CPC:Review of Renal Disease
|
|
|
- Colleen Booth
- 5 years ago
- Views:
Transcription




1 CPC:Review of Renal Disease GERALD B. APPEL, MD Vivette D Agati, MD Membranoproliferative GN 1

 Anti-HCV Ab s in 91% HCV RNA detected in 86% HCV RNA and anti-hcv Ab to C22-3 are concentrated in")
.")
2 Case I An 8 yo boy develops pedal edema and is found to have 4+ proteinuria on dipstick of uirne by pediatrician. His Ccr is normal; 24 hour urine proteinuria is 9 g/day; Palbumin is 2.3 g/dl; P cholesterol 346 mg/dl; all serologic tests including ANA, complement, VDRL, Hep B Sag-Ab, etc are normal. Evidence for HCV in Essential-Mixed Cryoglobulinemia (EMC) Anti-HCV Ab s in 91% HCV RNA detected in 86% HCV RNA and anti-hcv Ab to C22-3 are concentrated in cryoglobulin (Ferri, Clin Exp Rheum 9:621, 1991) (Johnson, NEJM, 328:465, 1993) Case I A) The boy s mother, your friend asks should a renal biopsy be performed? You answer ( Yes, No, Maybe, Patient is too young for your to be concerned with never happens in adults ). B) The mother wants to know if there is specific Rx for this disease. You answer ( Yes, No, Maybe, Don t know never happens in adults). C) If a renal biopsy were performed it would most likely show on light microscopy (1,2,3,4). 2





3 Case I D) If the biopsy is done it will most likely show by IF ( 1,2,3,4 ). 3





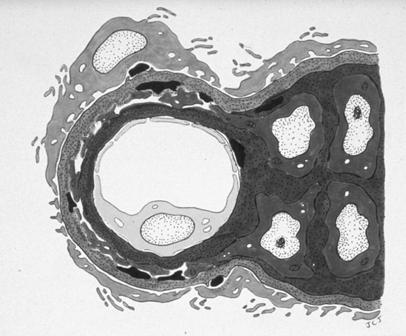
4 Case I Electron microscopy would most likely show ( 1,2,3,4). 4


 Since the patient s proteinuria is nonselective it is composed mostly of middle size globulins rathe than albumin ( T, F ).")
5 Case 2 A 19 yo AA college student is referred for 2nd opinion re her nephrotic syndrome. At 15 yo she was dxed w idiopathic NS w 16 g/d proteinuria, Palbumin 2.8 g/dl, Pcholesterol 300 mg/dl, Pcreatinine 1.0 mg/dl and neg. ANA, HBsAg-Ab, HCV, normal serum complement and BS. Bx then showed 22 glomeruli all WNL by LM, Neg by IF, and only fused foot processes by EM. She was Rxed w Prednisone 60 mg/d for several mo. w/o any change in proteinuria.edema has been controled w diuretics over 4 yrs and proteinuria is 5-10 g/day.proteinuira is non selective and her last Pcreatinine is 2.4 mg/dl Case 2 A) The pts GFR now is probably closest to 1) 10 cc/min, 2) 85 cc/min 3) 35 cc/min, 4) 70 cc/min. B) Since the patient s proteinuria is nonselective it is composed mostly of middle size globulins rathe than albumin ( T, F ). C) If a biopsy is done now it would most likely show by LM ( 1,2,3,4 ). Minimal Change Disease 5-10% Adults with NS, >85% children Usually sudden onset, hvy proteinuria, and edema In adults HBP 30%, Microhem 30 %,+/- Low GFR ( volume depletion ) Course : Respond to Strds, Relapse, No RF 5




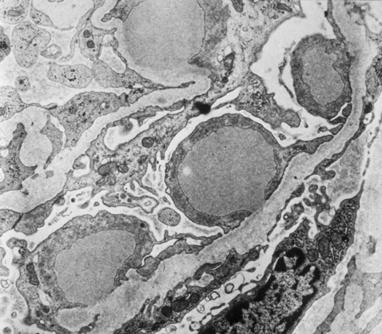
6 Case 2 D) Electron microscopy of the biopsy would most likely show ( 1,2,3,4 ). 6
 The patient asks if there is any proven therapy for her disease. You answer ( Yes, No, Maybe, If there is I don t know it ).")
 Creatinine Clearance as a Measure of Glomerular Filtration Rate C cr = volume of serum totally cleared of creatinine in a given interval (usually expressed")

7 Case 2 E) The patient asks if she will need dialysis some day. You answer ( Yes, No, Maybe, Everyone eventually will need dialysi if they live long enough ). F) The patient asks if there is any proven therapy for her disease. You answer ( Yes, No, Maybe, If there is I don t know it ). G) If the patient develops renal failure and gets a kidney TXP what are the chances the disease will recur in the TXP? ( 0%, 30%, 70%, 100% ) Creatinine Clearance as a Measure of Glomerular Filtration Rate C cr = volume of serum totally cleared of creatinine in a given interval (usually expressed as ml/min or L/Day Problems: Collection problems Must be steady state Over-estimates true GFR by 10-15% due to secretion of creatinine by tubule. Significant over-estimation at low GFR s Focal Segmental Glomerulosclerosis Increased frequency > 20% NS Blacks! In adults onset 2/3 NS, 1/3 proteinuria HBP > 30 %, Microhematuria >30 %, renal dysfunction 50 % Predictors of ESRD: hvy prot.,blks, high creatinine, on BX int fibrosis & Collapse Strds >50% respsond, cytoxan, cya, MMF Recurs 1/3 Txps- 7
 Clinical. Associated with heroin nephropathy, Obesity, SS disease chronic reflux nephropathy, late stage of FS prolif. GN, HIV.")

8 Case 2 Morphologic features similar to those seen in this case can also be seen frequently in which disease ( Use of Gold salts in rheumatoid arthritis, SLE, HIV disease, diabetes )? Focal Glomerulosclerosis (FSGS) Clinical. Associated with heroin nephropathy, Obesity, SS disease chronic reflux nephropathy, late stage of FS prolif. GN, HIV. Path: LM Focal segmental hyalin no inflammation IF IgM & C3 trapped in sclerotic lesions EM No deposits, fused foot processes Rx+Course Some respond to steroids or cytotoxic Usual relapse and/or become unresponsive Progresses to ESRDCan recur in Txp.( up to 30%) Proteinuria Dipstick Trace to 4+ semiquantitative Reflects concentration of protein not total thus affected by dilution Insensitive to globulins Bence Jones Protein 24 hr protein Collection problems Heavy excretion (over 3g/day) Usually glomerular disease Heavy excretion can be due to Bence Jones Proteins Case 3 A 62 yo businessman is admitted c/o 3 days of fever, cough and sputum. He has a R upper lobe infiltrate and middle lobe infiltrate on CXray. He is found to have 2+ proteinuria but no hematuria on adm. Urinalysis and his Pcreatinine is 1.1 mg/dl. Initial evaluation of his renal disease should include : 1) 24 hr collection for protein and creatinine, 2) renal USG, 3) repeat U/A in several days, 4) blood sample for anti-gbm antibodies. 8


 The medical student w you says he has cared for 2 pts already w edema: one with CHF and one w cirrhosis and ascites.")
9 Case 4 A 45 yo W M lawyer develops swelling of his feet. He states his eyes are swollen in the AM and he cannot put on his ring on his finger in the morning. At the end of the day his ankles and legs are swollen. His Pcreatinine 1.0 mg/dl, Palbumin 2.0 mg/dl, Pcholesterol 642 mg/dl, U/A 4+ protein 1+ heme, microscopic 3-5 rbc s,. All serologic tests including ANA, complementy, HepB and HCV, etc are WNL or negative. Case 4 B) You ask the patient if he has noted anything unusual about his urine. He answers: 1) It is dark 2) It is foamy 3) It is cloudy 4) It is coca cola colored. Case 4 A) The medical student w you says he has cared for 2 pts already w edema: one with CHF and one w cirrhosis and ascites. He asks why neither pt c/o periorbital edema like this pt. You answer. ( alternative tell medical student to do rectal exam on patient and quickly leave room to call nbephrologist for answer ) Case 4 C) Looking at this patients s urinalysis would most likely show: ( 1,2,3,4) 9





10 Case 4 D) Statistically this W adult with idiopathic nephrotic syndrome will most likely have which of the follow patterns on Bx by LM? ( 1,2,3,4 ). 10





11 Case 4 E) Silver stains can be very helpful in some diagnostic cases. In this biopsy they would most likely show? ( 1,2,3,4 ) 11





12 Case 4 F) IF staining for immunoglobulins and complement would be likely to show? ( 1,2,3,4) 12


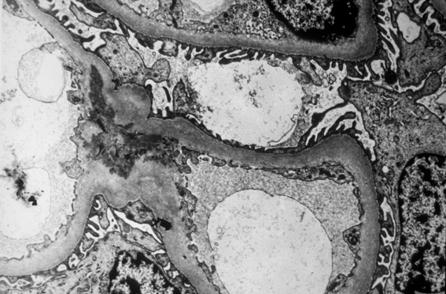


13 Case 4 G) Electron microscopy might show? ( 1,2,3,4) 13

.")
 What secondary form of NS has NOT been associated with this pattern?")

14 Case 4 H) The patient has the most likely pattern predicted on his biopsy. Your friend asks you the pathogenesis of this glomerular lesion. You answer ( alternative, another rectal exam and call nephrologist again ) I ) The patient asks if there is a cure for his disease. You answer ( Yes, No, Maybe ). J) The patient asks what the odds of his being on dialysis 10 yrs from now are. You answer ( 5%, 20%, 50%, 80% ). K) What secondary form of NS has NOT been associated with this pattern? ( w lung Cancer, w gold salt Rx, w HBV infection, w Lithium Rx for bipolar disease). Membranous Nephropathy Most common pattern idiopathic NS Caucasians Presents - proteinuria and NS HBP, microhematuria not rare Thromboses - RVT Pathology: thick cap walls + spikes IF + granular deposits, EM subepi deposits Course: ¼ spont remit, slow progressive RF Rx: Steroids alt cytoxan, CyA, other Nephrotic Syndrome Proteinuria: > 3.5 grams/24 hours Edema Hypoalbuminemia Hyperlipidemia 14
, SLE, Carcinomas, Medications (gold, captopril) Hypercoagulable state Renal vein thrombosis Rx: Steroids +")
 Urinalysis would most likely show which of the following ( 1,2,3,4 )?")
, P creatinine 1.")
15 Membranous Glomerulonephropathy Clinical: 30 40% W Adults with Idiopath N.S. (most common pattern) Associated with infections (Hep. B, Lues, malaria, schisto), SLE, Carcinomas, Medications (gold, captopril) Hypercoagulable state Renal vein thrombosis Rx: Steroids + cytotoxic, Ccyclosporine, MMF Course: Over 10 years 25% dead or ESRD 50% persistent prot / N.S. 25% Remit. 1. Sudden Deterioration Think RVT Think AIN 2. Elderly -? Underlying Tumor Case 5 A) Urinalysis would most likely show which of the following ( 1,2,3,4 )? Case 5 A 26 yo stock analyst while on vacation in Antigua develops a facial rash, low grade fever, lymphadenopathy, and arthritis of her hands, wrists, and ankles. Her ANA is + at 1:160, serum complement low, anti-dna antibody very elevated ( 1250 by ELISA ), P creatinine 1.6 mg/dl, and she has 3.4 g proteinuria/day. 15





16 Case 5 B) Renal biopsy might show all of the following EXCEPT which pattern by LM? ( 1,2,3,4 )? 16
 What pattern or Class of LN is most likley to be seen on the biopsy? ( Class II, III, Iv, V )?")
 anti-gbm antibodies.")

 The pt asks if a biopsy is necessary.")
17 Case 5 B) How often do patients w SLE have an entirely normal kidney biopsy? ( almost never, 10-20%, 30-40%, over 90% if no clinical renal disease ). C) What pattern or Class of LN is most likley to be seen on the biopsy? ( Class II, III, Iv, V )? D) The mechanism(s) of immune damage in DPLN include which of the following 1) chronic immune complex deposition 2) acute one-shot immune complex deposition c) in situ immune complex formation d) anti-gbm antibodies. F) LN recurs in most Kidney Txps but in a mild form ( T, F ) Case 6 A 43 yo jeweler has had insulin dependent diabetes mellitus for 21 yrs. His is poorly compliant with all his medications. Recently his MD noted proteinuria on the urine dipstick. On referral you find a BP of 145/85, a BS of 165 mg/dl, Pcreatinine 1.2 mg/dl, Cholesterol 320 mg/dl LDL cholesterol 222 mg/dl, 24 hr urinary protein 4g/d, and negative serologic evaluation. A) The pt asks if a biopsy is necessary. What part of the physical exam is helpful here? Table I Morphologic Patterns of Renal Involvement in SLE Class I Class II Class III Class IV Class V Normal Kidneys Mesangial Changes IIA Normal by LM, Positive by IF and EM IIB Mesangial Hypercellularity by LM, positive by IF and EM Focal and Segmental Proliferative Glomerulonephritis Diffuse Proliferative Glomerulonephritis Membranous Glomerulonephritis 17
.")



18 Case 6 B) If the biopsy is done it would be LEAST likely to show ( 1,2,3,4). Diabetes Mellitus: A Worldwide Public Health Problem 124 million patients with diabetes 2.1% of the world population 97% are patients with type 2 diabetes 221 million estimated by 2010 Complications of diabetes include - Coronary artery disease - Blindness - Peripheral vascular disease - Renal failure - Diabetic nephropathy - Disability Amos et al. Diabet Med. 1997;14(suppl 5):S1. - Stroke - Amputations 18

 Without a change in therapy the odds that this patient will progress to ESRD in 5 yrs are ( low, moderate, high, very high ). E) What might be done to slow the course to progressive ESRD here?")
19 Diabetes: The Most Common Cause of ESRD Primary Diagnosis for Patients Who Start Dialysis Other 10% Glomerulonephritis 13% No. of Patients 700 Projection Diabetes Hypertension 50.1% 27% 95% CI Number of dialysis 400 patients , , , R 2 =99.8% United States Renal Data System. Annual data report Case 6 C) What would be the most likely finding on EM of the biopsy? D) Without a change in therapy the odds that this patient will progress to ESRD in 5 yrs are ( low, moderate, high, very high ). E) What might be done to slow the course to progressive ESRD here? Treatment of Diabetic Nephropathy I. Control Glomerular Capillary Hypertension ( ACEinhib/ARBs ) II. Role of Glycemic Control III. Role of Blood Pressure Control IV. Role of Lipid Control 19
20 Lumen of Bowman s capsule Efferent arteriole The Glomerulus Proximal tubule Afferent arteriole RENAAL Primary Components % with event Doubling of Serum Creatinine Risk Reduction: 25% 30 p= Months P (+ CT) L (+ CT) P L % with event % with event ESRD 30 Risk Reduction: 28% p= Months P (+ CT) L (+ CT) ESRD or Death Risk Reduction: 20% 40 p= P 20 L Months P (+ CT) 762 L (+ CT) P L Angiotensin II Vascular Hypertrophy FGF Fibroblast Growth Factor Angiotensin II affects factors that modulate growth in cultured vascular smooth muscle cells TGFB1 Transforming Growth Factor Beta-1 PDGF Platelet Derived Growth Factor ILGF Insulin-like Growth Factor Case 7 A 52 yo F has had rheumatoid arthritis for 20 yrs and has been taking aspirin daily but no other medications for her disease. She develops edema and is found have the following labs: U/A 4+ protein, and maltese crosses, Pcreatinine 2.4 mg/dl, 24 hr prtoein 5.4 g/d, and negative or normal tests for complement, anti-dnaantibody, HBV, BS, HCV, etc. Kelbuchi, Y. et al, Hypertension, 21:1993. Itoh, H. et al, J Clin Invest, 91:1993. Study Titration Schedule Los 50 mg + prior therapy Maintain prior Antihypertensive therapy (excluding ACEI, AHA) NIDDM Patients with proteinuria N=1520 Los 100 mg + prior therapy Los 100 mg + Other Antihypertensive Therapy* (excluding ACEI, AHA) Goal BP <140/90 mmhg Case 7 A) Renal biopsy is most likely to show? ( 1,2,3,4 ). Placebo + prior therapy Placebo + prior therapy Placebo + Other Antihypertensive Therapy* (excluding ACEI, AHA) 2 Wks 4 Wks 4 Wks 4 Yrs Los: Losartan AIIA Angiotensin II Antagonists *Open-ended HCTZ (or flurosemide), beta blocker, CCB, alpha blocker or centrally-acting agent 20

 What other")

 What is a")

21 Case 7 B) What special stains might be useful here? C) What other diseases are commonly associated with this pathology? D) What is a differential diagnosis of proteinuria in a patient with Rheumatoid Arthritis? 21


 2) Occasional proliferative glomerular")
 3) Amyloid 5 10% 4) Arteritis (r/o PAN) 5) Complications of therapy a) Analgesics b) Gold c)")
22 Analgesic Nephropathy An international disease (Australia, Switzerland, Scandinavia, USA) Abusers and Users Headaches and Arthritis Female:Male 6:1 Large amounts over prolonged time periods Renal abnormalities sterile pyuria only mild proteinuria and hyperperfusion Decreased concentration ability Decreased net acid excretion Salt wasting Papillary necrosis Patients can recover function if they stop analgesic use Renal Disease in Rheumatoid Arthritis 1) Majority of patients no lesions or non-specific changes (in spite of high levels of CIC) 2) Occasional proliferative glomerular lesions (r/o SLE, MCTD, etc.) 3) Amyloid 5 10% 4) Arteritis (r/o PAN) 5) Complications of therapy a) Analgesics b) Gold c) Penicillamine d) Non-steroidal antiinflammatory agents i. AIN ii. Minimal Change in GN 22



23 Causes of Papillary Necrosis Pyelonephritis Obstruction Sickle Cell Disease Tuberculosis Cirrhosis Analgesic Abuse Radiation Diabetes (POSTCARD!) 23
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
The Nephrotic Syndrome
 The Nephrotic Syndrome Gerald B Appel, MD Vivette D Agati, MD Objectives Nephrotic Syndrome Define the nephrotic syndrome. Review the mechanism of proteinuria. Discuss the mechanisms of the major manifestations
The Nephrotic Syndrome Gerald B Appel, MD Vivette D Agati, MD Objectives Nephrotic Syndrome Define the nephrotic syndrome. Review the mechanism of proteinuria. Discuss the mechanisms of the major manifestations
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE
 Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome. Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium
 Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Evaluation and Management of Proteinuria. Negiin Pourafshar, MD University of Virginia Division of Nephrology
 Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Nephrotic Syndrome. Department of pediatrics The first affiliated hospital Sun Yat Sen University. Yue Zhihui ( 岳智慧 )
") Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Foamy Urine and Sickled Cells. Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA
 Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
GOOD MORNING. Welcome Applicants! Friday, October 31, (Happy Halloween!)
") GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Clinical Significance of ARF. Hospital Acquired Renal Insufficiency. Case - Acute Renal Failure. Hospital Acquired Renal Insufficiency
 Case - Acute Renal Failure 73 yo diabetic F w hx of mild HBP but normal renal function develops infection of R foot. Over 1 week fever, chills, inflammation swelling of her R foot and leg. She takes Motrin
Case - Acute Renal Failure 73 yo diabetic F w hx of mild HBP but normal renal function develops infection of R foot. Over 1 week fever, chills, inflammation swelling of her R foot and leg. She takes Motrin
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
11/9/2015. Childhood Nephrotic Syndrome: The Clinical Pathway. Learning Objectives. Nephrotic Syndrome - Definition. Proteinuria.
 Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
The CARI Guidelines Caring for Australasians with Renal Impairment. Specific management of IgA nephropathy: role of steroid therapy GUIDELINES
 Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Proteinuria (Protein in the Urine) Basics
 Basics") Proteinuria (Protein in the Urine) Basics OVERVIEW Proteinuria is the medical term for protein in the urine Urinary protein is detected by urine dipstick analysis, urinary protein: creatinine ratio (UP:C
Proteinuria (Protein in the Urine) Basics OVERVIEW Proteinuria is the medical term for protein in the urine Urinary protein is detected by urine dipstick analysis, urinary protein: creatinine ratio (UP:C
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
STEROID-RESISTANT NEPHROTIC SYNDROME (SRNS)
") MARIO NEGRI INSTITUTE FOR PHARMACOLOGICAL RESEARCH CLINICAL RESEARCH CENTRE FOR RARE DISEASES ALDO E CELE DACCO' Villa Camozzi - 24020 Ranica (Bergamo) Italy Telephone 39-35-4535304 fax 39-35-4535373 STEROID-RESISTANT
MARIO NEGRI INSTITUTE FOR PHARMACOLOGICAL RESEARCH CLINICAL RESEARCH CENTRE FOR RARE DISEASES ALDO E CELE DACCO' Villa Camozzi - 24020 Ranica (Bergamo) Italy Telephone 39-35-4535304 fax 39-35-4535373 STEROID-RESISTANT
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome
 P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH
 ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Proteinuria Nephrotic syndrome
 Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Proteinuria Nephrotic syndrome Pathophysiology & management Miriam Davidovits, MD Institute of Nephrology Schneider Children s Medical Center of Israel 1 Abnormal excretion of protein into the urine is
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Your Kidneys: Master Chemists of the Body
 Your Kidneys: Master Chemists of the Body National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation is developing guidelines for clinical care
Your Kidneys: Master Chemists of the Body National Kidney Foundation s Kidney Disease Outcomes Quality Initiative (NKF-KDOQI ) The National Kidney Foundation is developing guidelines for clinical care
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Renal Physiology - Lectures
 Renal Physiology 2011 Lisa M. Harrison-Bernard, PhD lharris@lsuhsc.edu Renal Physiology - Lectures Physiology of Body Fluids 2. Structure & Function of the Kidneys 3. Renal Clearance & Glomerular Filtration
Renal Physiology 2011 Lisa M. Harrison-Bernard, PhD lharris@lsuhsc.edu Renal Physiology - Lectures Physiology of Body Fluids 2. Structure & Function of the Kidneys 3. Renal Clearance & Glomerular Filtration
Dhanalakshmi.R II yr MD Stanley medical college
 Dhanalakshmi.R II yr MD Stanley medical college 10 Yr old female child - abdominal pain & vomiting for 1 day. Diffuse in nature, moderate in intensity, not related to food intake & radiates to back. No
Dhanalakshmi.R II yr MD Stanley medical college 10 Yr old female child - abdominal pain & vomiting for 1 day. Diffuse in nature, moderate in intensity, not related to food intake & radiates to back. No
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.