Last frontier of infection in critically ill patients
|
|
|
- Lenard Hancock
- 5 years ago
- Views:
Transcription

1 Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine


2 Liverpool School of Tropical Medicine
3 Sepsis Recognition Management Many Frontiers and not the last... Multidrug resistance System approaches

4 Point of care tests Not included Laboratory markers of infection eg Procalcitonin Selective decontamination Line management Ventilator associated pneumonia Other bundles of care Specific multiresistant organisms



5 Importance of Sepsis Increasing incidence 2% of hospital patients and 75% of ICU patients Overall mortality ~35% Leading cause of morbidity and mortality in ICU Bacteraemia 10-15% Severe sepsis 20-40% Septic shock 40-60% Sepsis and MOF >70%

6 Martin et al: N Engl J Med 2003;348:1546
7 Severe sepsis incidence and mortality increase with age Incidence per 100, Mortality Incidence Mortality % 0 0 < >85 Angus et al. Crit Care Med 2001; 29:1301
8 Relationship between mortality on ICU and the number of failed organs From Brealey & Singer, 2000

9 BUT In the UK only ~20% of cases are recognised and managed correctly in the emergency room National review of sepsis deaths just starting late 2013
10 Pathogenesis
11 Sepsis and septic shock Bacterial infection Excessive host response (SIRS) Host factors lead to cellular damage Organ damage Death



12 Sequelae of Sepsis Balanced response Resolution Host hyper-responsive SIRS/sepsis and Multi-Organ Dysfunction Host hypo-responsiveness Overwhelming sepsis and death

13 N Engl J Med 2013;369: DOI: /NEJMra

14 Host response N Engl J Med 2013;369:840-51

15 Organ failure N Engl J Med 2013;369:840-51
16 Recognition
17 Frequent failures Failure to recognise deteriorating patient Failure to recognise sepsis Postural hypotension Raised respiratory rate Hypoxia Acidosis



18 Scoring systems Gradation of specific state eg GCS Composite scores Readily available data eg age, pulse etc With/without laboratory variables Uses Diagnostic discrimination eg Meningitest Predict death/deterioration eg APACHE Determine management eg CURB 65
 NICE track& trigger tool")
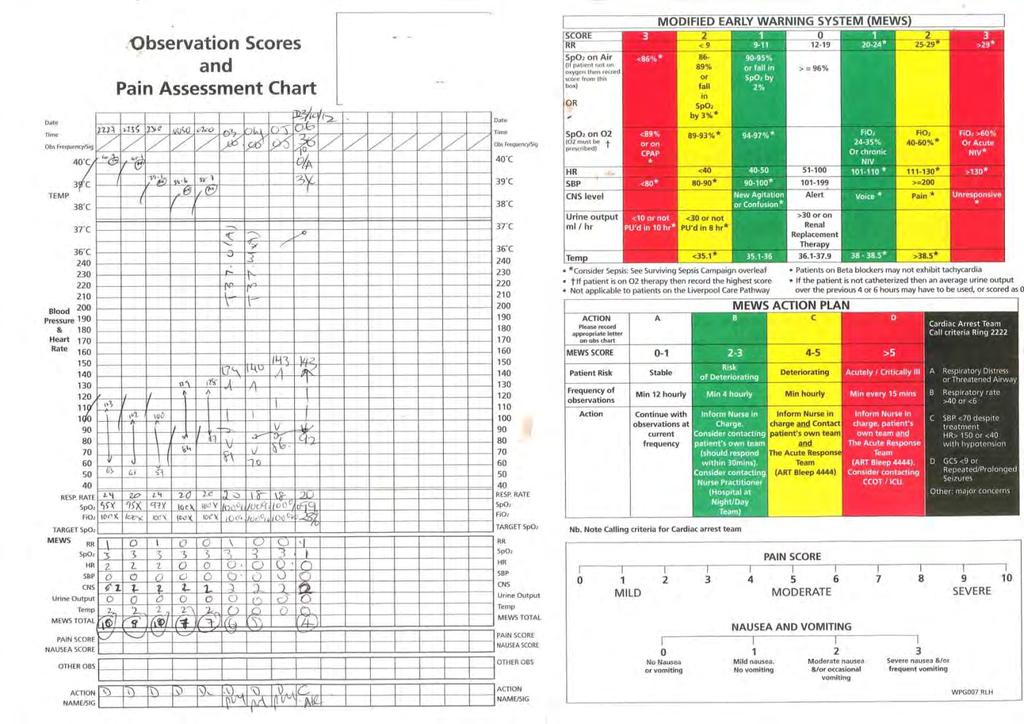
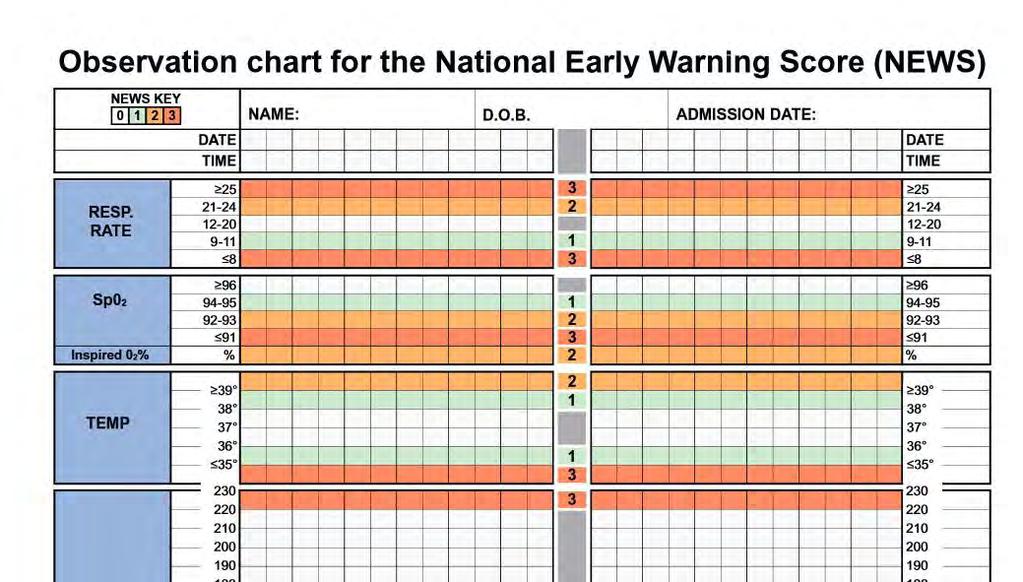
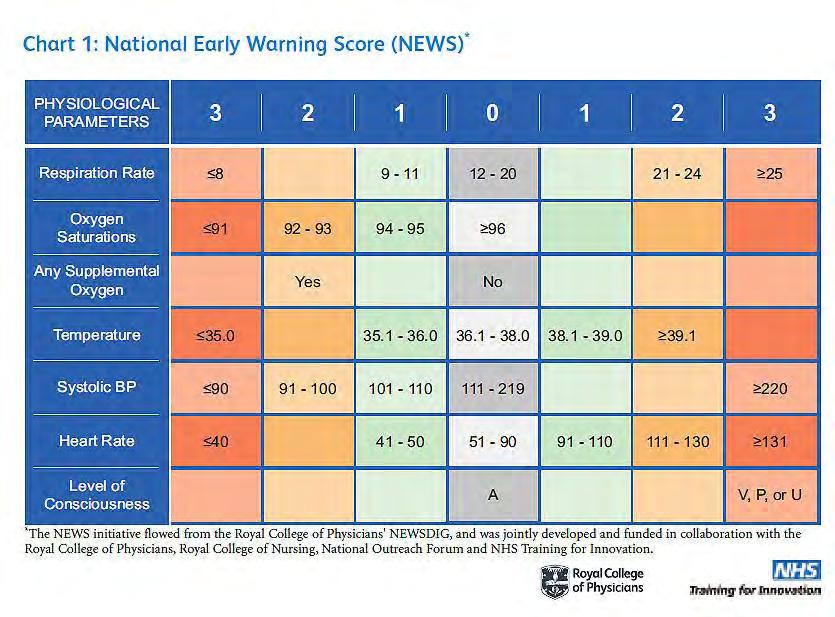
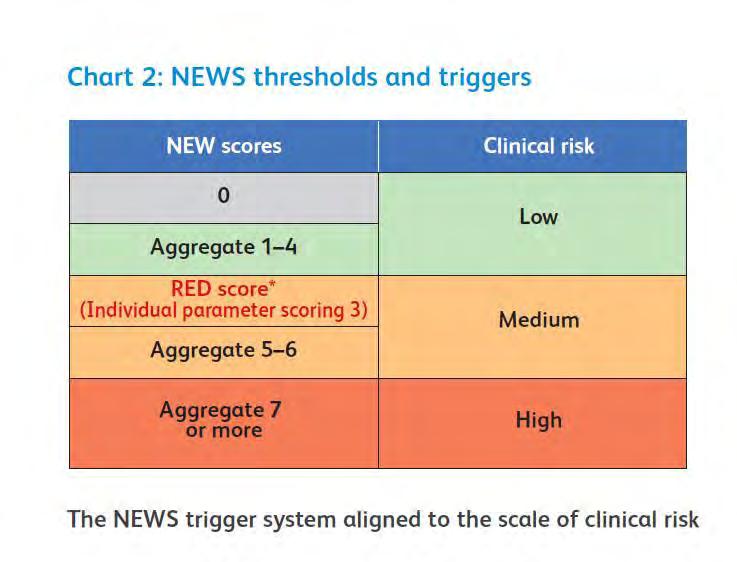
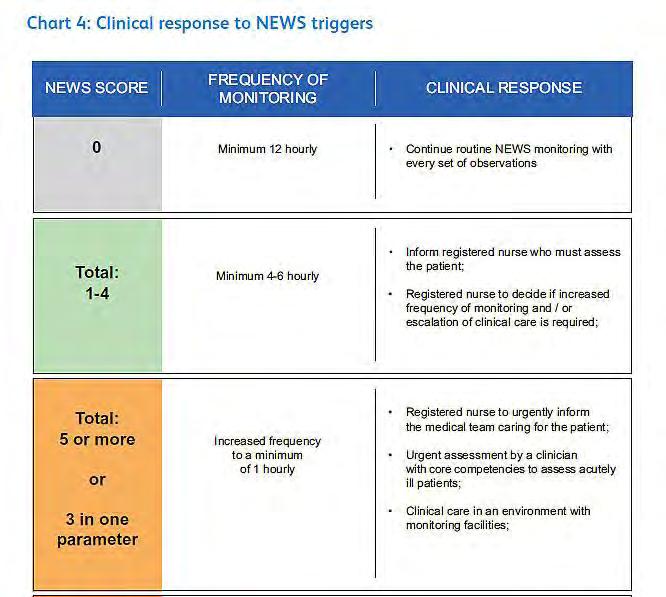
19 Track and trigger tools Modified Early Warning Score Simple measurements to alert busy ward staff of patient deterioration (MEWS) NICE track& trigger tool (2007)
20

21
22

23 Primary aim To identify sick patients early To detect and document changes in status To dictate changes in management In a standard manner across the NHS
24
25
26

27
28
29
30
31 Caveats Resources are needed to measure and record data Nurses Charts Information technology Need to review and act on changes Scores may not reflect illness severity in a minority review the patient too! Only validated in specific settings

32 Acute Med 2011; 10(3): patients at National Hospital, Colombo Useful to alert staff/prioritise need for ICU Modification to include age and laboratory parameters increases predictive values
:")
33 PLoS One May 2013; 8 (5): e64340

34 Frequent failures Failure to act on MEWS scores Failure to recognise sepsis Postural hypotension Raised respiratory rate Hypoxia Acidosis Failure to look for focal signs Source Metastatic spread Failure to take blood cultures or do LP
35 Management

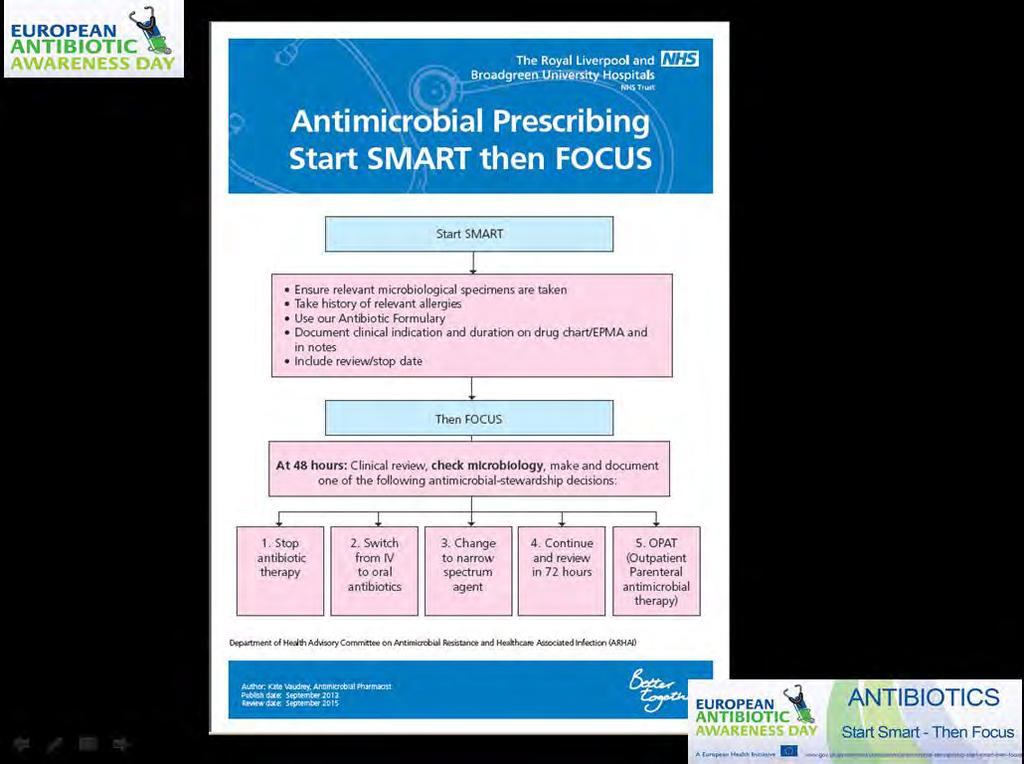
36 Severe sepsis - management Early resuscitation (ABC) Adequate fluid replacement Control of blood sugar Appropriate antibiotics Source control Role of steroids Other ancillary treatments eg GCSF, activated protein C

37 Surviving sepsis Dellinger et al. Crit Care Med 2004; 32:

38 Surviving Sepsis Campaign
 If hypotensive If serum lactate >4 Infection source identification & control Goal directed therapy for septic shock CVP>8, MAP>65 mmhg")
39 Resuscitation bundle <6hrs Measure serum lactate (or base excess) Blood cultures (x2) before antibiotics Broad spectrum antibiotic Within 3 hours in emergency room Within 1 hour in inpatient setting Begin goal directed fluid resuscitation (initial bolus 20ml/kg) If hypotensive If serum lactate >4 Infection source identification & control Goal directed therapy for septic shock CVP>8, MAP>65 mmhg

40 Early goal directed therapy Purpose: to adjust cardiac preload, afterload and contractility to balance oxygen delivery with oxygen demand Entry criteria: patients in the emergency dept with severe sepsis & shock Plan: randomise to 6h of EGDT before transfer to ICU Rivers et al, N Engl J Med :1368

 or mixed venous")
41 Initial resuscitation of sepsis: therapeutic goals Central venous pressure: 8 12 mmhg Mean arterial pressure: 65 mmhg Urine output: 0.5 ml/kg/h Central venous (SVC) or mixed venous oxygen saturation: 70%

42 Crit Care Med 2013 Feb;41(2): references Consensus using GRADE criteria

 risk of tachyarrhythmias Tight glucose control is harmful")
43 Sepsis Campaign 2012 update Antibiotics asap within 1 hour of septic shock or severe sepsis Fluids 30ml/kg and use crystalloids in severe sepsis and septic shock Crystalloids are preferable to colloids Use albumin if substantial amounts of crystalloids Target decreasing lactate with resuscitation Conflicting trials however increased need for renal replacement Rx using hydroxyethyl starches Use noradrenaline not dopamine (meta-analysis) risk of tachyarrhythmias Tight glucose control is harmful (target 180 mg%)

44 22 May 2012 at NEJM.org ( /NEJMe )
45 Non-antibiotic therapy for sepsis evidence base? Goal directed therapy Low dose steroids (CORTICUS) Intensive insulin therapy tight glycaemic control Activated protein C (PROWESS etc)
 No Intensive insulin therapy tight")
46 Non-antibiotic therapy for sepsis evidence base? Goal directed therapy Some Low dose steroids (CORTICUS) No Intensive insulin therapy tight glycaemic control No Activated protein C (PROWESS etc) No
47 Frequent medical failures Failure to recognise sepsis Postural hypotension Raised respiratory rate Hypoxia Acidosis Failure to look for focal signs Source Metastatic spread Failure to take blood cultures or do LP
48 Antimicrobials


49 Antibiotics in sepsis There is no, single, best regimen Consider the site of the infection Consider which organisms most often cause infection at that site Consider local resistance patterns Choose antibiotic(s) with appropriate spectrum After obtaining cultures, give antibiotics quickly and empirically at appropriate dose Revise the regimen as soon as culture & sensitivity results allow
 Toxicity")
50 Rational choice of antibiotics Efficacy Spectrum of activity Pharmacokinetics & pharmacodynamics Patterns of resistance Quality of manufacture (generics, forgery) Toxicity Availability Cost

51 Kumar A et al. Chest 2009; 136:
52 Appropriate antibiotics Study of 5715 patients in 3 countries Wide range of infection, in septic shock 80% received appropriate antibiotics Survival appropriate 52% inappropriate 10.3% adj OR 8.99 (95%CI ) p< Kumar A et al. Chest 2009; 136:

53 Timing of antibiotics Kumar A et al. Crit Care Med 2006; 34: Retrospective cohort 10 ICU N=2731 septic shock Survival if antibiotics given within 1 hr =79.9% Each further hour of delay decreases survival by 7.6%
54 Only 51.4% received antibiotics within 6 hours Kumar A et al Crit Care Med 2006; 34:
55 Common system failures Failure to record MEWS scores Failure to act on MEWS scores Nurses calling doctors Doctors responding to call Doctors using care bundle early Escalating decision to seniors Provision of resources including outreach teams and ICU

56 Common antimicrobial Failure to start early mistakes Failure to review previous laboratory results Failure to take into account previous antibiotic usage Failure to target therapy Failure to review later

57 Antibiotic policies Limit by consultation Limit by paperwork Limit by selective lab reporting Trust guidelines/formulary Audit & reinforce Concept of antibiotic stewardship

58 Guidelines PublicationsPolicyAndGuidance/DH_131062

59
60
61
62
63
64
65
66
67
68
69 Integration of AS and IPC


70 Point Prevalence of Antimicrobial Prescribing in European Hospitals 2009 ESAC-3 30% of inpatients were treated with antibiotics The proportion for treating HAI was 35%

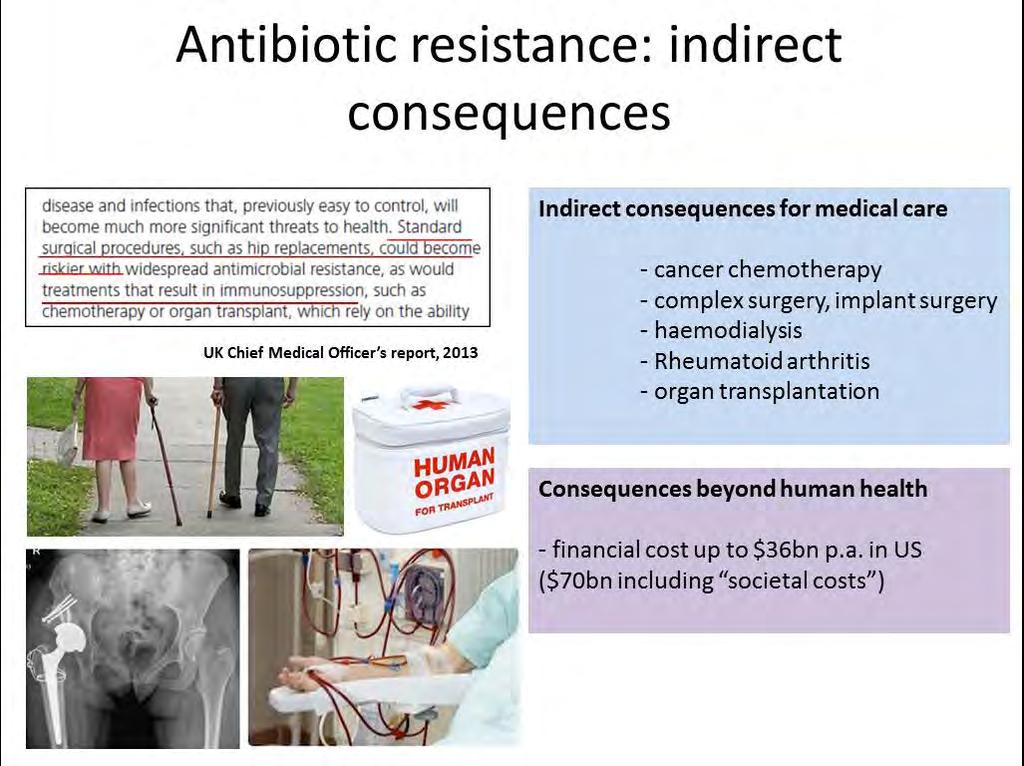
71 UK CMO Report 2013

72 UK CMO Report 2013

73 UK CMO Report 2013 Acute trusts and their boards will need to learn a new language and consider how to strengthen infection prevention and control practice using new methods of organisational and behavioural change to reinforce policy implementation.


74 Policies and guidelines are not enough. J Carthey et al BMJ 2011; 343





75 What could be done differently? How can we do better? Consider: Organisation Systems Teams
76 Organisational Approach required Increasing recognition in last five years that an organisational approach is required, along with appropriate technical expertise


77 Organisational Approach required Increasing recognition in last five years that an organisational approach is required, along with appropriate technical expertise


78 Whole Systems Approach Charani et al JAC 2010 Necessary to understand the factors that influence prescribing behaviour and decisions Address human factors Supporting choice architecture Making some small changes to existing systems Adopt a whole-system approach to support optimal prescribing choices

79 Greater Understanding of Antimicrobial Prescribing Behaviours Interventions to optimize antimicrobial prescribing behaviour are of poor quality and are not based on robust theoretical science. Behaviour and social science research is underutilized in the development of antimicrobial prescribing interventions. Qualitative evidence highlights the influence of social norms, attitudes, and beliefs on antimicrobial prescribing behaviour When designing and evaluating interventions in antimicrobial prescribing, these influences on prescribing are generally not considered. Charani E et al CID; 2011;53(7):651 62


80 Successful interventions based on.. Social process The sense of community Bottom up approach Importance of systems with network and teams The Milbank Quarterly 2011; 89(2):
81 Summary There are internationally agreed programmes on management of sepsis Adherence to these is often poor Simple approaches are required at every level of health care Sustained behaviour change requires a truly multidisciplinary approach
 Royal Liverpool University Hospital Dr Panduka Karunanayake")
82 Prof Jon Cohen Acknowledgments Brighton & Sussex Medical School Prof Alison Holmes Imperial College London Drs Mike Beadsworth, Emmanuel Nsutebu, Jonathon Folb Kate Vaudrey, Anne Neary (Pharmacists) Royal Liverpool University Hospital Dr Panduka Karunanayake Colombo
83 شكرا لكم على ا هتمامكم Thank you for your attention
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Sepsis and Antimcrobial Stewardship: Are they really mutually Exclusive?
 Sepsis and Antimcrobial Stewardship: Are they really mutually Exclusive? DR KATE ADAMS CONSULTANT INFECTIOUS DISEASES HULL AND EAST YORKSHIRE NHS TRUST AMS Sepsis No! At least not if the sepsis programme
Sepsis and Antimcrobial Stewardship: Are they really mutually Exclusive? DR KATE ADAMS CONSULTANT INFECTIOUS DISEASES HULL AND EAST YORKSHIRE NHS TRUST AMS Sepsis No! At least not if the sepsis programme
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Severe Sepsis/ Septic Shock. Fereshte Sheybani, MD. Assistant Professor in Infectious Diseases
 Severe Sepsis/ Septic Shock Fereshte Sheybani, MD. Assistant Professor in Infectious Diseases Sepsis is one of the oldest and most elusive syndromes in medicine. Hippocrates claimed that sepsis (σήψις)
Severe Sepsis/ Septic Shock Fereshte Sheybani, MD. Assistant Professor in Infectious Diseases Sepsis is one of the oldest and most elusive syndromes in medicine. Hippocrates claimed that sepsis (σήψις)
Saving Lives: Focusing on Severe Sepsis and Septic Shock
 Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Saving Lives: Focusing on Severe Sepsis and Septic Shock Deborah Cameron, RN, CPHQ Paul Pratt, RN Glenn Russ, RN Providence Little Company of Mary Medical Center San Pedro January 18, 2011 Objectives 1.
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Timing of Vasopressors in Septic Shock: How Soon is Too Soon?
 Timing of Vasopressors in Septic Shock: How Soon is Too Soon? Anand Kumar, MD Sections of Critical Care Medicine and Infectious Diseases Professor of Medicine, Medical Microbiology and Pharmacology University
Timing of Vasopressors in Septic Shock: How Soon is Too Soon? Anand Kumar, MD Sections of Critical Care Medicine and Infectious Diseases Professor of Medicine, Medical Microbiology and Pharmacology University
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
3/14/2017. Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care. Objectives. Developmental Response to Sepsis
 Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Sepsis and Septic Shock: New Definitions for Adults
 PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
The Oxford AHSN Sepsis Pathway
 From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway
 Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Where did it all begin?
 EXPLORE Healthcare Summit Sepsis: Can We Finally Just Relax on the SOFA? Mark Keuchel, D.O. Background: 1. Sepsis is a wide-spectrum disease process that remains poorly understood 2. Early-goal directed
EXPLORE Healthcare Summit Sepsis: Can We Finally Just Relax on the SOFA? Mark Keuchel, D.O. Background: 1. Sepsis is a wide-spectrum disease process that remains poorly understood 2. Early-goal directed
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Severe Sepsis & Septic Shock
 The College of Emergency Medicine Clinical Audits Severe Sepsis & Septic Shock EXCELLENCE IN EMERGENCY MEDICINE Contents Executive summary 3 Introduction 4 Audit history 4 Format of this report 4 Analysis
The College of Emergency Medicine Clinical Audits Severe Sepsis & Septic Shock EXCELLENCE IN EMERGENCY MEDICINE Contents Executive summary 3 Introduction 4 Audit history 4 Format of this report 4 Analysis
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Sepsis in primary care. Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells
 Sepsis in primary care Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells sepsisnurses@uhcw.nhs.uk Quiz!! OR Hands on your heads Hands on your hips Definition. The Third International Consensus Definition
Sepsis in primary care Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells sepsisnurses@uhcw.nhs.uk Quiz!! OR Hands on your heads Hands on your hips Definition. The Third International Consensus Definition
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
CEM Clinical Audits Severe Sepsis & Septic Shock
 CEM Clinical Audits 2011-12 Severe Sepsis & Septic Shock Introduction This report shows the results from an audit of the treatment of severe sepsis and septic shock against the clinical standards published
CEM Clinical Audits 2011-12 Severe Sepsis & Septic Shock Introduction This report shows the results from an audit of the treatment of severe sepsis and septic shock against the clinical standards published
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare