://soulscape.asia/give-flowers-more-life-by-making-your-own-potpourri Kantima Phisitkul, MD Clinical Assistant Professor Renal Diseases and Hypertension Division
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM.
 The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Southern Derbyshire Shared Care Pathology Guidelines. AKI guidelines for primary care
 Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP
 PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP OUTLINE INTRODUCTION BURDEN OF CKD DEFINITION OF PRE-DIALYSIS CARE (PDC) GOALS OF PDC IN CKD COMPONENTS OF PDC ADVANTAGES
PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP OUTLINE INTRODUCTION BURDEN OF CKD DEFINITION OF PRE-DIALYSIS CARE (PDC) GOALS OF PDC IN CKD COMPONENTS OF PDC ADVANTAGES
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER. The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR
 CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
Chronic kidney disease management primary care
 Care map information Information resources for patients and carers Aboriginal and Torres Strait Islanders DEFINITION OF CKD egfr
Care map information Information resources for patients and carers Aboriginal and Torres Strait Islanders DEFINITION OF CKD egfr
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,