Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC.
|
|
|
- Caitlin Barnett
- 5 years ago
- Views:
Transcription
1 Chronic Kidney Disease DR. SANJAY PANDEYA MD. FRCPC.
2 Objectives Review CKD and its implications for the family physician Review the relevance of CKD and ESRD, its complications and management issues in the patient on dialysis for the family physician
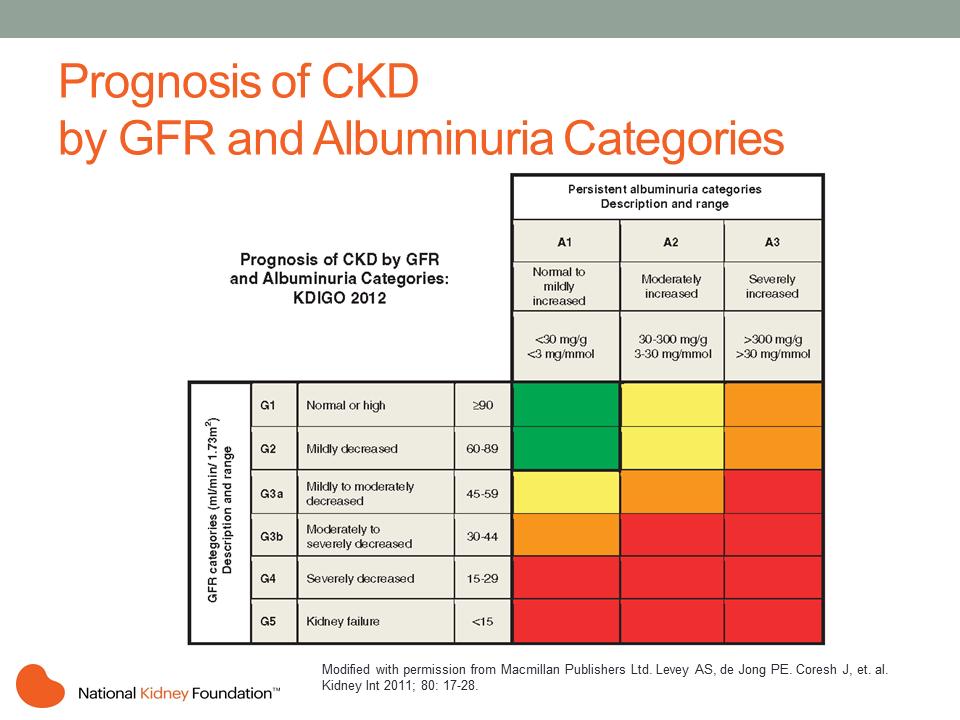
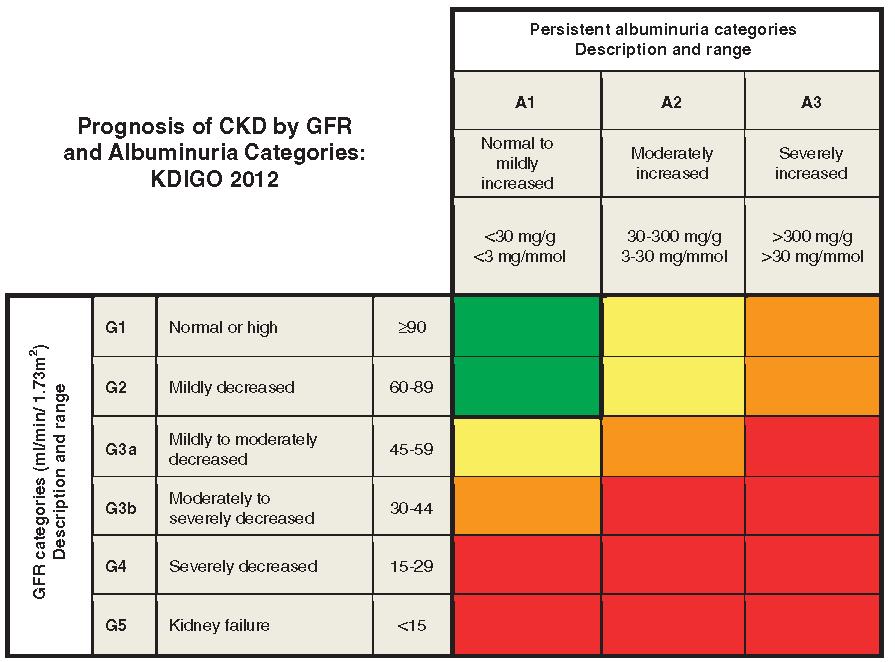
3 CKD Classification Stage Description GFR 1 Kidney Damage with normal or increased GFR >=90 2 Kidney Damage with mild decrease GFR Moderate decrease in GFR Severe decrease in GFR Kidney Failure <15 or RRT
4 Ontario Renal Network
5 Detection Test with egfr and urine ACR If egfr < 60, repeat in 3 months or sooner If urine ACR > 3 mg/mmol, repeat 1-2x over next 3 months Always consider reversible factors
6 Ontario Renal Network
7 Detection Box C: If egfr > 60 and urine ACR < 3 mg/mmol Patient does not have CKD Test annually Box A: If egfr < 30 and/or urine ACR > 60 Patient has CKD For low egfr GFR: CBC, lytes, Ca, Phos, Alb, PTH, urine R+M ACR: Urine R+M, electrolytes Refer to Nephrologist
8 Detection Box B: If egfr and/or urine ACR 3-60 Patient has CKD See Management box (to come) Check urine R+M, lytes Follow egfr, UACR q6 months If egfr stable x 2 years, check annually Refer to Nephrologist egfr < 60 and decline > 5 ml/min within 6 months * egfr < 30 or UACR > 60 egfr <45 and urine ACR BP control K+ disorders, RBC casts or hematuria (>20 RBC/hpf)
9 Ontario Renal Network
10 Manage CV Risk Factors Lifestyle modification, smoking cessation Lipid management for patients with CKD If with diabetes treat with a statin If without diabetes, age 50 treat with a statin If without diabetes, age <50, with risk such as having known coronary artery disease, prior stroke, or 10-year Framingham risk >10% treat with a statin (+/- ezetemibe if egfr<60) see KDIGO guidelines for further details For patients with diabetes, target HbA1c to appropriate level (see CDA guidelines)
11 Manage Minimize further kidney injury If possible, avoid nephrotoxins such as NSAIDs, IV and intra-arterial contrast, etc. (if egfr < 60) If contrast is necessary, consider oral hydration, withholding diuretics Sick Day Medication List (SADMAN) Sulfonylureas ACEI Diuretics Metformin ARB NSAIDS
12 Manage Slow Progression Measures BP and RAAS blockade (repeat creatinine and potassium 2 weeks after initiation of ACEI or ARB use): If with diabetes, target BP < 130/80, otherwise target BP < 140/90 * If with diabetes and with ACR > 3, start use of an ACEI or ARB as first-line therapy. If BP already < 130/80, use ACEI or ARB cautiously, monitoring for signs and symptoms of hypotension If without diabetes, ACR > 30 and BP > 140/90, start use of an ACEI or ARB as first-line therapy
13
14
15 BP CONTROL AND REDUCING PROTEINURIA
16 Recommended Office BP Treatment Targets Treatment consists of health behaviour ± pharmacological management Population SBP DBP High Risk 120 NA Diabetes < 130 < 80 All others* < 140 < 90 * Target BP with AOBP < 135/85 16
17 Cardio-renal continuum:the ultimate treatment goal is to reduce mortality Regress Retard Prevent Macroalbuminuria (>300 mg/d) Worsening nephropathy Reduce Microalbuminuria ( mg/d) Mortality Adapted from Dzau VJ, et al. Circulation. 2006;114;
18 Studies of Primary Prevention of Microalbuminuria (MAU) Regress Retard Prevent Macroalbuminuria Worsening nephropathy Reduce Microalbuminuria ROADMAP (olmesartan) BENEDICT (trandolapril) ADVANCE (perindopril) DIRECT (candesartan) MICRO-HOPE (ramipril) Mortality Adapted from Dzau VJ, et al. Circulation. 2006;114;
19 Studies of Secondary Prevention of Micro- and Macroalbuminuria Regress Retard Prevent Macroalbuminuria Worsening nephropathy Reduce Microalbuminuria Mortality IRMA-2 (irbesartan) ADVANCE (perindopril) ONTARGET (telmisartan, ramipril) TRANSCEND (telmisartan) Adapted from Dzau VJ, et al. Circulation. 2006;114;
20 Studies of Reduction in Risk of Renal Events and Worsening Nephropathy Regress Retard Prevent Macroalbuminuria Worsening nephropathy Reduce Microalbuminuria IDNT (irbesartan) IRMA-2 (irbesartan) RENAAL (losartan) ADVANCE (perindopril) ONTARGET (telmisartan, ramipril) TRANSCEND (telmisartan) ACCOMPLISH (benazapril, amlodipine) ROADMAP (olmesartan) Mortality Adapted from Dzau VJ, et al. Circulation. 2006;114;
21 ACE-inhibitor in T1DM with Macroalbuminuria Reduces Renal Outcomes Lewis EJ et al. N Engl J Med 1993;329: guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association
22 Reduced Risk of Renal Events Study Treatment Renal events vs control (RRR) IDNT 1 (n=1715) Irbesartan 300 mg vs placebo 20%* (P=0.02) RENAAL 2 (n=1513) IRMA 2 3 (n=590) ADVANCE 4 (n=11240) ONTARGET 5 (n=25620) TRANSCEND 6 (n=5927) Losartan mg vs placebo 16%* (P=0.02) Irbesartan 150 mg vs placebo -44%**, (P=0.05) Irbesartan 300 mg vs placebo 68%**, (P<0.001) Perindopril 4 mg / Indapamide 1.25 mg vs placebo 21%** (P=0.006) Telmisartan 80 mg vs ramipril 10 mg +0% (NS) Telmisartan 80 mg vs placebo +29% (NS) Primary Endpoint? Yes, as a composite Yes, as a composite * Composite of doubling of serum creatinine, end-stage renal disease, and all-cause mortality; ** nephropathy Adjusted for baseline levels of microalbuminuria and the BP achieved during the trial; Composite renal outcome of dialysis or doubling of serum creatinine, changes in estimated glomerular filtration rate (GFR), and changes in albuminuria 1. Lewis EJ, et al. N Engl J Med 2001;345(12): de Galan BE, et al. J Am Soc Nephrol 2009;20(4): Brenner BM, et al. N Engl J Med 2001; 345: Mann JF, et al. Lancet 2008;372(9638): Parving HH, et al. N Engl J Med 2001;345(12): Mann JF, et al. Ann Intern Med 2009;151(1):1-10. Table adapted from García-Donaire JA, et al. Blood pressure.2011; 20: No No; secondary Yes, as a composite Yes, as a composite
23 Lowering Blood Pressure Reduces Renal Events in Type 2 Diabetes n =11,140 ADVANCE Collaborative group J Am Soc Nephrol, 2009.
24 Studies of Reduction in Risk of Mortality Regress Retard Prevent Macroalbuminuria Worsening nephropathy Reduce Microalbuminuria IDNT (irbesartan) RENAAL (losartan) IRMA-2 (irbesartan) DIRECT (candesartan) ADVANCE (perindopril) ROADMAP (olmesartan) ONTARGET (telmisartan, ramipril) TRANSCEND (telmisartan) ACCOMPLISH (benazapril, amlodipine) Mortality Adapted from Dzau VJ, et al. Circulation. 2006;114;

25
26 Cochrane Meta-analysis: Reduction of All-Cause Mortality 26 Significant effect for ACE inhibitors vs. placebo Treatment Mortality RRR vs placebo ACE inhibitors* -16% [0.73, 0.97] Studies included in the analysis: ADVANCE, BENEDICT, EUCLID, HOPE, Kvetny 2001, RASS, Ravid 1998, Tuominen No significant effect for ARBs vs. Placebo ARB +12% NS Studies included in the analysis: DIRECT, Perrin 2008, RASS, ROADMAP, TRANSCEND. No significant effect for ACE inhibitors vs. ARBs ACE inhibitors -2% NS Studies included in the analysis: ON-TARGET, RASS 2002 Adapted from Lv J, et al. Cochrane Database of Syst Rev. 2012;12:CD doi: / cd pub3.
27 Manage Slow Progression Measures BP and RAAS blockade (repeat creatinine and potassium 2 weeks after initiation of ACEI or ARB use): If with diabetes, target BP < 130/80, otherwise target BP < 140/90 * If with diabetes and with ACR > 3, start use of an ACEI or ARB as first-line therapy. If BP already < 130/80, use ACEI or ARB cautiously, monitoring for signs and symptoms of hypotension If without diabetes, ACR > 30 and BP > 140/90, start use of an ACEI or ARB as first-line therapy
28 GLYCEMIC CONTROL
29 Beware of Other Causes of CKD CKD: Chronic kidney disease guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association 29
 diabetes.")
30 When to Consider Other Causes of CKD Known duration of DM >5 years DM: Diabetes mellitus; egfr: Estimated glomerular filtration rate guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association 30
31 DCCT: Reduction in Albuminuria Primary Prevention Secondary Intervention 34% RRR (p<0.04) 43% RRR (p=0.001) 56% RRR (p=0.01) Solid line = risk of developing microalbuminuria Dashed line = risk of developing macroalbuminuria RRR = relative risk reduction CI = confidence interval The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:
32 EDIC: Early Glycemic Control Reduces Long-term Risk of Impaired GFR Risk reduction with intensive therapy 50% (95% CI 18-69; p=0.006) DCCT/EDIC Research Group. N Engl J Med 2011;365:
33 UKPDS: Post-trial Monitoring Legacy Effect After median 8.5 years post-trial follow-up Aggregate Endpoint Any diabetes related endpoint RRR: 12% 9% P: Microvascular disease RRR: 25% 24% P: Myocardial infarction RRR: 16% 15% P: All-cause mortality RRR: 6% 13% Holman R, et al. N Engl J Med 2008;359. P:




34 Metformin (K/DOQI guidelines) 34 egfr < 30 = STOP egfr = REDUCE dose Metformin does NOT cause kidney problems egfr 45 = USE FULL DOSE egfr = estimated glomerular filtration rate in ml/min/1.73m 2 National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 update. Am J Kidney Dis 2012;60(5):
35 Prevention of Diabetic Nephropathy Optimal glycemic control in type 1 and type 2 diabetes has been shown to reduce the development and progression of nephropathy
36 LIPID LOWERING THERAPY
37 Lipid reduction and the progression of renal disease Fried, L, Kidney Int 59: ,2001
38 Reducing LDL cholesterol with simvastatin 20mg and ezitimibe 10 mg/day in CKD patients stage 3-5, reduced adverse cardiovascular but not renal events over 4.9 years Lancet 2011; 377:
39 Lipid-Lowering in HD patients 4D Trial 1255 DM patients on HD; Atorvastatin v. placebo Avg decline in LDL 3.1 to 1.9 No difference at 4y Post-hoc analysis reduction in those with LDL > 3.76 AURORA 2776 HD patients not on statin; Crestor 10 mg v. placebo No difference in composite CV outcome at 3.8 y SHARP 3023 pts; 1/3 on HD; Simvistatin+Ezetrol v. placebo Trend toward NS in reduction in atherosclerotic events
40 Lipids Recommendations Lipid management for patients with CKD If with diabetes treat with a statin If without diabetes, age 50 treat with a statin If without diabetes, age <50, with risk such as having known coronary artery disease, prior stroke, or 10-year Framingham risk >10% treat with a statin (+/- ezetemibe if egfr<60) see KDIGO guidelines for further details
41 ANEMIA
42 Anemia in CKD has multiple causes insufficient erythropoietin iron deficiency chronic inflammation hyperparathyroidism blood loss ACEi/ARB aluminum toxicity other causes of anemia McGonigle, KI, 25: , 1984
43 Hemoglobin (g/dl) Evolution of Anemia in CKD EPO level (mu/ml) Expected EPO levels N= <10 Creatinine Clearance (ml/min) 10 Adapted from Radtke HW et al Blood 1979;54:877 and Erslev AJ. N Engl J Med 1991;324:1339
44 Hemoglobin targets for CKD revised CHOIR: RCT to Hb 11.3 v 13.5 in 1432 with GFR Adverse CV outcomes in 13.5% (Hb 11.3) v 17.5% (Hb 12.6) No change in QOL measures Singh et al, NEJM 2006; 355: CREATE: RCT to Hb v in 603, GFR No difference in time to first CV event (but underpowered) Better QOL (vitality score SF36) in high Hb group Drueke et al NEJM 2006:355: TREAT: DM RCT in 4000 CKD (GFR 20-60), DM2, Hb < 11; Intervention: darbepoietin v placebo; Goal: Hb 13 g/dl or rescue if < 9 g/dl; Outcome: all cause mortality, CV morbidity no different but higher rate of stroke and thrombolic events JASN 21: 2 6, 2010.
45 ESA Treatment prior to initiating treatment: control BP (< 160/90 mmhg) ensure adequate B12, folate, Fe (% saturation > 20) CSN Target: hemoglobin g/l (as per symptoms) Ongoing monitoring
46 Bicarbonate Supplementation
47 Metabolic Acidosis CKD Association (AASK) trial, renal event rates were approximately three times higher in patients whose serum bicarbonate was <20 as compared with >25 meq/l. After controlling for other factors, a serum bicarbonate of 28 to 30 meq/l was associated with the lowest risk for renal events. (UMC) 5422 patients, those whose serum bicarbonate was 22 as compared with 25 to 26 meq/l had a significantly increased risk for progression of renal disease (CRIC) Among 3939 patients in the CRIC study mentioned above, lower serum bicarbonate was significantly associated with a higher risk of (adjusted hazard ratio 0.97 for every 1 meq/l lower serum bicarbonate)
48 Metabolic Acidosis Mortality Association veterans with non-dialysis dependent CKD, those whose serum bicarbonate was <22 meq/l had a significantly higher risk of mortality as compared with those whose bicarbonate was 26 to 29 meq/l CKD stages 2-4, the four-year mortality rate was higher among those with a serum bicarbonate less than or equal to 22 as compared with greater than 26 meq/l (approximately 3 versus 2 percent) = NS maintenance hemodialysis, the two-year mortality rate was lowest among those whose serum bicarbonate was 17 to 19 meq/l normal bicarbonate concentrations usually reflect reduced protein intake and malnutrition
49 Bicarbonate Supplementation Bicarbonate supplementaion slows progression of CKD (JASN 2009) N=134, egfr 16-30, baseline HCO mEq/L Rx: 600 mg tid (1.8 g or about 0.4 teaspoon baking soda a day) x 2yr; Outcome: lower mean rate of decline of creatinine clearance compared with the control group (1.88 versus 5.93 ml/min/1.73 m 2 per year 6.5% v 33% reached ESRD Daily oral sodium bicarbonate preserves glomerular filtration rate by slowing its decline in early hypertensive nephropathy (Kidney International 2010) RCT n=120 hn + albuminuia, egfr 75.6 ml/min, S.bicarbonate 26. Rx: NaHCO3 v NaCl v placebo: 0.5 meq/kg (2.9g or about 0.6 teaspoon baking soda a day) x 5 yr Outcome: egfr 67.6 v 65.2 v 64.0 ml/min (-1.5 v. 2 v 2.1 ml/min/1.73m2)
50 Bicarbonate Supplementation HCO3 < 22 mmol/l associated with higher risk of worsening renal function. in part to the adaptive response of surviving nephrons to the loss of their neighboring nephrons an increase in ammonia production Activation of the complement system, RAAS and endothelin-1 Rx: maintain bicarbonate levels > 22 mmol/l No evidence of deleterious effects
51 Metabolic Bone Disease
52 Hyperphosphatemia A tendency toward phosphate retention begins early in renal disease due to the reduction in the filtered phosphate load phosphate retention is intimately related to the common development of cardiovascular disease risk in chronic kidney disease
53 CVD Arch Intern Med. 2007;167: West et al, CJASN 2010; 5:S41-47
54 Vit D 2 or D 3 reduce P in diet< 1 g/day Vit D 1,25 sterols P binders Ca carbonate Ca acetate sevelamer lanthanum carbonate nicotinamide PTH X Calcimimetics

55 Prevalence of CAC with CKD not on Dialysis
56 Hyperphosphatemia Rx Dialysis Patient Phos goal Stage 3 to 5 (not on dialysis) Phos goal normal Dietary restriction Phosphate binders Aluminum based avoided except short term 4 weeks Calcium based Non-Al, Non-Ca based (especially in hypercalcemic0 Renagel Sevalamer Fosrenol Lanthanum Carbonate
57 Hyperparathyroidism - Rx In addition to therapy of hyperphosphatemia Vitamin D Rx initiated if vitamin D deficiency exists Low levels of 25(OH)D; cholecalciferol (D3) Vitamin D analogues calcitriol (Rocaltrol) alfacalcidiol (One-Alpha) Other Calcimimetics (Cinacalcet) and EVOLVE Increased incidence of achieving target PTH, Phos, Ca But cinacalcet did not decrease the risk of death or major cardiovascular events among hemodialysis patients Parathyroidectomy
58 Protein intake


59 Other Considerations

60 Dialysis Modality Dialysis Modality HD v. PD Independent/Home Modality
61 Other Considerations Dialysis Access AVF v. AVG v. Tunnelled Catheter preferred type of access is a native fistula because a mature fistula has the lowest risk of complications, lowest need for intervention, and the best long-term patency Vein preservation measures
62 Transplantation Transplant options DD v LD Extended Criteria Paired Exchange High Sensitivity (National)

63 Ontario Renal Network
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Kidney Disease. Chronic kidney disease (CKD) requiring dialysis. The F.P. s Role in the Management of Chronic. Stages
 requiring dialysis. The F.P. s Role in the Management of Chronic. Stages") Focus on CME at McMaster University The F.P. s Role in the Management of Chronic Kidney Disease By David N. Churchill, MD, FRCPC, FACP Presented at McMaster University CME Half-Day in Nephrology for Family
Focus on CME at McMaster University The F.P. s Role in the Management of Chronic Kidney Disease By David N. Churchill, MD, FRCPC, FACP Presented at McMaster University CME Half-Day in Nephrology for Family
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER. The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR
 CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Applying clinical guidelines treating and managing CKD
 Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Chronic Kidney Disease The 6 Pillars. Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre
 Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
Chronic Kidney Disease The 6 Pillars Dr. Tiina Podymow Associate Professor Division of Nephrology McGill University Health Centre None Disclosures Objectives 1. Describe evidence-based measures to slow
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist
 Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Transforming Diabetes Care
 Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Chronic Kidney Disease in Primary Care
 Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
Clinical Stream Chronic Kidney Disease in Primary Care Dr Gerald Waters Dr Gerald Waters Renal Physician Chronic Kidney Disease Chronic Kidney Disease Normal functions of Kidneys Management of CKD Drugs
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Long-Term Care Updates
 Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Chronic renal failure
 Chronic renal failure Alexander Woywodt MD FRCP Consultant Physician and Nephrologist / Hon. Senior Lecturer Lancashire Teaching Hospitals NHS Foundation Trust Carnforth 13 th th October 2010 Menu Epidemiology
Chronic renal failure Alexander Woywodt MD FRCP Consultant Physician and Nephrologist / Hon. Senior Lecturer Lancashire Teaching Hospitals NHS Foundation Trust Carnforth 13 th th October 2010 Menu Epidemiology
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Disclosures. Topics. Staging and GFR. K-DOQI Staging of Chronic Kidney Disease. Definition of Chronic Kidney Disease. Chronic Kidney Disease
 Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
Disclosures Chronic Kidney Disease Consultant: Baxter Healthcare J. Kevin Tucker, M.D. Brigham and Women s Hospital Massachusetts General Hospital Topics Staging of chronic kidney disease (CKD) How to
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
KDIGO conference on high CV risk associated with CKD. The role of BP in CKD stage 1-4
 KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
Diabetes Renal Disease Management. Dr Paul Laboi Dr Vijay Jayagopal York Hospital
 Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Effective Health Care Program
 Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
PROs for Drug Development. Melanie Blank, MD
 PROs for Drug Development in Chronic Kidney Disease Melanie Blank, MD Disclaimer The views expressed here represent my opinions and do not necessarily represent the views of the FDA. Overview Stagnation
PROs for Drug Development in Chronic Kidney Disease Melanie Blank, MD Disclaimer The views expressed here represent my opinions and do not necessarily represent the views of the FDA. Overview Stagnation
Primary Care Physicians and Clinicians. XXX on behalf of the Upper Midwest Fistula First Coalition. Chronic Kidney Disease (CKD) Resources
 Resources") August 10, 2007 To: From: RE: Primary Care Physicians and Clinicians XXX on behalf of the Upper Midwest Fistula First Coalition Chronic Kidney Disease (CKD) Resources Caring for patients with chronic kidney
August 10, 2007 To: From: RE: Primary Care Physicians and Clinicians XXX on behalf of the Upper Midwest Fistula First Coalition Chronic Kidney Disease (CKD) Resources Caring for patients with chronic kidney
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
RETARDING PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD)
") 13 : 6 RETARDING PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD) Abstract: Chronic Kidney Disease (CKD) is common, harmful and treatable. It is worldwide public health problem, with several adverse outcomes;
13 : 6 RETARDING PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD) Abstract: Chronic Kidney Disease (CKD) is common, harmful and treatable. It is worldwide public health problem, with several adverse outcomes;
PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP
 PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP OUTLINE INTRODUCTION BURDEN OF CKD DEFINITION OF PRE-DIALYSIS CARE (PDC) GOALS OF PDC IN CKD COMPONENTS OF PDC ADVANTAGES
PRE-DIALYSIS CARE IN CHRONIC KIDNEY DISEASE PATIENTS DR O. A ADEJUMO MBBS, FWACP, FMCP OUTLINE INTRODUCTION BURDEN OF CKD DEFINITION OF PRE-DIALYSIS CARE (PDC) GOALS OF PDC IN CKD COMPONENTS OF PDC ADVANTAGES
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction