The surgical strategy of hypertensive thalamus hemorrhage. Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital
|
|
|
- Nicholas Hampton
- 5 years ago
- Views:
Transcription
1 The surgical strategy of hypertensive thalamus hemorrhage Lu Ma, Chao You Dept. of Neurosurgery, West China Hospital
2 Preface Spontaneous Intracranial hemorrhage (SICH) Spontaneous thalamus hemorrhage---hypertensive thalamus hemorrhage in main land of China Hypertensive thalamus hemorrhage (HTH) was treated as a forbidden area for surgery for long time because of the high mortality and morbidity.
,")
 arteries, and posterior (medial and lateral)")
3 Anatomy The thalamus derives its blood supply from four arteries including the polar artery (posterior communicating artery), paramedian thalamic-subthalamic arteries, inferolateral (thalamogeniculate) arteries, and posterior (medial and lateral) choroidal arteries.
4 Categorization--bleeding sites Traditional: Medial---ventricle Lateral--- basilar ganglion Our categorization: limited thalamus hematoma (LTH) thalamic-ventricular hematoma (TVH) thalamic-basilar ganglion hematoma (TBH) thalamic-mesencephalic hematoma (TMH) mixed thalamus hematoma (involving three or more than three sites) (MTH)


5 limited thalamus hematoma M,52Y.O., admission for R limb numbness for 6h, without LOC,Diag: Left LTH,Conservative treatment and recovered well.

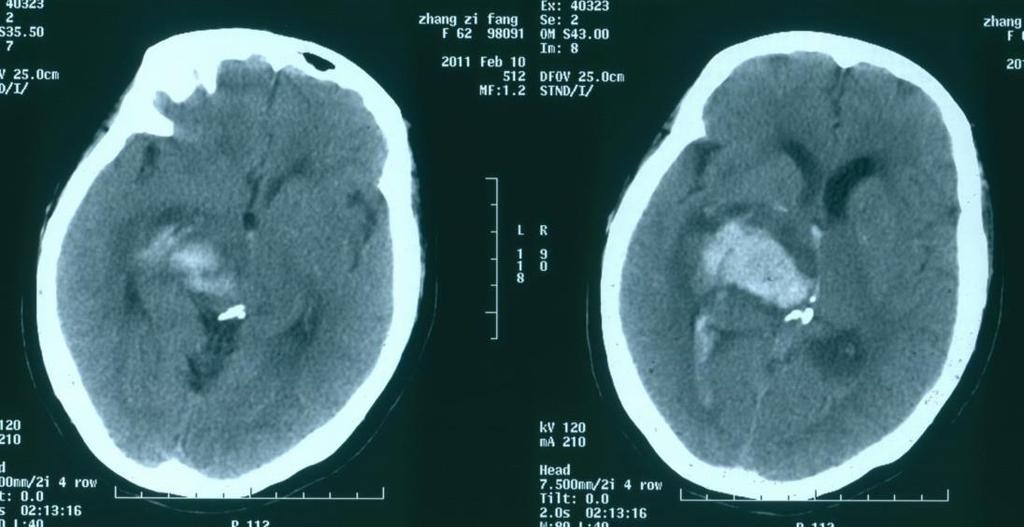
6 thalamic-ventricular hematoma M, 46Y.O., Admission for LOC for 4h, Diag: Left TVH

7 F,55Y.O., admission for sudden headache and LOC for 5h. Diag: left TVH

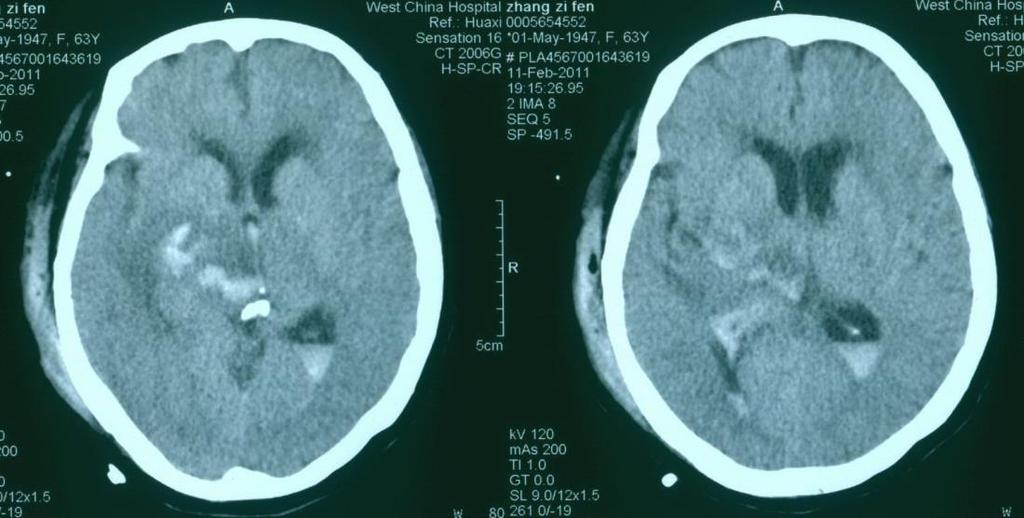
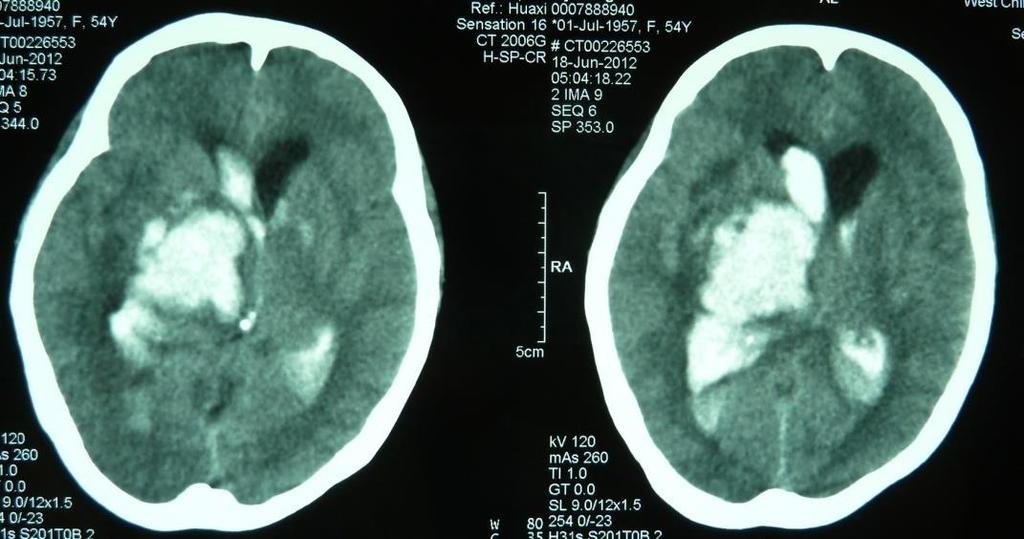
8 thalamic-basilar ganglion hematoma M, 67Y.O., admission for sudden left paralysis and LOC for 3h. Diag: right TBH
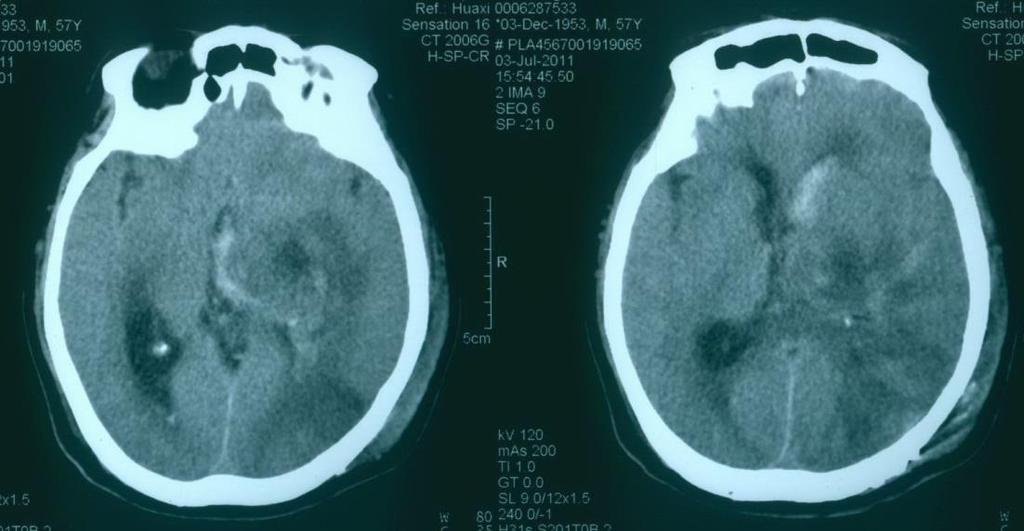
9 M,57Y.O., admission for LOC for 6h. Diag: right TBH

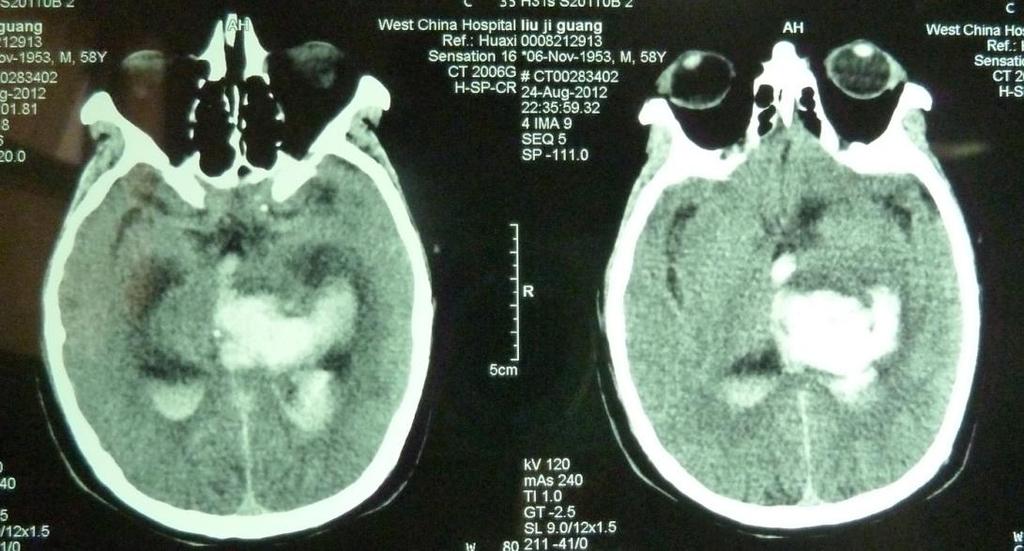
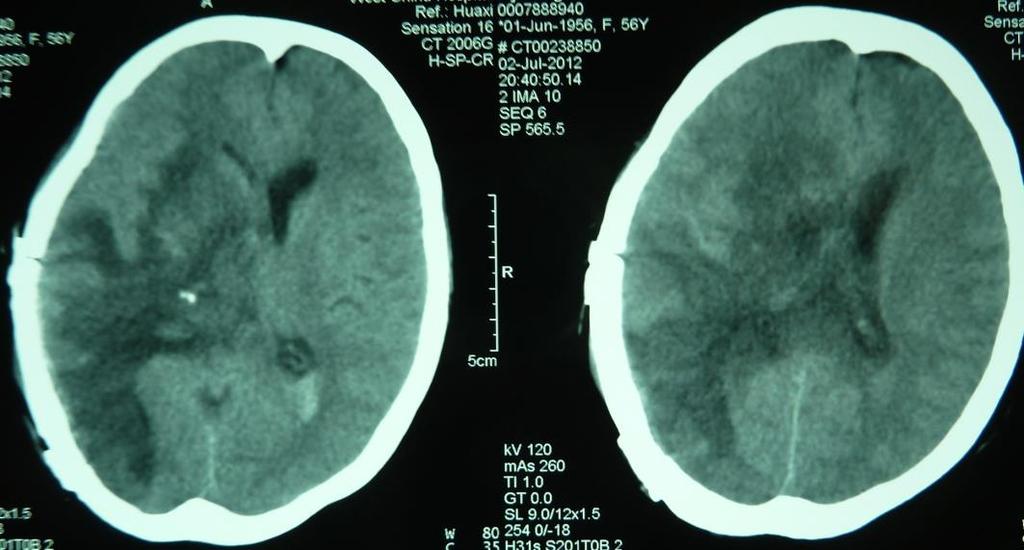
10 thalamic-mesencephalic hematoma M, 60Y.O., admission for seizure and LOC for 3h. Diag: right TMH
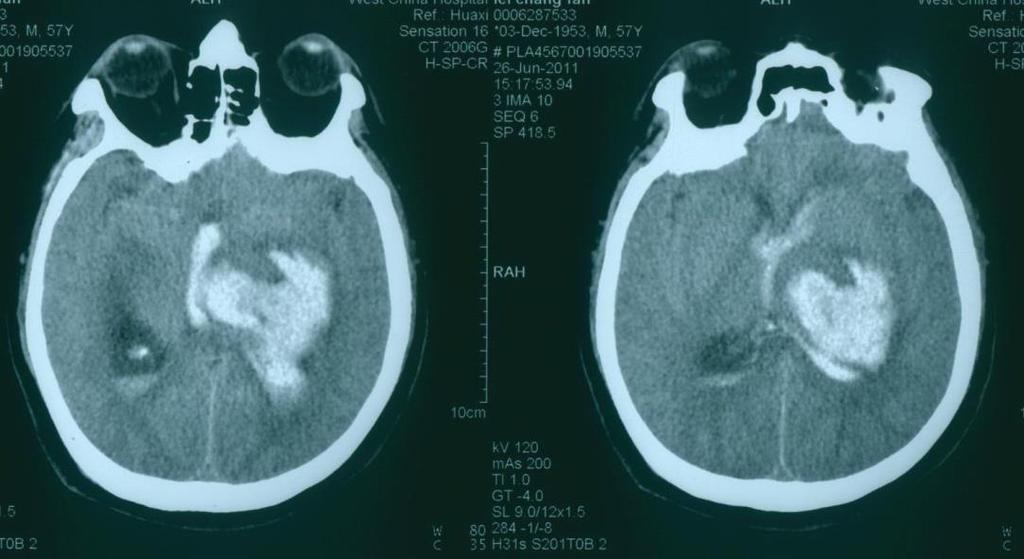
 M, 57Y.O., admission for LOC 6h.")
11 mixed thalamus hematoma (involving three or more than three sites) M, 57Y.O., admission for LOC 6h. Diag: left MTH
12 We retrospectively analyzed the cases of HTH from Jan 2014 to Jan 2017 in our department, compared the conservative and surgical treatment, and discuss the surgical strategy for HTH.
13 Method 160 cases were collected from Jan 2014 to Jan 2017 The diagnosis was consistent with the guidelines for the management of spontaneous intracranial hemorrhage of America. The cases were sent to our department for emergency with a clear hypertensive history. The CT scans confirmed the bleeding originally came from thalamus or thalamic area. All Cases GCS 4 when admitting.
14 87 males and 73 females with the age ranged from 38 to 82 years (mean59.3±1.1years) were collected in our data. There were 115 cases with a systolic pressure more than 180mmHg, 37cases with a systolic pressure more than 200mmHg. The average systolic pressure in our cases was 185±7 mmhg and the average diastolic pressure was 107±5 mmhg.
15 Our cases were categorized into five subtypes according to the bleeding sites and also into giant and moderate group according to the size of the hematoma. LTH TVH TBH TMH MTH size 30ml 30ml
16 Results There were 89 cases in the moderate group (size 30ml,LTH and TVH). The size of hematoma ranged from 30 to 5ml (mean12.5±1.8ml) in moderate group. There were also 27cases (30.0%) with the ventricular hematoma and 22 cases with obstructive hydrocephalus in moderate group. On the contrary, the giant hematoma group (more than 30ml in size, mainly MTH) had 71 cases. The size of hematoma ranged from 70 to 35ml (mean42.3±3.1ml). There were 59cases(83.1% )with the ventricular hematoma and 35 cases with obstructive hydrocephalus in giant group.
17 61 cases accepted conservative treatment and 24 cases accepted surgery in moderate group. In giant group the data for conservative and surgical treatment were 21 and 53 cases.
18 Moderate (n) Giant (n) Conservative Tr Surgery Total Burr hole Dr. Evacuation n= number of cases
19 The mortality in surgery group(9.4%)was much better than conservative group(61.1%) for giant thalamus hemorrhage. For moderate thalamus hemorrhage the mortality was no difference between conservative and surgery group.
20 1 M.O. mortality after treatment Moderate Giant Conservative Tr. 1.6%(1/61) 61.1%(11/18) Surgery 7.1%(2/28)* 9.4%(5/53)* * p=0.01
21 Discussion HTH: Controversial Surgery or Conservative tr. Enthusiasm for surgical evacuation of thalamic and pontine ICH has been limited. (America ICH guideline) Many Studies: STICH * * No Conclusion *
22 Based on the situation Reviewed observation More RCT Many Difficulties Class I, Level A evidence
23 Diagnostic standard for HTH Typical hypertensive history, BP(S/D) 180/110 mmhg With positive risk factors Typical HTH site and size in CT scan Clinical manifestations: LOC(GCS), Paralysis etc. Excluding other cerebral vascular diseases( Aneurysms, AVM, CM) by DSA, CTA and MRA, hemopathies, tumor apoplexy and toxication.
24 Categorization Moderate group (size 30ml,mainly LTH and TVH). Giant group ( 30ml in size, mainly MTH) LTH TVH TBH TMH MTH size 30ml 30ml
25 LTH,TBH,TMH Management Size 30ml, GCS > Conservative Tr. Size >30ml, GCS < Evacuation TVH,MTH: Size 30ml, GCS >12,no hydrocephalus ---Persistent LPD ( Con Tr.) Size 30ml, GCS < 12,hydrocephalus --- Burr hole drainage Size 30ml, GCS < 8,mostly cast of ventricle --- Evacuation Size>30ml, GCS < Evacuation or Con tr. (old, passive or scattered) Size >30ml, GCS =3, no breath, bilateral light reflex disappear---con Tr.
26 Operative nuances The size of the hematoma for HTH is relatively a less important factor than the Elevated ICP and mass effect when the choice of surgery or medication will be done. Gentle and careful! Intracavity manipulation. Evacuating but protecting the contusive and edematous brain tissue surrounding the hematoma.
27 Operative nuances Using Microscope! Minimally invasion. Combined with navigation, electrophysiological monitoring, and endoscope if possible. Find out the main responsible bleeding artery during the surgery if possible. Less using bipolar in thalamic area and avoiding heat injury.
28 Peri-operative administration BP control Infection prevention Temperature control Balance of serum electrolytes Nutrition support Rebleeding and embolization prevention Other complications
29 Cases presentation


30 LTH admission 10d after tr. M, 90Y.O., admission for sudden left limb numbness for 6h. No LOC, Diag: R LTH. Cons tr. And recovered well.


31 TVH- Persi st ent LPD admission 8d after dr. M, 65Y.O., admission GCS:10, CT revealed a TVH. After 8days persistent LPD, hematoma was absorbed.


32 TVH Burr hol e drai nage F, 46Y.O., CT showed a left TVH. After 7days burr hole dr., the hematoma almost disappeared.


33 TVH Cast of ventricle F, 73Y.O., admission for sudden LOC for 3h. LTVH cast. Evacuating the hematoma by trans-parietal sulcus approach.


34 Patient recovered 5 days after surgery


35 TVH Evacuation



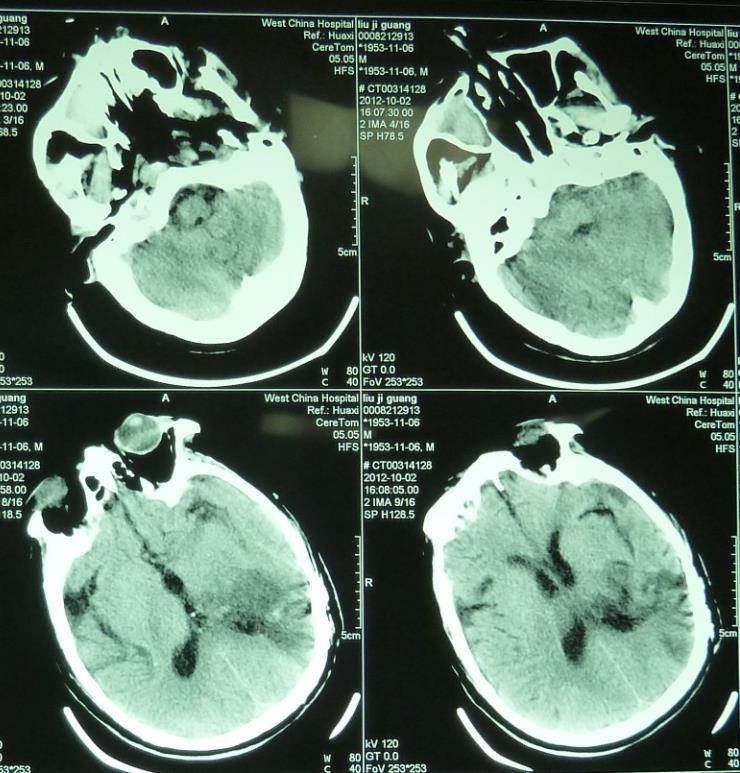
36 TBH Evacuation M, 62Y.O., admission for left limb paralysis and LOC for 8h. Diag: R TBH

37 MTH die M, 74Y.O, admission for LOC for 4h. Diag: R MTH The family refused surgery and the patient died after a 3days cons. tr.



38 MTH Burr hole drainage F, 50Y.O., admission for sudden headache and followed LOC for 7h. Diag: L MTH. Recovered after a 10 days burr hole dr.


39 MTH Evacuation
40 MTH Evacuation before after
41 MTH Evacuation before after
42 MTH Evacuation before after
43 Our limitations Retrospective analysis No long term follow-up( 2 y) and survival analysis Lots of lost to follow-up No morbidity analysis Only reviewed observation Multi-center RCT is in process now
44 Conclusion Surgery decreases the mortality and might be a very effective treatment for the giant hypertensive thalamus hematoma. At least, It gives the hope to the severe HTH patients.
45 Thanks for attention!
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage
 Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Louisiana State University Health Sciences Center
 Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Keyhole craniectomy in the surgical management of spontaneous intracerebral hematoma
 Neurology Asia 2007; 12 : 21 27 Keyhole craniectomy in the surgical management of spontaneous intracerebral hematoma S Balaji Pai, RG Varma, JKBC Parthiban, KN Krishna, RM Varma, *R Srinivasa,*PT Acharya,*BP
Neurology Asia 2007; 12 : 21 27 Keyhole craniectomy in the surgical management of spontaneous intracerebral hematoma S Balaji Pai, RG Varma, JKBC Parthiban, KN Krishna, RM Varma, *R Srinivasa,*PT Acharya,*BP
Brain Arteriovenous Malformations Endovascular Therapy and Associated Therapeutic Protocols Jorge Guedes Cabral de Campos
 Endovascular Therapy and Associated Therapeutic Protocols Jorge Guedes Cabral de Campos Neuroradiology Department Hospital de Santa Maria University of Lisbon CEREBRAL AVM CLINICAL / EPIDEMIOLOGY Brain
Endovascular Therapy and Associated Therapeutic Protocols Jorge Guedes Cabral de Campos Neuroradiology Department Hospital de Santa Maria University of Lisbon CEREBRAL AVM CLINICAL / EPIDEMIOLOGY Brain
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Original Article Remote cerebellar hemorrhage after microsurgical clipping of intracranial aneurysms: diagnosis and treatment a review of 13 cases
 Int J Clin Exp Med 2016;9(2):3681-3686 www.ijcem.com /ISSN:1940-5901/IJCEM0012155 Original Article Remote cerebellar hemorrhage after microsurgical clipping of intracranial aneurysms: diagnosis and treatment
Int J Clin Exp Med 2016;9(2):3681-3686 www.ijcem.com /ISSN:1940-5901/IJCEM0012155 Original Article Remote cerebellar hemorrhage after microsurgical clipping of intracranial aneurysms: diagnosis and treatment
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Supratentorial cerebral arteriovenous malformations : a clinical analysis
 Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Microsurgery for ruptured cerebellar arteriovenous malformations
 European Review for Medical and Pharmacological Sciences Microsurgery for ruptured cerebellar arteriovenous malformations S.-F. GONG 1,2, X.-B. WANG 1,3, Y.-Q. LIAO 1,2, T.-P. JIANG 1,2, J.-B. HE 1,2,
European Review for Medical and Pharmacological Sciences Microsurgery for ruptured cerebellar arteriovenous malformations S.-F. GONG 1,2, X.-B. WANG 1,3, Y.-Q. LIAO 1,2, T.-P. JIANG 1,2, J.-B. HE 1,2,
Treatment of Unruptured Vertebral Artery Dissecting Aneurysms
 33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
Explaining All of the Options for AVM: Cerebral Arteriovenous Malformation
 Explaining All of the Options for AVM: Cerebral Arteriovenous Malformation Recorded on: November 19, 2012 Bernard Bendok, M.D. Director of the Neurointerventional Program Northwestern Memorial Hospital
Explaining All of the Options for AVM: Cerebral Arteriovenous Malformation Recorded on: November 19, 2012 Bernard Bendok, M.D. Director of the Neurointerventional Program Northwestern Memorial Hospital
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs)
") Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
Life after ARUBA: Management of Unruptured Brain Arteriovenous Malformations (AVMs) Eric L. Zager, MD University of Pennsylvania Department of Neurosurgery No Disclosures Brain AVMs Incidence ~1 in 100,000
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma
 Original Contribution Kitasato Med J 2017; 47: 141-147 Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma Hiroyuki Koizumi, 1,2 Daisuke Yamamoto, 1 Yasushi Asari,
Original Contribution Kitasato Med J 2017; 47: 141-147 Efficacy of neuroendoscopic evacuation of traumatic intracerebral or intracerebellar hematoma Hiroyuki Koizumi, 1,2 Daisuke Yamamoto, 1 Yasushi Asari,
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA?
 INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
Treatment of Acute Hydrocephalus After Subarachnoid Hemorrhage With Serial Lumbar Puncture
 19 Treatment of Acute After Subarachnoid Hemorrhage With Serial Lumbar Puncture Djo Hasan, MD; Kenneth W. Lindsay, PhD, FRCS; and Marinus Vermeulen, MD Downloaded from http://ahajournals.org by on vember,
19 Treatment of Acute After Subarachnoid Hemorrhage With Serial Lumbar Puncture Djo Hasan, MD; Kenneth W. Lindsay, PhD, FRCS; and Marinus Vermeulen, MD Downloaded from http://ahajournals.org by on vember,
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score
 Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
EPISTAXIS. Nasal Trauma, and other emergencies. Marc A. Tewfik MDCM, MSc, FRCSC
 EPISTAXIS Nasal Trauma, and other emergencies Marc A. Tewfik MDCM, MSc, FRCSC Assistant Professor, McGill University Otolaryngology-Head & Neck Surgery DISCLOSURES Speaker/Consultant Merck Novartis MEDA
EPISTAXIS Nasal Trauma, and other emergencies Marc A. Tewfik MDCM, MSc, FRCSC Assistant Professor, McGill University Otolaryngology-Head & Neck Surgery DISCLOSURES Speaker/Consultant Merck Novartis MEDA
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Overview. Introduction. New Interventions for Acute Stroke. New Approaches to hemorrhagic Strokes
 Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT. G. Tamburrini, Rome
 INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT G. Tamburrini, Rome Incidence 2% of occasional neuroradiological findings From clinical studies (1960 s): 0.4-1% of intracranial space occupying
INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT G. Tamburrini, Rome Incidence 2% of occasional neuroradiological findings From clinical studies (1960 s): 0.4-1% of intracranial space occupying
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY
 Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Stereotactic Burr Hole Aspiration Surgery for Spontaneous Hypertensive Cerebellar Hemorrhage
 Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2012.14.3.170 Original Article Stereotactic Burr Hole Aspiration Surgery for Spontaneous
Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2012.14.3.170 Original Article Stereotactic Burr Hole Aspiration Surgery for Spontaneous
Overview of imaging modalities for cerebral aneurysms
 Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
MRI OF THE THALAMUS. Mohammed J. Zafar, MD, FAAN Kalamazoo, MI
 1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing