Yijuan Sun, Amarpreet Sandhu, Darlene Gabaldon, Jonathan Danaraj, Karen S. Servilla, and Antonios H. Tzamaloukas
|
|
|
- Charity Andrews
- 5 years ago
- Views:
Transcription
1 Case Reports in Nephrology Volume 2012, Article ID , 5 pages doi: /2012/ Case Report Development of Renal Failure without Proteinuria in a Patient with Monoclonal Gammopathy of Undetermined Significance: An Unusual Presentation of AL Kappa Amyloidosis Yijuan Sun, Amarpreet Sandhu, Darlene Gabaldon, Jonathan Danaraj, Karen S. Servilla, and Antonios H. Tzamaloukas Division of Nephrology, Raymond G. Murphy Veterans Affairs Medical Center, The University of New Mexico School of Medicine and VA Medical Center (111C), 1501 San Pedro SE, Albuquerque, NM 87108, USA Correspondence should be addressed to Yijuan Sun, yijuan.sun@va.gov Received 31 August 2012; Accepted 23 September 2012 Academic Editors: C. Garcia, C. I. Obialo, A. K. Saxena, and S. Zerbi Copyright 2012 Yijuan Sun et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. AL amyloidosis complicating monoclonal gammopathy of undetermined significance (MGUS) has usually a predominant glomerular deposition of lambda light chain. Heavy proteinuria is one of its cardinal manifestations. A 78-year-old man with a 9-year history of IgG kappa light-chain-mgus and normal urine protein excretion developed severe renal failure. Serum levels of kappa light chain and serum IgG had been stable while proteinuria was absent throughout the nine-year period. For the first eight years, he had stable stage III chronic kidney disease attributed to bladder outlet obstruction secondary to prostatic malignancy. In the last year, he developed progressive serum creatinine elevation, without any increase in the serum or urine levels of paraproteins or any sign of malignancy. Renal ultrasound and furosemide renogram showed no evidence of urinary obstruction. Renal biopsy revealed AL amyloidosis, with reactivity exclusive for kappa light chains, affecting predominantly the vessels and the interstitium. Glomerular involvement was minimal. Melphalan and prednisone were initiated. However, renal function continues deteriorating. Deposition of AL kappa amyloidosis developing during the course of MGUS predominantly in the wall of the renal vessels and the renal interstitium, while the involvement of the glomeruli is minimal, leads to progressive renal failure and absence of proteinuria. Renal biopsy is required to detect both the presence and the sites of deposition of renal AL kappa light chain amyloidosis. 1. Introduction The term monoclonal gammopathy of undetermined significance (MGUS) covers a spectrum of conditions characterized by production of a monoclonal immunoglobulin. The characteristic features of MGUS are a plasma concentration of the monoclonal protein less than 3 gm/dl, plasma cells representing less than 10% of all bone marrow cells, and absence of hypercalcemia, elevated serum creatinine, anemia (above 1.5 mg/dl), lytic bone lesions or severe symptomatic osteoporosis, and B-cell lymphoproliferative malignancy [1]. The prevalence of MGUS increases with age. In Olmsted County, MN, USA, 3.2% of the subjects 50 years old or older and 5.3% of the subjects 70 years old or older had MGUS [2]. A variety of life-threatening conditions may complicate MGUS. The risk of development of one of these conditions is approximately 1% per year of followup [3]. The list of conditions complicating MGUS includes multiple myeloma, Waldenstrom s macroglobulinemia, other lymphoproliferative malignancies such as chronic lymphocytic leukemia and IgM lymphoma, other hematologic malignancies, AL amyloidosis, chronic inflammatory demyelinating polyradiculopathy, autonomic neuropathy, osteoporosis, fractures of vertebrae and hips, liver and kidney transplants, hypercalcemia, and urticaria [3 5]. Renal disease, with a variety of histological pictures, complicates frequently the course of MGUS [6]. A distinct form of MGUS, light-chain-monoclonal gammopathy of undetermined significance (LC-MGUS), with a similar frequency of renal disease as the classical MGUS entity, has also been recognized [7]. AL amyloidosis with renal deposits of light chains is one of the conditions which may complicate
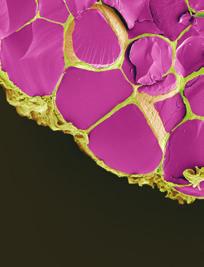
![2 Case Reports in Nephrology MGUS [6]. Nephrotic syndrome is the most frequent clinical presentation of this type of amyloidosis [6].](/docs-images/87/95098817/images/2-0.jpg "We present a patient who developed renal AL kappa amyloidosis manifested by progressive renal failure without proteinuria after several years of MGUS with stable paraprotein levels and renal function.")
2 2 Case Reports in Nephrology MGUS [6]. Nephrotic syndrome is the most frequent clinical presentation of this type of amyloidosis [6]. We present a patient who developed renal AL kappa amyloidosis manifested by progressive renal failure without proteinuria after several years of MGUS with stable paraprotein levels and renal function. Absence of extensive amyloid deposits in the glomeruli was the apparent reason for the absence of proteinuria in this patient. 2. Case Report A 78-year-old Caucasian man presented with stage V chronic kidney disease (CKD) in June MGUS had been diagnosed in early At that time, serum protein immunoelectrophoresis revealed a paraprotein with a concentration of 1.4 g/dl and characterized as IgG kappa by immunofixation; serum IgG was 2,263 mg/dl (normal range mg/dl); hemogram and serum IgA, IgM, albumin, calcium, and uric acid levels were normal; serum creatinine was 1.2 mg/dl; and urinalysis had no proteinuria. Bone marrow examination was not performed. In August 2003, he had a radical suprapubic prostatectomy for prostatic adenocarcinoma. He subsequently developed urinary incontinence with several bouts of urinary tract infection and stage III CKD with serum creatinine levels between 1.2 and 1.5 mg/dl. In November 2004, he had surgery for creation of artificial urinary sphincter. Between 2003 and 2012, his renal function remained stable. Serum levels of the paraprotein fluctuated between 1.4 and 2.3 g/dl, while serum IgG levels fluctuated between 1.4 and 2.4 g/dl. Serum-free kappa chain fluctuated between 38.3 and mg/dl (normal range mg/dl), and kappa/lambda ratio fluctuated between 4.20 and 8.36 (normal range ). Blood hemoglobin, white cell and platelet counts, and serum calcium and albumin remained within normal limits. Skeletal surveys showed no lytic bone lesions, while dual-energy X-ray absorptiometry (DEXA) studies showed osteopenia, but no osteoporosis. Serum creatinine was 2.28 mg/dl in January 2012 and increased progressively afterwards. He had not been on antihypertensive medications in the past and had no elevations of his blood pressure after the start of the rise in serum creatinine. Small amounts of IgG-kappa paraprotein ( mg/dl) were repeatedly detected in the urine. However, proteinuria, evaluated numerous times by urinalysis, spot urine protein to creatinine ratios and urine protein electrophoresis, had consistently remained in the normal range, even during episodes of urinary tract infection when pyuria and hematuria were present. Only one spot sample done while serum creatinine was 5.44 mg/dl in July 2012 had a small elevation of the urine protein/creatinine ratio to 0.3 mg/mg (normal values 0.2 mg/mg). Subsequent determinations of urine protein/creatinine ratio were all <0.2 mg/mg. Ultrasonography of kidneys, ureters and urinary bladder, and furosemide renogram did not disclose a urinary tract obstruction. A percutaneous kidney biopsy was performed in June At that time, serum creatinine was 3.86 mg/dl. Figure 1: Light microscopy. Adjacent efferent arteriole with significant deposits of amorphous eosinophilic material; glomerulus with same limited and segmental deposits in its wall; interstitium with the same deposits. The biopsy sample contained 45 glomeruli. On light microscopy, 15 glomeruli (33%) were globally sclerosed or severely hypoperfused. Discrete segmental expansion of the mesangial space by amorphous proteinaceous material was noted. Focal infiltration of the peritubular interstitium by amorphous, homogenous, acellular, and eosinophilic material was also noted. Approximately 50% of the sample showed extensive tubular atrophy and interstitial fibrosis. Arteries and arterioles showed the most striking finding: their walls were prominently infiltrated by the same amorphous eosinophilic material. The infiltrates caused severe narrowing of the vessels (Figure 1). Congo red staining of the biopsy revealed red affinity of the amorphous eosinophilic material (Figure 2(a)) and green birefringence upon examination under polarized light (Figure 2(b)). Immunofluorescence revealed reactivity for kappa light chains (Figure 3(a)) but negative for lambda light chain (Figure 3(b)). The kappa light chain deposits were small, discrete and segmental in the glomeruli, coarse and irregular in the interstitium, and pronounced, coarse and confluent in the wall of the vessels (Figure 3(a)). Electron microscopy showed very small and segmental deposits of nonbranching fibrils of 11.5 nm width in the mesangial areas and the subepithelial spaces of glomeruli and market thickening of the wall of arterioles by extensive accumulation of these nonbranching fibrils (Figures 4 and 5). The final histologic diagnosis was AL amyloidosis, with reactivity for kappa light chains exclusively and affecting predominantly the vessels and the interstitium, and only very focally and segmentally the glomeruli. Echocardiogram was not consistent with cardiac amyloidosis. He was started on melphalan and prednisone. However, his renal function progressively deteriorated, and hemodialysis was started in August Discussion A great variety of renal histological lesions has been associated with MGUS. Table 1 shows histological patterns of renal disease associated with MGUS reported in the literature [6, 8 25]. This large variety of renal lesions associated with
.")
.")


3 Case Reports in Nephrology 3 (a) (b) Figure 2: Congo red staining with red affinity primarily in the wall of the vessels and in the interstitium (a). The same structures show green birefringence on polarized light (b). (a) (b) Figure 3: Immunofluoresence study showing reactivity of the amorphous eosinophilic material for kappa light chains predominantly in vessels, limited in glomerulusc (a), but not lambda light chains (b). MGUS, the fact that the urinary findings may not conform to the expected findings in patients with a specific histological picture, which is illustrated by the patient of this report, plus the finding of renal pathology not associated with MGUS directly in some patients with MGUS and renal disease [6, 24], render kidney biopsy an indispensable tool for the diagnosis and management of renal disease complicating the course of MGUS. This point, however, has been established. The main point about AL amyloidosis secondary to MGUS illustrated by our patient is that the sites of deposition of amyloid in the kidneys are not always uniform and that clinical manifestations of renal disease are determined by the various sites of amyloid deposition. Moreover, this case presents with an uncommon deposition of kappa rather than lambda light chain. In addition to Bence Jones proteinuria, glomerular proteinuria, often in the nephrotic range, is a prominent manifestation of MGUS-related AL amyloidosis [6, 13]. The predominant site of AL amyloid deposition in the kidneys of patients with MGUS is the mesangium. In the study of Paueksakon et al. [6], all the 13 patients with MGUS and AL amyloidosis had mesangial expansion, and nephrotic syndrome was the most common clinical manifestation. Glomerular proteinuria is also a cardinal feature in patients with MGUS and other types of renal disease with primary glomerular involvement [7, 8, 11, 14, 16, 21 23]. Renal AL amyloidosis is not deposited exclusively in the glomeruli. Other kidney structures can be involved. In the study of Paueksakon et al. [6], AL amyloid deposits were also found in the renal interstitium in 8 of 13 patients and in the wall of the interlobular arteries in 7 of 13 patients.

![Renal histology References Cryoglobulinemic glomerulonephritis [6] AL amyloidosis [6, 13, 15, 24] Light chain cast nephropathy [6, 14, 24] Light chain deposition disease [6, 14, 19, 24] Heavy chain](/docs-images/87/95098817/images/4-1.jpg "deposition disease [6, 14, 24] Light chain and heavy chain deposition disease [6, 14] Light chain tubular crystal deposition [6] Waldenstrom s macroglobulinemic glomerulonephritis [8] Proliferative")
4 4 Case Reports in Nephrology Table 1: Renal histological lesions during the course of MGUS. Figure 4: Electron microscopy picture showing a greatly thickened renal vessel wall with accumulation of fibrils. Renal histology References Cryoglobulinemic glomerulonephritis [6] AL amyloidosis [6, 13, 15, 24] Light chain cast nephropathy [6, 14, 24] Light chain deposition disease [6, 14, 19, 24] Heavy chain deposition disease [6, 14, 24] Light chain and heavy chain deposition disease [6, 14] Light chain tubular crystal deposition [6] Waldenstrom s macroglobulinemic glomerulonephritis [8] Proliferative glomerulonephritis (several types) [9, 24, 25] Fibrillary or immunotactoid glomerulopathy [10, 11, 16, 18] Membranoproliferative glomerulonephritis [12, 22] Tubulointerstitial nephritis [17] Acute tubular necrosis [20] Membranous nephropathy [21] Dense deposit disease [23] Mixed lesions [14, 15] Acknowledgment Pathological figures are provided by the Division of Pathology, Brigham and Women s Hospital, Harvard Medical School, Boston, MA, USA. Figure 5: Higher magnification electron microscopy showing clearly the nonbranching fibrils in the wall of a renal vessel. One patient with MGUS and AL amyloid deposits exclusively in the arteries had heavy proteinuria, but she also had glomerular immune-type deposits [15]. The glomerular deposits of AL amyloid were minimal in our patient, while the deposits in the wall of the arteries, and to a lesser extent, the interstitium, were prominent. Commensurate with the paucity of glomerular deposits was a persistent and complete absence of glomerular proteinuria. Predominant amyloid deposits in sites other than the glomeruli have been described in AA amyloidosis. AA amyloidosis involving primarily tubular basement membranes presents with a picture of interstitial nephritis [26], while AA amyloidosis involving primarily the renal vessels presents with minimal or no proteinuria and progressive renal failure [27, 28]. We propose that in addition to AA amyloidosis, AL amyloidosis developing during the course of MGUS may also in rare instances involve predominantly the renal arteries and arterioles and cause renal failure without proteinuria. The fibrils in AL amyloidosis are derived from the variable region of lambda light chains in approximately 75 percent of cases and kappa in the remainder [29]. In this case, the diagnosis of AL kappa amyloidosis and its sites of deposition in the kidney by a kidney biopsy may guide the choice of treatment. References [1] P. Mollee, Current trends in the diagnosis, therapy and monitoring of the monoclonal gammopathies, The Clinical Biochemist Reviews, vol. 30, no. 3, pp , [2] R. A. Kyle, T. M. Therneau, S. V. Rajkumar et al., Prevalence of monoclonal gammopathy of undetermined significance, New England Medicine, vol. 354, no. 13, pp , [3] R. A. Kyle, T. M. Therneau, S. Vincent Rajkumar et al., A long-term study of prognosis in monoclonal gammopathy of undetermined significance, New England Medicine, vol. 346, no. 8, pp , [4] S. Y. Kristinsson, M. Björkholm,T.M.L.Anderssonetal., Patterns of survival and causes of death following a diagnosis of monoclonal gammopathy of undetermined significance: a population-based study, Haematologica, vol. 94, no. 12, pp , [5] J. P. Bida, R. A. Kyle, T. M. Therneau et al., Disease associations with monoclonal gammopathy of undetermined significance: a population-based study of 17,398 patients, Mayo Clinic Proceedings, vol. 84, no. 8, pp , [6] P.Paueksakon,M.P.Revelo,R.G.Horn,S.Shappell,andA. B. Fogo, Monoclonal gammopathy: significance and possible causality in renal disease, American Kidney Diseases, vol. 42, no. 1, pp , [7] A. Dispenzieri, J. A. Katzmann, R. A. Kyle et al., Prevalence and risk of progression of light-chain monoclonal gammopathy of undetermined significance: a retrospective population-based cohort study, The Lancet, vol. 375, no. 9727, pp , 2010.
5 Case Reports in Nephrology 5 [8]L.Morel-Maroger,A.Basch,F.Danon,P.Verroust,andG. Richet, Pathology of the kidney in Waldenström s macroglobulinemia. Study of sixteen cases, New England Medicine, vol. 283, no. 3, pp , [9] J. Lima, M. Monteagudo, M. Valles, F. Garcia-Bragado, M. Carrera, and M. Vilardell, Proliferative endo- and extracapillary glomerulonephritis and benign monoclonal IGM gammopathy, Nephron, vol. 56, no. 4, pp , [10] C.Rollino,R.Coppo,G.Mazzuccoetal., Monoclonalgammopathy and glomeulonephritis with organized microtubular deposits, American Kidney Diseases, vol. 15, no. 3, pp , [11] A. R. Esparza, J. A. Chazan, R. N. Nayak, and T. Cavallo, Fibrillary (immunotactoid) glomerulopathy: a possible role for kappa light chain in its etiology and/or pathogenesis, American Surgical Pathology, vol. 15, no. 7, pp , [12] H. G. Rennke, Secondary membranoproliferative glomerulonephritis, Kidney International, vol. 47, no. 2, pp , [13] A.Dysseleer,L.Michaux,J.P.Cosyns,E.Goffin, C. Hermans, and Y. Pirson, Benign monoclonal gammopathy turning to AL amyloidosis after kidney transplantation, American Kidney Diseases, vol. 34, no. 1, pp , [14] J. Lin, G. S. Markowitz, A. M. Valeri et al., Renal monoclonal immunoglobulin deposition disease: the disease spectrum, JournaloftheAmericanSocietyofNephrology, vol. 12, no. 7, pp , [15] G. S. Markowitz, M. P. Zdunek, and V. D. D Agati, Nephrotic syndrome, renal insufficiency, and a monoclonal gammopathy, American Kidney Diseases, vol.38,no.5,pp , [16] T. Nagao, T. Okura, K. I. Miyoshi et al., Fibrillary glomerulonephritis associated with monoclonal gammopathy of undetermined significance showing lambda-type Bence Jones protein, Clinical and Experimental Nephrology, vol. 9, no. 3, pp , [17] T. Hashimoto, K. Arakawa, Y. Ohta et al., Acquired fanconi syndrome with osteomalacia secondary to monoclonal gammopathy of undetermined significance, Internal Medicine, vol. 46, no. 5, pp , [18] S. Sundaram, R. Mainali, E. R. Norfolk, J. H. Shaw, and P. L. Zhang, Case report: fibrillary glomerulopathy secondary to light chain deposition disease in a patient with monoclonal gammopathy, Annals of Clinical and Laboratory Science, vol. 37, no. 4, pp , [19] T. Okura, K. I. Miyoshi, T. Nagao et al., Light chain deposition disease developing 15 years following the diagnosis of monoclonal gammopathy of undetermined significance, Internal Medicine, vol. 48, no. 2, pp , [20] I. M. Hii, M. L. Chen, and C. C. Chang, Benign monoclonal gammopathy-associated acute kidney injury: case report and literature review, Renal Failure, vol. 32, no. 5, pp , [21] S. de Seigneux, P. Bindi, H. Debiec et al., Immunoglobulin deposition disease with a membranous pattern and a circulating monoclonal immunoglobulin G with charge-dependent aggregation properties, American Kidney Diseases, vol. 56, no. 1, pp , [22] S. Sethi, L. Zand, N. Leung et al., Membranoproliferative glomerulonephritis secondary to monoclonal gammopathy, Clinical the American Society of Nephrology, vol. 5, no. 5, pp , [23] S. Sethi, W. R. Sukov, Y. Zhang et al., Dense deposit disease associated with monoclonal gammopathy of undetermined significance, American Kidney Diseases, vol. 56, no. 5, pp , [24] P. Stratta, L. Gravellone, T. Cena et al., Renal outcome and monoclonal immunoglobulin deposition disease in 289 old patients with blood cell dyscrasias: a single center experience, Critical Reviews in Oncology/Hematology, vol. 79, no. 1, pp , [25]F.Bidoux,S.Desport,V.Fremeaux-Bacchietal., Glomerulonephritis with isolated C3 deposits and monoclonal gammopathy: a fortuitous association? Clinical the American Society of Nephrology, vol. 6, no. 9, pp , [26] L. Valdez-Boyle, P. Adams, D. Wheeler, D. Malhotra, M. Pierdy, and A. H. Tzamaloukas, Renal amyloidosis presenting as interstitial nephritis, Clinical Nephrology, vol. 50, no. 4, pp , [27] H. M. Falck, T. Tornroth, and O. Wegelius, Predominantly vascular amyloid deposition in the kidney in patients with minimal or no proteinuria, Clinical Nephrology, vol. 19, no. 3, pp , [28] H. Uda, A. Yokota, K. Kobayashi et al., Two distinct clinical courses of renal involvement in rheumatoid patients with AA amyloidosis, Rheumatology, vol. 33, no. 8, pp , [29] V. Bellotti, G. Merlini, E. Bucciarelli, V. Perfetti, S. Quaglini, and E. Ascari, Relevance of class, molecular weight and isoelectric point in predicting human light chain amyloidogenicity, British Haematology, vol. 74, no. 1, pp , 1990.









6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Monoclonal gammopathies consist of. Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis REVIEW
 REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Multiple Myeloma Advances for clinical pathologists & histopathologists
 Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
WE PRESENT a patient with non insulindependent
 RENAL BIOPSY TEACHING CASE Monoclonal Gammopathy in a Type II Diabetic: A Case of Determined Significance Nancy J. Gritter, MD, Simin Goral, MD, and Agnes Fogo, MD INDEX WORDS: Monoclonal gammopathy; nephrotic
RENAL BIOPSY TEACHING CASE Monoclonal Gammopathy in a Type II Diabetic: A Case of Determined Significance Nancy J. Gritter, MD, Simin Goral, MD, and Agnes Fogo, MD INDEX WORDS: Monoclonal gammopathy; nephrotic
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Forms Revision: Myeloma Changes
 Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Light-Chain Mediated Acute Tubular Interstitial Nephritis. A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia
 Light-Chain Mediated Acute Tubular Interstitial Nephritis A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia Xin Gu, MD; Guillermo A. Herrera, MD Context. Acute renal failure
Light-Chain Mediated Acute Tubular Interstitial Nephritis A Poorly Recognized Pattern of Renal Disease in Patients With Plasma Cell Dyscrasia Xin Gu, MD; Guillermo A. Herrera, MD Context. Acute renal failure
Comparison of amyloid deposition in human kidney biopsies as predictor of poor patient outcome
 Castano et al. BMC Nephrology (2015) 16:64 DOI 10.1186/s12882-015-0046-0 RESEARCH ARTICLE Comparison of amyloid deposition in human kidney biopsies as predictor of poor patient outcome Open Access Ekaterina
Castano et al. BMC Nephrology (2015) 16:64 DOI 10.1186/s12882-015-0046-0 RESEARCH ARTICLE Comparison of amyloid deposition in human kidney biopsies as predictor of poor patient outcome Open Access Ekaterina
CORE CURRICULUM IN NEPHROLOGY Renal Manifestations of Plasma Cell Disorders
 CORE CURRICULUM IN NEPHROLOGY Renal Manifestations of Plasma Cell Disorders Nelson Leung, MD, 1 and S. Vincent Rajkumar, MD 2 INTRODUCTION Plasma cell dyscrasias represent a group of diseases characterized
CORE CURRICULUM IN NEPHROLOGY Renal Manifestations of Plasma Cell Disorders Nelson Leung, MD, 1 and S. Vincent Rajkumar, MD 2 INTRODUCTION Plasma cell dyscrasias represent a group of diseases characterized
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors of Renal Outcome
 International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Multiple intra-renal pathological injury patterns in resistant myeloma
 Multiple intra-renal pathological injury patterns in resistant myeloma Dharshan Rangaswamy 1, Mohit Madken 1, Mahesha Vankalakunti 2, Ravindra Prabhu Attur 1, and Shankar Prasad Nagaraju 1 1. Department
Multiple intra-renal pathological injury patterns in resistant myeloma Dharshan Rangaswamy 1, Mohit Madken 1, Mahesha Vankalakunti 2, Ravindra Prabhu Attur 1, and Shankar Prasad Nagaraju 1 1. Department
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Lec-14 د.خالد نافع. Medicine. Multiple Myeloma
 Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Article. Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy
 Article Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy Sanjeev Sethi,* Jason D. Theis,* Julie A. Vrana,* Fernando C. Fervenza,
Article Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy Sanjeev Sethi,* Jason D. Theis,* Julie A. Vrana,* Fernando C. Fervenza,
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Oncology Type of Article: Case Report Title:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Oncology Type of Article: Case Report Title:
Rituximab treatment for fibrillary glomerulonephritis
 Nephrol Dial Transplant (2014) 29: 1925 1931 doi: 10.1093/ndt/gfu189 Advance Access publication 27 May 2014 Rituximab treatment for fibrillary glomerulonephritis Jonathan Hogan, Michaela Restivo, Pietro
Nephrol Dial Transplant (2014) 29: 1925 1931 doi: 10.1093/ndt/gfu189 Advance Access publication 27 May 2014 Rituximab treatment for fibrillary glomerulonephritis Jonathan Hogan, Michaela Restivo, Pietro
Case Report Diaphragmatic Amyloidosis Causing Respiratory Failure: A Case Report and Review of Literature
 Volume 2015, Article ID 917157, 4 pages http://dx.doi.org/10.1155/2015/917157 Case Report Diaphragmatic Amyloidosis Causing Respiratory Failure: A Case Report and Review of Literature Aleksey Novikov,
Volume 2015, Article ID 917157, 4 pages http://dx.doi.org/10.1155/2015/917157 Case Report Diaphragmatic Amyloidosis Causing Respiratory Failure: A Case Report and Review of Literature Aleksey Novikov,
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease
 Case Study TheScientificWorldJOURNAL (2009) 9, 1348 1354 ISSN 1537-744X; DOI 10.1100/tsw.2009.164 A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1,
Case Study TheScientificWorldJOURNAL (2009) 9, 1348 1354 ISSN 1537-744X; DOI 10.1100/tsw.2009.164 A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1,
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Case Report Nonsecretory Multiple Myeloma and AL Amyloidosis Presenting with Nephrotic Range Proteinuria
 Case Reports in Nephrology Volume 2015, Article ID 635974, 4 pages http://dx.doi.org/10.1155/2015/635974 Case Report Nonsecretory Multiple Myeloma and AL Amyloidosis Presenting with Nephrotic Range Proteinuria
Case Reports in Nephrology Volume 2015, Article ID 635974, 4 pages http://dx.doi.org/10.1155/2015/635974 Case Report Nonsecretory Multiple Myeloma and AL Amyloidosis Presenting with Nephrotic Range Proteinuria
Renal manifestations of IgG4-related systemic disease
 Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Amyloidosis. James J. Stark, MD, FACP Medical Director Cancer Program Maryview Medical Center. Professor of Medicine Eastern Virginia Medical
 Amyloidosis James J. Stark, MD, FACP Medical Director Cancer Program Maryview Medical Center Professor of Medicine Eastern Virginia Medical School www.starkoncology.com 68 y.o. man admitted to MMC in March,
Amyloidosis James J. Stark, MD, FACP Medical Director Cancer Program Maryview Medical Center Professor of Medicine Eastern Virginia Medical School www.starkoncology.com 68 y.o. man admitted to MMC in March,
Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy: a case report
 Hirashio et al. BMC Nephrology (2018) 19:108 https://doi.org/10.1186/s12882-018-0905-6 CASE REPORT Open Access Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy:
Hirashio et al. BMC Nephrology (2018) 19:108 https://doi.org/10.1186/s12882-018-0905-6 CASE REPORT Open Access Favorable effect of bortezomib in dense deposit disease associated with monoclonal gammopathy:
Southern Derbyshire Shared Care Pathology Guidelines. MGUS (Monoclonal Gammopathy of Undetermined Significance)
") Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Clinical history. 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Cardiac catheterization: no CAD
 CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
A case of heavy chain deposition disease complicated by acquired angioedema.
 Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD
 Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
A Case of Myeloma Kidney With Glomerular C3 Deposition
 Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
Case Report World J Nephrol Urol. 2018;7(3-4):73-77 A Case of Myeloma Kidney With Glomerular C3 Deposition Asif Khan a, c, Khine Lam b, Suzanne El-Sayegh b, Elie El-Charabaty b Abstract Manuscript submitted
Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report of Neoadjuvant Use Enabling Complete Surgical Resection
 Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Jon Von Visger 1, Clarissa Cassol 2, Uday Nori 1, Gerardo Franco-Ahumada 1, Tibor Nadasdy 2 and Anjali A. Satoskar 2*
 Von Visger et al. BMC Nephrology (2019) 20:53 https://doi.org/10.1186/s12882-019-1239-8 CASE REPORT Open Access Complete biopsy-proven resolution of deposits in recurrent proliferative glomerulonephritis
Von Visger et al. BMC Nephrology (2019) 20:53 https://doi.org/10.1186/s12882-019-1239-8 CASE REPORT Open Access Complete biopsy-proven resolution of deposits in recurrent proliferative glomerulonephritis
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Long-Term Follow-up of Monoclonal Gammopathy of Undetermined Significance
 Original Article Long-Term Follow-up of Monoclonal Gammopathy of Undetermined Significance Robert A. Kyle, M.D., Dirk R. Larson, M.S., Terry M. Therneau, Ph.D., Angela Dispenzieri, M.D., Shaji Kumar, M.D.,
Original Article Long-Term Follow-up of Monoclonal Gammopathy of Undetermined Significance Robert A. Kyle, M.D., Dirk R. Larson, M.S., Terry M. Therneau, Ph.D., Angela Dispenzieri, M.D., Shaji Kumar, M.D.,
The New England Journal of Medicine
 A TRIAL OF THREE REGIMENS FOR PRIMARY AMYLOIDOSIS: COLCHICINE ALONE, MELPHALAN AND PREDNISONE, AND MELPHALAN, PREDNISONE, AND COLCHICINE ROBERT A. KYLE, M.D., MORIE A. GERTZ, M.D., PHILIP R. GREIPP, M.D.,
A TRIAL OF THREE REGIMENS FOR PRIMARY AMYLOIDOSIS: COLCHICINE ALONE, MELPHALAN AND PREDNISONE, AND MELPHALAN, PREDNISONE, AND COLCHICINE ROBERT A. KYLE, M.D., MORIE A. GERTZ, M.D., PHILIP R. GREIPP, M.D.,
Instructions for Plasma Cell Disorders (PCD) Post-HCT Data (Form 2116 Revision 3)
 Post-HCT Data (Form 2116 Revision 3)") (Form 2116 Revision 3) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Plasma Cell Disorders (PCD) Post-HCT Data Form. E-mail comments regarding the
(Form 2116 Revision 3) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Plasma Cell Disorders (PCD) Post-HCT Data Form. E-mail comments regarding the
Amyloidosis is caused by extracellular deposition of
 Mass Spectrometry Based Proteomic Diagnosis of Renal Immunoglobulin Heavy Chain Amyloidosis Sanjeev Sethi,* Jason D. Theis,* Nelson Leung, Angela Dispenzieri,* Samih H. Nasr,* Mary E. Fidler,* Lynn D.
Mass Spectrometry Based Proteomic Diagnosis of Renal Immunoglobulin Heavy Chain Amyloidosis Sanjeev Sethi,* Jason D. Theis,* Nelson Leung, Angela Dispenzieri,* Samih H. Nasr,* Mary E. Fidler,* Lynn D.
Szervusz [hi]everybody!
![Szervusz [hi]everybody!](/thumbs/89/98111920.jpg "Szervusz [hi]everybody!") Szervusz [hi]everybody! 1 Renal Injury due to Monoclonal Gammopathy Maria M. Picken MD, PhD mpicken@luc.edu MMPicken@aol.com ISA International Kidney Monoclonal Gammopathy Renal Pathology Society International
Szervusz [hi]everybody! 1 Renal Injury due to Monoclonal Gammopathy Maria M. Picken MD, PhD mpicken@luc.edu MMPicken@aol.com ISA International Kidney Monoclonal Gammopathy Renal Pathology Society International
Membranoproliferative Glomerulonephritis Secondary to Monoclonal Gammopathy
 Membranoproliferative Glomerulonephritis Secondary to Monoclonal Gammopathy Sanjeev Sethi,* Ladan Zand, Nelson Leung, Richard J.H. Smith, Dragan Jevremonic,* Sandra S. Herrmann, and Fernando C. Fervenza
Membranoproliferative Glomerulonephritis Secondary to Monoclonal Gammopathy Sanjeev Sethi,* Ladan Zand, Nelson Leung, Richard J.H. Smith, Dragan Jevremonic,* Sandra S. Herrmann, and Fernando C. Fervenza
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Sheena Surindran Grand Rounds 2/15/11
 Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Michael Joffe ST6 Haematology SpR
 Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance
 CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance S. Vincent
CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance S. Vincent
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
IgD Heavy-Chain Deposition Disease: Detection by Laser Microdissection and Mass Spectrometry
 IgD Heavy-Chain Deposition Disease: Detection by Laser Microdissection and Mass Spectrometry Virginie Royal,* Patrick Quint, Martine Leblanc, Richard LeBlanc, Garrett F. Duncanson, Robert L. Perrizo, Fernando
IgD Heavy-Chain Deposition Disease: Detection by Laser Microdissection and Mass Spectrometry Virginie Royal,* Patrick Quint, Martine Leblanc, Richard LeBlanc, Garrett F. Duncanson, Robert L. Perrizo, Fernando
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Vasishta Tatapudi, M.D. October 23 rd, 2012.
 Vasishta Tatapudi, M.D. October 23 rd, 2012. Case Summary Chief complaint: 45 year old African American male patient presented with left shoulder pain after minor trauma. History of present illness: Two
Vasishta Tatapudi, M.D. October 23 rd, 2012. Case Summary Chief complaint: 45 year old African American male patient presented with left shoulder pain after minor trauma. History of present illness: Two
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft
 Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Renal Involvement in Plasma Cell Dyscrasias
 Renal Involvement in Plasma Cell Dyscrasias Sunil Prakash Head of Nephrology Division, Department of Medicine, Central Hospital (N. Railways), New Delhi. 132 Abstract Multiple myeloma and amyloidosis are
Renal Involvement in Plasma Cell Dyscrasias Sunil Prakash Head of Nephrology Division, Department of Medicine, Central Hospital (N. Railways), New Delhi. 132 Abstract Multiple myeloma and amyloidosis are
Case Report AL-Amyloidosis Presenting with Negative Congo Red Staining in the Setting of High Clinical Suspicion: A Case Report
 Case Reports in Nephrology Volume 2012, Article ID 593460, 4 pages doi:10.1155/2012/593460 Case Report AL-Amyloidosis Presenting with Negative Congo Red Staining in the Setting of High Clinical Suspicion:
Case Reports in Nephrology Volume 2012, Article ID 593460, 4 pages doi:10.1155/2012/593460 Case Report AL-Amyloidosis Presenting with Negative Congo Red Staining in the Setting of High Clinical Suspicion:
Plasma cell dyscrasia with renal impairment including MGRS
 Plasma cell dyscrasia with renal impairment including MGRS ~ The importance of multi-departmental management ~ Dept. Nephrology, Japan Community Health Care Organization Sendai Hospital Shinichi Mizuno
Plasma cell dyscrasia with renal impairment including MGRS ~ The importance of multi-departmental management ~ Dept. Nephrology, Japan Community Health Care Organization Sendai Hospital Shinichi Mizuno
Minimal change disease: A case report of an unusual relationship
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Minimal change disease: A case report of an unusual relationship Fahad Edrees Washington University School
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Minimal change disease: A case report of an unusual relationship Fahad Edrees Washington University School
Multiple myeloma evolves from a clinically silent premalignant
 S. VINCENT RAJKUMAR Updated Diagnostic Criteria and Staging System for Multiple Myeloma S. Vincent Rajkumar, MD OVERVIEW There has been remarkable progress made in the diagnosis and treatment of multiple
S. VINCENT RAJKUMAR Updated Diagnostic Criteria and Staging System for Multiple Myeloma S. Vincent Rajkumar, MD OVERVIEW There has been remarkable progress made in the diagnosis and treatment of multiple
Understanding the Serum Free Light Chain Assays. Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc.
 Understanding the Serum Free Light Chain Assays Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. AL Amyloidosis: abnormality of proteins from Plasma Cells in the Bone Marrow Red
Understanding the Serum Free Light Chain Assays Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. AL Amyloidosis: abnormality of proteins from Plasma Cells in the Bone Marrow Red
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Ultrasound-guided percutaneous renal biopsyinduced accessory renal artery bleeding in an amyloidosis patient
 Zhang et al. Diagnostic Pathology 2012, 7:176 CASE REPORT Open Access Ultrasound-guided percutaneous renal biopsyinduced accessory renal artery bleeding in an amyloidosis patient Qing Zhang *, Yongqiang
Zhang et al. Diagnostic Pathology 2012, 7:176 CASE REPORT Open Access Ultrasound-guided percutaneous renal biopsyinduced accessory renal artery bleeding in an amyloidosis patient Qing Zhang *, Yongqiang