Digestive Pathology Lecture 7
|
|
|
- Lora Shields
- 6 years ago
- Views:
Transcription
1 Digestive Pathology Lecture 7 Reproduction Prohibited This file contains original text and images as well as materials adapted from copyrighted sources For use only as a temporary educational aid Partially or completely copying or distributing the contents of this file may constitute an infringement of the fair use exception for teaching faculty of the U.S. Copyright Law LSUHSC-New Orleans, 2015 Last updated October 1, 2015
2 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms

3 Duplicated/accessory gallbladder

4 Septate/bilobed, diverticular, malplaced gallbladder

5 Gallbladder, folded fundus, phrygian cap
6 Biliary atresia Complete obstruction Manifest within the first 3 months of life One-third of infants with neonatal cholestasis If untreated, secondary biliary cirrhosis develops within 3-6 months Accounts for 50-60% of children referred for liver transplantation Is the most common cause of death from liver disease in early childhood
7 Biliary atresia, two forms Fetal (aberrant development), 20% Perinatal (normal development, secondary injury), the most common Viral infection Apoptosis of bile duct epithelium Abnormal inflammatory response Genetic predisposition
:")
8 Biliary atresia etiology Pre- or perinatal viral infection (rotavirus, reovirus, cytomegalovirus), apoptosis of bile duct epithelium with aberrant MHC class II antigens expression, eliciting an abnormal inflammatory response in a geneticallypredisposed host, resulting in fibrosis and complete bile duct obstruction Semin Liver Dis 2012; 32(04):
9 Biliary atresia, Three types Type I: Common bile duct involved Patent proximal ducts Type II: Hepatic duct involved Patent (IIa) OR obliterated (IIb) cystic and common bile ducts Type III (majority of cases): Complete extrahepatic biliary atresia (including right and left hepatic ducts)
10 Biliary atresia, types Hepatic duct Common bile duct Hepatic duct, cystic duct & common bile duct Complete


11 Biliary-enteric anastomosis (A, B and C) Hepatoportoenterostomy (Kasai procedure, E, F)

12 Hepatoportoenterostomy (Kasai procedure) View of porta hepatis after transection. Gallbladder and all extrahepatic ducts have been removed from patient with type 3 biliary atresia. Several scattered small ducts are visible on the portal plate (arrows show portal plate). The Lancet, 374, 9702, 2009:
13 Choledochal cysts Congenital cystic dilatations or diverticula of the bile ducts Most manifest before age 10 More common in females, 4:1
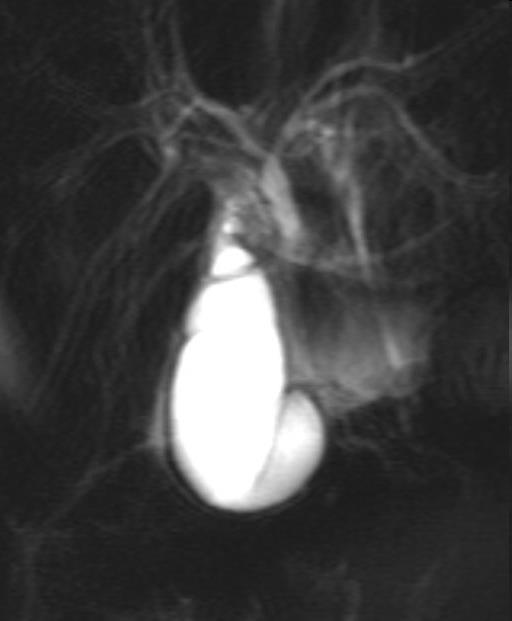
14 Choledochal cysts Single Dilatations (80-90%) Diverticulum Choledochocele Multiple Dilatations Caroli s
 Radiographics.rsna.")
15 Choledochocele ERCP image of a choledochocele, or type III choledochal cyst (arrow) Radiographics.rsna.org
, dilated common bile duct (black")

16 Choledochocele 31-year-old man with recurrent pancreatitis and choledochocele. ERCP demonstrates choledochocele (white arrow), dilated common bile duct (black arrow) and pancreatic duct (arrowhead) Intraoperative photograph shows open duodenum with cyst bulging into the lumen. Radiology Case Reports, Vol 3, No 3 (2008)
17 Choledochal cysts May cause: Neonatal cholestasis Recurrent biliary colic and/or jaundice Pancreatitis Predispose to: Stones Inflammation Stenosis Pancreatitis Cholangiocarcinoma

18 Choledochal cyst, type I Excision, biliary-enteric anastomosis Odze, Surgical Pathology of the GI Tract, Liver Biliary Tract and Pancreas
19 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms
20 Cholelithiasis Calculi (stones) in the gallbladder (gallstones) Present in 10-20% of the population Most are silent May cause RUQ/epigastric pain constant or postprandial (after fat-rich meals) Subsides gradually in 1 to 5 hours may radiate to the right scapular region may associate nausea and vomit
21 Gallstones, shape, size When solitary or few: large, round or oval When multiple: faceted (molded) Size decreases in proportion to their number Very small stones, called gravel, are more likely to escape the gallbladder and produce biliary obstruction Thick bile is called sludge, may also cause obstruction


22 Gallstones, rounded, faceted
23 Gallstones, composition Different amounts of: Cholesterol (yellow) Calcium bilirubinate (green-black) Calcium carbonate (gray-white) Classified as: Pure Mixed (80%) Combined (nucleus, shell)


24 Mixed stones

25 Combined stones
26 Gallstones, also classified as Cholesterol stones (80%) When made predominantly of cholesterol Pale-yellow, yellow-green, yellow-gray Pigmented When made predominantly of calcium bilirubinate Brown or jet black


27 Cholesterol stones


28 Pigmented stones
29 Gallstones, radiology Pure cholesterol stones are radiolucent Mixed/combined stones are radiopaque depending on their concentration of calcium

30 Gallstones, plain film

31 Gallstones, ultrasound
32 Cholesterol stones, nucleation In the bile, cholesterol is kept soluble by aggregation with phospholipids and bile acids (lithogenic index) Nucleation (crystallization) of cholesterol is promoted by Supersaturation of bile with cholesterol Microprecipitates of inorganic or organic calcium salts

33 Cholesterol, lecithin, bile acids balance Only below the solid line cholesterol is kept in solution (micelles)
34 Risk factors, cholesterol stones Native Americans, Hispanics, Northern European Age > 55 Female sex, oral contraceptives, estrogen replacement therapy, pregnancy Obesity Rapid weight reduction (gastric bypass) Hyperlipidemia Some cholesterol-lowering medications (fibrates) may increase the risk, others (statins) may decrease the risk Ileal dysfunction or bypass Gallbladder stasis Family history
35 Genetic mechanisms Cholesterol transporter ABCG5/G8 mutation: Cholesterol hypersecretion CYP7A1 mutation: Deficiency in the synthesis of bile acids MDR3 mutation: Defective phospholipid export pump in the canalicular membrane
36
37 Risk factors, pigmented stones Asian populations Hemolytic disorders (hyperbilirubinemia) Bacterial colonization of the biliary tree (bacterial glucuronidases) Parasitic colonization of the biliary tree (Ascaris lumbricoides, trematodes)

38 Pigmented gallstones Faceted pigmented gallstones in a gallbladder from a patient with a mechanical mitral valve prosthesis, leading to chronic intravascular hemolysis. Robbins Cotran
39 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms
40 Cholesterolosis Accumulation of cholesterol esters in foamy histiocytes within the lamina propria Related to cholesterol hypersecretion Grossly: strawberry gallbladder


41 Cholesterolosis


42 Cholesterolosis, strawberry gallbladder
43 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms
44 Cholecystitis Inflammation of the gallbladder Acute vs. chronic Calculus (majority) vs. acalculous
45 Acute cholecystitis Obstruction of gallbladder neck or cystic duct, by stones, gravel or sludge (90%) Acute acalculous cholecystitis Postpartum, postoperative, trauma, sepsis, shock Ischemia/shock (cystic artery is an end-artery with no collateral circulation) Prolonged restriction of oral feeding (lack cholecystokinin-induced contraction) Primary bacterial infection (diabetes, immunosuppression, HIV/AIDS)
46 Acute cholecystitis Symptoms: Nausea, vomiting Right upper quadrant, epigastric pain > 6 hours Murphy s sign Mild fever Mild to moderate leukocytosis Absence of high fever, chills, jaundice or hyperbilirubinemia Usually subsides within days May require immediate surgery Recurrence is common Acalculous cholecystitis is masked by underlying condition, high risk of gangrene and perforation

47 Acute cholecystitis
48 Chronic cholecystitis Cholelithiasis >90% Obstruction not always found Clinically Recurrent attacks of RUQ/epigastric pain as described for cholelithiasis Microscopically Chronic inflammation and fibrosis Outpouchings of the mucosa (Rokitansky-Aschoff sinuses)


49 Rokitansky-Aschoff sinuses


50 Porcelain gallbladder
51 Cholecystitis, complications Choledocholithiasis, cholangitis Sepsis Perforation, abscess, peritonitis Cholecystenteric fistula Gallstone ileus



52 Cholecystenteric fistula Gallstone ileus
53 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms
54 Choledocholithiasis Stones within the common bile duct Most originate in the gallbladder May also form within the bile duct with cysts, bacterial and parasitic infections Obstruction may cause: Pain and jaundice Cholangitis Secondary biliary cirrhosis Pancreatitis
55 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms
56 Cholangitis Inflammation of the biliary tract Results most commonly from Choledocholithiasis Other sources of obstruction Indwelling catheters Strictures Tumors Parasites Acute pancreatitis
57 Cholangitis, clinical findings The Charcot triad: RUQ pain Fever, chills Jaundice/hyperbilirubinemia
58 Cholangitis, complications Is a medical emergency, requires Prompt antibiotic therapy Endoscopic biliary drainage Surgical evacuation May cause: Hepatic abscesses Sepsis

59 Pyogenic abscesses, acute cholangitis
60 Gallbladder, extrahepatic biliary tract 1. Congenital abnormalities 2. Cholelithiasis 3. Cholesterolosis 4. Acute and chronic cholecystitis 5. Choledocholithiasis 6. Cholangitis 7. Neoplasms Gallbladder adenomas Gallbladder carcinomas Carcinomas of the extrahepatic bile ducts
61 Gallbladder adenomas Rare Similar to colonic adenomatous polyps may have a tubular, tubulovillous or villous architecture But are lined by gastric-type, intestinal-type or biliary-type epithelium Have malignant potential



62 Gallbladder adenomas J. Albores-Saavedra et al. Adenomas of the gallbladder. Human Pathology, 43:1506, 2012
63 Gallbladder cancer Infrequent Most are adenocarcinomas Risk factors: Gallstones (the strongest risk factor) Obesity Female sex, multiparity Old age In the US, higher rates in: Native Americans, Hispanics, Korean and Chinese Salmonella typhi/paratyphi, Helicobacter bilis, Helicobacter pylori, trematodes Anomalous pancreatobiliary junction


64 Gallbladder cancer


65 Gallbladder cancer
66 Gallbladder cancer Preoperative diagnosis is exceptional Symptoms are those associated with cholelithiasis Dismal survival
67 Carcinoma of extrahepatic bile ducts Most are adenocarcinomas Slightly more frequent in men Association with: Primary sclerosing cholangitis, IBD Choledochal cysts Trematodes
68 Carcinoma of extrahepatic bile ducts Signs (Courvoisier s sign): Progressive jaundice Painless, palpable gallbladder Most are not resectable Short survival


69 Ampullary, periampullary carcinoma

70 Klatskin s tumor
71 Pancreas 1. Congenital malformations Pancreas divisum Annular pancreas Ectopic pancreas Congenital cysts 2. Pancreatitis 3. Pancreatic cystic neoplasms 4. Pancreatic ductal adenocarcinoma 5. Pancreatic endocrine neoplasms

72 Pancreas divisum Dorsal and ventral duct systems fail to fuse Accessory duct Main duct Primordia fail to fuse Accessory duct minor papilla Main duct major papilla

73 Annular pancreas Tethering of the ventral primordium as it rotates A. Dorsal and ventral primordia at about 4 weeks of development. B. Tethering of the ventral bud tip to the duodenum and rotation lead to a ring of pancreatic tissue encircling the duodenum. C. annular pancreas with pancreas divisum; this combination is present in 29% of adult patients. Journal of the American College of Surgeons Volume 206, issue 5, 2008:
74 Ectopic/accessory pancreas Stomach Duodenum Jejunum Ileum Meckel diverticulum Mesentery May cause: Inflammation, bleeding Tumors


75 Congenital pancreatic cysts Autosomal dominant polycystic kidney disease Von Hippel Lindau disease. (a) Contrast material enhanced CT scan shows enhancing septa separating congenital pancreatic cysts. (b) Axial T2-weighted MR image shows cystic replacement of the pancreas and a serous microcystic pancreatic adenoma (arrow). RadioGraphics, 2006, 26:715
76 Pancreas 1. Congenital malformations 2. Pancreatitis Acute pancreatitis Pancreatic pseudocyst Chronic pancreatitis Autoimmune pancreatitis 3. Pancreatic cystic neoplasms 4. Pancreatic ductal adenocarcinoma 5. Pancreatic endocrine neoplasms
77 Acute pancreatitis, main causes 80% of cases: Alcohol (males) Biliary obstruction by gallstones (females) Cryptogenic: 10-20% (biliary sludge)
78 Acute pancreatitis, other causes Pancreas divisum, annular pancreas, choledochocele Periampullary tumors Hypertriglyceridemia Hypercalcemia, hyperparathyroidism Drugs (thiazide diuretics) Trauma (blunt, surgical) Ischemia (shock, vasculitis) Infections (Mumps) Mutations in trypsinogen Mutations in serine protease inhibitor Mutations causing abnormal bicarbonate secretion
79 Defense mechanisms Most pancreatic enzymes are secreted as proenzymes Proenzymes are activated by trypsin Trypsinogen is activated in the duodenum by enteropeptidase, avoiding intrapancreatic activation of other proenzymes Pancreatic acinar and ductal cells secrete trypsin inhibitors (serine protease inhibitor Kazal type 1) Lipase is secreted in its active form; however, for optimal function it requires colipase that does require activation by trypsin in the intestinal lumen
80 Acute pancreatitis, pathogenesis Pancreatitis occurs when normal defenses are deranged mostly by abnormal intrapancreatic activation of trypsin Alcohol Direct toxic effect Protein-rich secretion, protein plugs Contraction of sphincter of Oddi Obstruction by stones, gravel, sludge, choledochocele, tumors Viruses, drugs, trauma (direct acinar injury)
81 Hereditary pancreatitis Cationic trypsinogen gene mutation: Cleavage-resistant trypsin Serine protease inhibitor Kazal type 1 mutation: Inactive serine protease, an essential trypsin inhibitor Cystic fibrosis CFTR gene mutation: Abnormal bicarbonate secretion, inspissated secretions
82 Acute pancreatitis, morphology Inflammation Fat necrosis Released fatty acids combine with calcium to form dark precipitates Destruction of the parenchyma and vessels, hemorrhage


83 Acute pancreatitis


84 Acute pancreatitis
85 Acute pancreatitis Precipitated by: Alcoholic binge Overeating Drugs (opiates) Epigastric pain Stabbing, severe, referred to the upper back Jaundice If there is concomitant obstruction of the bile duct Hemorrhagic exudates: Periumbilical ecchymosis Flank ecchymosis Nodules of subcutaneous fat necrosis

86 Cullen s sign

87 Cullen s sign Periumbilical Turner s sign Flank

88 Subcutaneous fat necrosis
89 Acute pancreatitis, laboratory Elevation of amylase Elevation of lipase Hypocalcemia Hyperglycemia Leukocytosis Electrolyte disturbances
90 Acute pancreatitis, complications Disseminated intravascular coagulation Acute respiratory distress syndrome Shock, acute renal failure Abscess (sterile or infected) Splenic/portal venous thrombosis Pancreatic pseudocyst
91 Pancreatic pseudocyst Walled-off collection of debris and fluid rich in pancreatic enzymes Wall lacks epithelial lining Usually solitary Arise after episodes of acute pancreatitis, chronic pancreatitis with acute exacerbation May be caused by trauma (blunt, penetrating or operative) May retain a communication with the ductal system


92 Pancreatic pseudocyst
93 Pancreatic pseudocyst May Resolve spontaneously Become infected Compress adjacent structures Erode into adjacent vessels causing abundant bleeding Rupture
94 Chronic pancreatitis, causes Repeated bouts of acute pancreatitis Alcoholism, the most common cause Long-standing pancreatic duct obstruction (gallstones, neoplasms) Pancreas divisum Hereditary pancreatitis Tropical pancreatitis Autoimmune pancreatitis Idiopathic, up to 40%

95 Chronic pancreatitis, fibrosis, atrophy, dilated ducts with calcified concretions

96 Chronic pancreatitis calcifications


97 Chronic pancreatitis Fibrosis, chronic inflammation, acinar loss, fusion of islets, ductal dilatation with calcified concretions
98 Chronic pancreatitis, outcome Atrophy: With repeated attacks of acute pancreatitis amylase and lipase may fail to elevate after a substantial portion of the acinar parenchyma is lost Malabsorption (pancreatic insufficiency) Diabetes Chronic pain Pancreatic cancer With hereditary pancreatitis, 40% risk
99 Autoimmune pancreatitis Periductal inflammation with abundant IgG4- secreting plasma cells Periductal fibrosis with ductal narrowing Response to steroid treatment Older men Involvement of bile ducts and gallbladder and many other organ systems (IgG4-related disease) Often presents with obstructive jaundice, mimicking pancreatic cancer

100 Autoimmune pancreatitis
101 Pancreas 1. Congenital malformations 2. Pancreatitis 3. Pancreatic cystic neoplasms Serous Mucinous Intraductal papillary mucinous 4. Pancreatic ductal adenocarcinoma 5. Pancreatic endocrine neoplasms
102 Serous cystadenomas More common in women Microcystic (numerous small cysts) Clear, thin, straw-colored fluid Low cuboidal epithelium Almost always benign

103 Serous cystadenoma
104 Mucinous cystic neoplasm Arise almost exclusively in women Macrocystic (few large cysts) Thick, mucinous fluid Tall columnar epithelium Can be benign or malignant


105 Mucinous cystic neoplasm
106 Intraductal papillary mucinous neoplasm More common in men Arise in the main pancreatic ducts Intraductal proliferation of mucinous cells in papillary arrangements Mucin accumulation leads to cystic dilatation May be multifocal Can be benign or malignant

107 Intraductal papillary mucinous neoplasm


108 Intraductal papillary mucinous neoplasm
109 Pancreas 1. Congenital malformations 2. Pancreatitis 3. Pancreatic cystic neoplasms 4. Pancreatic ductal adenocarcinoma 5. Pancreatic endocrine neoplasms
110 Pancreatic (ductal) adenocarcinoma Incidence and mortality Greater in men than in women Greater in blacks than in whites Greater in Acadiana 5-year survival rate < 5%
111 Pancreatic cancer, incidence rate
112
113 Pancreatic adenocarcinoma, risk factors Smoking High-protein, high-fat diets Chronic pancreatitis, diabetes Hereditary pancreatitis Alcohol Exposure to gasoline products, pesticides Hereditary nonpolyposis colorectal cancer BRCA2, hereditary breast and ovarian cancer Peutz-Jeghers syndrome p16 mutation, 95% KRAS mutation, 80-90%

114 Genetic progression Annual Review of Pathology: Mechanisms of Disease. 2008;3:

115 Pancreatic intraepithelial neoplasia
116 Pancreatic adenocarcinoma, morphology Location: 60% arise in the head 20% diffusely 15% in the body 5% in the tail Microscopically: High invasiveness (perineural invasion, lymphatic invasion) Desmoplastic (scirrhous, fibrous)


117 Pancreatic ductal carcinoma, desmoplasia



118 Pancreatic ductal carcinoma Desmoplasia, perineural invasion
119 Clinical findings Pain Obstructive jaundice, palpable non-tender gallbladder (Courvoisier s sign) Migratory thrombophlebitis (Trousseau sign) Tumor procoagulants Tumor marker: CA19-9 Fewer than 20% are resectable
120 Pancreas 1. Congenital malformations 2. Pancreatitis 3. Pancreatic cystic neoplasms 4. Pancreatic ductal adenocarcinoma 5. Pancreatic endocrine neoplasms Insulinoma Gastrinoma Glucagonoma Other
121 Pancreatic endocrine neoplasms Only 2% of all pancreatic neoplasms May elaborate hormones Some are non-functional Morphologically similar to carcinoids May be associated with MEN I syndrome, hyperplasia or adenomas in: Pancreatic islets Adrenal cortex Parathyroid Pituitary


122 Pancreatic neuroendocrine tumor
123 Beta-cell tumors (insulinomas) The most common type May cause severe hypoglycemia Whipple triad: Fatigue, confusion, stupor, coma, convulsions Glucose < 50 mg/dl Attacks precipitated by fasting/exercise and relieved by feeding/glucose Usually small and encapsulated Only about 10% metastasize
124 G-cell tumors (gastrinomas) Located in the gastrinoma triangle : duodenum, pancreas and peripancreatic soft tissues Zollinger-Ellison syndrome Hypergastrinemia Multiple peptic ulcers (gastric, duodenal, jejunal), unresponsive to therapy Diarrhea Over half locally invasive or have metastasized at the time of diagnosis
125 Alpha-cell tumors (glucagonoma) Cause the glucagonoma syndrome: Mild diabetes Necrolytic migratory erythema Deep vein thrombosis Anemia Tendency to develop overwhelming infections Seen mostly perimenopausal and postmenopausal women Approximately 50% have metastases at the time of diagnosis

126 Necrolytic migratory erythema
127 Other endocrine neoplasms Somatostatinoma (Delta-cell tumors), may present with diabetes VIPomas (vasoactive intestinal peptide), may present with secretory diarrhea Carcinoids Tumors producing more than one hormone
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
Cholelithiasis (Gallstones)
") GALL BLADDER Cholelithiasis (Gallstones) Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates are higher in Latin American countries (20-40%)
GALL BLADDER Cholelithiasis (Gallstones) Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates are higher in Latin American countries (20-40%)
Diseases of exocrine pancreas
 Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Dr. Attila Zalatnai PATHOLOGY OF THE BILIARY TRACT AND PANCREAS
 Dr. Attila Zalatnai PATHOLOGY OF THE BILIARY TRACT AND PANCREAS MAIN COMPONENST OF THE BILE bile acid salts bilirubin (conjugated, direct!) cholesterol phospholipids fatty acids mucoproteins calcium water
Dr. Attila Zalatnai PATHOLOGY OF THE BILIARY TRACT AND PANCREAS MAIN COMPONENST OF THE BILE bile acid salts bilirubin (conjugated, direct!) cholesterol phospholipids fatty acids mucoproteins calcium water
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Radiology of hepatobiliary diseases
 GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
Sonography of Gall Bladder
 Sonography of Gall Bladder Vikram Dogra,MD Professor of Radiology, Urology and BME Director of Ultrasound Associate Chair of Education and Research University of Rochester, NY Objectives Describe the Congenital
Sonography of Gall Bladder Vikram Dogra,MD Professor of Radiology, Urology and BME Director of Ultrasound Associate Chair of Education and Research University of Rochester, NY Objectives Describe the Congenital
: Disease of extrahepatic biliary tract. : Jumana Abu Hamour : 6/12/2015. : Dr. Samir Bashir. 1 P a g e
 21 : Disease of extrahepatic biliary tract : Jumana Abu Hamour : 6/12/2015 : Dr. Samir Bashir 1 P a g e *Check last page please before you start. Cholelithiasis: -Small, round stones in the gallbladder.
21 : Disease of extrahepatic biliary tract : Jumana Abu Hamour : 6/12/2015 : Dr. Samir Bashir 1 P a g e *Check last page please before you start. Cholelithiasis: -Small, round stones in the gallbladder.
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Diseases of pancreas - Chronic pancreatitis
 Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Biliary Tract Disease. Emmet Andrews Cork University Hospital 6 th September 2010
 Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Disorders of the Liver and Pancreas
 Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract. Shannon Martinson, April 2016
 Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, April 2016 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary Injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, April 2016 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary Injury and responses
Biliary MRI w Eovist
 Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Histology. The pathology of the. bile ducts. pancreas. liver. The lecture in summary. Vt-2006
 Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Digestive system L 4. Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section
 Digestive system L 4 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the structure of liver. 2-Define liver lobule, and identify its zones. 3-Define portal
Digestive system L 4 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the structure of liver. 2-Define liver lobule, and identify its zones. 3-Define portal
CLASSIFICATION OF CHRONIC PANCREATITIS
 CLASSIFICATION OF CHRONIC PANCREATITIS EAGE, Podstgraduate Course, Prague, April 2010. Tomica Milosavljević School of Medicine, University of Belgrade Clinical Center of Serbia,Belgrade The phrase chronic
CLASSIFICATION OF CHRONIC PANCREATITIS EAGE, Podstgraduate Course, Prague, April 2010. Tomica Milosavljević School of Medicine, University of Belgrade Clinical Center of Serbia,Belgrade The phrase chronic
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
The pathology of pancreas
 5. Practice The pathology of pancreas 2017/2018. 2nd semester MACROSCOPY- MICROSCOPY THE STRUCTURE OF PANCREAS Exocrine: 80-85% Enzymes in the zymogenic granules of acinar cells: trypsin, chymotrypsin,
5. Practice The pathology of pancreas 2017/2018. 2nd semester MACROSCOPY- MICROSCOPY THE STRUCTURE OF PANCREAS Exocrine: 80-85% Enzymes in the zymogenic granules of acinar cells: trypsin, chymotrypsin,
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Disorders of the Liver, Gallbladder and Pancreas
 Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
Disorders of the Liver, Gallbladder and Pancreas Objectives: Disorders of the liver Disorders of the gall bladder Disorders of the pancreas Part 1: Disorders of the Liver 1 Jaundice: is a manifestation
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
Gallbladder & Pancreas Ultrasonography
 복부초음파 : 담낭과췌장 Gallbladder & Pancreas Ultrasonography 김정훈 Department of Radiology 1 Interaction of sound with matter (1) 반사 (Reflection) (2) 굴절 (Refraction) (3) 흡수 (Absorption) (4) 산란 (Scattering) 음향저항
복부초음파 : 담낭과췌장 Gallbladder & Pancreas Ultrasonography 김정훈 Department of Radiology 1 Interaction of sound with matter (1) 반사 (Reflection) (2) 굴절 (Refraction) (3) 흡수 (Absorption) (4) 산란 (Scattering) 음향저항
Chronic Pancreatitis
 Falk Symposium 161 October 12, 2007 Chronic Pancreatitis David C Whitcomb MD PhD Giant Eagle Foundation Professor of Cancer Genetics. Professor of Medicine, Cell biology & Physiology, and Human Genetics
Falk Symposium 161 October 12, 2007 Chronic Pancreatitis David C Whitcomb MD PhD Giant Eagle Foundation Professor of Cancer Genetics. Professor of Medicine, Cell biology & Physiology, and Human Genetics
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract. Shannon Martinson, March 2017
 Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
5. Which component of the duodenal contents entering the stomach causes the most severe changes to gastric mucosa:
 Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
Digestive System Module 6: Accessory Organs in Digestion: The Liver, Pancreas, and Gallbladder
 Connexions module: m49293 1 Digestive System Module 6: Accessory Organs in Digestion: The Liver, Pancreas, and Gallbladder Donna Browne Based on Accessory Organs in Digestion: The Liver, Pancreas, and
Connexions module: m49293 1 Digestive System Module 6: Accessory Organs in Digestion: The Liver, Pancreas, and Gallbladder Donna Browne Based on Accessory Organs in Digestion: The Liver, Pancreas, and
Acute And Chronic Pancreatitis
 Acute And Chronic Pancreatitis Objectives: At the end of this lecture the student will be able to: Recognize the predisposing factors of pancreatitis. Describe the different types of pancreatitis. Understand
Acute And Chronic Pancreatitis Objectives: At the end of this lecture the student will be able to: Recognize the predisposing factors of pancreatitis. Describe the different types of pancreatitis. Understand
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Liver, Pancreas and Gall Bladder Pathology
 Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
Malabsorption: etiology, pathogenesis and evaluation
 Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Pediatric Pancreatic Lesions
 Pediatric Pancreatic Lesions Pediatric Surgery Grand Rounds 9 October 2013 Tim Weatherall, PGY2 The University of Tennessee Health Science Center Memphis, TN Disclosures No financial interests to disclose
Pediatric Pancreatic Lesions Pediatric Surgery Grand Rounds 9 October 2013 Tim Weatherall, PGY2 The University of Tennessee Health Science Center Memphis, TN Disclosures No financial interests to disclose
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Cystic Biliary Atresia: Why Is It Important to Distinguish this from Congenital Choledochal Cyst?
 Bahrain Medical Bulletin, Vol. 36, No. 2, June 2014 Cystic Biliary Atresia: Why Is It Important to Distinguish this from Congenital Choledochal Cyst? Hussein Ahmed Mohammed Hamdy, MRCSEd, FEBPS* Hind Mustafa
Bahrain Medical Bulletin, Vol. 36, No. 2, June 2014 Cystic Biliary Atresia: Why Is It Important to Distinguish this from Congenital Choledochal Cyst? Hussein Ahmed Mohammed Hamdy, MRCSEd, FEBPS* Hind Mustafa
Magnetic resonance cholangiopancreatography (MRCP) is an imaging. technique that is able to non-invasively assess bile and pancreatic ducts,
 is an imaging. technique that is able to non-invasively assess bile and pancreatic ducts,") SECRETIN AUGMENTED MRCP Riccardo MANFREDI, MD, MBA, FESGAR Magnetic resonance cholangiopancreatography (MRCP) is an imaging technique that is able to non-invasively assess bile and pancreatic ducts, in
SECRETIN AUGMENTED MRCP Riccardo MANFREDI, MD, MBA, FESGAR Magnetic resonance cholangiopancreatography (MRCP) is an imaging technique that is able to non-invasively assess bile and pancreatic ducts, in
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Biliary Atresia. Karen F. Murray, MD Professor of Pediatrics Director, Hepatobiliary Program Seattle Children s
 Biliary Atresia Karen F. Murray, MD Professor of Pediatrics Director, Hepatobiliary Program Seattle Children s Biliary Atresia Incidence: 1/8,000-15,000 live births Girls > boys 1.5:1 The most common cause
Biliary Atresia Karen F. Murray, MD Professor of Pediatrics Director, Hepatobiliary Program Seattle Children s Biliary Atresia Incidence: 1/8,000-15,000 live births Girls > boys 1.5:1 The most common cause
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
DIGESTIVE. CHAPTER 17 Lecture: Part 1 Part 2 BIO 212: ANATOMY & PHYSIOLOGY II
 BIO 212: ANATOMY & PHYSIOLOGY II CHAPTER 17 Lecture: DIGESTIVE Part 1 Part 2 Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. SMALL INTESTINE DUODENUM > JEJUNUM
BIO 212: ANATOMY & PHYSIOLOGY II CHAPTER 17 Lecture: DIGESTIVE Part 1 Part 2 Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. SMALL INTESTINE DUODENUM > JEJUNUM
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Bile composition. Pathophysiology of Gallstone Formation and Pancreatitis. Bile
 Bile composition Pathophysiology of Gallstone Formation and Pancreatitis Robert F. Schwabe rfs2102@columbia.edu Phospholipids Miscellaneous (Pigment, Protein) (Lecithin) Bile Salts 0.7% 4% H 2 0 1% 12%
Bile composition Pathophysiology of Gallstone Formation and Pancreatitis Robert F. Schwabe rfs2102@columbia.edu Phospholipids Miscellaneous (Pigment, Protein) (Lecithin) Bile Salts 0.7% 4% H 2 0 1% 12%
Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4)
") Vert Phys PCB3743 Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4) T. Houpt, Ph.D. Anatomy of Digestive System Peristalsis Stomach and Acid Secretion Liver and Bile Secretion Pancreas and pancreatic
Vert Phys PCB3743 Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4) T. Houpt, Ph.D. Anatomy of Digestive System Peristalsis Stomach and Acid Secretion Liver and Bile Secretion Pancreas and pancreatic
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Causes of pancreatic insufficiency. Eugen Dumitru
 Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Imaging of common diseases of hepatobiliary and GI system
 Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Imaging of common diseases of hepatobiliary and GI system Natthaporn Tanpowpong, M.D. Diagnostic radiology Faculty of Medicine, Chulalongkorn University Normal plain radiograph A = Common bile duct
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Classification of choledochal cyst with MR cholangiopancreatography in children and infants: special reference to type Ic and type IVa cyst
 Classification of choledochal cyst with MR cholangiopancreatography in children and infants: special reference to type Ic and type IVa cyst Poster No.: C-1333 Congress: ECR 2011 Type: Educational Exhibit
Classification of choledochal cyst with MR cholangiopancreatography in children and infants: special reference to type Ic and type IVa cyst Poster No.: C-1333 Congress: ECR 2011 Type: Educational Exhibit
Slide 154: Pancreas, H&E
 Slide 154: Pancreas, H&E the pancreas, located adjacent to the duodenum, is a mixed exocrine and endocrine gland; it is usually readily identifiable by the presence of the interspersed endocrine pancreatic
Slide 154: Pancreas, H&E the pancreas, located adjacent to the duodenum, is a mixed exocrine and endocrine gland; it is usually readily identifiable by the presence of the interspersed endocrine pancreatic
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications: