Veni, vidi, vici I came, I saw, I... Conquered? Discussion and cases from my MFM rotation. Perinatal rounds March 30 th, 2010 Momoe Hyakutake, PGY 3
|
|
|
- Mitchell Moore
- 5 years ago
- Views:
Transcription

1 Veni, vidi, vici I came, I saw, I.... Conquered? Discussion and cases from my MFM rotation Perinatal rounds March 30 th, 2010 Momoe Hyakutake, PGY 3
2 Case based discussion on the following: 1) CCAM 2) Fetal tachycardia 3) Indomethacin tocolysis and ductus arteriosus constriction
3 Case 1
4 Mrs. TB 20 years old G2P1 LMP September 16, 2009 EDC June 26, 2010 based on LMP Regular 30 day cycles Sure of dates Routine prenatal care starting at 10 weeks GA
5 Mrs. TB Past medical history None Past surgical history None Past obstetrical history G1 2008, SVD of male infant at term, 8lbs Past gynecological history unremarkable
6 Mrs. TB Medications Prenatal vitamins Not taken preconception Allergies None Social history Quit smoking in 2009 Denies alcohol use Denies recreational drug use Family history unremarkable
7 Mrs. TB Abdominal pain at 9 weeks GA Normal ultrasound 9 weeks 2 days Adjusted EDC July 5, 2010 Pain subsequently resolved spontaneously MSS offered Patient declined Routine ultrasound on February 18, weeks GA Abnormal findings..... URGENT referral to perinatal!!!!!

8

9
10 CCAM Congenital cystic adenomatoid malformation of the lung Also called CPAM Developmental anomaly of the respiratory tract Excessive proliferation of terminal bronchioles, lacks normal alveoli Most common congenital lung lesion Incidence of 1:35,000
11 CCAM Can occur in either lung with no predominance Slightly higher incidence in males than females Mostly unilobar (85-95%)
12 Type % of postnatal cases Single or multiple large cysts surrounded by smaller cysts and compressed normal parenchyma Large cysts lined with pseudostratified ciliated epithelium Smaller cysts lined by cuboidal to columnar epithelium Associated anomalies rarely seen
13 Type % of postnatal cases Numerous smaller cysts Lined by cuboidal to columnar epithelial cells with thin, underlying fibromuscular layer Assiciated with higher incidence of cardiac, renal and chromosomal anomalies
14 Type % of postnatal cases Male predominance Small cystic lesions or solid lesions Adenomatoid in appearance
15 Type 0 Acinar dysplasia or agenesis Rare Incompatible with life
16 Type % of cases Peripheral cyst type Hamartomatous malformation of distal acinus Large thin-walled cysts located at periphery of the lobe, lined by smooth membrane
17 CCAM vs. BPS CCAM Communicates with the tracheobronchial tree Derives their arterial blood supply and venous drainage from normal pulmonary circulation BPS No connection to tracheobronchial tree Derives blood supply from anomalous systemic artery
18 Natural history Unpredictable growth between weeks GA Up to 40% undergo rapid proliferation and tumor enlargement Regression in 15% (rare if hydrops has developed) Growth usually reaches a plateau at 28 weeks




19 Adzick et al. 1998
20 Prognostic factors CCAM volume to head circumference ratio (CVR) height x width x length x 0.52 head circumference CVR 1.6, 80% risk of hydrops CVR 1.6, 2% risk of hydrops ***CCAMs with a dominant cyst may be unpredictable in their growth and expansion so should be excluded from this calculation



21 CVR = 4.7 x 2.8 x 4.3 x 0.52 = Therefore less than 2% risk of developing fetal hydrops
22 Treatment options Expectant Thoracocentesis / cyst-amniotic shunt Macrocystic, unilocular Percutaneous Fetal sclerotherapy Antenatal corticosteriod administration In utero fetal lobectomy Ex utero intrapartum therapy
23 Antenatal steriod treatment Curran et al Journal of pediatric surgery, 2010 Retrospective review 16 patients with predominantly microcystic CCAMs treated with single course of steriod 3 excluded, loss to follow-up 13/13 survived to delivery, 11/13 (85%) survived to neonatal discharge
24 Antenatal steriod treatment Morris et al. Journal of pediatric surgery, 2009 Retrospective review 15 patients with CCAM 13 hydropic, 2 non hydropic 7/13 (54%) initially responded to steroids 8/15 survived neonatal discharge Survival rate 53%
25 Antenatal steriod treatment Peranteau et al. Fetal diagnosis and therapy, 2007 Retrospective review 11 patients (10 micro, 1 macro) 5 patients had hydrops 4/5 (80%) resolution of hydrops 100% survival in all previously hydropic fetuses
26 Summery CCAM is the most common congenital lung lesion In the presence of hydrops mortality is 100% CVR can help identify fetuses at risk of developing hydrops Choice of therapy depends on type of lesion (microcystic vs macrocystic) Promising evidence supporting the use of antenatal steriods in the treatment of CCAM, espcially when its microcystic
27 Case 2
28 Mrs. NZ 29 years old G1P0 Started seeing her obstetrical care provider at 5 weeks gestation
29 Mrs. NZ LMP July 27, 2009 Regular monthly cycles EDD May 4, 2010 Past medical history Hypothyroidism Medications Synthroid 0.1mg po daily Folic acid 1mg po daily Allergy Lactose
30 Mrs. NZ Past surgical history Appendectomy Family history Niece with an atrial septal defect (no repair) Social history Non smoker No alcohol No recreational drug use
31 Mrs. NZ Uneventful first trimester Seen regularly for prenatal care Prenatal visit at 28+3 weeks GA.....


32 Fetal tachyarrhythmia
33
34
35 Work up Detailed ultrasounds evaluation of anatomy Cardiac Signs of hydrops Amniotic fluid level growth Fetal echocardiography Identify atrial and corresponding ventricular activity Cardiac function M mode Doppler
36 M-Mode echocardiography Simultaneous trace of ventricular and atrial contraction Cardiac rhythm and rate

37
38 Pulse wave doppler echocardiography Transducer transmits a series of pulses to detect motion Doppler shift that is measured is processed and then shown on screen in a spectral display Flow direction Flow velocity Flow characteristics
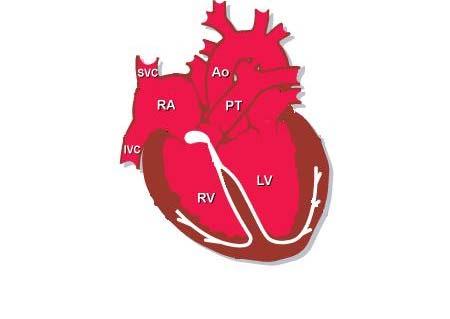
39 Pulse wave doppler echocardiography To assess cardiac arrhythmia Superior vena cava / ascending aorta Pulmonary vein / pulmonary artery Left ventricular inflow / outflow Innominate vein / aortic arch

40

41

42

43

44

45

46

47
48 Observation Management of fetal tachycardia No therapy but fetus is regularly monitored Delivery Prenatal therapy Transplacental drug therapy Direct fetal therapy Umbilical vein, IM, intraperitoneal, intraamniotic, or combination
49 Benign Premature atrial and ventricular No treatment required contractions Sustained tachyarrhythmia may develop in up to 1% of fetuses
50 Supraventricular tachycardia Deliver for neonatal medical treatment if term In utero medical treatment Can convert to normal sinus rhythm within 48 hours Conversion occurs easier in absence of hydrops
51 Digoxin Prolongs refractory period of the AV node Positive inotropic and negative chronotropic properties Placental transfer Fetal : maternal plasma concentration ratios between 0.4 and 0.9 Significantly decreased with hydrops
52 Digoxin Maternal adverse effects Anorexia Nausea Vomiting Headache Arrhythmia (ventricular extrasystoles, heart block) Contraindicated in Wolff-Parkinson-White syndrome
53 Digoxin Fetal tachycardia without hydrops Conversion rates of 32 71% Fetal tachycardia with hydrops Conversion rates of 10 20% (transplacental)
54 Sotalol Non selective β-blocker Class III antiarrhythmic Prolongs duration of action potential Increases refractory period of atrial and ventricular tissue Inhibits conduction in accessory bypass tracts Placental transfer Fetal : maternal plasma concentration ratios between 0.47 to 1.42
55 Sotalol Maternal adverse effects Fatigue Dizziness Dyspnea Palpattions Nausea / vomiting Torsade de Pointes tachycardia, 2.4%
56 Summery Sustained tachycardia can cause heart failure and lead to hydrops fetalis Fetal echocardiogram is an essential imaging technique to determine the type of tachycardia Both digoxin and sotalol are good first line treatment options If medications are started, must watch the patient carefully for side effects
57 Case 3
58 Mrs. BF 31 year old G2P1 at 30+2 weeks GA Presents to rural hospital with complaints of abdominal pain Started at 18:00, q10 minutes Increasing in frequency and intensity Seen by MD at 21:00 On exam, cervix is long, closed and posterior, soft.
59 Mrs. BF EDC April 12, 2010 based on 20 week ultrasound OB history 2009 delivery of female 34 weeks GA by cesarean section secondary to preeclampsia Current pregnancy minimal prenatal care. Normal 20 week ultrasound. Normal BP Pmhx Mild asthma
60 Mrs. BF Medications None Allergies No known drug allergies Social history Non smoker Denies alcohol use Denies recreational drug use
61 Mrs. BF 22:20 Patient given indomethacin 100mg PR 22:35 Patient given dexamethasone 6mg IM Transfer to RAH
62 Indomethacine Prostaglandin synthetase inhibitor First reported use in 1974 Nonselective inhibition of enzyme COX
63 PGE 2 and PGF 2 Increase myometrial contractility Coordinate contractions
64 Cochrane review, 2005 Compared to placebo Reduction in birth before 37 weeks (RR 0.21) Increase in gestation age, weighted mean difference 3.53 weeks Increase in birth weight, weighted mean difference g Compared to other tocolytics Reduction in birth before 37 weeks (RR.53)

65

66

67

68


69
70
71 Moise et al. 1993
72 Vermillion et al Retrospective review 72 fetuses 50% developed ductal constriction Mean age 30.9 ± 2.3 weeks Ductal constriction occurred by 31 weeks GA in 70% of affected fetuses
73 Vermillion et al. 1997

74
75 Should a different tocolytic been used?
76 Magnesium sulfate Most frequently used tocolytic in the United states Extracellular magnesium Suppresses calcium influx across cell membrane Intracellular magnesium Competitive inhibitor Inhibits myosin light-chain kinase activity
77 Magnesium sulfate Maternal side effects Nausea Vomiting Flushing Lethargy Dizziness Blurry vision Headache Pulmonary edema Shortness of breath Chest pain Cardiac arrest Pulmonary edema Shortness of breath Chest pain Cardiac arrest
78 Magnesium sulfate Cochrane review, 2002 No evidence of a clinically important tocolytic effect No evidence of any substantial improvements in neonatal morbidity Associated with an increase in fetal and pediatric deaths
79 Nifedipine Calcium channel blocker Inhibits calcium re-uptake by voltage dependent calcium channels in the myometrial cell wall Results in relaxation
80 Nifedipine Cochrane review 2002 Compared to any other tocolytic agents Statistically significant decrease in number of women giving birth within 7days (RR 0.76, 95% CI 0.60 to 0.97) and prior to 34 weeks GA (RR 0.83, 95% CI 0.69 to 0.99) NNT 11 (95% CI 6 to 100) Less respiratory distress syndrome, intraventricular hemorrhage, necrotising enterocolitis, jaundice Marked reduction in adverse maternal side effects
81 Summery Use of indomethacin between weeks GA should be carefully considered Consider ultrasound study of the ductus arteriosus if indomethacin is given after 30 weeks GA Nifedipine is a good alternative to indomethacin
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Lung sequestration and Scimitar syndrome
 Lung sequestration and Scimitar syndrome Imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Rotterdam, The Netherlands Pulmonary sequestration Pulmonary sequestration (PS)
Lung sequestration and Scimitar syndrome Imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Rotterdam, The Netherlands Pulmonary sequestration Pulmonary sequestration (PS)
Summary. HVRA s Cardio Vascular Genetic Detailed L2 Obstetrical Ultrasound. CPT 76811, 76825, _ 90% CHD detection. _ 90% DS detection.
 What is the role of fetal echocardiography (2D 76825, cardiovascular color flow mapping 93325) as performed in conjunction with detailed fetal anatomy scan (CPT 76811) now that AIUM requires limited outflow
What is the role of fetal echocardiography (2D 76825, cardiovascular color flow mapping 93325) as performed in conjunction with detailed fetal anatomy scan (CPT 76811) now that AIUM requires limited outflow
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
Kofinas Perinatal Providing Care to the Unborn
 Alexander D. Kofinas, MD Director, Kofinas Perinatal Associate Professor, Clinical Obstetrics and Gynecology Cornell University, College of Medicine Patient instructions for the use of Indomethacin and
Alexander D. Kofinas, MD Director, Kofinas Perinatal Associate Professor, Clinical Obstetrics and Gynecology Cornell University, College of Medicine Patient instructions for the use of Indomethacin and
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan
 PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
How Does Imaging Inform Fetal Cardiovascular Treatment?
 How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
By Dr.Asmaa Al sanjary
 By Dr.Asmaa Al sanjary Preterm delivery is defined by a birth occurring before 37 completed weeks of gestation. Prematurity is multifactorial and its incidence has increased during the last decade in most
By Dr.Asmaa Al sanjary Preterm delivery is defined by a birth occurring before 37 completed weeks of gestation. Prematurity is multifactorial and its incidence has increased during the last decade in most
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients
 Article Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients Zeev Weiner, MD, Abraham Lorber, MD, Eliezer Shalev, MD Objective. To examine the feasibility of
Article Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients Zeev Weiner, MD, Abraham Lorber, MD, Eliezer Shalev, MD Objective. To examine the feasibility of
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Evaluation of Fetal Arrhythmias
 REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Tocolytics. Tocolytics (terbutaline, magnesium sulfate injection) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.06 Subject: Tocolytics Page: 1 of 5 Last Review Date: September 15, 2016 Tocolytics Description Tocolytics
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.06 Subject: Tocolytics Page: 1 of 5 Last Review Date: September 15, 2016 Tocolytics Description Tocolytics
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Fetal Rhythm and Blues
 Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
PIAF study: Placental insufficiency and aortic isthmus flow Jean-Claude Fouron, MD
 Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
Index Note: Page numbers of article titles are in boldface type. A Acid base balance pregnancy-related changes to, 640 Acquired heart disease, 731 Acute fatty liver of pregnancy (AFLP), 618 Acute kidney
The Fetus: Five Top Do Not Miss Diagnoses. Doppler Ultrasound
 The Fetus: Five Top Do Not Miss Diagnoses Doppler Ultrasound Giancarlo Mari, MD, MBA Professor and Chair Department of Obstetrics and Gynecology University of Tennessee Health Science Center Memphis, TN
The Fetus: Five Top Do Not Miss Diagnoses Doppler Ultrasound Giancarlo Mari, MD, MBA Professor and Chair Department of Obstetrics and Gynecology University of Tennessee Health Science Center Memphis, TN
SWISS SOCIETY OF NEONATOLOGY. Peripartal management of a prenatally diagnosed large oral cyst
 SWISS SOCIETY OF NEONATOLOGY Peripartal management of a prenatally diagnosed large oral cyst May 2007 2 Fontana M, Berger TM, Winiker H, Jöhr M, Nagel H, Neonatal and Pediatric Intensive Care Unit (FM,
SWISS SOCIETY OF NEONATOLOGY Peripartal management of a prenatally diagnosed large oral cyst May 2007 2 Fontana M, Berger TM, Winiker H, Jöhr M, Nagel H, Neonatal and Pediatric Intensive Care Unit (FM,
Bits and Bobs secondary causes of heart problems. Dr Angela McBrien 9 th September 2017
 Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
Bits and Bobs secondary causes of heart problems Dr Angela McBrien 9 th September 2017 Not the heart Dextroposition Heart in the right chest with the apex to the left Often caused by left sided chest mass
COPYRIGHTED MATERIAL. The fetal circulation CHAPTER 1. Postnatal circulation
 1 CHAPTER 1 The fetal circulation The circulation in the fetus differs from that in the adult. Knowledge of the course and distribution of the fetal circulation is important to our understanding of the
1 CHAPTER 1 The fetal circulation The circulation in the fetus differs from that in the adult. Knowledge of the course and distribution of the fetal circulation is important to our understanding of the
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Preterm Labour and Tocolysis
 Title: CLINICAL GUIDELINES ID TAG Preterm Labour and Tocolysis Authors: Designation: Speciality / Division: Directorate: Dr L Bell, Dr K Price, Dr G McKeown, Mr D Sim Trainee, Trainee, CAH Consultant,
Title: CLINICAL GUIDELINES ID TAG Preterm Labour and Tocolysis Authors: Designation: Speciality / Division: Directorate: Dr L Bell, Dr K Price, Dr G McKeown, Mr D Sim Trainee, Trainee, CAH Consultant,
24. An infant with recurrent pneumonia underwent a frontal chest radiograph (Fig 24-A) followed by
 followed by") 24. An infant with recurrent pneumonia underwent a frontal chest radiograph (Fig 24-A) followed by diagnosis? ndings, what is the most likely A. Pulmonary sequestration B. Congenital pulmonary airway malformation
24. An infant with recurrent pneumonia underwent a frontal chest radiograph (Fig 24-A) followed by diagnosis? ndings, what is the most likely A. Pulmonary sequestration B. Congenital pulmonary airway malformation
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan
 CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
Before we are Born: Fetal Diagnosis of Congenital Heart Disease
 Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Failing right ventricle
 Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Assessment of fetal heart function and rhythm
 Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes!
 Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Case Based Fetal Lung Masses
 Case Based Fetal Lung Masses Advances in Fetal and Neonatal Imaging Course Orlando, Florida, January 28, 2017 Leann E. Linam, MD Associate Professor Radiology University of Arkansas for Medical Sciences/
Case Based Fetal Lung Masses Advances in Fetal and Neonatal Imaging Course Orlando, Florida, January 28, 2017 Leann E. Linam, MD Associate Professor Radiology University of Arkansas for Medical Sciences/
The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3-
 1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Medical Complications of Pregnancy
 Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Medical Complications of Pregnancy Systems Cardiovascular Pulmonary Endocrine Gastrointestinal Urologic Neurologic Cardiovascular System Physiologic anemia 3:1 increase of plasma volume:rbc mass Treat
Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias
 1386 JACC Vol 7. No 6 June 19X6 I3Xh-91 Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias JANETTE F. STRASBURGER, MD, JAMES C. HUHTA, MD, FACC, ROBERT J. CARPENTER,
1386 JACC Vol 7. No 6 June 19X6 I3Xh-91 Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias JANETTE F. STRASBURGER, MD, JAMES C. HUHTA, MD, FACC, ROBERT J. CARPENTER,
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
4/19/2018. St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT
 St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT Review Fetal Circulation Provide Indications for Umbilical Artery, Middle Cerebral Artery, and Ductus Venosus Doppler studies. Demonstrate normal
St. Cloud Hospital Perinatology Kristin Olson, RDMS, RVT Review Fetal Circulation Provide Indications for Umbilical Artery, Middle Cerebral Artery, and Ductus Venosus Doppler studies. Demonstrate normal
ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE
 Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Digoxin Therapy of Fetal Superior Ventricular Tachycardia: Are Digoxin Serum Levels Reliable?
 e272 Case Report THIEME Digoxin Therapy of Fetal Superior Ventricular Tachycardia: Are Digoxin Serum Levels Reliable? Antonio F. Saad, MD 1 Luis Monsivais, MD 1 Luis D. Pacheco, MD 1,2 1 Division of Maternal-Fetal
e272 Case Report THIEME Digoxin Therapy of Fetal Superior Ventricular Tachycardia: Are Digoxin Serum Levels Reliable? Antonio F. Saad, MD 1 Luis Monsivais, MD 1 Luis D. Pacheco, MD 1,2 1 Division of Maternal-Fetal
Major Forms of Congenital Heart Disease: Consultant Pediatric and Fetal Cardiology King Abdulaziz Cardiac Center, National Guard Hospital Riyadh
 Major Forms of Congenital Heart Disease: Impact of Prenatal Detection and Diagnosis Dr Merna Atiyah Consultant Pediatric and Fetal Cardiology King Abdulaziz Cardiac Center, National Guard Hospital Riyadh
Major Forms of Congenital Heart Disease: Impact of Prenatal Detection and Diagnosis Dr Merna Atiyah Consultant Pediatric and Fetal Cardiology King Abdulaziz Cardiac Center, National Guard Hospital Riyadh
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery s present: Early Repair Era
 Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
I n extrauterine life, narrow QRS supraventricular tachycardia
 1211 CONGENITAL HEART DISEASE Management of fetal tachyarrhythmia based on superior vena cava/aorta Doppler flow recordings J-C Fouron, A Fournier, F Proulx, J Lamarche, J L Bigras, C Boutin, M Brassard,
1211 CONGENITAL HEART DISEASE Management of fetal tachyarrhythmia based on superior vena cava/aorta Doppler flow recordings J-C Fouron, A Fournier, F Proulx, J Lamarche, J L Bigras, C Boutin, M Brassard,
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION
 ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
PULMONARY VENOLOBAR SYNDROME. Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital.
 PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Acute and Maintenance Page 1 of 11 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Acute and Maintenance Subcutaneous and Intravenous Tocolysis Professional
Acute and Maintenance Page 1 of 11 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: Acute and Maintenance Subcutaneous and Intravenous Tocolysis Professional
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
ISUOG Basic Training. Assessing the Neck & Chest Gihad Chalouhi, Lebanon
 ISUOG Basic Training Assessing the Neck & Chest Gihad Chalouhi, Lebanon Learning objectives 9 & 10 At the end of the lecture you will be able to: recognise the differences between the normal & most common
ISUOG Basic Training Assessing the Neck & Chest Gihad Chalouhi, Lebanon Learning objectives 9 & 10 At the end of the lecture you will be able to: recognise the differences between the normal & most common
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation
 First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
Fetal Arrhythmias: Diagnosis and Management. Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters
 Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters No industry or financial disclosures Thanks to Drs Abuhamad
Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters No industry or financial disclosures Thanks to Drs Abuhamad
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating)
") Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology (scores listed by Appropriate Use rating) Table 1: Appropriate indications (median score 7-9) Indication
Fetal Tetralogy of Fallot
 36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
A ccording to published reports, atrial flutter accounts for a
 913 CONGENITAL HEART DISEASE Review of diagnosis, treatment, and outcome of fetal atrial flutter compared with supraventricular tachycardia M Krapp, T Kohl, J M Simpson, G K Sharland, A Katalinic, U Gembruch...
913 CONGENITAL HEART DISEASE Review of diagnosis, treatment, and outcome of fetal atrial flutter compared with supraventricular tachycardia M Krapp, T Kohl, J M Simpson, G K Sharland, A Katalinic, U Gembruch...
What effects will proximal or distal disease have on a waveform?
 Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
SWISS SOCIETY OF NEONATOLOGY. Congenital ductus arteriosus aneurysm: serious or common?
 SWISS SOCIETY OF NEONATOLOGY Congenital ductus arteriosus aneurysm: serious or common? AUGUST 2011 * 2 Beauport L, Meijboom E, Vial Y, Gudinchet F, Truttmann AC, CHUV, Lausanne, Neonatology Unit (BL, TAC),
SWISS SOCIETY OF NEONATOLOGY Congenital ductus arteriosus aneurysm: serious or common? AUGUST 2011 * 2 Beauport L, Meijboom E, Vial Y, Gudinchet F, Truttmann AC, CHUV, Lausanne, Neonatology Unit (BL, TAC),
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Stroke in Pregnancy. Stroke in Pregnancy 6/23/13
 G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
CARDIOVASCULAR SYSTEM
 CARDIOVASCULAR SYSTEM Overview Heart and Vessels 2 Major Divisions Pulmonary Circuit Systemic Circuit Closed and Continuous Loop Location Aorta Superior vena cava Right lung Pulmonary trunk Base of heart
CARDIOVASCULAR SYSTEM Overview Heart and Vessels 2 Major Divisions Pulmonary Circuit Systemic Circuit Closed and Continuous Loop Location Aorta Superior vena cava Right lung Pulmonary trunk Base of heart
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Imaging of the Lung in Children
 Imaging of the Lung in Children Imaging methods X-Ray of the Lung (Anteroposterior, ) CT, HRCT MRI USG Congenital developmental defects of the lungs Agenesis, aplasia, hypoplasia Tension pulmonary anomalies
Imaging of the Lung in Children Imaging methods X-Ray of the Lung (Anteroposterior, ) CT, HRCT MRI USG Congenital developmental defects of the lungs Agenesis, aplasia, hypoplasia Tension pulmonary anomalies
disease, bronchopulmonary dysplasia, pulmonary hypoplasia and congenital diaphragmatic hernia.
 Neonatal Chest Imaging - What the Nurse Should Know Expires Monday, April 30, 2018 Nursing Michael J. Diament, M.D. Objectives 1. Describe a good technique for positioning a neonate for the purpose of
Neonatal Chest Imaging - What the Nurse Should Know Expires Monday, April 30, 2018 Nursing Michael J. Diament, M.D. Objectives 1. Describe a good technique for positioning a neonate for the purpose of
From Head to Toe Use of Advanced Dynamic Flow in prenatal ultrasound
 From Head to Toe Use of Advanced Dynamic Flow in prenatal ultrasound Without doubt, the B- Schwerdtfeger, R. tant diagnostic instrument. Furthermore, we use colour in feto- mode imaging is the most important
From Head to Toe Use of Advanced Dynamic Flow in prenatal ultrasound Without doubt, the B- Schwerdtfeger, R. tant diagnostic instrument. Furthermore, we use colour in feto- mode imaging is the most important
Nifedipine Tocolysis Regime Policy
 Document ID: MATY072 Version: 1.0 Facilitated by: Karen Wakelin, ACMM Issue Date: August 2010 Approved by: Maternity Quality Committee Review date: October 2017 Nifedipine Tocolysis Regime Policy Policy
Document ID: MATY072 Version: 1.0 Facilitated by: Karen Wakelin, ACMM Issue Date: August 2010 Approved by: Maternity Quality Committee Review date: October 2017 Nifedipine Tocolysis Regime Policy Policy
Mr. Eknath Kole M.S. Pharm (NIPER Mohali)
") M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
Pre-term birth occurs when a neonate is birthed or
 Susan L. Rideout, RN-C, BSN Pre-term birth occurs when a neonate is birthed or delivered prior to the completion of the 37th week of pregnancy. It s the leading cause of morbidity and the second leading
Susan L. Rideout, RN-C, BSN Pre-term birth occurs when a neonate is birthed or delivered prior to the completion of the 37th week of pregnancy. It s the leading cause of morbidity and the second leading
Cardiovascular Physiology. Heart Physiology. Introduction. The heart. Electrophysiology of the heart
 Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Admission/Discharge Form for Infants Born in Please DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
A. Incorrect! Think of a therapy that reduces prostaglandin synthesis. B. Incorrect! Think of a therapy that reduces prostaglandin synthesis.
 USMLE Step 1 - Problem Drill 02: Embryology Question No. 1 of 10 1. A premature infant is born with a patent ductus arteriosis. Which of the following treatments may be used as part of the treatment regimen?
USMLE Step 1 - Problem Drill 02: Embryology Question No. 1 of 10 1. A premature infant is born with a patent ductus arteriosis. Which of the following treatments may be used as part of the treatment regimen?
Arrhythmias. Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium.
 Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Atrial Flutter in Infants
 Journal of the American College of Cardiology Vol. 48, No. 5, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.04.091
Journal of the American College of Cardiology Vol. 48, No. 5, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.04.091
Large Arteries of Heart
 Cardiovascular System (Part A-2) Module 5 -Chapter 8 Overview Arteries Capillaries Veins Heart Anatomy Conduction System Blood pressure Fetal circulation Susie Turner, M.D. 1/5/13 Large Arteries of Heart
Cardiovascular System (Part A-2) Module 5 -Chapter 8 Overview Arteries Capillaries Veins Heart Anatomy Conduction System Blood pressure Fetal circulation Susie Turner, M.D. 1/5/13 Large Arteries of Heart
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
AWHONN Oregon Section 2014
 AWHONN Oregon Section 2014 Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth Hypertensive in Pregnancy Carol J Harvey, MS, RNC-OB, C-EFM Clinical Specialist Northside
AWHONN Oregon Section 2014 Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth Hypertensive in Pregnancy Carol J Harvey, MS, RNC-OB, C-EFM Clinical Specialist Northside
Drugs used in obstetrics
 Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
Drugs used in obstetrics Drugs used in obstetrics Drugs may be used to modify uterine contractions. These include oxytocic drugs used to stimulate uterine contractions both in induction of labour and to
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
Evaluation of Fetal Pulmonary Veins During Early Gestation by Pulsed Doppler Ultrasound: A Feasibility Study
 J. Fetal Med. (March 2015) 2:27 32 DOI 10.1007/s40556-015-0038-y ORIGINAL ARTICLE Evaluation of Fetal Pulmonary Veins During Early Gestation by Pulsed Doppler Ultrasound: A Feasibility Study Aldo L. Schenone
J. Fetal Med. (March 2015) 2:27 32 DOI 10.1007/s40556-015-0038-y ORIGINAL ARTICLE Evaluation of Fetal Pulmonary Veins During Early Gestation by Pulsed Doppler Ultrasound: A Feasibility Study Aldo L. Schenone
Prenatal diagnosis of long QT syndrome: Implications for delivery room and neonatal management
 Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications