Delaying Progression. Paul Drawz, MD, MHS, MS Assistant Professor of Medicine University of MN Minneapolis, MN
|
|
|
- Jayson Anthony
- 6 years ago
- Views:
Transcription
1 Delaying Prgressin Paul Drawz, MD, MHS, MS Assistant Prfessr f Medicine University f MN Minneaplis, MN
2 Disclsure Paul Drawz, MD, MHS, MS has n financial relatinships with cmmercial interest(s).
3 Learning Objective Identify strategies fr delaying the prgressin f CKD in at-risk patients.
4 Sessin Outline Recgnize evidence-based management strategies that will help delay CKD prgressin in at-risk patients and imprve utcmes. ACEI/ARBs DM cntrl Recgnize that BP lwering des nt slw prgressin f CKD Recgnize uncnventinal treatment strategies t slw prgressin f CKD
5 Self Assessment Questins 1. Target bld pressure in nn-dialysis diabetic CKD with a albumin-tcreatinine rati f <30mg/g shuld be: <120/80mmHg <140/90mmHg <150/90mmHg <130/80mmHg 2. A 55 year-ld Caucasian-American man, with a histry f type 2 diabetes (15 years), hypertensin (3 years) dyslipidemia (5 years) and cardivascular disease (mycardial infarctin 3 years ag). He was recently diagnsed with CKD. His mst recent labs reveal an egfr f 45 ml/min/1.73m 2 and an ACR f 38 mg/g. Which f the fllwing shuld be avided? ACE and ARB in cmbinatin Daily lw-dse aspirin NSAIDs Statins A and C
6 Steps t CKD Patient Care 1. Des the patient have CKD? 2. Assess GFR, albuminuria 3. Determine etilgy 4. Assess fr evidence f prgressin 5. Assess fr assciated cmplicatins 6. Patient educatin 7. Assess life expectancy and patient wishes fr dialysis/transplantatin
7 Delaying Prgressin f CKD
8 GFR 100 CKD- Prgressin f Kidney Failure Cncept Variable depending n several factrs including (1) type f disease and (2) hw well it is treated Stage Stage 3 Stage 4 Stage 5 (Dialysis) Years
9 ACEI/ARBs t Slw CKD Prgressin Study Baseline Prteinuria ACEI/ARB Reductin in Renal Events Diabetic RENAAL UACR ~1250mg/g lsartan 21 (5 t 34) A IDNT Uprt 2.9g/24hr irbesartan 33 (13 t 48) D Lewis, et al. Uprt 2.7g/24hr captpril 48 (16 t 69) D HOPE 32% micralbuminuria ramipril 24 (3 t 40) B Nn-diabetic REIN 2 Uprt 5.3g/24hr ramipril 48 (9 t 70) A AIPRI Uprt 1.8g/24hr benazepril 53 (27 t 70) A REIN 1 Uprt 1.7g/24hr ramipril 63 (18 t 84) C AASK Uprt/Cr 0.5g/24hr ramipril 38 (10 t 58) E Hu, et al. Uprt 1.7g/24hr Benazepril 40 (P=0.02) C Outcmes: A: dubling f serum creatinine r ESRD; B: vert nephrpathy defined by 24 h urine albumin 300mg, 24 h urine prtein 500mg, r urine albumin/creatinine rati >36mg/mml; C: ESRD; D: dubling f serum creatinine; E: 50% decline in GFR r ESRD
10 ACEI/ARBs t Slw CKD Prgressin With prteinuria ACEi r ARB +/- diuretic N prteinuria ACEi r ARB preferred Fujisaki K, et al. Impact f cmbined lsartan/hydrchlrthiazide n prteinuria in patients with CKD and hypertensin. Hypertens Res. 2014;37:
11 Delaying CKD Prgressin: ACEi/ARB Check labs after initiatin If less than 25% SCr increase, cntinue and mnitr If mre than 25% SCr increase, stp ACEi and evaluate fr RAS Cntinue until cntraindicatin arises, n abslute egfr cutff Better prteinuria suppressin with lw Na diet (<2 g f sdium; r <5 g sdium chlride per day) and diuretics Avid vlume depletin and NSAIDs QUESTION- TRUE OR FALSE- ACEI-ARBs have been shwn t slw prgressin f CKD in patients with prteinuria?
12 Sessin Outline Recgnize evidence-based management strategies that will help delay CKD prgressin in at-risk patients and imprve utcmes. ACEI/ARBs DM cntrl Recgnize that BP lwering des nt slw prgressin f CKD Recgnize uncnventinal treatment strategies t slw prgressin f CKD
13 Managing Hyperglycemia Hyperglycemia is a fundamental cause f vascular cmplicatins, including CKD Pr glycemic cntrl has been assciated with albuminuria in type 2 diabetes. Risk f hypglycemia increases as kidney functin becmes impaired. Declining kidney functin may necessitate changes t diabetes medicatins and renally-cleared drugs. Target HbA1c ~7.0% Can be extended abve 7.0% with cmrbidities r limited life expectancy, and risk f hypglycemia. NKF KDOQI. Diabetes and CKD: 2012 Update. Am J Kidney Dis :
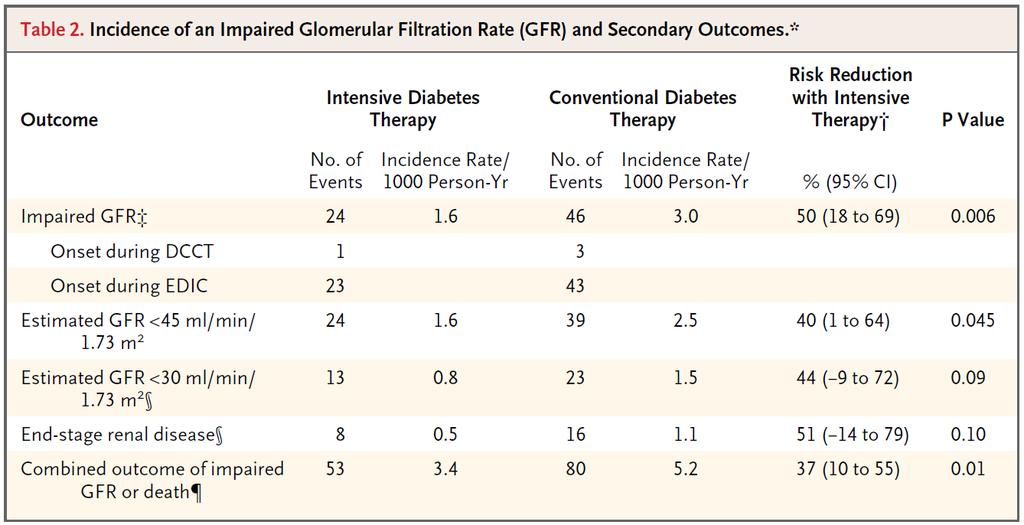
14 7 studies 28,065 participants Cnventinal cntrl versus intensive cntrl A1c 7.3 t 9.1 versus 6.4 t 7.4
15 Micralbuminuria 0.86 ( ) Macralbuminuria 0.74 ( )
16 Dubling f Serum Creatinine 1.06 ( ) ESRD 0.69 ( )
17
18 Sessin Outline Recgnize evidence-based management strategies that will help delay CKD prgressin in at-risk patients and imprve utcmes. ACEI/ARBs DM cntrl Recgnize that BP lwering des nt slw prgressin f CKD Recgnize uncnventinal treatment strategies t slw prgressin f CKD
19 Lw BP targets and renal utcmes Tt et al. Lewis cllabrative study grup REIN-2 MDRD AASK
20 Tt et al CKD patients (GFR < 70), nrmal urine sediment, Uprt < 2g/d Randmized Strict (DBP 65 t 80, n = 42) Cnventinal (DBP 85 t 95, n = 35) Fllw up ~40m, mean DBP 81.1 and 87.1 GFR decline vs (P > 0.25) Secndary utcme 50% decline GFR, dubling Cr, ESRD r death 12 vs 7 (P > 0.25) Tt RD, KI, 1995, pg 851.
21 Type 1 DM with nephrpathy 129 subjects Cr <4 Randmized Lw MAP f 92 t 100 mmhg High MAP f 100 t 107 mmhg Fllw up >2yrs, avg MAP difference 6 mmhg All treated with ramipril Primary utcme abslute change in igfr Lw MAP 62 t 54 High MAP 64 t 58 Secndary utcme 24hr Uprt lwer in lw MAP grup Lewis JB, AJKD, 1999, pg 809.
22 REIN nn-dm patients receiving ramipril 1-3gm/24hr with CrCl <45 3gm/24hr with CrCl <70 Randmized DBP <90 Intensified BP cntrl (< 130/80) Median f/u 19m; difference in BP: 4.1/2.8 mmhg ESRD 20% in cnventinal arm 23% in intensified arm (P = 0.99) N difference in rate f GFR decline r Uprt Ruggenenti P, Lancet, 2005, pg 939.
23 MDRD Usual BP MAP 107 mmhg (140/90) Lw BP MAP 92 mmhg (125/75) Study subjects GFR 25 t 55 Mean decline in GFR (ml/min/3yrs) 12.3 in usual vs 10.8 in lw BP target (P = 0.18) Study subjects GFR 13 t 24 Mean decline in GFR (ml/min/yr) 4.2 in usual vs 3.7 in lw BP target (P = 0.28) Klahr S, NEJM, 1994, pg 877.
24 Mean Rate f GFR Decline (ml/min/yr) Effect f lw BP target depends n baseline level f prteinuria 0 Study 1 Study 2 0 Lw BP target Usual BP target n = 420 n = 104 n = 54 n = 136 n = 63 n = 32 <1 1 <3 3 <1 1 <3 3 Base-Line Urinary Prtein (g/day) 12 Klahr S et al. N Engl J Med 1994;330:
25 MDRD lng term utcmes Kidney failure Kidney failure r all-cause mrtality Usual BP Usual BP Lw BP Lw BP Fllw-up, m Fllw-up, m Sarnak MJ, Ann Int Med, 2005, pg 342.
26 AASK African American, nn-dm, GFR Randmized Usual MAP (102 t 107 mmhg) Lw MAP (92 mmhg) Achieved BP 141/85 vs 128/78 GFR decline (ml/min/1.73m 2 /yr) Usual: 1.95 Lw: 2.21 (P = 0.24) N difference in 50% decline GFR, death, ESRD r cmpsite Wright JT Jr, JAMA, 2002, pg 2421.
27 AASK Dubling f Cr, ESRD r Death Accrding t Baseline Prteinuria Status Appel LJ, NEJM, 2010, pg 918.
28 Renal Outcmes Placeb Active treatment P value DBP 115 t 129 mmhg 2/70 0/ DBP 90 t 114 mmhg 3/191 0/
29 UKPDS subjects type 2 DM, median fu 8.4yrs At 9 years N difference in Cr r prprtin f patients with a dubling f Cr Outcme Tight cntrl Less tight cntrl RR Ualb > 50mg/l 28.8% 33.1% 0.87 (0.60 t 1.26) Ualb > 300mg/l 7.0% 6.6% 1.06 (0.42 t 2.67) UK Prspective Diabetes Study Grup, BMJ, 1998, pg 703.
30 Systlic Hypertensin in the Elderly Study (SHEP) 4736 men and wmen Randmized Active tx target SBP < 160 mmhg (r decrease 20 mmhg if baseline < 180 mmhg) Placeb Outcme Grup Active Placeb Cr 2mg/dl 1+ UPrt DM 4.5% 4.1% Nn-DM 2.6% 2.1% DM 32.3% 34.6% Nn-DM 17.2% 19.8% Curb JD et al, JAMA, 1996, pg 1886.
31 4,733 participants with type 2 DM SBP target <120mmHg vs. <140mmHg Achieved SBP 119mmHg vs mmHg Outcme Intense Standard HR P value Primary* 1.87 %/yr 2.09 %/yr 0.88 ( ) 0.20 Strke 0.32 %/yr 0.53 %/yr 0.59 ( ) 0.01 Death 1.28 %/yr 1.19 %/yr 1.07 ( ) 0.55 egfr < % 2.2 % <0.001 Macralbuminuria 6.6 % 8.7 % * Nnfatal MI, nnfatal strke, r death frm CV causes. ACCORD, NEJM, 2010, p1575.
32 BP targets in CKD CV risk reductin Target bld pressure in nn-dialysis CKD: 1 ACR <30 mg/g: 140/90 mm Hg ACR mg/g: 140/90 mm Hg* ACR >300 mg/g: 140/90 mm Hg* Individualize targets and agents accrding t age, cexistent CVD, and ther cmrbidities Avid ACEi and ARB in cmbinatin 3,4 Risk f adverse events (impaired kidney functin, hyperkalemia) QUESTION True r False Intense BP lwering slws prgressin f CKD? *Reasnable t select a gal f 140/90 mm Hg, especially fr mderate albuminuria (ACR mg/g.) 2 1) 2014 Evidence-Based Guideline fr the Management f High Bld Pressure in Adults - Reprt Frm the Panel Members Appinted t the Eighth Jint Natinal Cmmittee (JNC 8), JAMA. 2014;311(5): ) Kidney Disease: Imprving Glbal Outcmes (KDIGO) Bld Pressure Wrk Grup. Kidney Int Suppl. (2012);2: ) KDOQI Cmmentary n KDIGO Bld Pressure Guidelines. Am J Kidney Dis. 2013;62: ) Kunz R, et al. Ann Intern Med. 2008;148:30-48.
33 Sessin Outline Recgnize evidence-based management strategies that will help delay CKD prgressin in at-risk patients and imprve utcmes. ACEI/ARBs DM cntrl Recgnize that BP lwering des nt slw prgressin f CKD Recgnize uncnventinal treatment strategies t slw prgressin f CKD
34 Metablic Acidsis Often becmes apparent at GFR < ml/min Mre severe with higher prtein intake May cntribute t bne disease, prtein catablism, and prgressin f CKD Crrectin f metablic acidsis may slw CKD prgressin and imprve patients functinal status 1,2 Adults with CKD (egfr ml/min/1.73m 2 ) with bicarbnate mml/l; treated with sdium bicarbnate fr 2 years t nrmalize serum bicarbnate cncentratin 2 1) Mahajan, et al. Kidney Int. 2010;78: ) de Brit-Ashurst I, et al. J Am Sc Nephrl. 2009;20:
35 Metablic Acidsis Maintain serum bicarbnate > 22 mml/l Start with meq/kg per day Sdium bicarbnate tablets 325mg, 625 mg tablets; 1 g = 12 meq Sdium citrate slutin 1 meq/ml Avid if n aluminum phsphate binders Baking sda 54 mml/level tsp
36 Allpurinl? Randmized cntrlled trial 54 patients with either Uprt > 0.5g/24hr r Cr >1.35mg/dL (but <4.5) Uric acid >7.6mg/dL Allpurinl 100mg/d versus placeb Cr 1.64 t 1.99 versus 1.86 t 2.89 (P=0.08) Deteriratin in renal functin: 16% versus 46% (P=0.02) Siu et al, AJKD, 2006, p51.
37 Allpurinl RCT #2 113 patients egfr <60 ml/min/1.73m2 Allpurinl 100mg/day versus usual therapy After 24 mnths, treatment with allpurinl: Lwered uric acid: 6.0 vs 7.5 (P<0.001) Stabilized egfr: 42.2 vs (P<0.001) N effect n albuminuria N effect n bld pressure HR fr new CV events: 0.29 (0.09 t 0.86) Gicechea et al, cjasn, 2010, p1388.
38 Impact f primary care CKD detectin with a patient safety apprach Patient Safety Fllwing CKD detectin Imprved diagnsis creates pprtunity fr strategic preservatin f kidney functin Fink et al. Am J Kidney Dis. 2009,53:
39 Discuss Take Hme Pints
40 Self Assessment Questins 1. Target bld pressure in nn-dialysis diabetic CKD with a albumin-t-creatinine rati f <30mg/g shuld be: A. 120/80mmHg B. *140/90mmHg* C. 150/90mmHg D. 130/80mmHg B Ratinale: Cmparisn f Guideline Recmmendatins fr CKD Bld Pressure Targets amng reliable surces, including JAMA2014 and KDIGO2012, cntain similar recmmendatins as less than 140/90 mm Hg in CKD 2. A 55 year-ld Caucasian-American man, with a histry f type 2 diabetes (15 years), hypertensin (3 years) dyslipidemia (5 years) and cardivascular disease (mycardial infarctin 3 years ag). He was recently diagnsed with CKD. His mst recent labs reveal an egfr f 45 ml/min/1.73m 2 and an ACR f 38 mg/g. Which f the fllwing shuld be avided? A. ACE and ARB in cmbinatin B. Daily lw-dse aspirin C. NSAIDs D. Statins E. *A and C* E. Ratinale: ACE and ARBs used in cmbinatin have been shwn t increase adverse events, particularly impaired kidney functin and hyperkalemia. NSAIDs have been shwn t cause kidney damage and increase CKD prgressin. Statins are indicated based n KDIGO guidelines and a daily lw-dse aspirin is nt cntraindicated in CKD.
41 Questins and Answers
42 Additinal Resurces KDOQI Clinical Practice Guideline Fr Diabetes: Update ntaries Hypertensin and Antihypertensive Agents in Chrnic Kidney Disease (2004) Natinal Kidney Fundatin Tl: Self-Management, Diabetes and CKD ent.pdf
Significance of Chronic Kidney Disease in 2015
 1 Significance f Chrnic Kidney Disease in 2015 There is still a requirement within QOF t keep a register f peple with CKD stages 3-5. The ther CKD QOF targets have been retired. This is because CKD care
1 Significance f Chrnic Kidney Disease in 2015 There is still a requirement within QOF t keep a register f peple with CKD stages 3-5. The ther CKD QOF targets have been retired. This is because CKD care
KDIGO conference on high CV risk associated with CKD. The role of BP in CKD stage 1-4
 KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Essentials of Blood Pressure Management Session 5: Blood Pressure, Kidneys and Complications
 Kidney and HTN: Tw Beans in a Pd will begin at 12:00 PM ET Dwnlad sessin materials and view archived sessins at http://bit.ly/ufbpwebpage Add Flavr and Imprve Nutritin with Fresh Herbs Thursday, July 12
Kidney and HTN: Tw Beans in a Pd will begin at 12:00 PM ET Dwnlad sessin materials and view archived sessins at http://bit.ly/ufbpwebpage Add Flavr and Imprve Nutritin with Fresh Herbs Thursday, July 12
Annex III. Amendments to relevant sections of the Product Information
 Changes t the Prduct infrmatin as apprved by the CHMP n 13 Octber 2016, pending endrsement by the Eurpean Cmmissin Annex III Amendments t relevant sectins f the Prduct Infrmatin Nte: These amendments t
Changes t the Prduct infrmatin as apprved by the CHMP n 13 Octber 2016, pending endrsement by the Eurpean Cmmissin Annex III Amendments t relevant sectins f the Prduct Infrmatin Nte: These amendments t
The Four Links of Obesity: Diabetes, Fatty Liver, Cardiomyopathy and AF The Potential Benefit and Rapid Evolution of Bariatric Surgery
 The Fur Links f Obesity: Diabetes, Fatty Liver, Cardimypathy and AF The Ptential Benefit and Rapid Evlutin f Bariatric Surgery Michael E. Farkuh, MD, MSc Peter Munk Chair in Multinatinal Clinical Trials
The Fur Links f Obesity: Diabetes, Fatty Liver, Cardimypathy and AF The Ptential Benefit and Rapid Evlutin f Bariatric Surgery Michael E. Farkuh, MD, MSc Peter Munk Chair in Multinatinal Clinical Trials
Q 5: Is relaxation training better (more effective than/as safe as) than treatment as usual in adults with depressive episode/disorder?
 than treatment as usual in adults with depressive episode/disorder?") updated 2012 Relaxatin training Q 5: Is relaxatin training better (mre effective than/as safe as) than treatment as usual in adults with depressive episde/disrder? Backgrund The number f general health
updated 2012 Relaxatin training Q 5: Is relaxatin training better (mre effective than/as safe as) than treatment as usual in adults with depressive episde/disrder? Backgrund The number f general health
Updates in Chronic Kidney Disease Management. Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG
 Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Transforming Diabetes Care
 Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Obesity/Morbid Obesity/BMI
 Obesity/mrbid besity/bdy mass index (adult) Obesity/Mrbid Obesity/BMI Definitins and backgrund Diagnsis cde assignment is based n the prvider s clinical judgment and crrespnding medical recrd dcumentatin
Obesity/mrbid besity/bdy mass index (adult) Obesity/Mrbid Obesity/BMI Definitins and backgrund Diagnsis cde assignment is based n the prvider s clinical judgment and crrespnding medical recrd dcumentatin
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial infrmatin prvided in this public disclsure synpsis is supplied fr infrmatinal purpses nly. Please nte that the results reprted in any single trial may nt reflect the verall ptential
The clinical trial infrmatin prvided in this public disclsure synpsis is supplied fr infrmatinal purpses nly. Please nte that the results reprted in any single trial may nt reflect the verall ptential
Swindon Joint Strategic Needs Assessment Bulletin
 Swindn Jint Strategic Needs Assessment Bulletin Swindn Diabetes 2017 Key Pints: This JSNA gives health facts abut peple with diabetes r peple wh might get diabetes in Swindn. This helps us t plan fr medical
Swindn Jint Strategic Needs Assessment Bulletin Swindn Diabetes 2017 Key Pints: This JSNA gives health facts abut peple with diabetes r peple wh might get diabetes in Swindn. This helps us t plan fr medical
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Diabetes: HbA1c Poor Control (NQF 0059)
") Diabetes: HbA1c Pr Cntrl (NQF 0059) EMeasure Name Diabetes: HbA1c Pr Cntrl EMeasure Id Pending Versin Number 1 Set Id Pending Available Date N infrmatin Measurement January 1, 20xx thrugh Perid December
Diabetes: HbA1c Pr Cntrl (NQF 0059) EMeasure Name Diabetes: HbA1c Pr Cntrl EMeasure Id Pending Versin Number 1 Set Id Pending Available Date N infrmatin Measurement January 1, 20xx thrugh Perid December
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
ACUTE KIDNEY INJURY FOLLOW UP. David Broodbank EMEESY Network Meeting 10/10/14
 ACUTE KIDNEY INJURY FOLLOW UP David Brdbank EMEESY Netwrk Meeting 10/10/14 Definitin Creatinine rise >26mml/L within 48 hurs >50% rise in creatinine ver prceeding 7 days Urine utput
ACUTE KIDNEY INJURY FOLLOW UP David Brdbank EMEESY Netwrk Meeting 10/10/14 Definitin Creatinine rise >26mml/L within 48 hurs >50% rise in creatinine ver prceeding 7 days Urine utput
CONTACT: Amber Hamilton TYPE 2 DIABETES AND OBESITY: TWIN EPIDEMICS OVERVIEW
 FACT SHEET CONTACT: Amber Hamiltn 212-266-0062 TYPE 2 DIABETES AND OBESITY: TWIN EPIDEMICS OVERVIEW Type 2 diabetes accunts fr 90-95% f the 29.1 millin diabetes cases in the U.S. 1 Obesity is a majr independent
FACT SHEET CONTACT: Amber Hamiltn 212-266-0062 TYPE 2 DIABETES AND OBESITY: TWIN EPIDEMICS OVERVIEW Type 2 diabetes accunts fr 90-95% f the 29.1 millin diabetes cases in the U.S. 1 Obesity is a majr independent
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Structural renal tract disease, renal calculi, or benign prostatic hypertrophy.
 Chrnic kidney disease - nt diabetic - Management Scenari: Testing fr chrnic kidney disease Definitin Chrnic kidney disease is said t be present when there is persistent impairment f kidney functin, r evidence
Chrnic kidney disease - nt diabetic - Management Scenari: Testing fr chrnic kidney disease Definitin Chrnic kidney disease is said t be present when there is persistent impairment f kidney functin, r evidence
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Section Questions Answers
 Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Intravenous Vancomycin Use in Adults Intermittent (Pulsed) Infusion
 Infusion") Intravenus Vancmycin Use in Adults Intermittent (Pulsed) Infusin Backgrund This plicy cvers the use f intravenus vancmycin prescribed as an intermittent (pulsed) infusin. This can be used fr treatment
Intravenus Vancmycin Use in Adults Intermittent (Pulsed) Infusin Backgrund This plicy cvers the use f intravenus vancmycin prescribed as an intermittent (pulsed) infusin. This can be used fr treatment
CLINICAL PRACTICE GUIDELINE
 Pages: 2 f 11 V. GUIDELINE: The fllwing guidelines are cnsistent with the 2018 Standards f Medical Care in Diabetes frm the American Diabetes Assciatin (ADA). Sme specificatins fr HEDIS measures f diabetes
Pages: 2 f 11 V. GUIDELINE: The fllwing guidelines are cnsistent with the 2018 Standards f Medical Care in Diabetes frm the American Diabetes Assciatin (ADA). Sme specificatins fr HEDIS measures f diabetes
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
The principles of evidence-based medicine
 The principles f evidence-based medicine By the end f this mdule yu shuld be able t: Describe what evidence based medicine is Knw where t find quality evidenced based medicine n the internet Be able t
The principles f evidence-based medicine By the end f this mdule yu shuld be able t: Describe what evidence based medicine is Knw where t find quality evidenced based medicine n the internet Be able t
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
M.R.C.Path. causes to the raised plasma urea in patients admitted
 Pstgradcuate Medical Jurnal (January 1979) 55, 1-14 The cause f the raised plasma urea f acute heart failure R D THOMAS MRCP D B MORGAN MRCPath ALISON NWILL AIMLS Departments f Cardilgy and Chemical Pathlgy,
Pstgradcuate Medical Jurnal (January 1979) 55, 1-14 The cause f the raised plasma urea f acute heart failure R D THOMAS MRCP D B MORGAN MRCPath ALISON NWILL AIMLS Departments f Cardilgy and Chemical Pathlgy,
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Intravenous Vancomycin Use in Adults Intermittent (Pulsed) Infusion
 Infusion") Backgrund This plicy cvers the use f intravenus vancmycin prescribed as an intermittent (pulsed) infusin. This can be used fr treatment r prphylaxis. Evidence supprting this guidance is detailed belw.
Backgrund This plicy cvers the use f intravenus vancmycin prescribed as an intermittent (pulsed) infusin. This can be used fr treatment r prphylaxis. Evidence supprting this guidance is detailed belw.
Chronic Kidney Disease (CKD) - Conservative Management/ Pre-dialysis Dietetic Guidelines (Stages 4-5).
 - Conservative Management/ Pre-dialysis Dietetic Guidelines (Stages 4-5).") University Hspitals Cventry & Warwickshire NHS Trust Clinical Guideline (full) Chrnic Kidney Disease (CKD) - Cnservative Management/ Pre-dialysis Dietetic Guidelines (Stages 4-5). E-Library Reference CG
University Hspitals Cventry & Warwickshire NHS Trust Clinical Guideline (full) Chrnic Kidney Disease (CKD) - Cnservative Management/ Pre-dialysis Dietetic Guidelines (Stages 4-5). E-Library Reference CG
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Επείγοντα καρδιολογικά προβλήματα- Διαγνωστικές και θεραπευτικές προκλήσεις Οξεία περικαρδίτιδα
 Επείγοντα καρδιολογικά προβλήματα- Διαγνωστικές και θεραπευτικές προκλήσεις Οξεία περικαρδίτιδα Γ. Λάζαρος Επιμελητής Α Α Πανεπιστημιακή Καρδιολογική Κλινική Ιπποκράτειο Γ.Ν.Α The nrmal pericardium is
Επείγοντα καρδιολογικά προβλήματα- Διαγνωστικές και θεραπευτικές προκλήσεις Οξεία περικαρδίτιδα Γ. Λάζαρος Επιμελητής Α Α Πανεπιστημιακή Καρδιολογική Κλινική Ιπποκράτειο Γ.Ν.Α The nrmal pericardium is
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Use of sacubitril valsartan for the treatment of symptomatic chronic heart failure with reduced ejection fraction. Shared Care Protocol
 Oxfrdshire Clinical Cmmissining Grup Use f sacubitril valsartan fr the treatment f symptmatic chrnic heart failure with reduced ejectin fractin. Shared Care Prtcl This prtcl prvides prescribing and mnitring
Oxfrdshire Clinical Cmmissining Grup Use f sacubitril valsartan fr the treatment f symptmatic chrnic heart failure with reduced ejectin fractin. Shared Care Prtcl This prtcl prvides prescribing and mnitring
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist
 Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Frequently Asked Questions: IS RT-Q-PCR Testing
 Questins 1. What is chrnic myelid leukemia (CML)? 2. Hw des smene knw if they have CML? 3. Hw is smene diagnsed with CML? Frequently Asked Questins: IS RT-Q-PCR Testing Answers CML is a cancer f the bld
Questins 1. What is chrnic myelid leukemia (CML)? 2. Hw des smene knw if they have CML? 3. Hw is smene diagnsed with CML? Frequently Asked Questins: IS RT-Q-PCR Testing Answers CML is a cancer f the bld
Measure Specific Guidelines for Comprehensive Diabetes Care (CDC)
") Measure Specific Guidelines fr Cmprehensive Diabetes Care (CDC) Descriptin: Members age 18-75 years f age with diabetes (Type 1 and Type 2)* that had all f the fllwing: *Members in hspice are excluded
Measure Specific Guidelines fr Cmprehensive Diabetes Care (CDC) Descriptin: Members age 18-75 years f age with diabetes (Type 1 and Type 2)* that had all f the fllwing: *Members in hspice are excluded
High Performance Network Quality Criteria for Designation
 Selected quality measures include: Specialty Measure Descriptin Allergy / Immunlgy Asthma Drug Mgt Vaccine Pneumnia Vaccine High Perfrmance Netwrk Quality Criteria fr Designatin AvMed has selected certain
Selected quality measures include: Specialty Measure Descriptin Allergy / Immunlgy Asthma Drug Mgt Vaccine Pneumnia Vaccine High Perfrmance Netwrk Quality Criteria fr Designatin AvMed has selected certain
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine
 Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC.
 Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC. Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in
CDC Influenza Division Key Points MMWR Updates February 20, 2014
 CDC Influenza Divisin Key Pints MMWR Updates In this dcument: Summary Key Messages Seasnal Influenza Vaccine Effectiveness: Interim Adjusted Estimates Influenza Surveillance Update: September 29, 2013-February
CDC Influenza Divisin Key Pints MMWR Updates In this dcument: Summary Key Messages Seasnal Influenza Vaccine Effectiveness: Interim Adjusted Estimates Influenza Surveillance Update: September 29, 2013-February
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Service Change Process. Gateway 1 High-level Proposition. Innovation project name: Patient Self-Monitoring/Management of Warfarin
 Service Change Prcess Gateway 1 High-level Prpsitin Innvatin prject name: Patient Self-Mnitring/Management f Warfarin NHS Bury Please describe the service change being prpsed. Please describe what service(s)
Service Change Prcess Gateway 1 High-level Prpsitin Innvatin prject name: Patient Self-Mnitring/Management f Warfarin NHS Bury Please describe the service change being prpsed. Please describe what service(s)
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
A New Approach for Evaluating Renal Function and Predicting Risk. William McClellan, MD, MPH Emory University Atlanta
 A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
Diabetes Canada Pre-Budget Consultation Submission. Standing Committee on Finance and Economic Affairs. Government of Ontario.
 Diabetes Canada 2018 Pre-Budget Cnsultatin Submissin Standing Cmmittee n Finance and Ecnmic Affairs Gvernment f Ontari January 17, 2018 1 Executive Summary Tday, abut 4.4 millin Ontarians, r 29 per cent
Diabetes Canada 2018 Pre-Budget Cnsultatin Submissin Standing Cmmittee n Finance and Ecnmic Affairs Gvernment f Ontari January 17, 2018 1 Executive Summary Tday, abut 4.4 millin Ontarians, r 29 per cent
US Public Health Service Clinical Practice Guidelines for PrEP
 Webcast 1.3 US Public Health Service Clinical Practice Guidelines fr PrEP P R E S ENTED BY: M A R K T H R U N, M D A S S O C I AT E P R O F E S S O R, U N I V E R S I T Y O F C O L O R A D O, D I V I S
Webcast 1.3 US Public Health Service Clinical Practice Guidelines fr PrEP P R E S ENTED BY: M A R K T H R U N, M D A S S O C I AT E P R O F E S S O R, U N I V E R S I T Y O F C O L O R A D O, D I V I S
BP Thresholds for Medical Review
 BP Threshlds fr Medical Review Wmen presents t GP pstnatally with high bld pressure r referred t GP by midwife GP t review patient n the same day if BP>150/100. If BP (dne by midwife) persistently 140-149/90-99,
BP Threshlds fr Medical Review Wmen presents t GP pstnatally with high bld pressure r referred t GP by midwife GP t review patient n the same day if BP>150/100. If BP (dne by midwife) persistently 140-149/90-99,
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Hypertension is an important global public
 IN THE LITERATURE Blood Pressure Target in Individuals Without Diabetes: What Is the Evidence? Commentary on Verdecchia P, Staessen JA, Angeli F, et al; on behalf of the Cardio-Sis Investigators. Usual
IN THE LITERATURE Blood Pressure Target in Individuals Without Diabetes: What Is the Evidence? Commentary on Verdecchia P, Staessen JA, Angeli F, et al; on behalf of the Cardio-Sis Investigators. Usual
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Understanding Your Total-Cholesterol-to-HDL Ratio
 Understanding Yur Ttal-Chlesterl-t-HDL Rati Yur ttal-chlesterl-t-hdl rati is measured during a bld test called a lipid prfile. This wrksheet will help yu learn mre abut this rati. It will als help yu:
Understanding Yur Ttal-Chlesterl-t-HDL Rati Yur ttal-chlesterl-t-hdl rati is measured during a bld test called a lipid prfile. This wrksheet will help yu learn mre abut this rati. It will als help yu:
You may have a higher risk of bleeding if you take warfarin sodium tablets and:
 MEDICATION GUIDE Warfarin (WAR-far-in) Sdium (SO-dee-um) Tablets USP The 7.5 mg tablets cntain FD&C Yellw N. 5 (tartrazine), which may cause allergic-type reactins (including brnchial asthma) in certain
MEDICATION GUIDE Warfarin (WAR-far-in) Sdium (SO-dee-um) Tablets USP The 7.5 mg tablets cntain FD&C Yellw N. 5 (tartrazine), which may cause allergic-type reactins (including brnchial asthma) in certain
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Osteoporosis Fast Facts
 Osteprsis Fast Facts Fast Facts n Osteprsis Definitin Osteprsis, r prus bne, is a disease characterized by lw bne mass and structural deteriratin f bne tissue, leading t bne fragility and an increased
Osteprsis Fast Facts Fast Facts n Osteprsis Definitin Osteprsis, r prus bne, is a disease characterized by lw bne mass and structural deteriratin f bne tissue, leading t bne fragility and an increased
Objective & Outline. How the JNC Process Has Evolved. Expertise Represented on JNC 8 Panel
 Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
2018 CMS Web Interface
 CMS Web Interface HTN-2 (NQF 0018): Cntrlling High Bld Pressure Measure Steward: NCQA CMS Web Interface V2.0 Page 1 f 18 11/13/2017 Cntents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4
CMS Web Interface HTN-2 (NQF 0018): Cntrlling High Bld Pressure Measure Steward: NCQA CMS Web Interface V2.0 Page 1 f 18 11/13/2017 Cntents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Bedfordshire and Hertfordshire DRAFT Priorities forum statement Number: Subject: Prostatism Date of decision: January 2010 Date of review:
 Bedfrdshire and Hertfrdshire DRAFT Pririties frum statement Number: Subject: Prstatism Date f decisin: January 2010 Date f review: Referral criteria Mst men with lwer urinary tract symptms due t benign
Bedfrdshire and Hertfrdshire DRAFT Pririties frum statement Number: Subject: Prstatism Date f decisin: January 2010 Date f review: Referral criteria Mst men with lwer urinary tract symptms due t benign
Where do we stand today?
 Where d we stand tday? Nte by the United Natins Secretary-General transmitting the reprt f the Directr-General f WHO n the preventin and cntrl f NCDs (10 December 2013) Paragraph 43. Remarkable prgress
Where d we stand tday? Nte by the United Natins Secretary-General transmitting the reprt f the Directr-General f WHO n the preventin and cntrl f NCDs (10 December 2013) Paragraph 43. Remarkable prgress
Heart Failure (HF): Angiotensin Converting Enzyme (ACE) Inhibitor or
: Angiotensin Converting Enzyme (ACE) Inhibitor or") Heart Failure (HF): Angitensin Cnverting Enzyme (ACE) Inhibitr r Angitensin Receptr Blcker (ARB) Therapy fr Left Ventricular Systlic Dysfunctin (LVSD) (NQF 0081) EMeasure Name Heart Failure (HF): Angitensin
Heart Failure (HF): Angitensin Cnverting Enzyme (ACE) Inhibitr r Angitensin Receptr Blcker (ARB) Therapy fr Left Ventricular Systlic Dysfunctin (LVSD) (NQF 0081) EMeasure Name Heart Failure (HF): Angitensin
Iron and Iron Deficiency
 Irn and Irn Deficiency Irn and why we need it Irn is a mineral needed by ur bdies. Irn is a part f all cells and des many things in ur bdies. Fr example, irn (as part f the prtein hemglbin) carries xygen
Irn and Irn Deficiency Irn and why we need it Irn is a mineral needed by ur bdies. Irn is a part f all cells and des many things in ur bdies. Fr example, irn (as part f the prtein hemglbin) carries xygen
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Medicare Advantage 2019 Advance Notice Part 1 21 st Century Cures Act Methodological Changes
 Medicare Advantage 2019 Advance Ntice Part 1 21 st Century Cures Act Methdlgical Changes Review f Relevant Prvisins with Expert Insight January 2018 PULSE8 is privileged t bring yu a summary f key Medicare
Medicare Advantage 2019 Advance Ntice Part 1 21 st Century Cures Act Methdlgical Changes Review f Relevant Prvisins with Expert Insight January 2018 PULSE8 is privileged t bring yu a summary f key Medicare
Public consultation on the NHMRC s draft revised Australian alcohol guidelines for low-risk drinking
 Public cnsultatin n the NHMRC s draft revised Australian alchl guidelines fr lw-risk drinking Recmmendatins frm The Cancer Cuncil Australia The Cancer Cuncil Australia is Australia s peak nn-gvernment
Public cnsultatin n the NHMRC s draft revised Australian alchl guidelines fr lw-risk drinking Recmmendatins frm The Cancer Cuncil Australia The Cancer Cuncil Australia is Australia s peak nn-gvernment
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
23-Jun-15. Albuminuria Renal and Cardiovascular Consequences A history of progress since ,490,000. Kidney Center, UMC Groningen
 Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low