A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
|
|
|
- Adelia Harrell
- 5 years ago
- Views:
Transcription




1 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015

2 Outline Neuroanatomy and physiology (85 slides ) Raised ICP considerations Intracranial haemorrhage Shunt complications Headache- when to worry

3 Raised Intracranial Pressure Do not forget metabolic reasons/encephalopathies

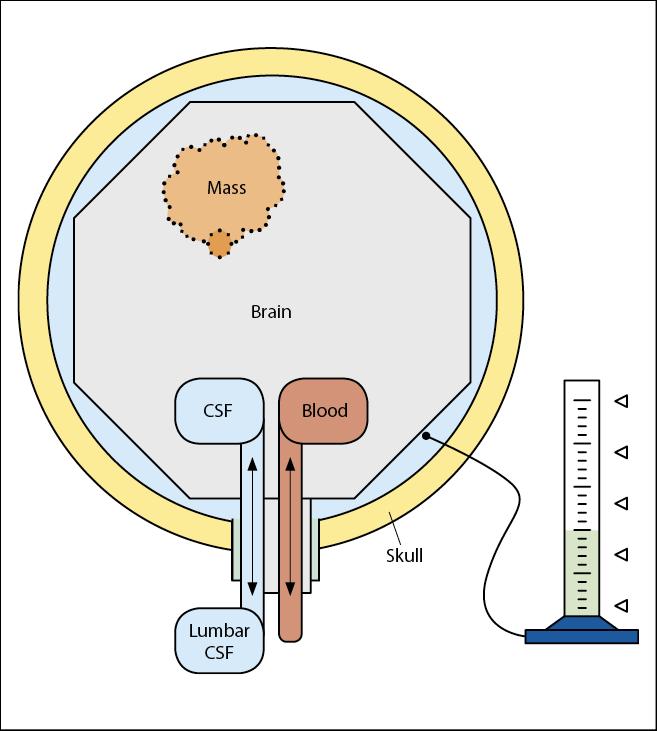
4 Raised ICP in a nutshell Elevated ICP is defined as intracranial pressure 20 mm Hg for >5 minutes. This impairs arterial blood flow, producing ischemia Cerebral Perfusion Pressure = MAP ICP Keep CPP > 60, ICP < 20

5 Clinical signs Headache Nausea/Vomiting Visual disturbances Focal signs Behavioural changes
6 Autoregulation Right shift in hypertensive individuals

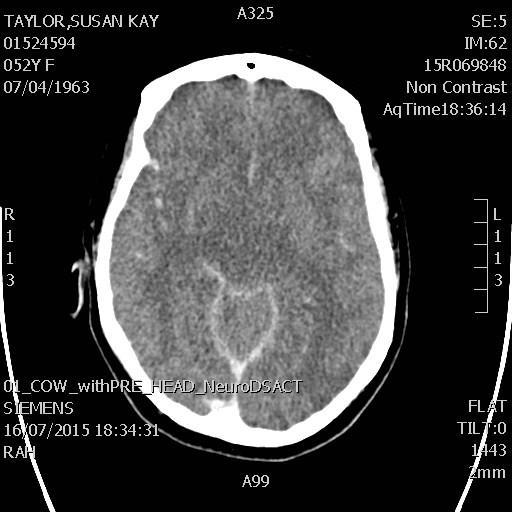
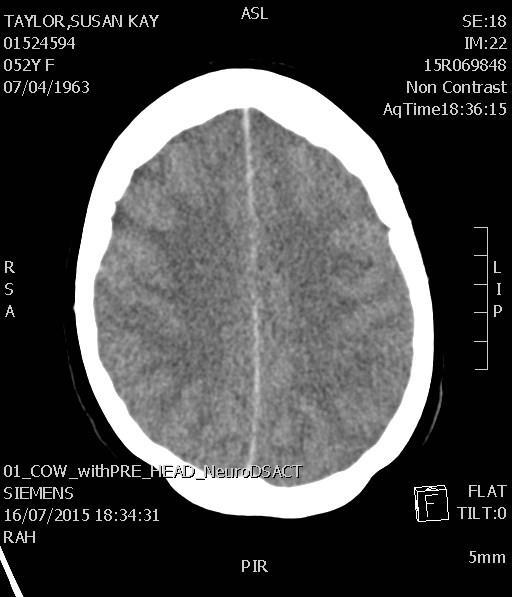

7 Raised ICP on CT Normal
 Trauma: Cervical collars not too tight Hypertonic")
8 Basic and not so basic measures Prevent Hypoxia Elevation of head and trunk Normocapnoea, Normothermia Keep neck straight Avoid jugular vein compression ( ETT tie) Trauma: Cervical collars not too tight Hypertonic saline

9 Intubation, Ventilation, Sedation Reduce coughing, pain response, enables ventilation Reduces fluctuations in ICP Decreases cerebral metabolic rate can cause drop in MAP impairing CPP necessitating vasopressors
 of large bore peripheral cannula over 10 minutes")
10 Osmodiuretics 7.5% Saline 4 ml / kg (to a maximum of 250ml) of large bore peripheral cannula over 10 minutes Mannitol 20% 1.5-2g/kg (ph 6.3) over 30 min If signs of actual or impending herniation


11 Surgical options Mass removal Ventricular drainage Craniectomy (Biopsy)

12 Steroids and monitoring Steroids: oedema around tumours and abscess- NOT in haemorrhage/traumatic brain injury Intracerebral monitoring
13 Summary: Raised ICP Just about any intracerebral and many systemic pathologies can cause raised ICP Much can be done to optimize condition in ED Simple measures go a long way

14 Intracerebral haemorrhage Approximately per 100,000/year 350 hypertensive haemorrhages per 100,000 elderly individuals/year 19 y old post amphetamines
15 Mortality

16 J Neurol Neurosurg Psychiatry 2005;76: % are independent six months after intracerebral bleeding
17 Clinical signs The younger, the more dramatic the onset Alteration in level of consciousness (approximately 50%) Nausea and vomiting (approximately 40-50%) Headache (approximately 40%) Seizures (approximately 6-7%) Focal neurological deficits

18 Causes Hypertension Arteriovenous malformation Aneurysmal rupture Cerebral amyloid angiopathy Intracranial neoplasm Coagulopathy Haemorrhagic transformation of an ischemic infarct Cerebral venous thrombosis Sympathomimetic drug abuse Moyamoya Sickle cell disease Eclampsia or postpartum vasculopathy Infection Vasculitis
 guidelines for the management of spontaneous intracerebral hemorrhage 2014 SA Stroke Network Protocols and Procedures November")
19 Emergency Management ABC AHA Scientific Statement Guidelines for the Management of Spontaneous Intracerebral Hemorrhage 2010 European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage 2014 SA Stroke Network Protocols and Procedures November 2014
20 For all of us who struggle to find CTs, ICU beds or anyone who cares. Initial monitoring and management of ICH patients should take place in an intensive care unit with physician and nursing neuroscience intensive care expertise Rapid neuroimaging with CT or MRI is recommended to distinguish ischemic stroke from ICH

21 Imaging as soon as possible Code stroke approach!
: (The Lancet August 2013): early surgery does not increase the rate of death or disability at 6 months Infratentorial: Unclear how,")
22 Surgery Supratentorial: no evidence to support surgical intervention on a routine may be of value for patients with a GCS score Early surgery versus initial conservative treatment (STICH II): (The Lancet August 2013): early surgery does not increase the rate of death or disability at 6 months Infratentorial: Unclear how, when, and for whom surgical evacuation should be performed in adults with infratentorial ICH. Minimally Invasive Surgery: Work in progress


23 External Ventricular Drains No RCTs, about how, when, and for whom to place an EVD in Outcome of patients with intraventricular haemorrhage worse


24 Admitted with Labyrinthitis asleep GCS 6
25 Blood pressure management in ICHsuggestions, but check local protocols In acute ICH within 6 h of onset intensive blood pressure reduction (systolic target <140 mmhg in <1 h) is safe and may be superior to a systolic target <180 mmhg. No specific agent can be recommended. (Rapid Blood-Pressure Lowering in Patients with Acute Intracerebral Hemorrhage NEJM 2013: over 2800 patients (INTERACT 2)
 trial: ATACH II currently recruiting Eg Labetalol, Esmolol, SNIP, (Nicardipine, Enalapril) Local")
26 Blood pressure management in ICH: check local protocols Antihypertensive Treatment in Acute Cerebral Hemorrhage (ATACH) trial: ATACH II currently recruiting Eg Labetalol, Esmolol, SNIP, (Nicardipine, Enalapril) Local protocols/guidelines

27 Summary: ICH Anyone with stroke symptoms could have a bleed Early imaging Management of blood pressure Still poor prognosis with high mortality and morbidity No straight forward surgical pathways

28 VA and VP shunts Obstruction Disconnection Infection
 Brain tumour (benign or malignant) Spina")

29 Indications for ventriculoperitoneal Shunts Hydrocephalus (congenital/acquired) Brain tumour (benign or malignant) Spina bifida Congenital aqueductal stenosis Craniosynostosis Dandy-Walker syndrome Arachnoid cyst Idiopathic intracranial hypertension
30 Shunt obstruction 50% of all shunt failures due to obstruction. ventricular catheter blockage is by far the most common Symptoms are generally the same, raised ICP clinical picture influenced by the aetiology of the hydrocephalus and the patient's age.

31 Shunt obstruction Children with myelomeningocele have greatest variability of clinical manifestations, 9-29% of possibilities of underestimating a shunt malfunction only on clinical grounds One third of patients with shunt malfunction may have "normal" imaging data

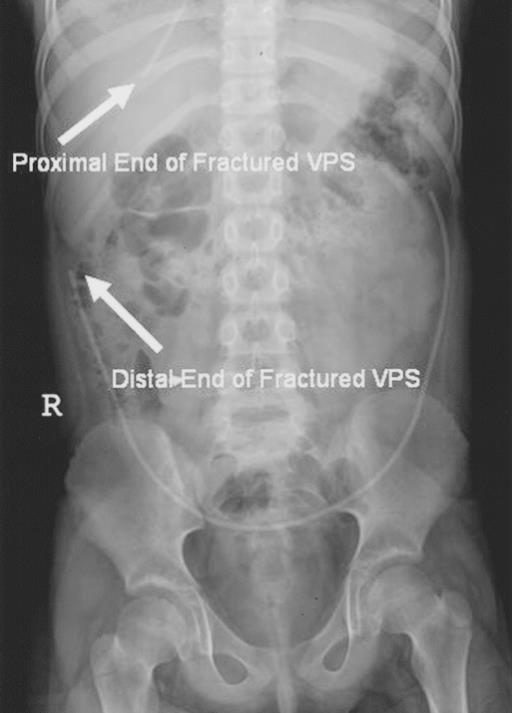
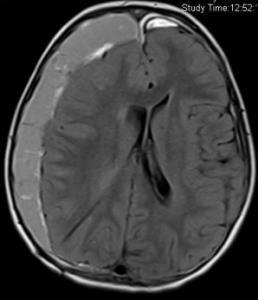

32 Imaging Occasional cause of neurological deterioration with shunt
33 Common Pathogens Associated With Ventriculoperitoneal Shunt Infections Early Infection (85%) (Within Weeks of Shunt Placement or Revision) Coagulase-negative Staphylococci (ie, S. epidermidis ) 50% Staphylococcus aureus 33% Late Infection (15%) (Several Months After) Stenotrophomonas Serratia marcescens Candida albicans Pseudomonas aeruginosa

34 Diagnosis High index of suspicion Trust the patient, parents and carers Initially no specific neurological signs or signs of raised ICP Cerebrospinal fluid for analysis Imaging




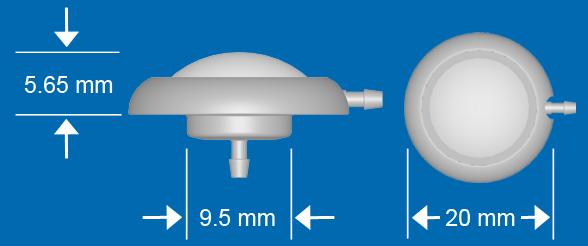
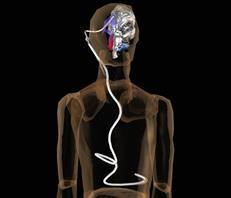
35 VP shunt tap



36 Treatment Often includes shunt revision Intraventricular vancomycin Systemic antibiotics
37 Summary: Shunts Patients with shunts often have comorbidities that make diagnosis complex Imaging not always reliable High index of suspicion Expert advice
 comes in complaining about a")
38 And now to a crowd favourite am. A 49-year-old woman (could be me ) comes in complaining about a terrible headache following an argument
39 .. continued developed over approximately 15 minutes much better since she took two oxycodone tablets mild photophobia without any focal neurological signs minimal neck pain (gardening yesterday)
40 . but wait there is more The headache is almost like her typical migraine. Neurologically normal CT? LP? Oral/IM /IV pain meds Discharge? Or should I hand her over to the morning shift..

41 Headaches in ED 4.5% of presentations Overwhelmingly benign headache syndromes (tension, migraine, cluster etc)
42 Characteristics of headache with serious underlying pathology History Explosive onset and severe at onset No similar headaches in the past (2 edged sword) Concomitant infection Altered mental status Headache with exertion Illicit dugs- particularly amphetamines and cocaine Family history Age over 50 Immunosuppression
43 Characteristics of headache with serious underlying pathology Physical examination Neurologic abnormalities Decreased level of consciousness Meningismus Toxic appearance Papilledema


44 What is a sudden headache? Severe persistent headache Reaches maximal intensity within seconds or only a few minutes Always warrants investigation If CT negative- LP

45 LOW-RISK PATIENTS prior headaches without substantial change to normal who present to the emergency department due to failure of their standard therapy regimen
46
47
48
49 Summary: Headaches Systematic approach Risk stratify Every patient warrants thorough assessment- patients with migraines get SAH If sudden headache- negative CT warrants LP


50
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Hemorrhagic Stroke. Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
 Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Louisiana State University Health Sciences Center
 Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Index. C Capillary telangiectasia, intracerebral hemorrhage in, 295 Carbon monoxide, formation of, in intracerebral hemorrhage, edema due to,
 Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Update in Management of Acute Spontaneous Intracerebral Haemorrhage
 Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC
 Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Pediatric Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Pediatric Neurosurgery Pediatric neurosurgeons
Introduction to Neurosurgical Subspecialties: Pediatric Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Pediatric Neurosurgery Pediatric neurosurgeons
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
The three main subtypes of stroke
 Neurology 55 Spontaneous intracerebral haemorrhage in the elderly Spontaneous Intracerebral Haemorrhage (ICH) is defined as bleeding into the brain parenchyma without accompanying trauma. This condition
Neurology 55 Spontaneous intracerebral haemorrhage in the elderly Spontaneous Intracerebral Haemorrhage (ICH) is defined as bleeding into the brain parenchyma without accompanying trauma. This condition
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts
 Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts Exceptional healthcare, personally delivered Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts What is hydrocephalus? Hydrocephalus is the build up of an excess
Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts Exceptional healthcare, personally delivered Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts What is hydrocephalus? Hydrocephalus is the build up of an excess
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
Supratentorial cerebral arteriovenous malformations : a clinical analysis
 Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
AHA/ASA Guideline. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults
 AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults 2007 Update A Guideline From the American Heart Association/American Stroke Association Stroke Council,
AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults 2007 Update A Guideline From the American Heart Association/American Stroke Association Stroke Council,
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
INTRACEREBRAL HAEMORRHAGE:
 INTRACEREBRAL HAEMORRHAGE: WHAT IS THE CAUSE? Prof. Charlotte Cordonnier Head, Department of neurology & stroke centre Director, Lille haemorrhagic stroke research program Lille University Hospital France
INTRACEREBRAL HAEMORRHAGE: WHAT IS THE CAUSE? Prof. Charlotte Cordonnier Head, Department of neurology & stroke centre Director, Lille haemorrhagic stroke research program Lille University Hospital France
Complex Hydrocephalus
 2012 Hydrocephalus Association Conference Washington, DC - June 27-July1, 2012 Complex Hydrocephalus Marion L. Walker, MD Professor of Neurosurgery & Pediatrics Primary Children s Medical Center University
2012 Hydrocephalus Association Conference Washington, DC - June 27-July1, 2012 Complex Hydrocephalus Marion L. Walker, MD Professor of Neurosurgery & Pediatrics Primary Children s Medical Center University
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Children with Hypertension in ED
 Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
HHS Public Access Author manuscript Am J Emerg Med. Author manuscript; available in PMC 2016 April 01.
 The excess cost of inter-island transfer of intracerebral hemorrhage patients Kazuma Nakagawa, MD 1,2, Alexandra Galati, BA 2, and Deborah Taira Juarez, ScD 3 1 Neuroscience Institute, The Queen s Medical
The excess cost of inter-island transfer of intracerebral hemorrhage patients Kazuma Nakagawa, MD 1,2, Alexandra Galati, BA 2, and Deborah Taira Juarez, ScD 3 1 Neuroscience Institute, The Queen s Medical
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
PA SYLLABUS. Syllabus for students of the FACULTY OF MEDICINE No.2
 Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions
 https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60