Chris Douglass. BGS Trainees Weekend 2018
|
|
|
- Bruno Marsh
- 6 years ago
- Views:
Transcription
1 Chris Douglass
2 A term used to describe other clinical conditions which can mimic a stroke and confound diagnosis. brain tumours, epilepsy subdural haematosis. Neurologic abnormalities similar to a stroke can also be the result of imbalances of glucose, sodium and calcium.
3 Can be 30-50% of acute stroke evaluations. 19% Libman et al. Arch Neurol 1995; 52 (11): % Rønning et al. Tidssker NorLeageforan 2005;16: % Hemmen et al. J. Stroke Cerebrovasc Dis. 2008; 17 (1): % Hand et al. Stroke 2006; 37 (3): % Röther et al Poster AHA International Stroke Conference
4 411 patients coded as stroke in SanDiego Stroke Centre 19 ICH 6 SAH 3 SDH 11 old CVA 11 hypotension 5 migraine 10 seizures 8 intoxication 6 mass lesion 7 hypoglycaemia 18 other 42% of these mimics had an acute disease caused by a severe neurological condition other than stroke

5 52 were strokes (40 ischaemic, 6 bleeds, 6 TIAs). 48 were mimics 9 Functional 8 Seizures 6 Migraines 4 Infection with old CVA symptoms 4 Tumour 3 Labyrinthitis 3 Bell s palsy 2 Vasculitis in known neurology patients 2 Delirium 7 Others (Hypotension, Hemifacial spasm, Hypoglycaemia (ABCDEFG), Respiratory failure, Concussion, Anaemia Hb=2, Infective exacerbation of MS)
6
7
8 PC; Sudden onset tingling in right face and arm with dysarthria HPC; 2 episodes of right face pins and needles lasting 10 minutes in last 2 weeks. PMH; Left occipital lobe stroke years ago Lung cancer, completed courses of chemo and radiotherapy.

9




10
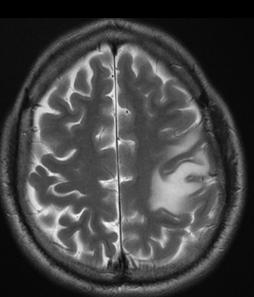
11 PC; sudden onset dense left sided weakness, arm 0/5, leg 2/5, left sided neglect, gaze preference to the right HPC; dragging left leg for 2 weeks, ½ stone weight loss last few months CXR CT Witnessed focal motor seizures with Todd s paresis



12


13
14 5% of tumours have a stroke like presentation Acute onset due to Bleed into a lesion Extrinsic compression of vascular structures Obstructive hydrocephalus Todd s paresis Scan appearances of early mass effect more likely to indicate tumour as stroke oedema may take hours to occur
15 Sudden onset aphasia, only able to say yes/no. NIHSS of 7. CT and CTA reported as normal so thrombolysed. Had a seizure after tpa infusion completed so rescanned and when second scan compared to the first in hindsight a left frontal lobe abnormality was seen on original CT. Had an MRI at the 24 hour point and this showed changes consistent with a high grade GBM, subsequently confirmed on biopsy.






16 BG S ne es ai Tr W en d ee k 20 18
17 PC; found on floor with dense left sided weakness and slurred speech SH; alcohol abuse o/e; global weakness, unsafe swallow CT reported as brainstem infarction Required PEG feeding, tracheostomy, prolonged stay on neuro-rehab unit


18



19 BG S ne es ai Tr W en d ee k 20 18
20 Osmotic demyelination syndrome Can be in the pons or other areas of the brain Common in alcoholism, rapid correction of hyponatraemia or with use of cyclosporin in liver transplantation whenever a patient who is gravely ill with alcoholism and malnutrition or a systemic medical disease develops confusion, quadriplegia, pseudobulbar palsy, and pseudo coma ( locked-in syndrome ) over a period of several days, one is justified in making a diagnosis of central pontine myelinolysis
21 PC; Sudden onset slurred speech, facial weakness, nystagmus. CT reported as left postero-frontal ischaemia MRI requested



22 BG S ne es ai Tr W en d ee k 20 18
23 Sudden onset vertigo can be central (stroke) or peripheral Dix Hallpike test Duration of nystagmus Central lesions Persistent Peripheral lesions Less than 60 secs Onset of nystagmus Immediate Delay of 0-40 secs Fatiguability of nystagmus Character of nystagmus Severity of symptoms Non-fatiguable Variable Mild (but marked nystagmus) Fatiguable Fixed; torsional upwards towards lower most ear Severe vertigo with nausea
24 PC; left sided weakness HPC; 2 weeks headache and left sided heaviness o/e; keen to keep his cap on scalp dressing oozing

25



26

27 Knocked on neighbour s door at midnight Naked, sweaty, confused. Right sided weakness 5 days frontal headache 2 days cough Lives alone, alcohol abuse, self-neglect Chest clear, normal heart sounds

28

29

30

31

32

33 Treated with Ceftriaxone and Metronidazole. Fungal and Toxoplasmosis serology awaited. Echo no obvious abnormality but will need a TOE. HIV -ve Seizures in this admission. Blood and CSF cultures -ve. CSF WCC 32, CSF glucose 3.2/ serum Glu 5.8, CSF protein 1.33 CRP 208 Remains confused and agitated. Not keeping any clothes on. Echo x3 NAD (High BMI, agitated so poor views)
34 Acute or subacute worsening of signs in same vascular territory as old stroke Patients with previous stroke who become unwell with hyponatraemia, sepsis or severe fatigue (lying on floor all night) whose clinical signs worsen. Clues are old stroke on CT and in history with new symptoms consistent with old stroke. Patients improve when sepsis or other cause treated. Raised CRP, WCC or low sodium.
35 Difficult when stroke and aspiration pneumonia overlap Sepsis may cause stroke (mycotic emboli, hypercoagulable state)

36
37 Seizures after stroke study Arch Neurol; : % of patients have post stroke seizures 8.6% of ischaemic strokes (40% in first 24 hours) 10.6% of haemorrhagic strokes (57% in first 24 hrs) 3.4% in first 24 hours 2% at onset 2.5% have recurrent seizures
38 328 patients had prolonged video-eeg pre epilepsy surgery work up PP occurred in 44 patients (13.4%) PP was always unilateral and always contralateral to the seizure focus The mean duration of PP was 174 seconds (range 11 seconds to 22 minutes) Of all seizures followed by PP, the following features were noted: Obvious ictal motor activity was seen in 78% Very slight ictal motor activity was seen in 10 % No ictal motor activity was seen in nearly 10 % Gallmetzer etal "Postictal paresis in focal epilepsies-- incidence, duration, and causes: a video-eeg monitoring study." 62 (12). pp
39 Rolack et al JNNP 1992;55:63-64 Post-epileptic paralysis persisted from half an hour to 36 hours, with a mean of 15 hours. The nature, duration, and severity of PEP were unrelated to the duration or severity of the seizures, the presence or absence of underlying lesions, or any changes on the EEG. Weakness always persisted longer than other symptoms. Post-epileptic paralysis occurred sporadically
40 27% have a headache at onset of the stroke Primary headache disorders account for 10% of stroke mimics Migraines can be associated with conditions causing increased stroke risk Anti-phospholipid syndrome CADASIL & MELAS Carotid dissection

41
42 waxdis Serene Branson
43 Usually young Usually lack vascular risk factors (but beware angina ) Often multiple unexplained symptoms or syndromes over many years or operations Often other diagnoses such as: sero-negative SLE/sero-negative arthritis fibromyalgia cholecystectomy, appendicectomy and hysterectomy May or may not have any psychiatric history apparent
44 History usually vague, long list inconsistent within one telling inconsistent between tellings contains mutually inconsistent features Presentation often delayed e.g. 3/7 after onset of severe hemiparesis
45 Variable signs from one examination to another. No objective features e.g. tone, reflexes, plantars Variable effort & power grunts/grimaces agonist/antagonist encourage up to normal ( one finger test ) collapsing quality to the weakness Mutual inconsistencies e.g. numb hand/tie laces/make-up/jewellery/buttons high-heels Non-sensical sensory signs turn over no vibration on sternum finger to nose

46 2005 by BMJ Publishing Group Ltd Hoover s sign. J Stone et al. J Neurol Neurosurg Psychiatry 2005;76:i2-i12

47

48

49
50 2005 by BMJ Publishing Group Ltd Hemisensory disturbance. Charcot 1889 J Stone et al. J Neurol Neurosurg Psychiatry 2005;76:i2-i12

51
52 Winkler et al Stroke 2009; 40: /250 thrombolysed patients were mimics. Mostly seizures Global aphasia with no hemiparesis 3/7 mimics (43%) cf 8/243 (3.3%) strokes Thrombolysed Strokes; 1.2% angioedema, 5.3% symptomatic intracranial bleed, 12.3% asymptomatic intracranial bleed. Thrombolysed Mimics; 0%, 0%, 0%
53 Scott PA. Ann. Emerg. Med (5): /151 (7%) patients thrombolysed in ED were stroke mimics 0% intracerebral bleeds mrs and age were lower in mimic group

54 113 consecutive thrombolysed patients /113 had negative MRI at 24 hours 10 conversion disorder 2 Todd s paresis 4 TIA -4 migraine -3 encephalopathy Cost $185,822 cost of MRI on admission = $110,543 A median excessive cost of $5,427 per admission
55 Stroke mimic patients classified according to initial NIHSS. NIHSS indicates National Institutes of Health Stroke Scale. Ali S F et al. (2014). The TeleStroke Mimic (TM) Score: A Prediction Rule for Identifying Stroke Mimics Evaluated in a Telestroke Network. Journal of the American Heart Association /JAHA Ali S F et al.

56 Seizures 17% Systemic infection 17% Brain tumour 15% Toxic/metabolic 13% Positional vertigo 6% Conversion Disorder Migraine Syncope Transient global amnesia

57 Decreased level of consciousness and normal eye movements increased the odds of a stroke mimic being present Abnormal visual fields, initial diastolic blood pressure greater than 90 mmhg, atrial fibrillation, and history of angina decreased the odds of mimic being present.
58 Strokes that imitate other diseases Gradual or stuttering onset No clear arterial territory Subthalamic nucleus stroke Hemiballismus/myoclonus Bilateral thalamic strokes Persistent acute global amnesia Limb shaking TIA Focal epilepsy Cortical stroke (hand motor Peripheral nerve lesion area) Bilateral Occipital CVA Confusion/delerium
59
60
61

62

63
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Using the Neuro Exam to Diagnose Mimics
 Using the Neuro Exam to Diagnose Mimics Jennifer Simpson, MD Neurohospitalist Vascular Neurologist None 2 Review the differential diagnosis for stroke Identify patients physical examination findings that
Using the Neuro Exam to Diagnose Mimics Jennifer Simpson, MD Neurohospitalist Vascular Neurologist None 2 Review the differential diagnosis for stroke Identify patients physical examination findings that
Stroke Mimics. Atlantic Canada Stroke Conference. Dr Warren Fieldus FRCP
 Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Failure to wake. Robin S. Howard
 Failure to wake Robin S. Howard National Hospital for Neurology and Neurosurgery, Queen Square St. Thomas Hospital, Guys & St. Thomas NHS (Foundation) Trust Royal College of Physicians - November 2017
Failure to wake Robin S. Howard National Hospital for Neurology and Neurosurgery, Queen Square St. Thomas Hospital, Guys & St. Thomas NHS (Foundation) Trust Royal College of Physicians - November 2017
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
A Stroke, is a Stroke is a Stroke.or is it? Stroke Mimics and Red Flags. Liz O Brien Stroke Nurse Practitioner Royal North Shore Hospital Sydney
 A Stroke, is a Stroke is a Stroke.or is it? Stroke Mimics and Red Flags Liz O Brien Stroke Nurse Practitioner Royal North Shore Hospital Sydney Elizabeth O'Brien, Stroke NP RNSH, Smart Outline of Presentation
A Stroke, is a Stroke is a Stroke.or is it? Stroke Mimics and Red Flags Liz O Brien Stroke Nurse Practitioner Royal North Shore Hospital Sydney Elizabeth O'Brien, Stroke NP RNSH, Smart Outline of Presentation
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
All that blacks out is not syncope: a neurological view of transient loss of consciousness
 All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
10/13/2017. AllinaHealthSystems. Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program
 Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
HYPERACUTE STROKE CASE STUDIES. By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH
 HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
HYPERACUTE STROKE CASE STUDIES By Mady Roman Hyper Acute Stroke Nurse Practitioner RHH MC Case study 82 years old, lady 9:30 well, in touch with her son 11:30 hairdresser came to her house and found her
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
The Neurologic Examination. John W. Engstrom, M.D. University of California San Francisco School of Medicine
 The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health
 what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Most hypertensive: headache, vomiting, seizures, changes in mental status, fever, changes EKG
 Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Suspected neurological conditions: clinical questions
 Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Neurologic Examination
 John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Dr Jo-Anne Pon. Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch
 Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
Ischemic Stroke in Critically Ill Patients with Malignancy
 Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Dizziness: Neurological Aspect
 Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Epilepsy after two different neurosurgical approaches
 Journal ofneurology, Neurosurgery, and Psychiatry, 1976, 39, 1052-1056 Epilepsy after two different neurosurgical approaches to the treatment of ruptured intracranial aneurysm R. J. CABRAL, T. T. KING,
Journal ofneurology, Neurosurgery, and Psychiatry, 1976, 39, 1052-1056 Epilepsy after two different neurosurgical approaches to the treatment of ruptured intracranial aneurysm R. J. CABRAL, T. T. KING,
Pause for thought. Dr Jane Anderson Consultant Neurologist
 Pause for thought Dr Jane Anderson Consultant Neurologist Which is the top cause of years lived with disability worldwide? 1. COPD 2. Low Back pain 3. Diabetes 4. Migraine with medication overuse headache
Pause for thought Dr Jane Anderson Consultant Neurologist Which is the top cause of years lived with disability worldwide? 1. COPD 2. Low Back pain 3. Diabetes 4. Migraine with medication overuse headache
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
e) None of the above e) None of the above
 None of the above e) None of the above") Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
MIGRAINE CLASSIFICATION
 MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
T he neurological examination is often used to decide
 545 PAPER Detection of focal cerebral hemisphere lesions using the neurological examination N E Anderson, D F Mason, J N Fink, P S Bergin, A J Charleston, G D Gamble... See end of article for authors affiliations...
545 PAPER Detection of focal cerebral hemisphere lesions using the neurological examination N E Anderson, D F Mason, J N Fink, P S Bergin, A J Charleston, G D Gamble... See end of article for authors affiliations...
Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease
 Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease Summary Outline of the presentation of stroke in paediatric patients with sickle cell disease, urgent investigations,
Guideline for the Acute Management of Stroke in Paediatric Patients with Sickle Cell Disease Summary Outline of the presentation of stroke in paediatric patients with sickle cell disease, urgent investigations,
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management