Dissection and Stroke
|
|
|
- Elvin Roberts
- 5 years ago
- Views:
Transcription
1 Dissection and Stroke CoxHealth Stroke Conference 2017 Thoracic Aorta Stroke 2017 Supra-aortic Trunks Carotid Artery Vertebral Artery 1

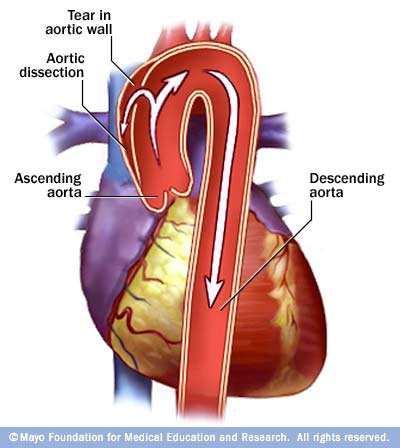
2 The development of a tear of the inner lining of the artery -the intima-- extending into the media What is a Dissection? This tear may extend distally, disrupting branches or ultimately leading to aneurysm formation Thrombus formation and embolization is a potential outcome 2


3 3


4 4


5 5
6 Dissection of the Ascending Aorta Incidence: At least 30 per million per year Most common manifestation of acute aortic syndrome Mortality of 1% per hour First repair DeBakey, Cooley and Creech 1954 WHO? Male Age: 60s and 70s Hypertension Prior cardiac surgery (aortic valve repair) Bicuspid aortic valve Atherosclerosis of aorta 6
7 Less than 10%: --younger than age 40 WHO? --normotensive --history of cardiac surgery or bicuspid aortic valve Marfan syndrome, Ehlers-Danlos syndrome, etc Ascending Dissection: Presentation Gaul C, Dietrich W, Friedrich I et al. Neurological symptoms in type A aortic dissection. Stroke 2007;38: Dept of Neurology, Nuremburg 7
8 Gaul et al, STROKE Background and Purpose Aortic dissection typically presents with severe chest or back pain. Neurological symptoms may occur because of occlusion of supplying vessels or general hypotension. Especially in pain-free dissections diagnosis can be difficult and delayed. Methods Clinical records of 102 consecutive patients with aortic dissection (63% male, median age 58 years) analyzed for medical history, preoperative clinical characteristics, treatment and outcome with emphasis on neurological symptoms. Results Thirty patients showed initial neurological symptoms (29%). Only two-thirds of them reported chest pain Neurological symptoms were attributable to ischemic stroke (16%), spinal cord ischemia (1%), ischemic neuropathy (11%), and hypoxic encephalopathy (2%). In aortic dissections, neurological symptoms are often dramatic and may dominate the clinical picture and mask the underlying condition. The frequency of neurological involvement varies from 17% to 40%. Many neurological findings have supposedly been overlooked because of incompleteness of neurological examination in critically ill patients. Remarkably, pain is not an obligatory symptom of aortic dissection. 13.9% of patients noted no pain, matching reported ranges of pain-free dissections between 5% and 15%. Approximately half of patients who did not report pain solely showed neurological symptoms. 8

9 Neuro symptoms in 29% of patients Presentation:? Chest Pain? --ischemic stroke 16% --ischemic neuropathy 11% --hypoxic encephalopathy 2% --spinal cord ischemia 1% 9


10 10
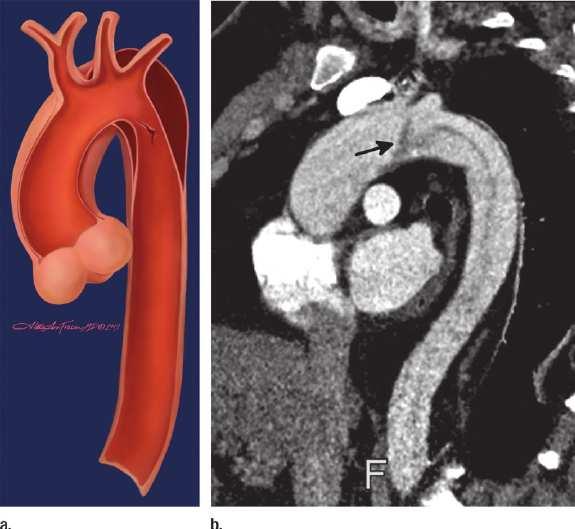
11 Isolated dissecting aneurysm of the brachiocephalic artery associated with contained rupture Tomoaki Hirose, MD et al Gen Thorac Cardiovasc Surg (2012) 60: Brachiocephalic Dissection A 79-year-old man with no history of trauma with sudden onset of headache and backache. CT showed an isolated dissection associated with contained rupture of the brachiocephalic artery. The proximal aortic arch was successfully replaced using antegrade selective cerebral perfusion. The patient recovered uneventfully. Brachiocephalic Artery Dissection BMJ Case Rep. 2015; 2015: bcr Published online 2015 Aug /bcr Isolated brachiocephalic artery dissection presenting as acute stroke Hariharasudan Mani and Sharat Ahluwalia 11
12 A 41-year-old obese man with undiagnosed hypertension Presented with ataxia, slurred speech and left facial weakness Onset: acute, but the day before Brachiocephalic Dissection Sought medical help the next morning for persistence of symptoms Non smoker, no other medical history or trauma Family history: grandparents had strokes in their 60s, cause unknown. No family history of coagulopathy, aortic dissection or connective tissue disorders Brachicephalic Dissection: Exam BP 190/119 mm Hg LEFT, 170/110 mmhg RIGHT Left facial asymmetry, upper motor facial palsy Minimal dysarthria No extremity motor or sensory deficits No cerebellar signs On standing, tendency to drift left 12

13 Brachiocephalic Dissection: Imaging CT: acute ischemic infarct of the right basal ganglia. Brachiocephalic Dissection: Imaging 13

14 Other work-up: hypercoagulopathy lab and echo are normal Now What? Treated with heparin anticoagulation, bridged to Coumadin Long Term: Minimal residual dysarthria and facial asymmetry Aortic dissection most commonly presents with tearing chest pain, but 14% of patients discussed here had no pain and only neurologic symptoms Supra Aortic Trunk Dissection may present with minimal or misleading symptoms (headache, backache, ataxia, dysarthria) Subsequent ischemic stroke is believed to be due to thromboembolism Antithrombotic therapy, with either full anticoagulation or antiplatelet agents, is the treatment of choice Anticoagulation may prevent occlusion of a stenotic vessel and minimise distal embolisation. 14
15 Cervical Artery Dissection Carotid Vertebral Arch Neurosci Oct; 2(4): e Published online 2015 Oct 17. doi: /archneurosci Cervical Artery Dissection: A Review of the Epidemiology, Pathophysiology, Treatment, and Outcome Christina A. Blum 1 and Shadi Yaghi 2 Cervical Artery Dissection Cervical artery dissection is a common cause of stroke in young adults, with a prevalence of up to 20% in this population and an annual incidence rate of 2.6 to 2.9 per 100,000 1, 2. The true incidence is likely higher because many cases with dissection may go undiagnosed due to minor self-limited clinical symptoms. In population-based studies, the mean age of occurrence is approximately 45 years and there appears to be a slight gender predisposition favoring males (53-57%) 3, 4. Furthermore, there seems to be seasonal variation, with dissection more likely to occur in the winter 5. Cervical artery dissection is classified based on the artery involved (vertebral vs. carotid) and the location of involvement (intracranial vs. extracranial). The most common type is extracranial internal carotid dissection which typically occurs 2-3 cm above the bifurcation and accounts for up to 2.5% of all first strokes. 6 15

16 Heritable connective-tissue disorders Ehlers-Danlos syndrome type IV Fibromuscular dysplasia Cystic medial necrosis Marfan syndrome Autosomal dominant polycystic kidney disease Osteogenesis imperfecta type I Oral contraceptives Hypertension Neck manipulation or strain - This can result from intentional manipulation or from other strain that may occur during sports activities, yoga, or even apparently minimal activity (eg, overhead painting) Blunt trauma from high impact and seemingly minor mechanisms of injury Penetrating trauma Wearing a three-point restraint seat belt during a motor vehicle crash Smoking Respiratory tract infection (related to seasonal distribution?) 16

17 The clinical manifestations of dissections depend on the artery involved. Carotid artery dissections typically begin with ipsilateral neck pain or headache and a partial Horner's followed by retinal or cerebral ischemia. The presence of any two of the three elements in the triad strongly suggests the diagnosis of carotid dissection 20. The headache caused by dissection has no specific features and can resemble migraine or cluster headaches. 16 Common headache characteristics include sudden onset, unilateral, constant, and throbbing. Other headache characteristics including a thunderclap headache can also be seen. The Horner is usually partial (miosis and ptosis without anhidrosis) due to the fact that sudomotor fibers of the face travel along the external carotid artery. Focal neurological symptoms as a result of cerebral or retinal ischemia may be transient or persistent and are variable. Conversely, vertebral artery dissections typically present with occipito-cervical pain, which may be followed by a variety of posterior circulation ischemic symptoms including vertigo, dysarthria, visual field deficit, ataxia, and diplopia. Although strokes from vertebral artery dissection most frequently involve the lateral medulla and cerebellum, spinal cord infarction may occur when extracranial branches are affected. When intracranial carotid or vertebral dissections are complicated by pseudoaneurysm formation, local symptoms due to compression of adjacent structures can occur. For example, cranial nerves XII, IX and X are closest in proximity to the carotid artery and are those most commonly involved in carotid artery dissection. Furthermore, rupture of a pseudoaneurysm can cause subarachnoid hemorrhage presenting with an acute thunderclap headache and carrying a relatively high mortality and morbidity

18 Diagnosis Cervical artery dissection is suspected clinically and confirmed by neuroimaging techniques including magnetic resonance imaging (MRI), computerized tomographic angiography (CT), and conventional angiography. The sensitivity and specificity of each test varies based on the location and extent of the dissection. The preferred method of diagnosis is magnetic resonance angiography (MRA) along with a T1 axial cervical MRI with fat saturation technique due its lack of radiation, high sensitivity and specificity, and ability to visualize an intramural hematoma (Figure 1). 22 CTA also has high sensitivity and specificity and may also be used but is associated with radiation exposure and potential technical challenges. 23, 24 In patients with CAD, a CTA can show the double lumen sign (true and false lumen) (Figure 1) or a flame-like taper of the lumen. Carotid ultrasound with color doppler is another screening test that can be used. 22 Although it is non-invasive, this technique is operator dependent and is of poor diagnostic value in patients with intracranial carotid dissection and those with vertebral dissections. Although ultrasound has been shown to have high sensitivity in patients with extracranial carotid dissection and ischemic symptoms 25, in patients with headache and isolated Horner this technique is poor. 26 A possible explanation is that in patients with local symptoms only, the dissection rarely causes luminal narrowing and thus may be missed on color doppler. 27 Catheter angiogram should not be routinely used to diagnose dissection for several reasons, including inability to visualize intramural hematomas and being an invasive test that may potentially cause an iatrogenic dissection, especially in a patient population with underlying vessel wall weakness. 18

19 Pathophysiology of stroke due to CAD Although the exact mechanism of stroke in patients with CAD is unclear, the most likely mechanism is artery-to-artery embolism of a thrombus or fragments of a thrombus that form in the false lumen. This has been demonstrated by brain imaging showing embolic appearing infarcts in most patients with dissection who suffered from strokes 34. Other possible mechanisms include hypo-perfusion causing watershed infarctions if there is severe vessel narrowing, occlusion of the dissected vessel, or, less commonly the intimal flap occluding the ostium of a branch of the dissected vessel. In one study that included 172 patients with CAD out of which 58% had evidence of an acute stroke on diffusion weighted MRI, the mechanism of stroke was found to be thromboembolic in 85% of cases, secondary to hemodynamic failure in 12%, and due to a mixed mechanism in 3% of cases 35. In another study, the presence of luminal narrowing was not associated with stroke occurrence; however patients with occlusive dissection had larger infarcts than those with non-occlusive dissections
20 Natural history of CAD Patients with CAD tend to have a good prognosis. The main predictor of poor outcome is cerebral infarction, which occurs in about 70% of patients with CAD 2, however this is based on data available from stroke centers and thus is subject to referral bias. Strokes related to CAD typically occur in the first 2 weeks after the dissection 37, 38 and the risk of stroke falls dramatically beyond that time point, resembling what is seen with symptomatic carotid stenosis. In population-based cohorts, the risk of recurrent stroke from CAD is less than 3% 37, 38. In general, patients with CAD have resolution and healing of the blood vessel on follow-up imaging 6 months after diagnosis (Figure 3) 39. Although the dissected vessel usually has complete recanalization, residual stenosis or occlusions may persist 2. Even in those who do not recanalize, the risk of stroke recurrence remains very low. One of the complications of CAD is the development of a pseudo-aneurysm that tends to persist on repeat imaging 40. The risk of rupture is around 1% 3, 4 and typically occurs in intracranial vessels lacking an external elastic lamina, causing subarachnoid hemorrhage with a relatively high mortality rate. Although CAD tends to occur only once, about 7% of patients have recurrent CAD seven years from the diagnosis 41. Patients with dissection who have a stroke tend to have a good longterm outcome with 75% being functionally independent at 3 months 16. Carotid Dissection Can J Neurol Sci May;35(2): Extracranial carotid and vertebral artery dissection: a review. Redekop GJ 1. Author information Abstract Dissection of the extracranial carotid and vertebral arteries is increasingly recognized as a cause of transient ischemic attacks and stroke. The annual incidence of spontaneous carotid artery dissection is 2.5 to 3 per 100,000, while the annual incidence of spontaneousvertebral artery dissection is 1 to 1.5 per 100,000. Traumatic dissection occurs in approximately 1% of all patients with blunt injury mechanisms, and is frequently initially unrecognized. Overall, dissections are estimated to account for only 2% of all ischemic strokes, but they are an important factor in the young, and account for approximately 20% of strokes in patients less than 45 years of age. Arterial dissection can cause ischemic stroke either by thromboemboli forming at the site of injury or as a result of hemodynamic insufficiency due to severe stenosis or occlusion. Available evidence strongly favors embolism as the most common cause. Both anticoagulation and antiplatelet agents have been advocated as treatment methods, but there is limited evidence on which to base these recommendations. A Cochrane review on the topic of antithrombotic drugs for carotid dissection did not identify any randomized trials, and did not find that anticoagulants were superior to antiplatelet agents for the primary outcomes of death and disability. Healing of arterial dissections occurs within three to six months, with resolution of stenosis seen in 90%, and recanalization of occlusions in as many as 50%. Dissecting aneurysms resolve on followup imaging in 5-40%,decrease in size in 15-30%, and remain unchanged in 50-65%. Resolution is more common in vertebral dissections than in carotid dissections. Aneurysm enlargement occurs rarely. The uncommon patient presenting with acute hemodynamic insufficiencyshould be managed with measures to increase cerebral blood flow, and in this setting emergency stent placement to restore cerebral perfusion may be considered, provided that irreversible infarction has not already occurred. 20
21 Lancet Neurol Apr;14(4): doi: /S (15) Epub 2015 Feb 12. Antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): a randomised trial. CADISS trial investigators, Markus HS, Hayter E, Levi C, Feldman A, Venables G, Norris J. Collaborators (78) Erratum in Corrections. [Lancet Neurol. 2015] Abstract BACKGROUND: Extracranial carotid and vertebral artery dissection is an important cause of stroke, especially in young people. In some observational studies it has been associated with a high risk of recurrent stroke. Both antiplatelet drugs and anticoagulant drugs are used to reduce risk of stroke but whether one treatment strategy is more effective than the other is unknown. We compared their efficacy in the Cervical Artery Dissection in Stroke Study (CADISS), with the additional aim of establishing the true risk of recurrent stroke. METHODS: We did this randomised trial at hospitals with specialised stroke or neurology services (39 in the UK and seven in Australia). We included patients with extracranial carotid and vertebral dissection with onset of symptoms within the past 7 days. Patients were randomly assigned (1:1) by an automated telephone randomisation service to receive antiplatelet drugs or anticoagulant drugs (specific treatment decided by the local clinician) for 3 months. Patients and clinicians were not masked to allocation, but investigators assessing endpoints were. The primary endpoint was ipsilateral stroke or death in the intention-to-treat population. The trial was registered with EUDract ( ) and ISRN (CTN ). FINDINGS: We enrolled 250 participants (118 carotid, 132 vertebral). Mean time to randomisation was 3 65 days (SD 1 91). The major presenting symptoms were stroke or transient ischaemic attack (n=224) and local symptoms (headache, neck pain, or Horner's syndrome; n=26). 126 participants were assigned to antiplatelet treatment versus 124 to anticoagulant treatment. Overall, four (2%) of 250 patients had stroke recurrence (all ipsilateral). Stroke or death occurred in three (2%) of 126 patients versus one (1%) of 124 (odds ratio [OR] 0 335, 95% CI ; p=0 63). There were no deaths, but one major bleeding (subarachnoid haemorrhage) in the anticoagulant group. Central review of imaging failed to confirm dissection in 52 patients. Preplanned per-protocol analysis excluding these patients showed stroke or death in three (3%) of 101 patients in the antiplatelet group versus one (1%) of 96 patients in the anticoagulant group (OR 0 346, 95% CI ; p=0 66). INTERPRETATION: We found no difference in efficacy of antiplatelet and anticoagulant drugs at preventing stroke and death in patients with symptomatic carotid and vertebral artery dissection but stroke was rare in both groups, and much rarer than reported in some observational studies. Diagnosis of dissection was not confirmed after review in many cases, suggesting that radiographic criteria are not always correctly applied in routine clinical practice. J Vasc Surg Aug;54(2):370-4; discussion 375. doi: /j.jvs Epub 2011 May 28. Long-term outcomes of internal carotid artery dissection. Rao AS 1, Makaroun MS, Marone LK, Cho JS, Rhee R, Chaer RA. OBJECTIVE: The natural history of acute carotid artery dissection is poorly characterized. The purpose of this study is to report on single institutional long-term outcomes. METHODS: A retrospective review of patients treated for acute spontaneous or posttraumatic carotid artery dissection over a 20-year period from August 1989 to July 2009 was performed. RESULTS: Twenty-nine patients with a mean age of 47 ± 19.6 years were identified with acute carotid dissection. Six (25%) were related to trauma, while 23 (79%) were spontaneous. Neurologic symptoms included contralateral limb weakness (55%), facial pain (35%), and Horner's syndrome (21%). Eight patients (28%) presented with an acute hemispheric stroke. Diagnostic imaging modalities used included computed tomography angiography (52%), magnetic resonance angiography (41%), and conventional angiography (48%). Twenty percent of patients had complete carotid occlusion and 25% had near occlusion. Most dissections (65%) had intracranial extension, and 35% were limited to the extracranial cervical internal carotid. The majority (96%) of patients were treated conservatively with anticoagulation or antiplatelet therapy or both. One patient underwent stenting for persistent symptoms resulting in complete recovery. There were two deaths, one from unrelated traumatic injuries and the other from unknown causes. Long-term follow-up was available for 20 patients: 14 had complete symptom resolution (70%) and five (25%) had partial clinical symptom resolution. Two patients had initial resolution of symptoms, with subsequent recurrence that was successfully managed conservatively. Follow-up imaging revealed luminal patency in 79% of patients with minimal residual stenosis. Two patients developed a small asymptomatic internal carotid aneurysm that did not require treatment. Mean follow-up was days. CONCLUSIONS: Most cervical carotid dissections can safely be conservatively managed, with the majority achieving anatomic and symptomatic resolution, with low rates of recurrence over long-term follow-up. 21


22 22

23 BioMed Research International Volume 2017 (2017), Article ID , 6 pages Review Article: Treatment of Cervical Artery Dissection: Antithrombotics, Thrombolysis, and Endovascular Therapy Jing Peng,1 Zunjing Liu,2 Chunxia Luo,1 Lin Chen,1 Xianhua Hou,1 Li Xiao,1 and Zhenhua Zhou1 1Department of Neurology of Southwest Hospital, Third Military Medical University, No. 30 Gaotanyan Road, Chongqing , China 2Department of Neurology, China-Japan Friendship Hospital, 2 Yinghua Dongjie, Hepingli, Beijing , China 23
24 lysis in CAD from randomized controlled studies. In a recent meta-analysis on patients receiving intravenous thrombolysis and arterial therapies in the Safe Implementation of Thrombolysis in Stroke International Stroke Thrombolysis Register (SITS-ISTR) as of March 2010, 180 cases of CAD patients with acute ischemic stroke (with an average NIHSS score of 16) were investigated, of whom 67% received intravenous thrombolysis therapy and 33% received arterial thrombolysis therapy; the outcome was that the overall incidence of intracranial hemorrhage, the overall mortality rate, and the proportion of patients with a good prognosis were 3.1%, 8.1%, and 41%, respectively. Compared with stroke cases caused by other etiologies in the SITS-ISTR, the CAD patients receiving thrombolysis therapies showed no significant differences in terms of safety and prognosis [27]. Thus, we believe that the treatment of CAD-induced acute ischemic stroke using intravenous rtpawithin 4.5 h of onset is safe. However, we should strive to develop new therapeutic strategies to lower the mortality and disability rates of CAD patients after thrombolytic therapy [25]. Endovascular treatment has been widely used to treat cardiovascular and cerebrovascular diseases [28]. However, randomized controlled studies on the application of endovascular treatment or surgeries for CAD patients have not been reported to date [29, 30], and the efficacy and safety of endovascular therapy or surgical treatment have not been evaluated in CAD patients. Endovascular treatment has been primarily used in CAD patients with failed antithrombotic treatment with contraindications for anticoagulation and a pseudoaneurysm and when stent implantation is the main vascular interventional procedure. Due to the special pathological physiology of cervical artery dissection, the method of endovascular treatment is cervical artery stenting. Endovascular treatment/surgical treatment for CAD should be limited because CAD patients have a lower risk of recurrent ischemic stroke, there is no significant correlation with CAD-induced vascular stenosis and pseudoaneurysm, and endovascular/surgical treatments are traumatic. With the development of vascular interventional procedures, the application of endovascular treatment in CAD patients may be underestimated; furthermore, it was previously believed that the dissection leads to clinical events mainly through thromboembolism rather than hypoperfusion; thus, antithrombotic therapy has been the preferred treatment for CAD [31]. However, endovascular treatment can also be viewed as the preferred option for the treatment of CAD patients, especially when the patient has both an embolism and obvious hypoperfusion [32]. In this case, endovascular treatment can effectively relieve stenosis, increase blood flow, and improve low perfusion. In a retrospective study, 140 cases of CAD patients received stenting, and angiographic follow-up was conducted for an average of 12.8 months. The results showed that dissection-induced vascular stenosis was significantly improved and that secondary stroke events accounted for only 1.4% of cases. Thus, endovascular therapy could effectively improve CAD-induced vascular stenosis and reduce the incidence of ischemic stroke [33]. Multiple overlapping stents could also effectively reduce the blood flow velocity in pseudoaneurysms and promote thrombosis, thereby shrinking the pseudoaneurysm or causing it to disappear. Previous studies showed that dissection stenosis of CAD patients undergoing stenting therapy could be largely eased, from 71% to complete remission [29]. In terms of the progression of CAD and the structural damage to the vessel wall, patients in the acute stage and Borgess type IB and II patients would significantly benefit from the use of stenting as the preferred treatment [23]. 24
Management of cervicocephalic arterial dissection. Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery
 Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Management of cervicocephalic arterial dissection Ciro G. Randazzo, MD, MPH Thomas Jefferson University Hospital, Department of Neurosurgery Definition Disruption of arterial wall, either at level of intima-media
Internal Carotid Artery Dissection
 May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
May 2011 Internal Carotid Artery Dissection Carolyn April, HMS IV Agenda Presentation of a clinical case Discussion of the clinical features of ICA dissection Discussion of the imaging modalities used
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Carotid Artery Dissection Causing an Isolated Hypoglossal. Nerve Palsy
 Archives of Clinical and Medical Case Reports doi: 10.26502/acmcr.96550035 Volume 2, Issue 5 Case Report Carotid Artery Dissection Causing an Isolated Hypoglossal Muzzammil Ali*, Yatin Sardana Nerve Palsy
Archives of Clinical and Medical Case Reports doi: 10.26502/acmcr.96550035 Volume 2, Issue 5 Case Report Carotid Artery Dissection Causing an Isolated Hypoglossal Muzzammil Ali*, Yatin Sardana Nerve Palsy
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
Corporate Medical Policy
 Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias. UCSF Vascular Symposium April 7-9, Acute Aortic Dissection
 Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Animesh Rathore, MD 4/21/17. Penetrating atherosclerotic ulcers of aorta
 Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
PERPHERAL ARTERY ANEURYSM. By Pooja Sharma and Susanna Sebastianpillai
 PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
Case 9799 Stanford type A aortic dissection: US and CT findings
 Case 9799 Stanford type A aortic dissection: US and CT findings Accogli S, Aringhieri G, Scalise P, Angelini G, Pancrazi F, Bemi P, Bartolozzi C Department of Diagnostic and Interventional Radiology, University
Case 9799 Stanford type A aortic dissection: US and CT findings Accogli S, Aringhieri G, Scalise P, Angelini G, Pancrazi F, Bemi P, Bartolozzi C Department of Diagnostic and Interventional Radiology, University
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Treatment of Unruptured Vertebral Artery Dissecting Aneurysms
 33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
Bilateral blunt carotid artery injury: A case report and review of the literature
 CASE REPORT Bilateral blunt carotid artery injury: A case report and review of the literature S Cheddie, 1 MMed (Surg), FCS (SA); B Pillay, 2 FCS (SA), Cert Vascular Surgery; R Goga, 2 FCS (SA) 1 Department
CASE REPORT Bilateral blunt carotid artery injury: A case report and review of the literature S Cheddie, 1 MMed (Surg), FCS (SA); B Pillay, 2 FCS (SA), Cert Vascular Surgery; R Goga, 2 FCS (SA) 1 Department
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Isolated Unilateral Hypoglossal Nerve Palsy Due to Vertebral Artery Dissection
 CM&R Rapid Release. Published online ahead of print October 26, 2011 as Case Report Isolated Unilateral Hypoglossal Nerve Palsy Due to Vertebral Artery Dissection Karthik Mahadevappa, MBBS 1 ; Thomas Chacko,
CM&R Rapid Release. Published online ahead of print October 26, 2011 as Case Report Isolated Unilateral Hypoglossal Nerve Palsy Due to Vertebral Artery Dissection Karthik Mahadevappa, MBBS 1 ; Thomas Chacko,
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
10/19/12. Uncommon Causes of Stroke. José Biller, MD, FACP, FAAN, FAHA Disclosures. Dr. Biller has no disclosures to report
 10/19/12 Uncommon Causes of Stroke José Biller, MD, FACP, FAAN, FAHA Loyola University Chicago Stritch School of Medicine Chicago, IL José Biller, MD, FACP, FAAN, FAHA Disclosures Dr. Biller has no disclosures
10/19/12 Uncommon Causes of Stroke José Biller, MD, FACP, FAAN, FAHA Loyola University Chicago Stritch School of Medicine Chicago, IL José Biller, MD, FACP, FAAN, FAHA Disclosures Dr. Biller has no disclosures
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Screening and Management of Blunt Cereberovascular Injuries (BCVI)
") Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
Grady Memorial Hospital Trauma Service Guidelines Screening and Management of Blunt Cereberovascular Injuries (BCVI) BACKGROUND Blunt injury to the carotid or vertebral vessels (blunt cerebrovascular injury
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke
 Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Review Article Treatment of Cervical Artery Dissection: Antithrombotics, Thrombolysis, and Endovascular Therapy
 Hindawi BioMed Research International Volume 2017, Article ID 3072098, 6 pages https://doi.org/10.1155/2017/3072098 Review Article Treatment of Cervical Artery Dissection: Antithrombotics, Thrombolysis,
Hindawi BioMed Research International Volume 2017, Article ID 3072098, 6 pages https://doi.org/10.1155/2017/3072098 Review Article Treatment of Cervical Artery Dissection: Antithrombotics, Thrombolysis,
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Diseases of the Aorta
 Diseases of the Aorta ASE Review 2018 Susan E Wiegers, MD, FASE, FACC Professor of Medicine My great friend Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives Aneurysm Dissection
Diseases of the Aorta ASE Review 2018 Susan E Wiegers, MD, FASE, FACC Professor of Medicine My great friend Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives Aneurysm Dissection
How to manage the left subclavian and left vertebral artery during TEVAR
 How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D.
 CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Ryan M. Degen, MD, Matthew E. Fink, MD, Lisa Callahan, MD, Kenton Fibel, MD, Jim Ramsay, ATC, and Bryan T. Kelly, MD
 A Case Report & Literature Review Internal Carotid Artery Dissection After Indirect Blunt Cervical Trauma in an Ice Hockey Goaltender Ryan M. Degen, MD, Matthew E. Fink, MD, Lisa Callahan, MD, Kenton Fibel,
A Case Report & Literature Review Internal Carotid Artery Dissection After Indirect Blunt Cervical Trauma in an Ice Hockey Goaltender Ryan M. Degen, MD, Matthew E. Fink, MD, Lisa Callahan, MD, Kenton Fibel,
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Posterior Cerebral Artery Aneurysms with Common Carotid Artery Occlusion: A Report of Two Cases
 Journal of Neuroendovascular Therapy 2017; 11: 371 375 Online March 3, 2017 DOI: 10.5797/jnet.cr.2016-0114 Posterior Cerebral Artery Aneurysms with Common Carotid Artery Occlusion: A Report of Two Cases
Journal of Neuroendovascular Therapy 2017; 11: 371 375 Online March 3, 2017 DOI: 10.5797/jnet.cr.2016-0114 Posterior Cerebral Artery Aneurysms with Common Carotid Artery Occlusion: A Report of Two Cases
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns
 CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
Non Atheromatous Lesions Fibromuscular Dysplasia. Rod Samuelson, MD Babak Jahromi,, MD Elad Levy, MD Adnan Siddiqui,, PhD, MD Nick Hopkins, MD
 Non Atheromatous Lesions Fibromuscular Dysplasia Rod Samuelson, MD Babak Jahromi,, MD Elad Levy, MD Adnan Siddiqui,, PhD, MD Nick Hopkins, MD Presenter Disclosure Information L. Nelson Hopkins MD FINANCIAL
Non Atheromatous Lesions Fibromuscular Dysplasia Rod Samuelson, MD Babak Jahromi,, MD Elad Levy, MD Adnan Siddiqui,, PhD, MD Nick Hopkins, MD Presenter Disclosure Information L. Nelson Hopkins MD FINANCIAL
Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom
 J Headache Pain (2012) 13:247 253 DOI 10.1007/s10194-012-0420-2 BRIEF REPORT Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom Hajime Maruyama Harumitsu Nagoya
J Headache Pain (2012) 13:247 253 DOI 10.1007/s10194-012-0420-2 BRIEF REPORT Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom Hajime Maruyama Harumitsu Nagoya
University Journal of Medicine and Medical Sciences
 ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial
 An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated
An aneurysm is a localized abnormal dilation of a blood vessel or the heart Types: 1-"true" aneurysm it involves all three layers of the arterial wall (intima, media, and adventitia) or the attenuated
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
. 8. Pharmacological treatment in acute stroke 8.3 Antiplatelet and anticoagulant treatment in stroke due to arterial dissection
 . 8. Pharmacological treatment in acute stroke 8.3 Antiplatelet and anticoagulant treatment in stroke due to arterial dissection Reference Evidence Tables PHARM4 What is the safety and efficacy of anticoagulants
. 8. Pharmacological treatment in acute stroke 8.3 Antiplatelet and anticoagulant treatment in stroke due to arterial dissection Reference Evidence Tables PHARM4 What is the safety and efficacy of anticoagulants
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
IMAGING the AORTA. Mirvat Alasnag FACP, FSCAI, FSCCT, FASE June 1 st, 2011
 IMAGING the AORTA Mirvat Alasnag FACP, FSCAI, FSCCT, FASE June 1 st, 2011 September 11, 2003 Family is asking $67 million in damages from two doctors Is it an aneurysm? Is it a dissection? What type of
IMAGING the AORTA Mirvat Alasnag FACP, FSCAI, FSCCT, FASE June 1 st, 2011 September 11, 2003 Family is asking $67 million in damages from two doctors Is it an aneurysm? Is it a dissection? What type of
Optimal repair of acute aortic dissection
 Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Disclosures: Acute Aortic Syndrome. A. Michael Borkon, M.D. Director of CV Surgery Mid America Heart Institute Saint Luke s Hospital Kansas City, MO
 Acute Aortic Syndrome Disclosures: A. Michael Borkon, M.D. Director of CV Surgery Mid America Heart Institute Saint Luke s Hospital Kansas City, MO No financial relationships to disclose 1 Acute Aortic
Acute Aortic Syndrome Disclosures: A. Michael Borkon, M.D. Director of CV Surgery Mid America Heart Institute Saint Luke s Hospital Kansas City, MO No financial relationships to disclose 1 Acute Aortic
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
Common clinical presentation and possible ischemic
 Facial Diplegia Complicating a Bilateral Internal Carotid Artery Dissection O. Gout, MD; I. Bonnaud, MD; A. Weill, MD; A. Moulignier, MD; J.J. Quenet, MD; J. Moret, MD; P. Bakouche, MD Background and Purpose
Facial Diplegia Complicating a Bilateral Internal Carotid Artery Dissection O. Gout, MD; I. Bonnaud, MD; A. Weill, MD; A. Moulignier, MD; J.J. Quenet, MD; J. Moret, MD; P. Bakouche, MD Background and Purpose
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries
 Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
Imaging for Peripheral Vascular Disease
 Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography
 Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography Dr. Pramod Shaha 1, Dr. Vinay Raj R 2, Dr. (Brig) K. Sahoo 3 Abstract: Aim & Objectives:
Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography Dr. Pramod Shaha 1, Dr. Vinay Raj R 2, Dr. (Brig) K. Sahoo 3 Abstract: Aim & Objectives:
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period
 Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period Marysia Tweet, MD NASCI Annual Meeting October 18 th, 2016 2016 MFMER slide-1 DISCLOSURE No relevant financial relationship(s)
Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period Marysia Tweet, MD NASCI Annual Meeting October 18 th, 2016 2016 MFMER slide-1 DISCLOSURE No relevant financial relationship(s)
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011
 Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Advances in the treatment of posterior cerebral circulation symptomatic disease
 Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Spontaneous Coronary Artery Dissection
 Spontaneous Coronary Artery Dissection Malissa J. Wood, MD FACC FAHA Co-Director MGH Heart Center Corrigan Women s Heart Health Program Massachusetts General Hospital 40 y/o female transferred from OSH
Spontaneous Coronary Artery Dissection Malissa J. Wood, MD FACC FAHA Co-Director MGH Heart Center Corrigan Women s Heart Health Program Massachusetts General Hospital 40 y/o female transferred from OSH
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
THORACIC AORTIC DISSECTION
 The Essence of Aortic Dissection THORACIC AORTIC DISSECTION Aortic dissection can be classified as acute if it s onset has been less than 14 days or chronic if its onset has been more than 14 days. Mortality
The Essence of Aortic Dissection THORACIC AORTIC DISSECTION Aortic dissection can be classified as acute if it s onset has been less than 14 days or chronic if its onset has been more than 14 days. Mortality
Descending aorta replacement through median sternotomy
 Descending aorta replacement through median sternotomy Mitrev Z, Anguseva T, Belostotckij V, Hristov N. Special hospital for surgery Filip Vtori Skopje - Makedonija June, 2010 Cardiosurgery - Skopje 1
Descending aorta replacement through median sternotomy Mitrev Z, Anguseva T, Belostotckij V, Hristov N. Special hospital for surgery Filip Vtori Skopje - Makedonija June, 2010 Cardiosurgery - Skopje 1
Cervical Spine Adjusting and the Vertebral Artery
 www.fisiokinesiterapia.biz Cervical Spine Adjusting and the Vertebral Artery Contemporary perspectives on patient safety and protection, clinical reality and patient management Why? Currently the single
www.fisiokinesiterapia.biz Cervical Spine Adjusting and the Vertebral Artery Contemporary perspectives on patient safety and protection, clinical reality and patient management Why? Currently the single
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
AORTIC DISSECTION. DISSECTING ANEURYSMS OF THE AORTA or CLASSIFICATION
 DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
DISSECTING ANEURYSMS OF THE AORTA or AORTIC DISSECTION CLASSIFICATION DeBakey classified aortic dissections into types I, II, and III :- Type I dissection the tear site originates in the ascending aorta,
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost