Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
|
|
|
- Bruce Morgan
- 5 years ago
- Views:
Transcription
 Positive DPL or sonogram (FAST) Suspect retroperitoneal injury Unknown")
1 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology & Maryland Shock-Trauma University of Maryland School of Medicine Which Blunt Trauma Patients Should Be Studied by Abdominal CT? Hemodynamic stability maintained Unreliable clinical assessment Positive abdominal exam without overt signs (rebound, rigidity) Positive DPL or sonogram (FAST) Suspect retroperitoneal injury Unknown source of blood loss
2 Overview BMI < 0.5% admissions to trauma BMI 3-5% of patients having laparotomy for blunt trauma Clinical signs present < 50% initially DPL variable results for BMI (sensitivity 69%) Sonography - 52% sensitive Non-operative management of solid organ injuries requires high accuracy for BMI Role of CT Is Controversial Role of CT Is Controversial Many literature studies, mainly surgical, cite low sensitivity and high reader dependence (mainly 80 s, early 90s) More recent studies using helical and MDCT indicate consistently higher CT accuracy 75% of respondents to AAST survey use CT most or all of the time for possible BMI Still actively debated (EAST) 13% perforated SB injuries missed by CT # # Fakhry SM, Watts DD, Luchette FA. J Trauma 2003;54:
3 CT of bowel and mesenteric injury 1995 to 2002: 36 cases of BM injury 16 isolated and 20 non-isolated injuries Initial CT scan was abnormal in 74% (17 out of 23), and 83% on retrospect (2 additional cases) CT scans were abnormal (initial and repeat) in 96% (22 out of 23). Free fluid (78%), mesenteric stranding or edema (39%), bowel wall hematoma, or edema (30%). Free air 31%, oral contrast extravasation 15% Sharma et al. The role of computed tomography in diagnosis of blunt intestinal and mesenteric trauma (BIMT). J Emerg Med Jul;27(1): Oral vs. no oral contrast N= 20 patients (500 blunt trauma reviewed) Sensitivity and specificity of CT imaging for the detection of BBMIs were 95.0% and 99.6% CT imaging of the abdomen without oral contrast for detection of BBMIs compares favorably with CT imaging using oral contrast.? Confidence level Allen TL, et al. Computed tomographic scanning without oral contrast solution for blunt bowel and mesenteric injuries in abdominal trauma. J Trauma Feb;56(2):
4 MDCT Technique (16-slice) MDCT Technique (16-slice) 0.75 or 1.5mm X 16mm slice thickness Pitch 1.25 Oral contrast (add rectal for penetrating injury) IV contrast ml (350 mg/ml) Intravenous 6 ml/sec X 15 sec., then 4/sec. X 15 sec. (skull base to pubis) 3-5 mm reconstructions for PACS Use 1mm reconstructed images for reference and MPR, 3D, volumetric studies Diagnostic (operative) CT Signs of Full-thickness Bowel Injury Bowel contrast extravasation Pneumoperitoneum, intramural, intramesenteric air without known or alternative source (20% sensitive) Direct visualization of tear in wall (rare)

5 CT Pneumoperitoneum Consider other sources of air Look for free air beneath anterior abdominal wall, adjacent liver, porta hepatis, between bowel loops More cephalad air in abdomen suggests more cephalad bowel source Look in mesentery, bowel wall, portal vein Use bone or lung settings for search Only about 20% sensitive Distinguish from pneumothorax

6 Pneumoperitoneum: windows & levels for bone or lung Jenunal Perforation Blunt Trauma




7 Was DPL performed? Jejunum: Blunt fullthickness injury





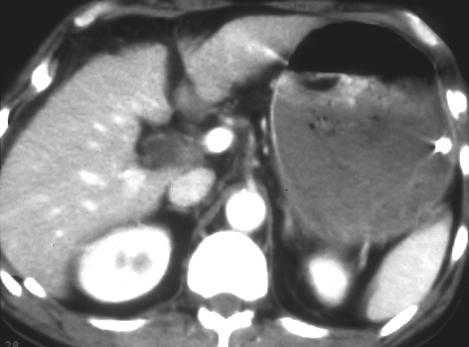
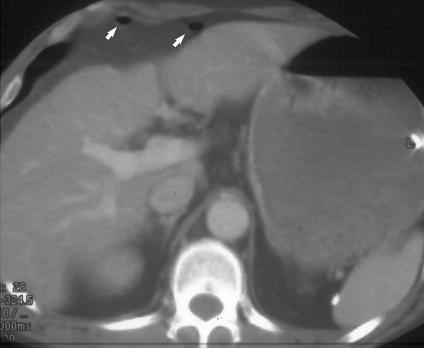
8 Subtle free air: Colon rupture Duodenal rupture



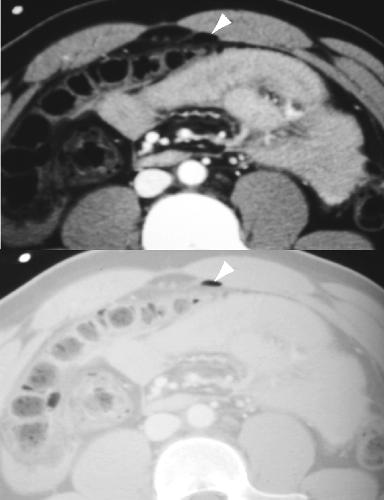
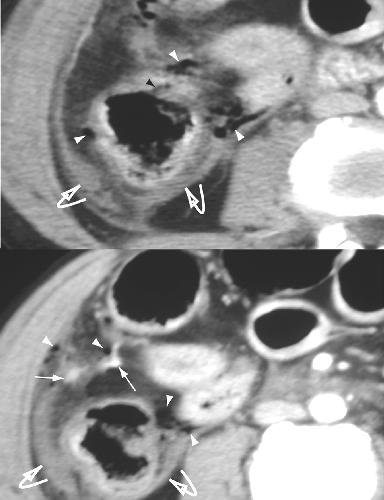
9 Direct rupture of duodenum; free air & hematoma Colon rupture: Intramural air, free air air


10 Intramural duodenal air air delayed duodenal hematoma 4d 4d Oral contrast leak Oral contrast leak Requires oral contrast Spills into low resistance peritoneal space Active bleeding usually dissects into mesentery and has surrounding hematoma Extravasated urine from intraperitoneal bladder rupture can confuse diagnosis (delayed imaging)



11 Oral contrast spillage: OR jejunal perforation Fecal spillage right colon & Lumbar Hernia
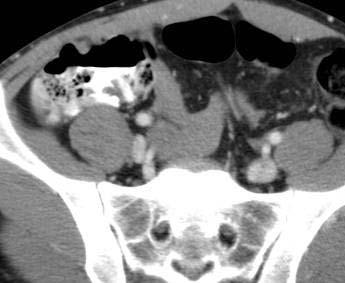
12 Indirect Signs of Bowel Injury: Indirect Signs of Bowel Injury: Bowel wall thickening (subjective) Adjacent mesenteric infiltration or hematoma Dilated, fluid-filled loops - atonic Increased wall contrast enhancement Free fluid of? source Bowel Wall Thickening Normal bowel 1-2 mm partially distended; 3-4 mm when collapsed Seen in proximal small bowel most commonly 5-6 mm mild thickening, 7-8mm moderate, >8 mm marked Contusion localized thickening involving adjacent loops (prox. jejunum) No other findings equals contusion Bowel wall hematoma can co-exist


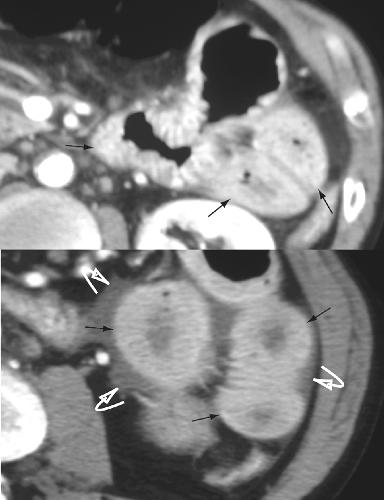
13 Bowel contusion & free fluid: Full-thickness bowel injury

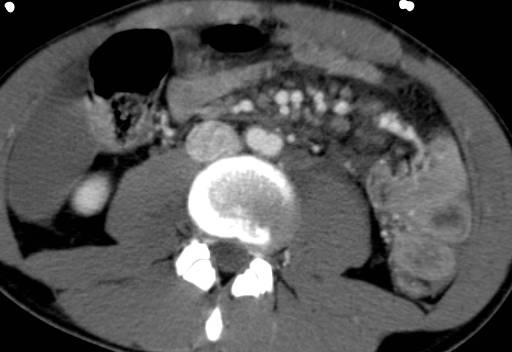

14 Bowel Contusion Jejunal perforation at OR




15 Horse kicks broom into abdomen! Duodenal transection direct diagnosis Delayed colonic hematoma; Pt. on anticoagulants

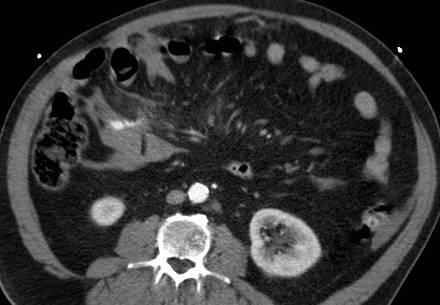
16 Bowel Wall Enhancement Bowel Wall Enhancement Patchy increased density in bowel with thickened wall Often seen with mesenteric edema Mechanism: slowed perfusion, leaky capillaries, re-perfusion phenomenon Mandates careful follow-up Thick-walled enhancing bowel


17 Enhancing small bowel wall Intraperitoneal Fluid Intraperitoneal Fluid Always measure fluid density Trace amount occasionally seen in cul-desac of women of child-bearing years May be the only sign of injury to bowel/mesentery or solid organ (20%+) Larger amounts of fluid in more locations increases chance of injury Mesenteric triangles (bowel mesenteric origin likely)

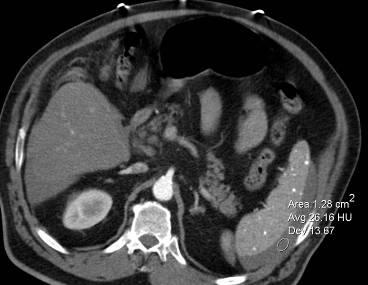
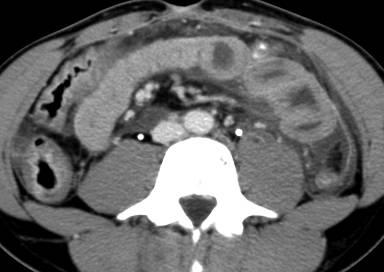
18 Pelvic Fluid: Male CT of Mesenteric Injury CT of Mesenteric Injury Active bleeding Hematoma Infiltration (misty, hazy) Triangle sign of intramesenteric fluid Fascial thickening Difficult to distinguish operative from non-operative lesions


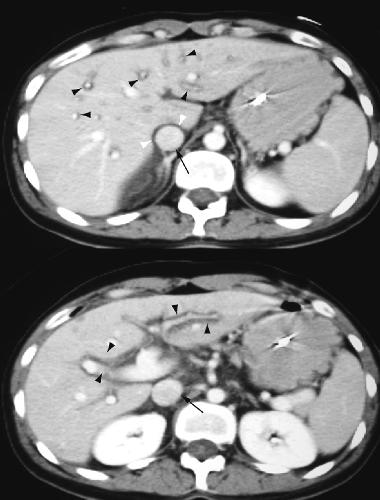
19 Mild mesenteric contusion (misty- hazy) Mesenteric hematoma: renal infarct






20 Colonic contusion with mesenteric tear -hematoma Colonic contusion with mesenteric tear -hematoma Active mesenteric bleeddelayed diffusion



21 Active mesenteric bleed: Sentinel clot Mesenteric hematoma: Sentinel clot clot




22 Active Mesenteric Bleed Delayed Active bleeding mesenteric hematoma; Tear at at root of of mesentery


23 Active mesenteric bleed Enveloping Mesenteric Hematoma


 Diagnostic peritoneal")
24 Intramural gastric hematoma Management for Indirect CT Findings Serial physical examination * F/U CT 6-8 hours Follow-up sonography (same examiner) Diagnostic peritoneal lavage (WBC, bile) Exploration





25 MVC: Abdominal Pain- initial CT Follow-up CT 10 hr. Jejunal rupture in OR

26 Mimics & Masks of Bowel Injury Mimics & Masks of Bowel Injury Shock bowel: follows prolonged hypotension or cardiac arrests Diffuse bowel wall thickening Patchy increased enhancement Dilated, fluid-filled bowel Small bowel mainly involved Mesenteric edema common Usually flat IVC, renal veins May see increased renal and adrenal enhancement, decreased spleen density
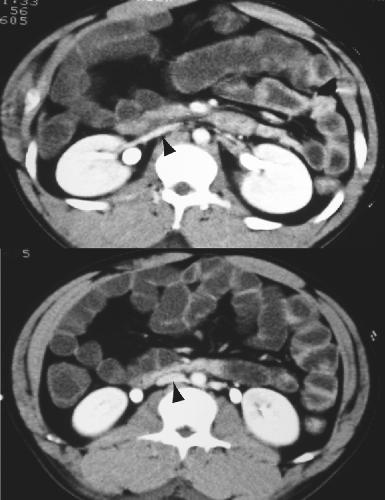
27 Shock Bowel Shock Bowel Shock Bowel Shock Bowel


28 Shock Bowel: Small bowel & colon Shock bowel



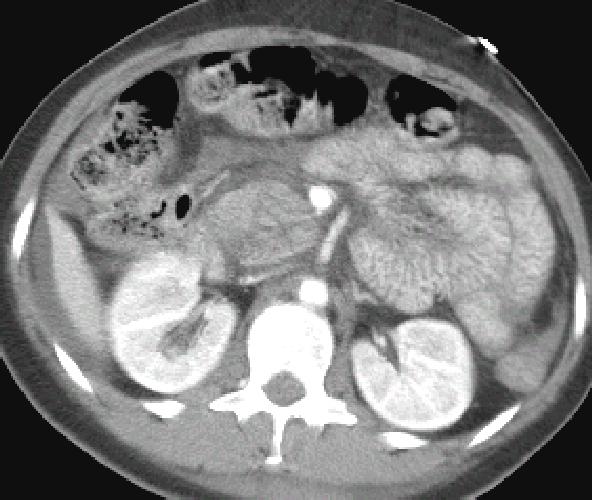
29 Shock Bowel Shock Bowel Mimics & Masks of Bowel Injury Mimics & Masks of Bowel Injury Increased venous return pressure Over resuscitation, cardiac tamponade, tension pneumothorax, hematoma compressing IVC Distended IVC and renal veins Diffuse edematous small bowel and mesentery Often retroperitoneal, pericholecystic edema and peritoneal fluid Rarely involves colon



30 Pericardial Tamponade Increased CVP Periportal lymphedema

31 Increased CVP Small bowel edema Summary What are the CT findings of bowel and mesenteric injury? Which of those findings indicates need for surgical intervention? observation? anxiety? What are the major concurrent trauma findings that mimic or mask signs of bowel and mesenteric injury?

32 Thank You
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Imminent Cardiac Collapse: The Catastrophe You Cannot Afford To Miss
 Imminent Cardiac Collapse: The Catastrophe You Cannot Afford To Miss Presenting Authors Ameya J Baxi, MD (baxi@uthscsa.edu) Carlos Restrepo, MD Disclaimer: We do not have any conflict of interest or financial
Imminent Cardiac Collapse: The Catastrophe You Cannot Afford To Miss Presenting Authors Ameya J Baxi, MD (baxi@uthscsa.edu) Carlos Restrepo, MD Disclaimer: We do not have any conflict of interest or financial
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China
 Review Article Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China Jingshan Gong, Dongdong Mei, Minjie Yang, Jianmin Xu, Yangyang Zhou Department of Radiology,
Review Article Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China Jingshan Gong, Dongdong Mei, Minjie Yang, Jianmin Xu, Yangyang Zhou Department of Radiology,
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Multidetector CT Findings of Bowel Transection in Blunt Abdominal Trauma
 Original rticle Gastrointestinal Imaging http://dx.doi.org/10.3348/kjr.2013.14.4.607 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2013;14(4):607-615 Multidetector CT Findings of owel Transection in
Original rticle Gastrointestinal Imaging http://dx.doi.org/10.3348/kjr.2013.14.4.607 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2013;14(4):607-615 Multidetector CT Findings of owel Transection in
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Advances in Emergency Imaging
 Hampton Symposium,, October 16 th, 2010 Advances in Emergency Imaging Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General Hospital
Hampton Symposium,, October 16 th, 2010 Advances in Emergency Imaging Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General Hospital
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
FAST Focused Assessment with Sonography in Trauma
 FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
Question 1 History. Likely Diagnosis Differential. Further Investigation or Management. Requires Paediatric Surgical referral for laparotomy
 Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
The Questionable Utility of Oral Contrast for the Patient with Abdominal Pain in the Emergency Department
 The Questionable Utility of Oral Contrast for the Patient with Abdominal Pain in the Emergency Department Jonathan Rakofsky, MD PGY3 Henry Ford Hospital Emergency Medicine Program December 2014 All patients
The Questionable Utility of Oral Contrast for the Patient with Abdominal Pain in the Emergency Department Jonathan Rakofsky, MD PGY3 Henry Ford Hospital Emergency Medicine Program December 2014 All patients
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Isolated Gallbladder Perforation in Cases of Blunt Trauma Abdomen
 CASE SERIES Isolated Gallbladder Perforation in Cases of Blunt Trauma Abdomen Gupta MK 1, Ahmad K 1, Kumar A 1, Santhalia PK 1, Joshi BR 2, Rauniyar RK 1 1 Department of Radiodiagnosis and Imaging, 2 Department
CASE SERIES Isolated Gallbladder Perforation in Cases of Blunt Trauma Abdomen Gupta MK 1, Ahmad K 1, Kumar A 1, Santhalia PK 1, Joshi BR 2, Rauniyar RK 1 1 Department of Radiodiagnosis and Imaging, 2 Department
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Blunt liver trauma- brief review and computed tomography role
 Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Advanced Imaging Practice CSB068
 Advanced Imaging Practice CSB068 Week 1 Peer Review - Evaluation of work by one or more people of similar competence to the producer - A form of self-regulation about improving quality and upholding standards
Advanced Imaging Practice CSB068 Week 1 Peer Review - Evaluation of work by one or more people of similar competence to the producer - A form of self-regulation about improving quality and upholding standards
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Primary epiploic appendagitis versus omental infarction : The role of MDCT
 Primary epiploic appendagitis versus omental infarction : The role of MDCT e-poster: EE-125 Congress: ESGAR 2010 Type: Educational Exhibit Topic: Diagnostic / Mesentery and Peritoneum Authors: P. Kraniotis,
Primary epiploic appendagitis versus omental infarction : The role of MDCT e-poster: EE-125 Congress: ESGAR 2010 Type: Educational Exhibit Topic: Diagnostic / Mesentery and Peritoneum Authors: P. Kraniotis,
If your patient is stable, perform a complete assessment using inspection, auscultation, percussion, and pal- By Cynthia Blank-Reid, RN, CEN, MSN
 Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
U Lecture Objectives. U Nordic Forum Trauma & Emergency Radiology. Bowel obstruction. U Bowel Obstruction: Etiologies
 Nordic Forum Trauma & Emergency Radiology Lecture Objectives Bowel Obstruction To illustrate the spectrum of acute obstruction of the small and the large bowel To explain how these bowel obstructions may
Nordic Forum Trauma & Emergency Radiology Lecture Objectives Bowel Obstruction To illustrate the spectrum of acute obstruction of the small and the large bowel To explain how these bowel obstructions may
PAPER. Defining the Role of Computed Tomography in Blunt Abdominal Trauma
 Defining the Role of Computed Tomography in Blunt Abdominal Trauma Use in the Hemodynamically Stable Patient With a Depressed Level of Consciousness Jay D. Pal, MD, PhD; Gregory P. Victorino, MD PAPER
Defining the Role of Computed Tomography in Blunt Abdominal Trauma Use in the Hemodynamically Stable Patient With a Depressed Level of Consciousness Jay D. Pal, MD, PhD; Gregory P. Victorino, MD PAPER
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
Role of Focused Assessment with Sonography for Trauma (FAST) and in abdominal trauma: Radiologist s perspective
 and in abdominal trauma: Radiologist s perspective") Original Research Article Role of Focused Assessment with Sonography for Trauma (FAST) and CT scan in abdominal trauma: Radiologist s perspective Nirav Patel 1*, Niket Domadia 2, Konark Sarvaiya 1, Anil
Original Research Article Role of Focused Assessment with Sonography for Trauma (FAST) and CT scan in abdominal trauma: Radiologist s perspective Nirav Patel 1*, Niket Domadia 2, Konark Sarvaiya 1, Anil
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Whole Body CT Protocol Update 2018
 Whole Body CT Protocol Update 2018 10 th Nordic Course in Trauma Radiology Gothenburg, Sweden K.SHANMUGANATHAN M.D. Disclosure of Commercial Interest Neither I nor my immediate family members have a financial
Whole Body CT Protocol Update 2018 10 th Nordic Course in Trauma Radiology Gothenburg, Sweden K.SHANMUGANATHAN M.D. Disclosure of Commercial Interest Neither I nor my immediate family members have a financial
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
APPENDICITIS AND ITS APPEARANCES ON CT
 APPENDICITIS AND ITS APPEARANCES ON CT APPENDICITIS Results from acute inflammation of the appendix. Most common abdominal surgical emergencies. Diagnosis usually clinical based on physical exam and lab
APPENDICITIS AND ITS APPEARANCES ON CT APPENDICITIS Results from acute inflammation of the appendix. Most common abdominal surgical emergencies. Diagnosis usually clinical based on physical exam and lab
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Pitfalls in the CT diagnosis of appendicitis
 The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
Proceedings of the 11th International Congress of the World Equine Veterinary Association
 www.ivis.org Proceedings of the 11th International Congress of the World Equine Veterinary Association 24 27 September 2009 Guarujá, SP, Brazil Next Meeting : Nov. 2-6, 2011 - Hyderabad, India Reprinted
www.ivis.org Proceedings of the 11th International Congress of the World Equine Veterinary Association 24 27 September 2009 Guarujá, SP, Brazil Next Meeting : Nov. 2-6, 2011 - Hyderabad, India Reprinted
Abdominal compartment syndrome: radiological signs
 Abdominal compartment syndrome: radiological signs Poster No.: C-0903 Congress: ECR 2011 Type: Scientific Exhibit Authors: R. Ignarra, C. Acampora, R. MAZZEO, C. muzj, L. Romano ; 1 1 2 2 3 3 1 4 4 napoli/it,
Abdominal compartment syndrome: radiological signs Poster No.: C-0903 Congress: ECR 2011 Type: Scientific Exhibit Authors: R. Ignarra, C. Acampora, R. MAZZEO, C. muzj, L. Romano ; 1 1 2 2 3 3 1 4 4 napoli/it,
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
Radiology. Undergraduate Radiology Sample Questions
 Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
CT - the prime instrument for the critical. Critical Decisions & Critical Bleeds
 Critical Decisions & Critical Bleeds Bertil Leidner, MD Karolinska University Hospital Huddinge Stockholm, Sweden CT - the prime instrument for the critical patient t The critical patient Traumatized In
Critical Decisions & Critical Bleeds Bertil Leidner, MD Karolinska University Hospital Huddinge Stockholm, Sweden CT - the prime instrument for the critical patient t The critical patient Traumatized In
The Flat Cava Sign Revisited: What is its Significance in Patients Without Trauma?
 Recha S. Eisenstat 1 Allen C. Whitford 2 Michael J. Lane 2 Douglas S. Katz 1 Received June 14, 2001; accepted after revision August 2, 2001. The opinions and assertions contained herein are the private
Recha S. Eisenstat 1 Allen C. Whitford 2 Michael J. Lane 2 Douglas S. Katz 1 Received June 14, 2001; accepted after revision August 2, 2001. The opinions and assertions contained herein are the private
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Traumatic Retroperitoneal Injuries: Review of Multidetector CT Findings 1
 Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois
 ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 13:40-14:00
ENTEROCOLITIDES CAN YOU TELL THEM APART ON MDCT? Richard M. Gore, MD North Shore University Medical Center University of Chicago Evanston, Illinois SCBT/MR 2010 San Diego, California March 8, 2010 13:40-14:00
The Sentinel Clot Sign: a Useful CT Finding for the Evaluation of Intraperitoneal Bladder Rupture Following Blunt Trauma
 The Sentinel Clot Sign: a Useful CT Finding for the Evaluation of Following Blunt Trauma Sang Soo Shin, MD 1 Yong Yeon Jeong, MD 1 Tae Woong Chung, MD 1 Woong Yoon, MD 1 Heoung Keun Kang, MD 1 Taek Won
The Sentinel Clot Sign: a Useful CT Finding for the Evaluation of Following Blunt Trauma Sang Soo Shin, MD 1 Yong Yeon Jeong, MD 1 Tae Woong Chung, MD 1 Woong Yoon, MD 1 Heoung Keun Kang, MD 1 Taek Won
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
Point of Care Ultrasound (PoCUS)
") Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
In the name ofgod. Abdomen 3. Dr. Zahiri
 In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
Emergency Ultrasound. Case ECG. Potential diagnoses. An 80-year-old man in shock. ED patient with non traumatic undifferentiated hypotension
 Emergency Ultrasound An 80-year-old man in shock Case 80/M Present with chest pain Found low BP 62/44 at triage Resus. Room Pulse 86 Temp 35.6, SpO2 95% (RA) No history of drug overdose Past health PAF,
Emergency Ultrasound An 80-year-old man in shock Case 80/M Present with chest pain Found low BP 62/44 at triage Resus. Room Pulse 86 Temp 35.6, SpO2 95% (RA) No history of drug overdose Past health PAF,
Kristina M. Nowitzki, M.D., Ph.D. and Hao S. Lo, M.D. University of Massachusetts Medical School, Worcester, MA
 Kristina M. Nowitzki, M.D., Ph.D. and Hao S. Lo, M.D. University of Massachusetts Medical School, Worcester, MA Outline I. Introduction highlighting normal renal enhancement physiology including normal
Kristina M. Nowitzki, M.D., Ph.D. and Hao S. Lo, M.D. University of Massachusetts Medical School, Worcester, MA Outline I. Introduction highlighting normal renal enhancement physiology including normal
MAKING THE GRADE FOR PEDIATRIC TRAUMA THE REVIEW AND IMPLEMENTATION OF COMPUTED TOMOGRAPHIC (CT) GRADING FOR SOLID ABDOMINAL ORGAN INJURY
 GRADING FOR SOLID ABDOMINAL ORGAN INJURY") MAKING THE GRADE FOR PEDIATRIC TRAUMA THE REVIEW AND IMPLEMENTATION OF COMPUTED TOMOGRAPHIC (CT) GRADING FOR SOLID ABDOMINAL ORGAN INJURY AUTHORS & DISCLOSURE OF COMMERCIAL INTEREST: Jennifer Thomas 1
MAKING THE GRADE FOR PEDIATRIC TRAUMA THE REVIEW AND IMPLEMENTATION OF COMPUTED TOMOGRAPHIC (CT) GRADING FOR SOLID ABDOMINAL ORGAN INJURY AUTHORS & DISCLOSURE OF COMMERCIAL INTEREST: Jennifer Thomas 1
Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015
![Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015](/thumbs/83/87309292.jpg "Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015") Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Pitfalls of the Pediatric Chest and Abdomen SPR 2017
 Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Curious case of Misty Mesentery
 Curious case of Misty Mesentery Poster No.: C-1385 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit T. Simelane 1, H. Khosa 2, N. Ramesh 2 ; 1 Dublin/IE, 2 Portlaoise/IE Abdomen, Anatomy,
Curious case of Misty Mesentery Poster No.: C-1385 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit T. Simelane 1, H. Khosa 2, N. Ramesh 2 ; 1 Dublin/IE, 2 Portlaoise/IE Abdomen, Anatomy,