SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT. Neeraj Naval, MD Baptist Neurological Institute
|
|
|
- Merryl Owens
- 5 years ago
- Views:
Transcription
1 SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT Neeraj Naval, MD Baptist Neurological Institute
2 Disclosures/ COI Nothing to disclose (what happens in Vegas stays in Vegas) No Conflict of interest
3 Non-modifiable Impact Factors (ICH Score) Age: < 80 : 0 > 80 : 1 GCS score : : : 2 ICH location : Supratentorial : 0 Infratentorial : 1 ICH volume (AxBxC/2) < 30 ml : 0 > 30 ml : 1 IVH No : 0 Yes : 1 Total: 0-6
4 ICH Overview: (Outcome model) ICHS Mortality (%)
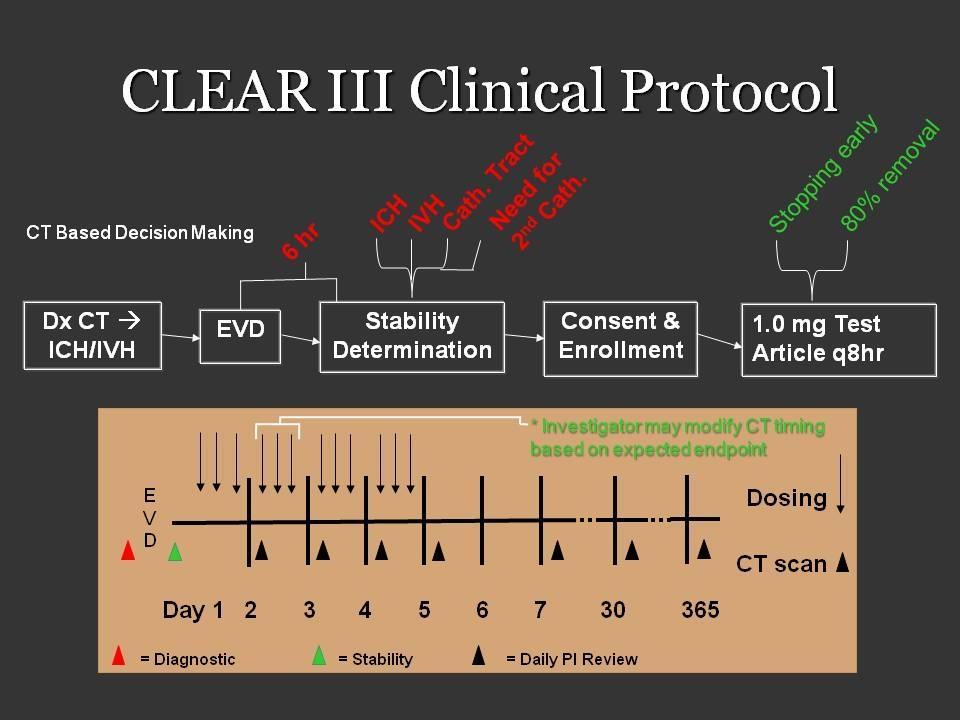
5 Lecture Focus: Modifiable Impact Factors Modifiable Risk factors for Outcomes aka Complications of ICH Mass effect (Hematoma expansion- Hemostasis) A) Blood pressure control B) Hemostatic therapy C) Reversal of bleeding diathesis Mass effect (Cerebral edema/ Intracranial HTN) Hydrocephalus (sec to IVH): CLEAR 3 Seizures: ppx? Recurrent ICH
6 Lecture Focus: EXCLUDED Reversal of NOAC (Dr. Rama/ Chen) Role of Surgery in ICH: STITCH, STICH 2 (Dr. Lopes) Role of Surgery in ICH: Incl. Minimally Invasive surgery (Dr. Lopes)
7 ICH Overview: Impact Approximately 500,000 new strokes occur every year in the United States, 15% of them are hemorrhagic strokes. These numbers are expected to double during next 50 years. Increased longevity of the population. Overall population based mortality of ICH patients remains high: 6% die before reaching a hospital. 30 to 50% die within the first 30 days. GCS < 8 and ICH volume > 60 cc > 90% 30-day mortality Independent living after ICH: After 1 month: 10%, After 6 months: 20%.





8 ICH Overview: Location Putaminal Thalamic Lobar Caudate Pontine

9 ICH: presentation 50% CAA 50% Other Majority HTN Qureshi; N Engl J Med 2001;344:
10 ICH Overview: Etiology PRIMARY ICH Hypertensive Cerebral amyloid angiopathy Cryptogenic SECONDARY ICH Trauma AVM Intracranial aneurysm Coagulopathy Hemorrhagic conversion of ischemic stroke Dural sinus thrombosis Intracranial tumor Cavernous malformation Dural AV fistula Venous angioma Cocaine use CNS vasculitis/ RCVS Mayer;Lancet Neurol 2005;4(10):662-72




11 Mass Effect: Blood pressure/ Hematoma expansion 38%>33% growth over 24h 73% some growth over 24h Independent predictor of bad outcome Davis; Neurology 2006;66(8):





12 Hematoma enlargement within 6 hours from symptom onset
13 ICH and IVH: Complications Hematoma enlargement Early hematoma growth in ~ 30% of ICH patients within 3 hours of onset can cause significant neurologic deterioration. 1 cc larger volume ICH = 7% more likely to have worse clinical outcomes
14 Blood Pressure Targets Association vs true evidence Cause-effect Does increased Blood pressure cause more bleeding? Or is it a marker for more severe neurological injury (increased ICH volume = Kocher Cushing s reflex) Treatment effect Does better blood pressure control actually lead to hemostasis? Or does it lead to worsening perihematomal ischemia?
15 Best available evidence in 90s 1. Increased BP is associated with larger ICH volumes: SBP goal < 160 (Retrospectively observed association) 2. Small-moderate ICH volumes (<45 cc) are NOT associated with perihematomal ischemia (Powers et al) ADC on MRI suggests inflammation (vasogenic edema) > ischemia (cytotoxic injury) 15-20% acute decrease in BP in first 6 hours not associated with decrease in critical perfusion. MAP goal < 130 or SBP < 180 (1999 AHA guidelines)
16 Available evidence in 21 st century ATACH pilot: small Pilot study showing better hemostasis with SBP goal < 160 than historical controls. ATACH study showed trends towards decreased hematoma expansion and PHE in compared to compared to ATACH 2 ongoing INTERACT: Mean 1.6 cc decreased in RCT with SBP goal < 140 compared to SBP < 180; 36% reduced risk of SHE, no difference in clinical outcomes (safe and non-inferior). AHA revised guidelines: If ICP elevation an issue, Control ICP with SBP goal < 180 until ICP controlled, otherwise SBP < 160. SBP < 140 is considered SAFE
17 ?? Best available evidence in 21 st century INTERACT 2 Trend (p 0.06) towards improved functional outcomes with SBP < 140 compared to 180 Significant difference if using ordinal analysis (not pre-specified) Median GCS 14, median ICH volume 11 cc 75% of enrolled patients with ICH volume < 20 cc Restricted admission criteria to SBP < 220 Nearly 70% patients enrolled in China No consistency in choice of HTN meds Investigators not blinded (higher rates of hemostatic therapy in study group) No difference in hematoma expansion rates (1.4 cc difference) or mortality (12% each) AHA revised guidelines x 2: SBP < 140 is SAFE and can be potentially effective in improving functional outcomes (Level of Evidence IIB) in patients similar to those enrolled in INTERACT 2.
18 Mass Effect: Hemostasis: Novo7 trial Phase 2 B trial for Activated factor patients with 100 each in 40, 80, 160 mcg/kg and placebo within 4h symptom onset Placebo mrs % 55% 49% 54% Complications 2% % Mortality: 29% to 18%
19 (Not So) FAST trial FAST Placebo vs. rfviia (20µg/kg or 80µg/kg) within 4hr n=841 Hematoma expansion Functional outcome No difference in good outcome, bad outcome or death?benefit ICH volume<60ml; Age 70; 2.5h to treatment; IVH<5mL Mayer;N Engl J Med 2008;15;358(20): Stroke 2009;40:833-40
20 Why did FAST fail? Mortality: Novo7: 26%, Placebo: 21% Randomization: IVH in 29% Placebo, 41% study drug Liberal inclusion criteria (age up to 80, GCS 6-8 OK, large ICH volumes ok) Post-hoc analysis: Benefit in Novo-7 group Age < 70 ICH Volume < 60 cc IVH < 5cc Drug within 2.5h Too little, too late. Could we predict who would have expanded hematomas?

21 SPOT SIGN
22 Contrast extravasation/ Spot sign Spot sign +ve: 77% likelihood of hematoma expansion (Wada et al) Spot sign ve: 4% likelihood of hematoma expansion (NPV 96%) PREDICT TRIAL: > 33% increase or absolute increase of 6cc PPV 60% NPV 78% Sensitivity: 51% Specificity: 85%

23 SPOT SIGN CTA spot sign NON- CON CTA POST- CON NON- CON Delgado; Stroke 2009; Jun; EPUB ahead of print; Wada; Stroke 2007;38:
24 Contrast extravasation/ Spot sign What can we do about this data? Hemostatic agents ongoing trials (STOP-IT, SPOTLIGHT study) More aggressive BP control.. SBP goal 140? Reversal of platelet dysfunction PLT transfusion (PATCH trial)? Reversal of coagulopathy.high risk patients? TRIAGE
25 Coagulopathies in a snapshot Warfarin: PCC >> FFP (Sarode et al), + Vit K IV NOAC: PCC (Xa), specific inhibition (DTI) tpa: NS: Cryoprecipitate + platelets +/- FFP S: Antifibrinolytic therapy (tranexamic acid/ Amicar) Heparin gtt: Protamine (no more than 50mg; administration time based) LMWH (lovenox): 0-8h: 1 mg protamine: 1 mg lovenox 8-12h: 0.5mg Protamine: 1 mg lovenox 12-24h: None unless surgery/ ongoing bleeding or ARF/ CRF Fondaparinaux:??
26 ASA/ Plavix Reversal ASA:? Platelets PATCH trial Plavix: Half life 8 hours?plt/ ddavp (MOA- vwf) DDAVP: Uremic platelet dysfunction,? Anti-PLT (PFA correction) Indication for PLT transfusion A) Hematoma expansion/ Neurological deterioration B) Spot Sign + C) Surgical intervention (including EVD) D) Abnormal PFA
27 Intracranial HTN: Clinical signs NEUROLOGICAL Blown pupils, anisocoria (new) Altered mental status Decerebrate/ decorticate posturing Increase in ICP (if monitored) NON-NEUROLOGICAL Cushings response: Hypertension, reflex bradycardia, irregular respirations) Nausea, vomiting
28 ABCs Airway: GCS < 8 GCS > 8 with impending neurological deterioration Cough/ gag/ increased secretions (Coplin et al) Breathing: Ataxic/ cluster breathing patterns Sat probe: Avoid hypoxia, sat goals > 94% ABG/ ETCO2: Co2 goal Circulation: MAP > 70 CPP > 60 (TBI)/ > 70 (comatose ICH/SAH), ICP < 20
29 Hyperventilation Decrease in PCO2 from 40 to 30 mmhg --- Cerebral vasoconstriction % decrease in CBF/ 1 mmhg decrease in PCO2 (30% reduction in CBF) --- decreased ICP Prolonged Cerebral vasoconstriction --- Cerebral Ischemia CSF Ph normalizes --- Rebound Hyperemia --- Reperfusion Injury --- Rebound Increase in ICP Caution: Avoid prophylactic use, avoid prolonged use
30 Hyperosmolar therapy Options Mannitol (1-1.5 gm/kg) Hypertonic saline (3% bolus / 23.4% 30 cc bullet )
31 Mannitol gm/kg 20% mannitol, acts within minutes, peaks at 1 h duration 4-6 hours. Failure to respond: 2 nd dose 1.5-2gm/kg Can give through peripheral IV Watch for Hypotension secondary to increased diuresis
32 Hypertonic saline 23.4% Saline 30 cc bolus, may repeat with second bullet Requires Central venous access Follow with maintenance 3% saline infusion with Na goal Effective in mannitol failures Watch for acute hypotension
:554-559, March 2011. DOI: 10.1097/CCM.")
33 Mannitol vs Hypertonic saline Hypertonic saline versus mannitol for the treatment of elevated intracranial pressure: A meta-analysis of randomized clinical trials *. Kamel, Hooman; Navi, Babak; Nakagawa, Kazuma; Hemphill, J; Claude III MD, MAS; Ko, Nerissa Critical Care Medicine. 39(3): , March DOI: /CCM.0b013e318206b9be 2011 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
34 Relative risk of successful control of elevated ICP Hypertonic saline versus mannitol for the treatment of elevated intracranial pressure: A meta-analysis of randomized clinical trials *. Kamel, Hooman; Navi, Babak; Nakagawa, Kazuma; Hemphill, J; Claude III MD, MAS; Ko, Nerissa Critical Care Medicine. 39(3): , March DOI: /CCM.0b013e318206b9be 2011 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
35 Difference in mean quantitative reduction of ICP Hypertonic saline versus mannitol for the treatment of elevated intracranial pressure: A meta-analysis of randomized clinical trials *. Kamel, Hooman; Navi, Babak; Nakagawa, Kazuma; Hemphill, J; Claude III MD, MAS; Ko, Nerissa Critical Care Medicine. 39(3): , March DOI: /CCM.0b013e318206b9be 2011 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
36 Advantages Mannitol May be given through PIV 23.4% saline Higher reflection coefficient Maintains intravascular volume status May be followed by 3% saline as continuous infusion?more robust action?longer duration of action? Greater impact on brain oxygenation (Oddo et al)
37 ICP monitor / IVC placement Intraventricular catheter (IVC) facilitates CSF drainage ICP monitoring useful with unreliable clinical exam (GCS < 8) Cerebral herniation possible without ICP elevation Over-drainage especially in setting of cerebellar lesions can cause upward herniation
38 Brain Code Supportive treatment HOB > 30 degrees Minimize neck compression Sedation, minimize agitation Maintain Volume status Maintain Circulatory status (MAP goals) Seizure prophylaxis Glycemic control Goal of normothermia
39 Seizures Incidence of seizures with ICH: Lobar 14% seizures, deep 4% (Bladin et al) Phenytoin associated with worse outcomes in ICH, CVA, SAH, TBI. Naidech et al: 10-fold increase in poor outcomes with phenytoin Fatal Flaws ICH volume, IVH volume and location were NOT a predictor of outcomes Difference in ICH volume in 2 groups > 20 cc, admission GCS 10 to 14
40 Seizure Prophylaxis: Counter-argument Up to 26% of ICH patients could have only somnolence as manifestation of NCSE if monitored using ceeg monitoring (Vespa et al): 26% Break up by location: 28% lobar, 21% deep. Recommendation: Routine prophylaxis for spontaneous ICH is NOT recommended. Recommendation is relevant for SPONTANEOUS ICH. If considering AED for any reason (temporal ICH, underlying structural lesion, craniotomy, cocaine use), consider alternative to PHT for prophylaxis for lobar ICH ceeg monitoring is highly advisable in patents with AMS following ICH.


41 Hydrocephalus/ IVH: Tuhrim et al




42 Hydrocephalus/ IVH
43

44
45

46 Subject Post-rebleed


47 IVH expansion before after
48 CLEAR 3 Results Pragmatic Phase 3 randomized control trial for tpa vs saline through EVD Outcome assessment at 6 months: Primary endpoint: mrs 0-3: 48% tpa vs 45% control (NS) Secondary outcomes: egos: ND Mortality lower in tpa group: p 0.006, NNT 10 66% home/ rehab (tpa) vs 56% (control): p 0.06 Bleed: 2.6% vs 2% (safe) Infection rates marginally lower (???)
49 CLEAR 3 Results Subgroup analysis: Clot lysis more effective in post hoc analysis in.. A) IVH volume over 20 cc (10% higher rates of mrs 0-3) B) Time to treat < 48h So what now. CLEAR 4? 5? 6?
 n=465 90d outcome RCT minimally invasive surgery for basal ganglia ICH Cannula placed inside clot and tpa 1mg q8h x max 72h injected")
50 ICH: MISTIE Stereotactic thrombolysis/aspiration MINIMALLY INVASIVE CRANIOPUNCTURE RCT minimally invasive surgery for basal ganglia ICH Cannula placed inside clot and 10,000U- 50,000U urokinase injected followed by aspiration (dose based on hematoma volume) n=465 90d outcome RCT minimally invasive surgery for basal ganglia ICH Cannula placed inside clot and tpa 1mg q8h x max 72h injected and aspirated until: 1. ICH volume 10cc 2. 80% decrease 3. Dose limit reached +tx -tx MRS % 41% Dead 8% 9%
51 Recurrent ICH: Vascular imaging Cerebral angiography To make the etiological diagnosis in cases of: Aneurysms AVM s Vasculitis Dural AV fistula
52 Vascular imaging Cerebral angiography In young patients (< 45 y/o) w/o risk factors for ICH, the yield of angiography can reach 48% in putaminal, thalamic and posterior fossa ICH. In young patients with lobar ICH, yield of angiography can reach 65%. The yield of cerebral angiography in primary IVH is high regardless the age of the patient (50 to 67%), commonest cause AVM > aneurysm. In this study of 206 ICH patients, any patient > 45 y/o with h/o hypertension, and hypertensive on presentation with ICH in classic locations (BG/ thalamus), the yield of angiography was ZERO (Zhu et al)
53 Recuurent ICH: CTA/ MRI MRI To make the etiological diagnosis in cases of: Brain tumors (Primary) CTA Brain mets: (Lung, Breast, Renal, Melanoma, Choriocarcinoma, Thyroid) Cavernous malformations Amyloid angiopathy Venous infarctions (CTV) To make the etiological diagnosis in cases of: Aneurysms AVMs (Spot Sign)
54 ICH Recurrence risk Anticoagulation: Hold for 7-10 days (shorter in patients with prosthetic valve) Reversal based on severity of bleed and indication for AC Assess risk-benefit of long term AC in A Fib (CHADS 2 score/ HAS-BLED). Assess alternatives to AC (IVC filter, anti-plt) Assess risk for recurrent bleed (high with cortical/ amyloid ICH, low with Hypertensive bleed)
55 ICH: Recurrence risk Anti-platelets: Hold for 7 days; assess risk vs benefit of long term antiplatelet therapy. Statins: controversial (SPARCL vs met-analysis) If lobar ICH and weaker indication for statins (hypercholesterolemia) or strong indication (CAD/ CVA) but low LDL, may be advisable to stop statins If deep ICH (hypertensive) and strong indication for statins (h/o MI, CVA), may continue Acutely may lower peri-hematomal edema
56 Thank you for allowing me to speak beyond my allotted time
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Intracerebral Hemorrhage
 Intracerebral Hemorrhage J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director,
Intracerebral Hemorrhage J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director,
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Jan 5, Coma 8 years. Jan 11, 2014
 Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Intracerebral Hemorrhage
 Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Management of Intracerebral Haemorrhage
 Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC
 Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Update in Management of Acute Spontaneous Intracerebral Haemorrhage
 Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Index. C Capillary telangiectasia, intracerebral hemorrhage in, 295 Carbon monoxide, formation of, in intracerebral hemorrhage, edema due to,
 Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Klinikum Frankfurt Höchst
 Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
Blood pressure management in hemorrhagic stroke Blood pressure in acute ICH Do we need additional trials after INTERACT2 and ATTACH-II? Focus.de Department of Neurology,, Germany Department of Neurology,
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Hemorrhagic Stroke. Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
 Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY. Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center
 UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Content 1. Relevance 2. Principles 3. Manangement
 Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Welcome to our MISTIE III Safety Forum September 12, 2016
 Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Hemorrhage. Dr. Al Jin Nov. 17, 2015
 Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD
 Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD") FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Tim Rausch, FNP-BC UPMC Presbyterian Hospital Pittsburgh, PA
 Tim Rausch, FNP-BC UPMC Presbyterian Hospital Pittsburgh, PA I have no financial interest in any of the products contained in this lecture nor am I receiving any financial compensation from any company
Tim Rausch, FNP-BC UPMC Presbyterian Hospital Pittsburgh, PA I have no financial interest in any of the products contained in this lecture nor am I receiving any financial compensation from any company
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
SPONTANEOUS INTRACEREBRAL HEMORRHAGE
 SPONTANEOUS INTRACEREBRAL HEMORRHAGE Intracerebral hemorrhageis an acute and spontaneous extravasationof blood into the brain parenchyma that may extend into the ventricles and subarachnoid space. It is
SPONTANEOUS INTRACEREBRAL HEMORRHAGE Intracerebral hemorrhageis an acute and spontaneous extravasationof blood into the brain parenchyma that may extend into the ventricles and subarachnoid space. It is
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia
 Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
Updates from 2017 International Stroke Conferences
 Updates from 2017 International Stroke Conferences Ravi Menon, MD Swedish Neuroscience Institute May 11, 2017 Seattle, WA 1 Disclosures No relevant financial disclosures Clinical trial involvement: Former
Updates from 2017 International Stroke Conferences Ravi Menon, MD Swedish Neuroscience Institute May 11, 2017 Seattle, WA 1 Disclosures No relevant financial disclosures Clinical trial involvement: Former
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Objectives. Definition 3/21/2017. Spontaneous, Nontraumatic Intracerebral Hemorrhage
 Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP-BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM Objectives
Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP-BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM Objectives
HHS Public Access Author manuscript Am J Emerg Med. Author manuscript; available in PMC 2016 April 01.
 The excess cost of inter-island transfer of intracerebral hemorrhage patients Kazuma Nakagawa, MD 1,2, Alexandra Galati, BA 2, and Deborah Taira Juarez, ScD 3 1 Neuroscience Institute, The Queen s Medical
The excess cost of inter-island transfer of intracerebral hemorrhage patients Kazuma Nakagawa, MD 1,2, Alexandra Galati, BA 2, and Deborah Taira Juarez, ScD 3 1 Neuroscience Institute, The Queen s Medical
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage
 Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage Authors Joji B. Kuramatsu, Stefan T. Gerner, Hagen B. Huttner, Stefan Schwab Affiliation University Hospital Erlangen Department
Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage Authors Joji B. Kuramatsu, Stefan T. Gerner, Hagen B. Huttner, Stefan Schwab Affiliation University Hospital Erlangen Department
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
AHA/ASA Guideline. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults
 AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults 2007 Update A Guideline From the American Heart Association/American Stroke Association Stroke Council,
AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults 2007 Update A Guideline From the American Heart Association/American Stroke Association Stroke Council,
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Outlook for intracerebral haemorrhage after a MISTIE spell
 Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
11 th Annual Cerebrovascular Symposium 5/11-12/2017. Hypertonic Use D E R E K C L A R K
 Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Online Supplementary Data. Country Number of centers Number of patients randomized
 A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Sinus Venous Thrombosis
 Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
5/15/2018. Reduced Platelet Activity
 ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville